
Abstract
Purpose:
Various modes of therapy have been directed at breaking the vicious cycle at early stage of synovitis in haemophilia patients. This study was planned to assess the short-term clinico-radiological outcome of chronic knee synovitis among haemophilia A patients post phosphorus-32 (P-32) radiosynoviorthesis.
Methods:
P-32 samarium radiocolloid was injected into the knee and patients were followed up at 1 and 3 months, respectively. Clinical outcomes was assessed using Tegner Lysholm scores (TLSs), Modified Knee Society Clinical Rating System (MKSS) score and circumference of the knee joint. The radiological outcomes were assessed using X-ray, ultrasonography and bone scan.
Results:
Among the fifteen haemophilia A patients studied, there was statistically significant difference in TLS (χ 2(2) = 27.887 and p value < 0.001), MKSS scores (χ 2(2) = 27.745 and p < 0.001) and circumference of the knee joint (χ 2(2) = 21.333 and p < 0.001) at preoperatively, 1- and 3-month follow-up. There were no changes noted in follow-up X-rays compared with the preoperative X-ray. Ultrasonography showed that clinical improvement was more in suprapatellar and medial parapatellar regions in the last 2 months compared to the first month of follow-up. Post P-32 bone scan showed marked decrease in uptake in the affected knee joint suggestive of radio ablation of synovial tissue.
Conclusion:
P-32 radiosynoviorthesis done for chronic synovitis among haemophilia A patients showed significant improvement in both clinical and radiological parameters. Ultrasonography can be utilized as non-invasive radiological modality for follow-up of P32 response for knee joint.
Keywords
Introduction
Haemophilia is an X-linked disease which predominantly affects males. Haemophilia A exhibits a wide range of clinical severity according to level of factor VIII serum level. 1 In all symptomatic patients, there is a tendency towards easy bruise and haemorrhage after trauma, spontaneous bleeding into various joints and after operative procedures. The most characteristic feature of haemophilia is synovitis. Recurrent bleeding occurs predominantly in the joints, and eventually, there is hemosiderin release from lysed RBC’s which incites synovial inflammation and consequently a cycle of synovitis–hemarthrosis synovitis occurs. 2 Intraarticular bleeds incite a cycle of synovitis which perpetuates bleeding into knee joint.
Various modes of therapy have been directed at breaking this vicious cycle at early stage of synovitis itself. Intraarticular steroids have been used to suppress synovial proliferation. 3 This therapy however causes increased risk of relapse and thus may have to be given repeatedly. It is also associated with numerous articular complications. Surgical procedures include arthroscopic debridement and subtotal synovectomy, permanent ankylosis in functional position and total joint replacement. Surgical synovectomy even though was successful initially, it required prolonged hospital stay, risks associated with general anaesthesia, intraoperative surgical risks, risk of perioperative bleeding and prolonged rehabilitation post-operatively. Many patients had difficulty regaining range of movements. Haemophiliac patients had to undergo surgery under cover of factor VIII for the fear of uncontrollable haemorrhage and patients having clotting factor inhibitors were not the candidates for surgical synovectomy. 4
Radiosynoviorthesis being a minimally invasive procedure significantly regresses the hypertrophic synovium, episodes of bleeding and articular pain. For radiosynoviorthesis, isotopes emitting β-energy after decaying are injected into the joints. Radioisotopes like yttrium-90, rhenium-186 or phosphorous-32 (P-32) have been used for this purpose. These radioisotopes, which are β emitters, generate free radicals resulting in apoptosis and finally ablation of inflamed synovial membrane. 5 Moreover, these molecules are safe and cause no damage to the articular surface.
Few studies showing good results have been published worldwide documenting the efficacy of radiosynoviorthesis in rheumatoid arthritis, haemophilia and pigmented villonodular synovitis. In conditions like haemophilia where factor replacement is expensive, radiosynoviorthesis help reducing the number of rebleeds improving not only joint function but reduces significant economic burden to the patients. 6
With this background, this study was done to assess the short-term clinico-radiological outcome of chronic knee synovitis among haemophilia A patients post P-32 radiosynoviorthesis.
