
Abstract
Background:
Operative treatment of displaced patella fracture dates back to Lister in 1877. Nowadays, steel wires remain the material of choice in tension band technique despite complications such as wire breakage, suboptimal placement, or skin impingement. We propose using a high-tensile strength braided tape-shaped polyblend suture (FiberTape®, Arthrex, Naples, Florida, USA) as an alternative that could minimize complications related to steel wires.
Method:
Between February 2014 and April 2018, 15 patients with displaced patella fractures (three distal pole, five transverse, and seven comminuted fractures) underwent our proposed method. Open fracture reduction was performed to optimize anatomy before figure-of-eight fixation with FiberTape®. An Ethibond-2 suture was also added as cerclage for stability. Postoperatively, an extension brace was given for wound resting, before progressing to mobilization exercises with a hinge-knee brace. At follow-ups, the knee’s range-of-motion (ROM), along with bone healing status from radiographs, was assessed.
Results:
The mean operation time was 84.5 min, and all surgeries were performed or supervised by the same senior surgeon. Eight patients were discharged from follow-up (mean follow-up of 9.9 months) after achieving good ROM and fracture healing. One patient defaulted, and the remaining is still being followed-up. There was no wound complication or knot impingement in all cases. One patient required manipulation under anesthesia due to stiffness, and one experienced malunion due to poor compliance to rehabilitation protocol.
Conclusion:
Fixation using a high-tensile strength braided suture may be an equally effective method in the management of displaced patella fracture. However, larger sample size is useful to provide a more definitive conclusion.
Keywords
Introduction
With the predicted increase in the elderly population, there will be an inevitable increase in traumatic fractures due to an elderly’s decrease in function and mobility. Patella fractures remain a common condition that orthopedic surgeons face, though accounting for only around 1% of all skeletal fractures. 1 Current treatment for patella fractures can be traced back to Dr Joseph Lister in 1877 where he experimented on metallic wires to fix open patella fractures in the process of perfecting his antiseptic technique. 2,3 His surgical method eventually evolved into the tension band wiring technique we use today.
Traditionally, surgical treatment of patella fractures involves clear wound dissection down to fracture. Upon clearing of hematoma and reduction of fracture, alignment was temporarily held in place using Kirschner wires (K wires). Fixation was then performed by inserting one metallic wire as a tension band through the quadricep tendon and patella tendon in a figure-of-eight fashion, thus converting tensile forces over the anterior aspect of the knee joint into compression forces at the joint line. 4 An additional wire may be inserted as a cerclage around the patella for compression. Finally, retinaculum is repaired with sutures. However, this technique works best for simple transverse patella fractures; distal pole patella fractures or multifragmentary fractures may require alternative fixation methods 5 as the distal pole fragment or posterior cortex of the comminuted fracture may not be intact to allow compression. To fix distal pole patella fractures, three axial a transosseous tunnels are created, and a transosseous suturing technique employing nonabsorbable sutures may be used. Nevertheless, be it simple transverse fractures, distal pole fractures, or comminuted fractures, complications from traditional fixation methods such as wire breakage from fatigue, migration or loosening of wires, skin impingement or even skin penetration from wires may still occur. 6,7,8 Incorrect positioning of cerclage or undertightening of wires may also lead to early postoperative fracture displacement and loss of reduction. In addition, with metallic wires, patient might also experience metal irritation to the surrounding soft tissue. 9 In one study, reoperation rate arising from complications for patients treated with metallic wiring alone was over 40%. 10
At our center, we have revised and changed the surgical procedure by not only changing the order of retinaculum repair but also utilized high-tensile strength sutures instead of metallic wires. While traditional fixation method with metal wires uses only one wire for figure-of-eight fixation, this technique uses two FiberTape sutures that rest parallel, yet offset from each other, in a figure-of-eight fashion on the surface of the patella. By doing so, we minimize aforementioned complications arising from a century-old technique, while at the same time provide an alternative method of treatment even for fractures with complicated fracture patterns. Ultimately, none of the patients in this study required revision surgery.
Methods
We propose to use a high-tensile strength braided tape-shaped polyblend suture fix a reduced patella fracture. In our center, 2 mm FiberTape by Arthrex® (Naples, Florida, USA) was utilized. All our patients underwent either general or spinal anesthesia in a supine position. A tourniquet was also placed in upper thigh during the procedure. Using an anterior midline approach, an incision around 1–2 cm longer than the longitudinal length of the patella was made. Upon exposure of the patella, the retinaculum at both sides of the patella was first repaired. Contrary to fixation using a transosseous suture, a FiberTape was tied to a strand of 2-0 Nylon suture with a large curved needle, which was subsequently passed through the patella and quadriceps tendon. This procedure was repeated for a second strand of FiberTape and they were each hand-tied in a figure-of-eight fashion as shown in Figure 1. By doing so, we ensure that the two parallel strands of FiberTapes rest closely on the surface of the bone, while at the same time, preventing the FiberTapes from cutting into the patella as we aim to distribute the stress evenly between the two strands. They were tightened sequentially for three times per strand to provide maximum tension. An additional Ethibond suture is added as a cerclage for additional stability. In this procedure, Kirschner wires were not required to temporarily hold the reduced fracture. Intraoperative X-ray screening was utilized to ensure compression of fracture even with 90° of knee flexion before wound closure (Figure 2).
