
Abstract
Introduction
Lower limb amputation has significant morbidity and mortality. This study reviews the potential factors affecting the one-year mortality rate after lower limb amputation in the Hong Kong Chinese population.
Methods
Cases with lower limb amputations (toe, ray, below-knee, and above-knee amputations) from a regional hospital from January 2016 to December 2017 were recruited. Amputations due to trauma were excluded. The one-year mortality rate and the potential risk factors (age, sex, length-of-stay, multiple operations, extent of surgery (minor vs. major), medical comorbidities including (1) end-stage renal failure (ESRF), (2) cardiac diseases, (3) ischemic heart disease, (4) peripheral vascular disease and (5) diabetes mellitus) were analyzed by multiple logistic regression using Matlab 2018a.
Results
A total of 132 patients were recruited (173 operations). The one-year mortality rate was 36.3%. The mean age at death was 72.2 years. The results of the regression analysis showed patients having ESRF (β = 2.195, t 120 = 3.008, p = 0.003) or a major amputation (including above- or below-knee amputation) (β = 1.079, t 120 = 2.120, p = 0.034), had a significantly higher one-year mortality. The remaining factors showed no significant effect. The one-year mortality rate in ESRF patients was 77.8%; while the one-year mortality rate without ESRF was 29.8%. The mean age at death in the ESRF group was 62.9 years; while that without ESRF was 76.1 years. The one-year mortality for patients with major amputation was 45.8% while that for minor amputation was 20.4%.
Conclusion
ESRF and major amputation are factors that increase the one-year mortality rate after lower limb amputation.
Introduction
Lower limb amputation has significant morbidity and mortality. The one-year mortality after lower limb amputation was stated as around 50% in western countries. 1 However, local statistics are lacking. The aim of this study is to review the potential factors affecting the one-year mortality rate after lower limb amputation in the Hong Kong Chinese population.
Methods
This is a retrospective case study. Cases who received lower limb amputations (toe, ray, below knee amputation (BKA), and above knee amputation (AKA)) from a regional hospital from January 2016 to December 2017 were recruited. Major causes of amputation include (1) chronic ischemia associated with peripheral vascular disease (PVD); (2) infection or complications related to diabetes mellitus (DM), (3) acute lower limb ischemia, and (4) necrotizing fasciitis. Amputations due to trauma were excluded. Among the cases who received low limb amputation, the one-year mortality rate and the potential risk factors associated with higher one-year mortality (age, sex, length-of-stay, multiple operations, extent of surgery (minor vs. major), medical comorbidities including (1) end-stage renal failure (ESRF), (2) cardiac diseases (except ischemic heart disease (IHD)), (3) IHD, (4) PVD; and (5) DM) were identified and analyzed by multiple logistic regression using Matlab 2018a. A p-value <0.05 is statistically significant. The 1-year mortality is counted from the last lower limb amputation patient received. Length of stay is defined as the duration of in-patient stay for the last operation. For patients defined as having multiple operations, he/she must have undergone more than one lower limb operation either in current or previous related hospital admissions. Minor operations are defined as receiving toe/ray amputation as the last operation. Major amputations are defined as receiving BKA/AKA (single/ bilateral) as the last operation.
Results
A total of 132 patients were recruited, including 76 male and 56 female patients. The mean age at operation was 71.2 years old. The mean length of stay was 31.75 days. 32 (24.2%) patients had multiple operations. There were 173 operations in total. There were 78 toe/ray amputations; 37 BKAs; 56 AKAs; 1 bilateral BKA; 1 bilateral AKA. There were 18 (13.6%) patients who had ESRF (11 patients had peritoneal dialysis (PD); 5 patients had hemodialysis; 2 patients were not on any renal replacement therapies), 21 (15.9%) patients with cardiac disease other than IHD, 18 (13.6%) patients with IHD, 45 (34.1%) patients with PVD and 95 (72.0%) patients with diabetes. There were 48 in 132 (36.4%) patients who died within 1 year after the operation. The mean age at death was 72.2 years. Among 48 patients who died within 1 year, 27 patients died due to sepsis; 17 patients died due to causes other than sepsis (i.e. cardiac diseases, renal failure, fluid overload, pulmonary conditions other than infection); four patients died of unknown causes.