Materials and methods
A prospective observational study was done among haemophilia A patients with chronic knee synovitis attending a tertiary care centre, Pondicherry, India. The study was carried out during March 2014 to November 2015. The study was approved by the Institute Scientific Advisory Committee and the Institute Ethics Committee for human studies.
All patients with cases of chronic synovitis of knee joint of more than 3 months duration and patients age more than 7 years attending the outpatient department were included in the study. Patients who had advanced knee arthritis of any cause, patient with prior knee surgery, local skin infection around knee, neuropathic joint and infectious arthritis of knee joint were excluded from the study.
Clinical evaluation of knee was done, and baseline clinical and radiological parameters were noted before doing radiosynoviorthesis. Clinical parameters were studied using Tegner Lysholm scoring scale 7 , which is a subjective scoring scale. The objective assessment was done using Knee Society Clinical Rating System 8 and the joint circumference measured just above the upper margin of the patella. The radiological parameters were studied using X-ray of affected knee, ultrasonographic (USG) assessment of synovial thickness and three-phase 99mTc-methylene diphosphonate (MDP) bone scintigraphy for assessment of inflammation in chronic synovitis.
Tegner Lysholm score (TLS) scale is patient-based assessment questionnaire designed to assess knee symptoms primarily with ligamentous injuries, meniscal tears, patella femoral pain and knee osteoarthritis. The maximum score is 100 points.
Modified Knee Society Clinical Rating System (MKSS) is an objective knee scoring system that is based on clinical parameters. Scoring points include for pain, stability and range of motion and deduction scores for extension lag, flexion contracture and malalignment after clinical examination of affected knee. The maximum knee score is 100 points.
The joint circumference was measured just at the upper margin of patella with knee extension or permissible minimum flexion deformity in centimetre scale with non-expandable measuring tape. All the three clinical parameters were measured at pre-radiosynoviorthesis, 1- and 3-month follow-up.
X-ray evaluation of knee was done, and an image is recorded. This images the femur, tibia and fibula, patella and surrounding soft tissues. Weight bearing images are taken anteroposterior view and lateral view of the knee for radiological assessment. The X-ray outcome was reported as whether there was any improvement or not (yes/no) compared with the baseline X-ray. The outcome was measured using the criteria such as decreased joint space, subchondral cyst presence/absence, erosion of joint margins and juxtaarticular osteopenia.
USG assessment of synovial thickness was done using a high frequency transducer probe of 8–12-MHz probe. Synovial thickening appears as hypoechoic or heterogeneous proliferation. With patient in supine position knee is flexed to 20–30° to stretch the quadriceps. Deep to distal third of the quadriceps, maximal synovial thickness is calculated. For medial synovial thickness keeping the transducer obliquely, leg is rotated externally maintaining 20–30° knee flexion and similarly with internal rotation with knee flexion for lateral synovial thickening measurement in millimetre at pre P-32, 1 and 3 months, respectively.
Bone scan was performed in the Department of Nuclear Medicine. Tc99 labelled MDP dose of 0.25-mCi/kg body weight was injected intravenously. Blood flow images (first phase) acquired, immediately after the intravenous injection of 99mTc-MDP, with area of interest (knee) under the field of view of the gamma camera. Blood pool images (second phase) acquired within 5 min following tracer injection and skeletal phase (third phase) acquired after 2 h of tracer injection. Bone scan was performed at baseline before P-32 administration and 3 months following P-32 radiosynoviorthesis.
Factor VIII was given both during pre and post P-32 radiosynoviorthesis to prevent bleeding into joints after radioisotope injection.
Factor VIII injection required calculation 9
All haemophilia patients underwent factor VIII replacement during the procedure. Routine prophylaxis of factor VIII was given according to patient weight (kg) and percentage of desired levels of pre and post radiosynoviorthesis is calculated by the following formula:

Desired factor level increase was taken as pre-injection 40% of normal and post-injection (day 1) as 30% of normal.
P-32 samarium radiocolloid was supplied to the institute by the Board of Radiation and Technology (BRIT), Mumbai, India. The administered activity of P-32 samarium colloid ranged from 10 to 40 MBq depending on the age and knee joint size for therapy. In adults, the dose administered is 37 MBq and in case of children’s the dose would be 40–50% of the adult dose.