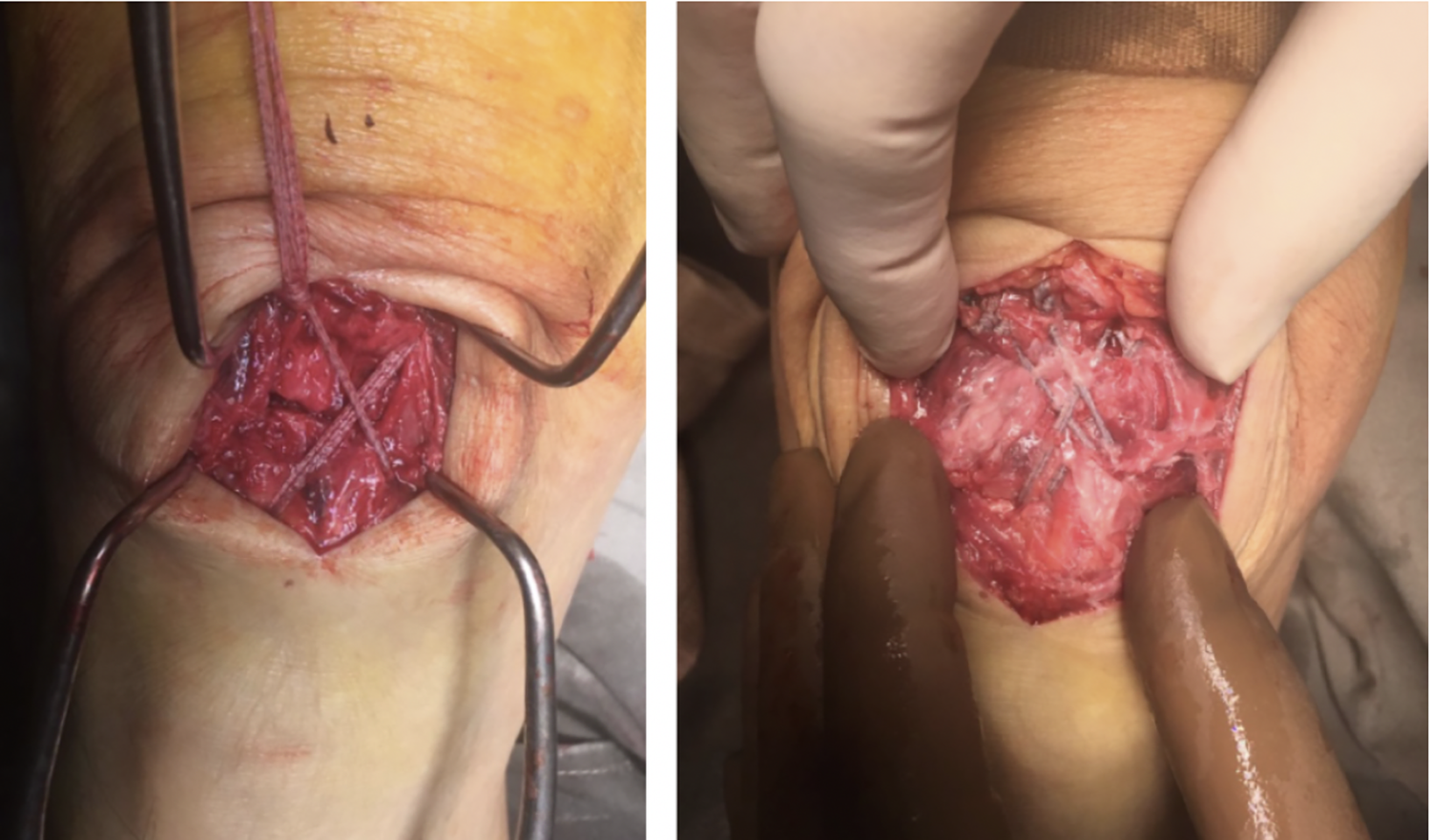
Demonstration of fiberTape alignment after fixation.