Before multiple logistic regression analysis was performed, a test showed that the auto-correlations between the risk factors were low (|r|<0.5), and the variance inflation factor of each factor was also low (all below 1.653). The results of the regression analysis showed that two out of ten risk factors showed a significantly higher risk of one-year mortality (Table 1). These factors are (1) ESRF (β = 2.195, t 120 = 3.008, p = 0.003) and (2) major amputation (including AKA or BKA) (β = 1.079, t 120 = 2.120, p = 0.034). The remaining factors: age (p = 0.339), sex (p = 0.601), multiple operations (p = 0.873), days of hospital stay (p = 0.230), cardiac disease except for IHD (p = 0.928), IHD (p = 0.876), PVD (p = 0.116), and diabetes (p = 0.509), showed no significant effect.
Results of regression analysis showed that 2 of the 10 risk factors showed a significantly higher risk of one-year mortality.
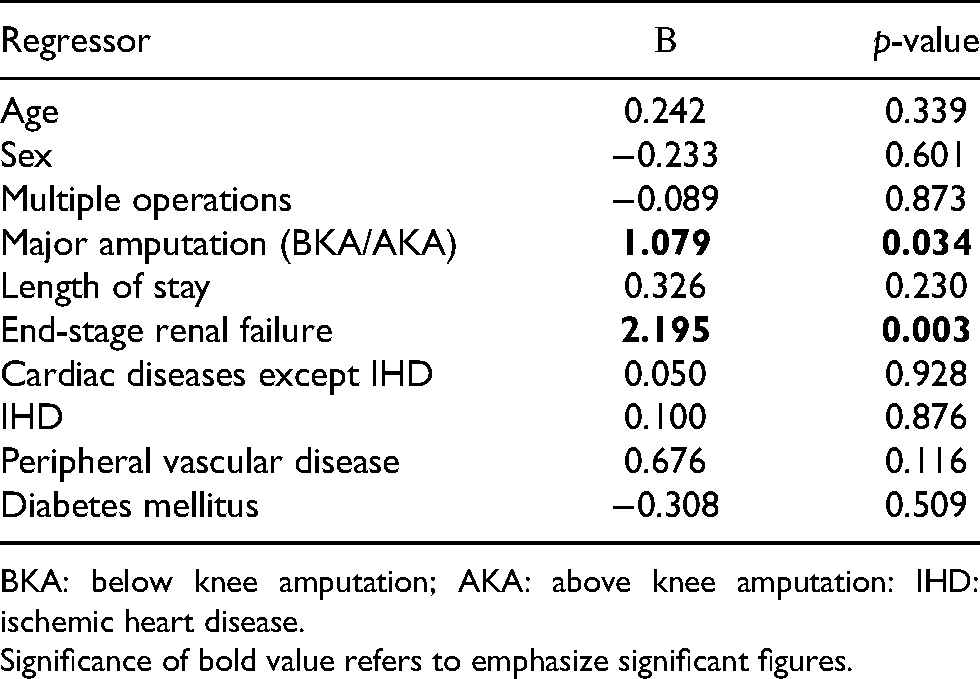
BKA: below knee amputation; AKA: above knee amputation: IHD: ischemic heart disease. Significance of bold value refers to emphasize significant figures.