Technique of radiosynoviorthesis
Under all aseptic precautions, patient is made to lie with knee gently flexed by an underlying cushion. Cleaning and draping of knee region were done. Patients were injected P-32 samarium colloid radioisotope to knee joint under local anaesthesia. With the fingers of the left hand, the patella is pushed slightly lateral, so that the left thumb can easily palpate the place between the lateral upper border of the patella and the insertion of the rectus femoris tendon. Then slightly posterior to the patella, the needle is inserted. The first drops of the local anaesthetic are injected subcutaneously. Synovial fluid aspirations were done but not complete aspiration, so that sufficient distribution volume is left. If there is lack of effusion, instillation of about 10–30 ml of saline was done, to provide a sufficient distribution of volume. Complete blood aspiration was done before injection, if any. The radioisotope P-32 samarium colloid was administered; then needle is flushed with 1-ml triamcinolone simultaneously by insulin syringe withdrawing the needle from the knee joint. The injected joint was passively flexed and extended five times to distribute the P-32 evenly. 10 The distribution of radiotracer of P-32 colloid in the joint was confirmed under gamma camera next day (post therapy distribution scan). The procedure was done with 1 day admission basis, and patients were sent home next day. The patients were advised to keep the injected joint immobilized for 3 days with plaster of Paris slab. Mild local pain was treated using analgesics. Patient was reviewed after 3 days for wound inspection. Follow-up at 1 and 3 months for clinical and radiological evaluation was done using the same scores and radiological methods as done in preoperatively. Follow-up three-phase bone scan was done at 3 months follow-up to assess the changes in synovial inflammation.
Data entry and statistical analysis
Data was entered using Microsoft Excel and analysed using IBM SPSS Version 20. Continuous variables like age and scores (TLS score, MKSS score and USG) were expressed using median (IQR). Categorical variables like sex and factor levels were expressed using proportions. Friedman test was used to see for significant difference in scores at different time periods, and post hoc tests were run using Wilcoxon signed-rank test. Statistical significance was set at p value less than 0.05 and 0.017 as cut-off for post hoc tests.
Results
Among the 15 male patients followed up median (IQR) age was 20 (10–23) years. The minimum age was 8 years and maximum 30 years. Six (40%) were under the age of 15 years and nine (60%) were above the age of 15 years. Among the 15 patients, four of them had estimated factor levels of 1% and eight of them had factor levels between 1% and 5%, whereas three of them had factor levels of more than 5%.
Friedman test showed that there was a statistically significant difference in TLS score at preoperatively, 1- and 3-month follow-up (χ 2(2) = 27.887 and p value < 0.001). There was also statistically significant difference in MKSS scores at preoperatively, 1 and 3 months follow-up (χ 2(2) = 27.745 and p < 0.001). Similarly, a statistically significant difference was noted in the circumference of the knee joint at the level of supra patellar region at preoperatively, 1 and 3 months follow-up (χ 2(2) = 21.333 and p < 0.001). Post hoc analysis with Wilcoxon signed-rank tests is shown in Table 1. Both TLS and MKSS scores and also the circumference of knee joint at the level of suprapatellar region showed that the clinical improvement is more in the last 2 months compared to the first month as shown by the difference in the median scores as shown in Table 1.
Subjective and objective assessment of clinical improvement in chronic knee synovitis among haemophilia A patients post P-32 radiosynoviorthesis (N = 15).

TLS: Tegner Lysholm score; MKSS: Modified Knee Society Clinical Rating System. aWilcoxon signed-rank test.
X ray evaluation showed changes like joint effusion, juxtaarticular osteoporosis and widened intercondylar notch which were stable in 3 months study period. There were no changes noted in follow-up X-rays compared with the preoperative X-ray.
Table 2 shows the suprapatellar, medial parapatellar and lateral parapatellar synovial thickness of the knee joint during preoperative, 1 and 3 months follow-up done using ultrasonography. The clinical improvement was more in suprapatellar and medial parapatellar regions in the last 2 months compared to the first month as shown by the difference in the median scores. But, the clinical improvement was consistent in the last 2 months and the first month in the lateral parapatellar as shown by the difference in the median scores.