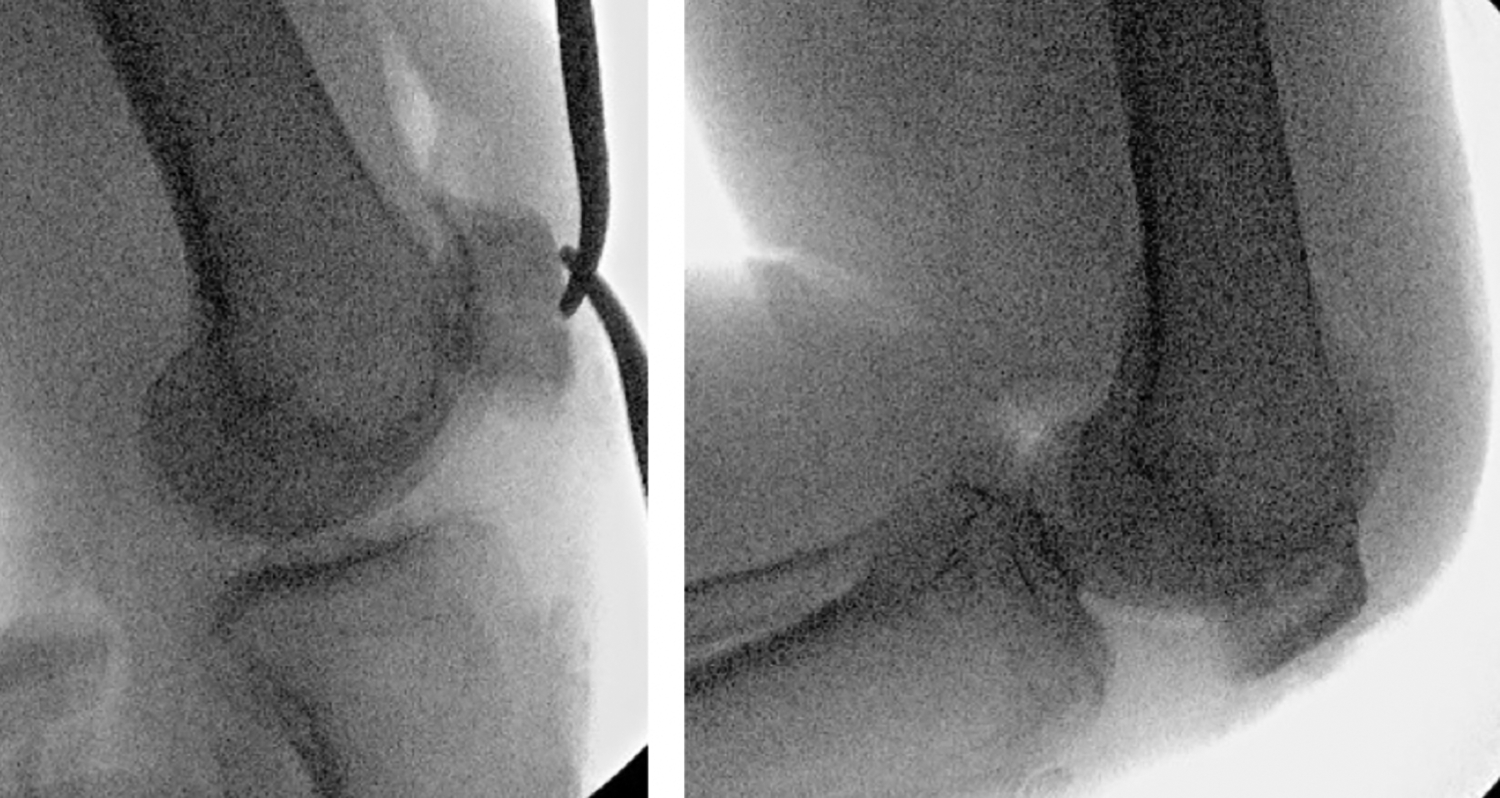
Intraoperative X-ray screening with knee flexion to confirm fracture stability postfixation.
Postoperatively, each patient was given an extension knee brace for wound resting for 2 weeks, before graduating to a hinge knee brace with 0–45° range for 2 weeks, then finally 0–90° range for two more weeks. The hinge knee braces were removed by postoperative 6 weeks. Overall, the postoperative rehabilitation protocol with the braces was the same as the one utilized for patients treated with traditional metallic tension band wires.
Between February 2014 and April 2018, 15 patients with patella fractures underwent this procedure. Early on, their surgeries were performed by a single senior surgeon, and they were subsequently performed or supervised by the same senior surgeon to ensure consistent surgical techniques. A patient’s knee range of motion (ROM) and healing status from follow-up X-rays were documented.
Results
Of the 15 patients, there were 9 male and 6 female patients. Average age for total patient group was 58.5 years old (49.1 years old for female group and 53.4 years old for male group). There were five simple transverse patella fractures, three distal pole fractures, and seven comminuted fractures. The overall mean operation time was 84.5 min, with a range of 49–117 min. The mean operation times for simple transverse patella fracture fixation, distal pole fracture fixation, and comminuted patella fracture fixation were 73.8, 81.3, and 86 min, respectively. Initial learning curve as well as cases of comminuted fractures requiring more meticulous fixation could account for the longer operation durations.