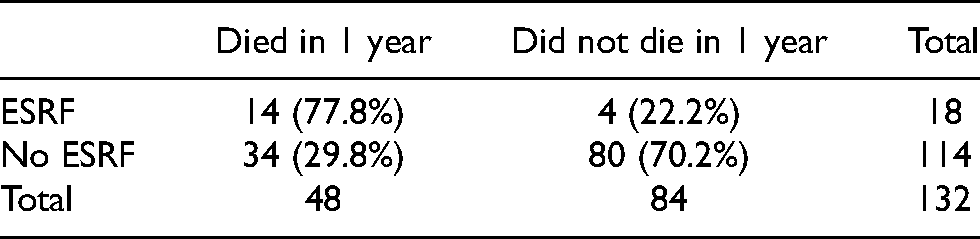
Looking into details, the 1-year mortality rate in ESRF patients was 77.8% (14 in 18 patients); while the 1-year mortality rate without ESRF was 29.8% (34 in 114 patients) (Table 2). The mean age at death in the ESRF group was 62.9 years; while that without ESRF was 76.1 years. Table 3 shows the demographics and outcomes of the 18 ESRF patients in our study. Among the 14 ESRF patients who died within 1 year, 7 of them died of sepsis or infection, while the others died of other causes. There is no evident correlation between sepsis/infection and ESRF. The 1-year mortality rate in ESRF patients who had minor lower limb amputation was 66.7% (4 in 6 patients); while the 1-year mortality rate in patients without ESRF who had minor lower limb amputation was 14.0% (6 in 43 patients) (Table 4).
One-year mortality rate in end-stage renal failure (ESRF) patients after lower limb amputation.
Demographics and outcomes of the 18 ESRF patients in our study (Y = yes; N = no).
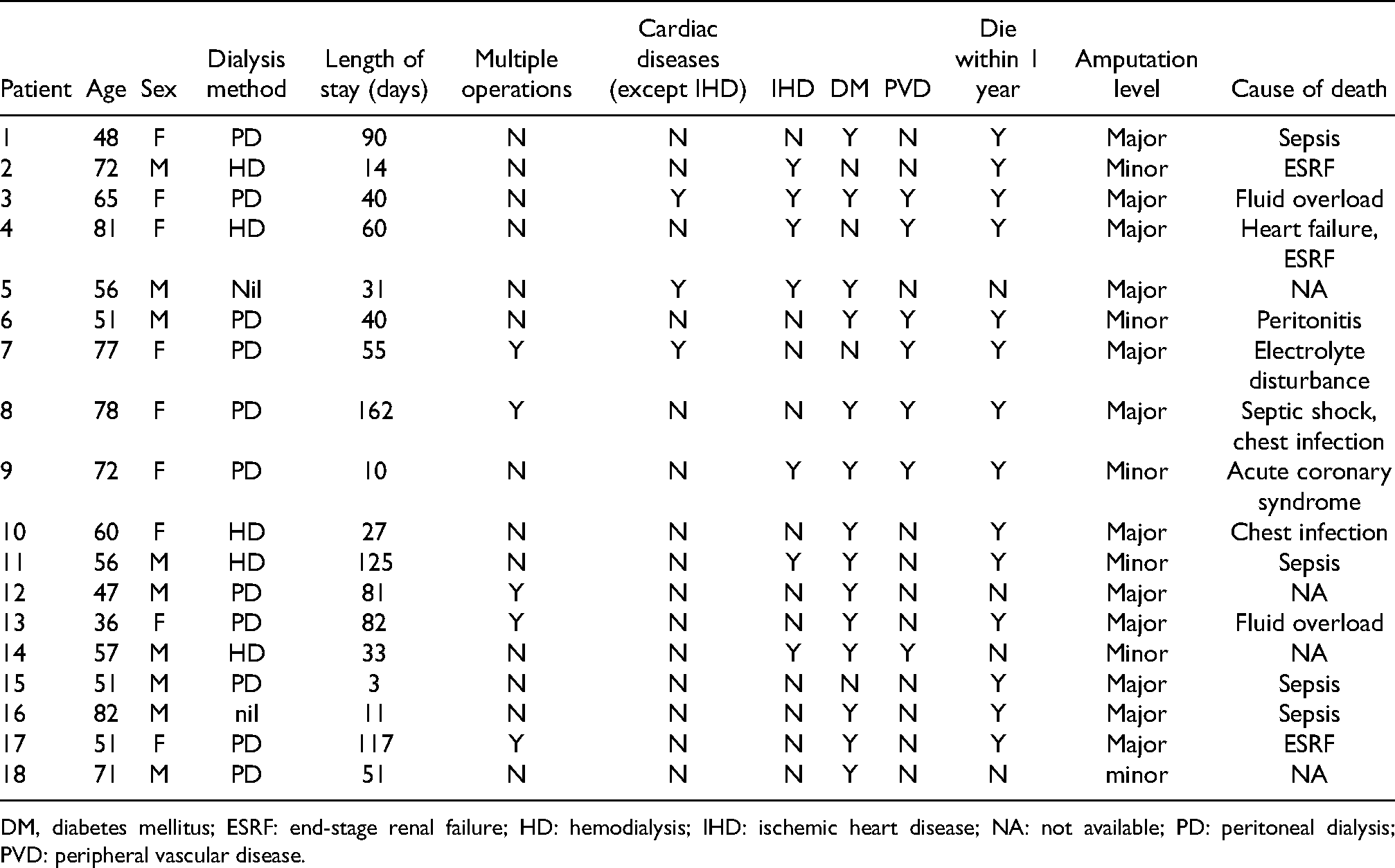