Sonological assessment in chronic knee synovitis among haemophilia A patients post P-32 radiosynoviorthesis (N = 15).
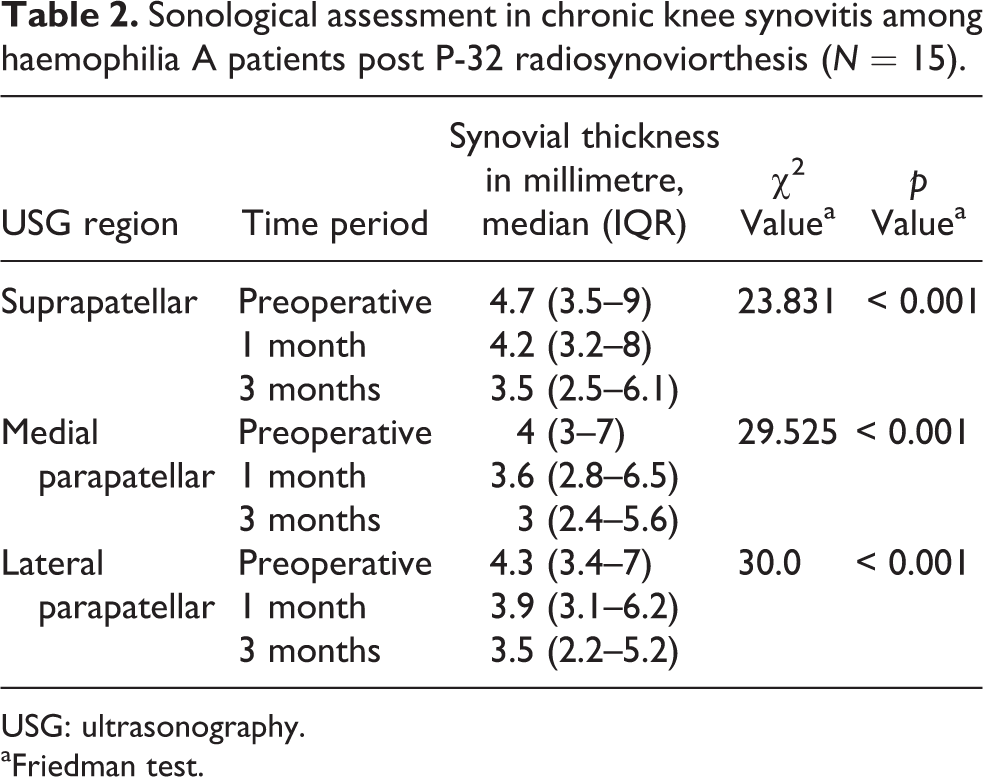
USG: ultrasonography.
aFriedman test.
Bone scan preoperatively showed increased tracer distribution in flow, tissue pool and increased tracer uptake in delayed phase in the affected knee joints (three-phase positive). Scan done later showed marked decrease in uptake in the affected knee joint suggestive of radio ablation of synovial tissue.
Discussion
Radiosynoviorthesis is a novel method of treatment used for chronic synovitis. It causes radio synovial ablation and halts progression of synovitis. Among all the radioisotopes, we have evaluated P-32 radioisotope in haemophilic synovitis and various inflammatory chronic synovitis, as various literature outside India has shown successful outcomes in chronic synovitis and also easy availability of this radioisotope in our institution. There are also no reported studies from India which looked into P-32 isotope use in radiosynovectomy.
The present study was designed to evaluate the early clinical and radiological outcomes of radiosynoviorthesis in haemophilia and chronic synovitis. Since there was easy availability of P-32, as this colloid was supplied to the institute by BRIT, we choose this radionucletide for the study. P-32 being a pure β emitter with particle size between 6–20 µm, 3–5-mm penetration and half-life of 14 days is currently the agent of choice in the United States and Canada. 11
Among the patients studied, all of them were followed up for 3 months after P-32 radiosynoviorthesis. All showed clinical improvement in both subjective (measured using TLS) and objective (measured using MKSS and circumference of knee joint at the suprapatellar region) measurements. As there are no reported studies from India which looked into P-32 isotope use in radiosynoviorthesis, we compared our study results with those studies done outside India. Among the various studies conducted, the clinical improvement was shown to be in the range between 60% and 80% across various joints in nine studies published between 1982 and 1991 by Das 12 . The follow-up time in different studies ranged between 1 month and 5 years.
The difference in the rates of clinical improvement across studies can be attributed to various factors. First, the measurements of clinical outcomes are done using different scoring systems. Second, we have assessed early outcomes (i.e. at 1 and 3 months) compared to other studies which have assessed outcomes after a longer period of time. Third, our study had all patients who were aged less than 30 years compared to different age groups across other studies. Fourth, the current study focused on only knee joint unlike others who had studied in more than one type of joints and use of different radio isotopes in the study.
All the patients showed improvement in radiological outcomes at both 1- and 3-month follow-up. In the current study, X-ray images showed to have no role in the study the short outcomes of P-32 injections.
Assessment of synovial thickness showed that sonological improvement was more in suprapatellar and medial parapatellar regions in the last 2 months compared to the first month but in the lateral parapatellar region, the improvement was consistent. The delay in regression of synovium indicates the time taken for radio ablation of hypertrophic synovial tissue, necrosis and destruction.
The radiological outcomes measured in different studies showed improvement between 80% and 90%. 13 Most of the studies had used X-ray or magnetic resonance imaging to capture the radiological improvement. Our study used X-ray, USG and also bone scan to measure the radiological improvement. In our study, X-ray did not show any signs of improvement in any of the patients compared with the other two modalities which showed significant improvements in all the patients. This shows that X-ray may not be the right method to assess the immediate radiological outcomes in post radio synovectomy patients. The difference in the outcome rates may be attributed to the use of different modalities to measure outcomes and also for all the other reasons as explained for the clinical improvement.
We had no immediate complications in any patients. Other studies have noted immediate complications such as drug extravasations and superficial skin necrosis. The radiation dose to the gonads is negligible, and the hypothetical morbidity from induction of tumours by whole body radiation is low. An increased risk for cancer after radiosynoviorthesis has not been reported. Infection in joints is very rare (one in 35,000) because intense beta radiation by radioisotope kills the bacteria. Thrombosis and lymph oedema may occur. 14
The study has few strengths. First, this is the first prospective clinical study in India, which evaluated short-term beneficial effect of P-32 radio synovectomy. Second, we have used non-invasive modality like ultrasonography to capture the radiological improvement. Third, both objective and subjective scoring systems were done to assess the clinical outcome in the patients. As only one investigator assessed the clinical outcomes in both subjective and objective components in all the patients, there was no chance of inter-observer variability.
The study also has few limitations. We could not capture the factor VIII usage levels before and after radio synovectomy, which could have been used as a marker for clinical improvement. As this study was planned to assess short-term outcomes, we were not able to assess the long-term outcomes of P-32 radio synovectomy.
The study has few implications. Our study showed that X-ray may not be useful to measure improvement in post radiosynoviorthesis patients. We have also showed that ultrasonography, which is a non-invasive procedure and does not have any radiological exposure, can be used to assess the immediate outcomes in post radiosynoviorthesis patients. Ultrasonography use can be made standardized by developing a scoring system which could be validated using the variables studied in the current study. The study also establishes a need for a standard protocol for P-32 radiosynoviorthesis that has to be formulated in the future.
Conclusion
P-32 radiosynoviorthesis done for chronic synovitis among haemophilia A patients showed significant improvement in both clinical and radiological parameters. The improvement was more so in the last 2 months compared to the first month follow-up after treatment. X-ray images have no role to study the short outcomes of P-32 radiosynoviorthesis. USG can be utilized as non-invasive radiological modality for follow-up of P32 response for knee joint.
Footnotes
Acknowledgements
We acknowledge the great help provided by Dr Mahendra M Reddy in statistical evaluation of the data for this study. We also acknowledge Dr P Nalini for factor VIII support from Haemophilia Society, Puducherry, India.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.