DM, diabetes mellitus; ESRF: end-stage renal failure; HD: hemodialysis; IHD: ischemic heart disease; NA: not available; PD: peritoneal dialysis; PVD: peripheral vascular disease.
One-year mortality rate in patients with/without end-stage renal failure (ESRF) who had minor lower limb amputation.

Among the 18 ESRF patients, risk factors including DM, PVD, extent of surgery, and method of dialysis were further analyzed using Fisher's exact test to look for any association between these factors and a higher risk of 1-year mortality after lower limb amputation. Results showed that none of these factors were associated with a statistically significant higher 1-year mortality (p = 0.225, 0.518, 0.423, and 0.605) (Tables 5 to 8).
One-year mortality rate in ESRF patients with/without DM after lower limb amputation (p = 0.225).
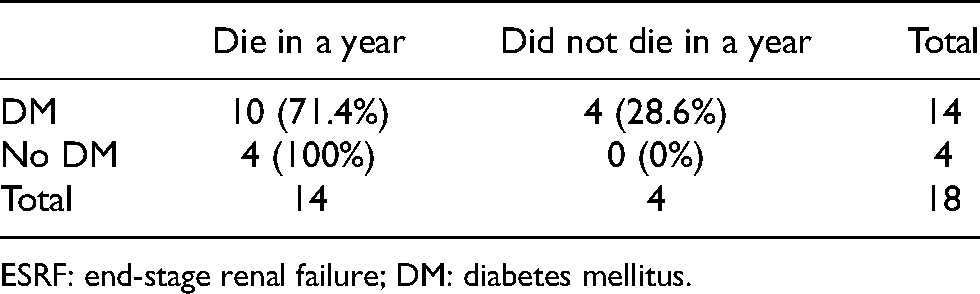
ESRF: end-stage renal failure; DM: diabetes mellitus.
One Year mortality rate in ESRF patients with/without PVD after lower limb amputation (p = 0.518).
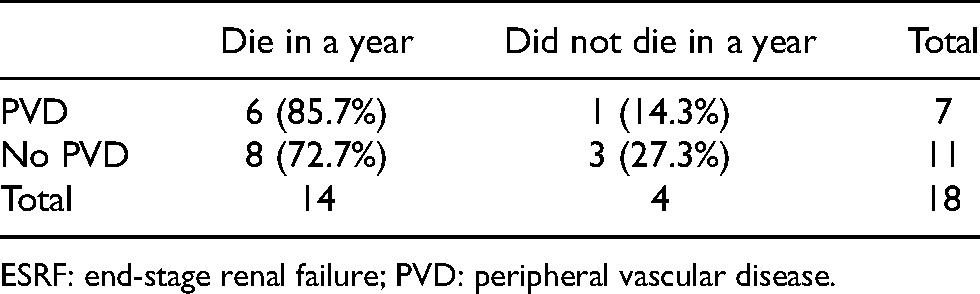
ESRF: end-stage renal failure; PVD: peripheral vascular disease.
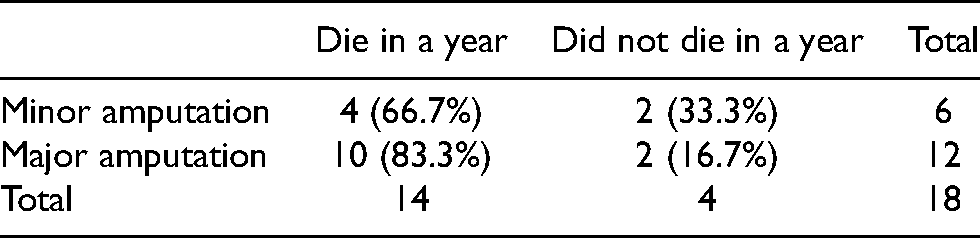
One-year mortality rate in end-stage renal failure (ESRF) patients after minor/ major lower limb amputation (p = 0.423).
One-year mortality rate in ESRF patients who had PD/non-PD after lower limb amputation (p = 0.605).
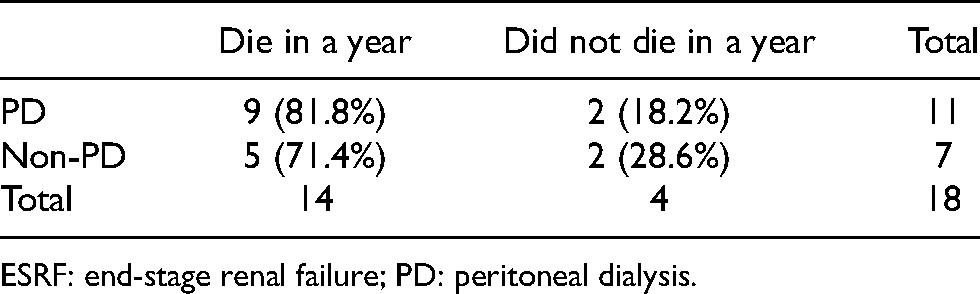
ESRF: end-stage renal failure; PD: peritoneal dialysis.
The 1-year mortality for patients with major amputation was 45.8% (38 in 83 patients); while the 1-year mortality rate for patients with minor amputation was 20.4% (10 in 49 patients) (Table 9).
One-year mortality rate in patients having major amputation (including BKA and AKA), compared to those with minor amputation (toe/ray amputation).
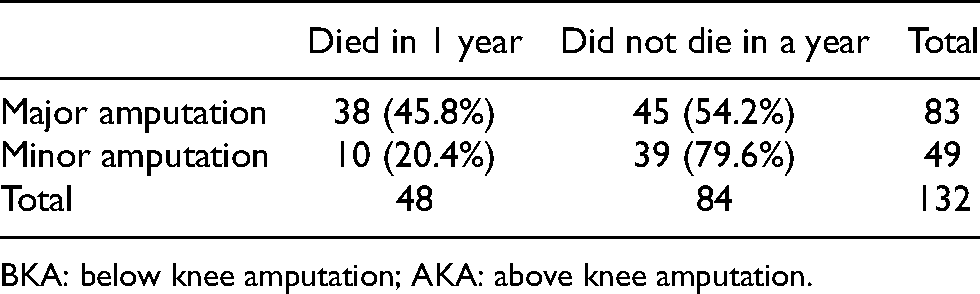
BKA: below knee amputation; AKA: above knee amputation.
Discussion
Our study showed that the one-year mortality rate after lower limb amputation in patients with ESRF is significantly higher than those without ESRF. A study by Dossa 2 showed the overall mortality rate in ESRF patients after lower limb amputation was 24%, whereas the overall mortality rate was only 7% in non-ESRF patients (p = 0.001). Another study by Aulivola et al. 3 showed a 1-year mortality rate of 48% among patients with ESRF, while the 1-year mortality rate was only 25% in those without ESRF after lower limb amputation (p < 0.001). 3 Shah et al. 4 also showed a hazard ratio of 2.5 when comparing the 1-year mortality in patients with ESRF to those without ESRF after lower limb amputation (p < 0.001). Our study, compared to the above Western studies, showed a higher 1-year mortality rate in ESRF patients after lower limb amputation (77.8%) (Table 2). We postulated that this might be due to cultural differences between local and western countries. Local patients tend to seek medical treatment at a later stage, which resulted in higher mortality. Another reason we could postulate is that in our locality, most ESRF patients received PD; while those patients in the Western countries received hemodialysis. This might also affect the prognosis after lower limb amputation.
In our study, a high 1-year mortality (66.7%) was found among ESRF patients with only minor lower limb amputation (Table 4). It signifies a higher risk of postoperative mortality in ESRF patients, regardless of the level of amputation. There was a high prevalence of concomitant DM (77.8%) and PVD (38.9%) among ESRF patients in our study. However, analysis of these patients showed that DM, PVD, extent of surgery, and method of dialysis were not associated with higher 1-year mortality after amputation (Tables 5–8). ESRF itself was already associated with a higher postoperative mortality. Factors that contributed to the higher mortality rate in patients with ESRF may include (1) fluid overload; (2) electrolytes imbalances; (3) immunocompromised status. These factors will result in delayed and poor wound healing, as well as a higher rate of wound infection.
The overall 1-year mortality for patients with major amputation (45.8%) was higher than that after minor amputation (20.4%) (Table 9). There are several explanations for the higher mortality after major amputations, these patients are (1) associated with more advanced PVD; (2) associated with more severe sepsis on presentation; (3) greater amount of blood loss; (4) higher risk of perioperative cardiac events due to alteration in circulatory volume and (5) required a longer period of immobilization post-operatively and hence resulted in higher risks of pneumonia, pressure sores, deep vein thrombosis, pulmonary embolism. These factors could all contribute to a higher 1-year mortality rate.
Our study can be used in daily clinical practice as there is not much local data on lower limb amputation previously. We face patients requiring lower limb amputations every day, and most of them carry medical comorbidities, including a significant number with ESRF. The quoted mortality figures and risk factors affecting mortality can be used during patient discussion and guide our decision-making.
Limitations
Our study is retrospective, the number of patients recruited was relatively small, and among them, only 18 patients suffered from ESRF. The results generated may not represent all ESRF patients who underwent lower limb amputation. The results generated may still be affected by confounders, although multiple logistic regression was used and the auto-correlations between the risk factors were low. Fisher's exact test was used to further analyze ESRF patients, but it was unable to control confounders. Regression analysis was not used here as the sample size was too small (18 ESRF patients only). In reality, there were also a number of patients with undiagnosed/unlabeled PVD, particularly in those with ESRF and DM. So the percentage of patients with PVD might be underestimated.
Conclusion
In conclusion, ESRF and receiving a major amputation are the two most significant risk factors for 1-year mortality after lower limb amputation. Prevention of lower limb amputation with aggressive foot care and patient education in ESRF patients should be advocated. It is also important to explain the risks of high one-year mortality to these groups of patients and their families to make an informed decision for the operation.
Footnotes
Ethics approval
The research has been approved by the Research Ethics Committee (Kowloon Central/ Kowloon East) on 17 September 2020, according to the guidance of the Declaration of Helsinki and ICH GCP Guidelines. Ref: KC/KE-20-0201/ER-4.
Declaration
The research has been presented in the 40th Annual Congress of the Hong Kong Orthopaedic Association held on 31 October–1 November 2020.
Author contributions
All authors contributed to the (1) concept or design, (2) acquisition of data, (3) analysis or interpretation of data, (4) drafting of the manuscript, and (5) critical revision for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.