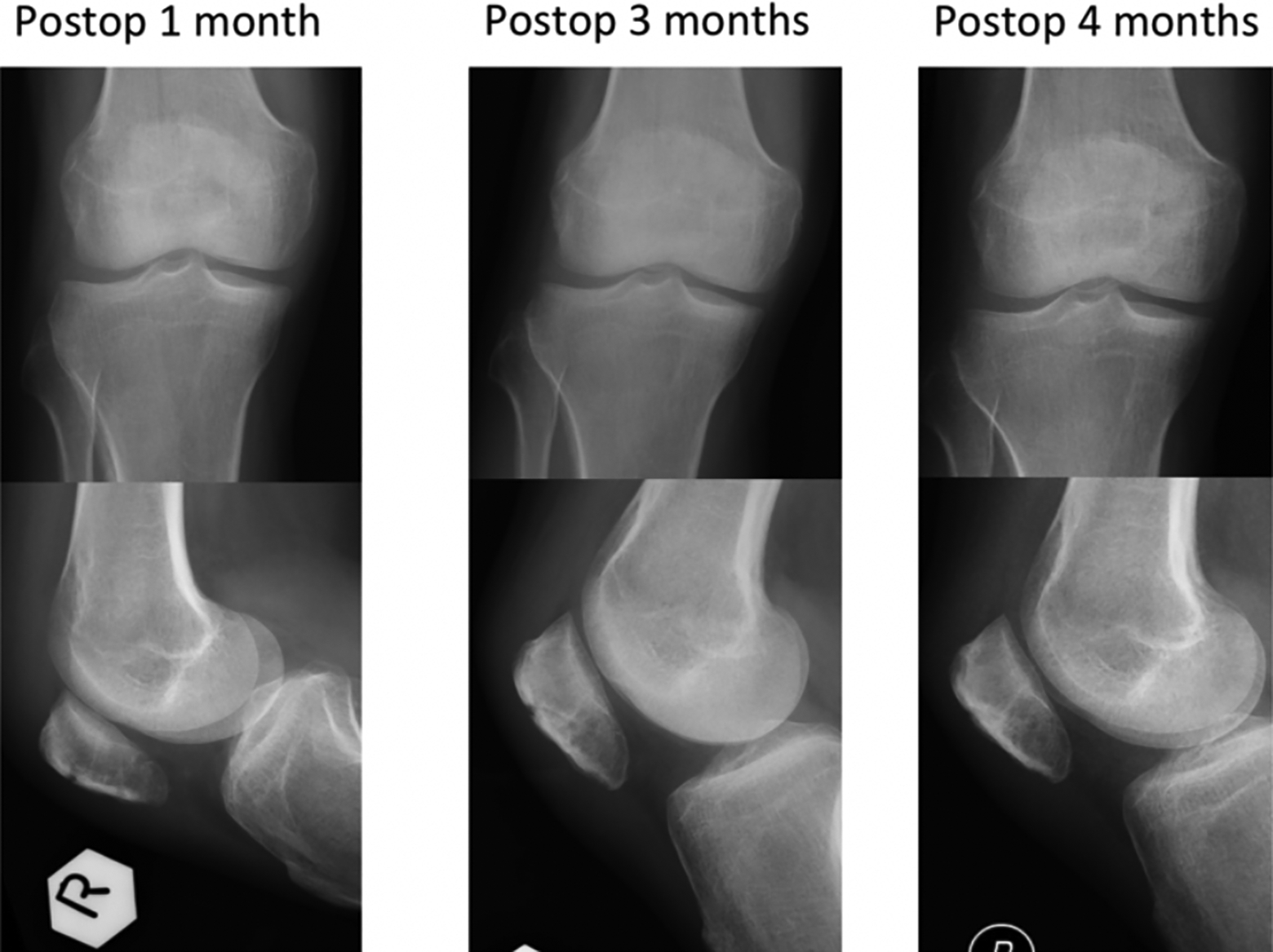
Eight patients were subsequently discharged from outpatient follow-ups within 1.5 years, with a mean follow-up period of 9.9 months. Six patients were still under our care as of September 2018, while one patient, who was also a known substance abuser, was defaulted follow-ups. Of the patients discharged, the mean knee range at their last follow-ups was 0–127.1°, while the mean overall knee range of all the patients (based on documented range at their latest follow-up) was 0–118.3°. All the patients that were discharged from follow-ups had healed fractures on their latest X-rays, examples of which could be appreciated in Figure 3. The overall average healing time based on follow-up X-rays was 2.9 months, while the healing times for simple transverse patella fractures, distal pole fractures, and comminuted fractures were 3, 1.7, and 3.3 months, respectively.
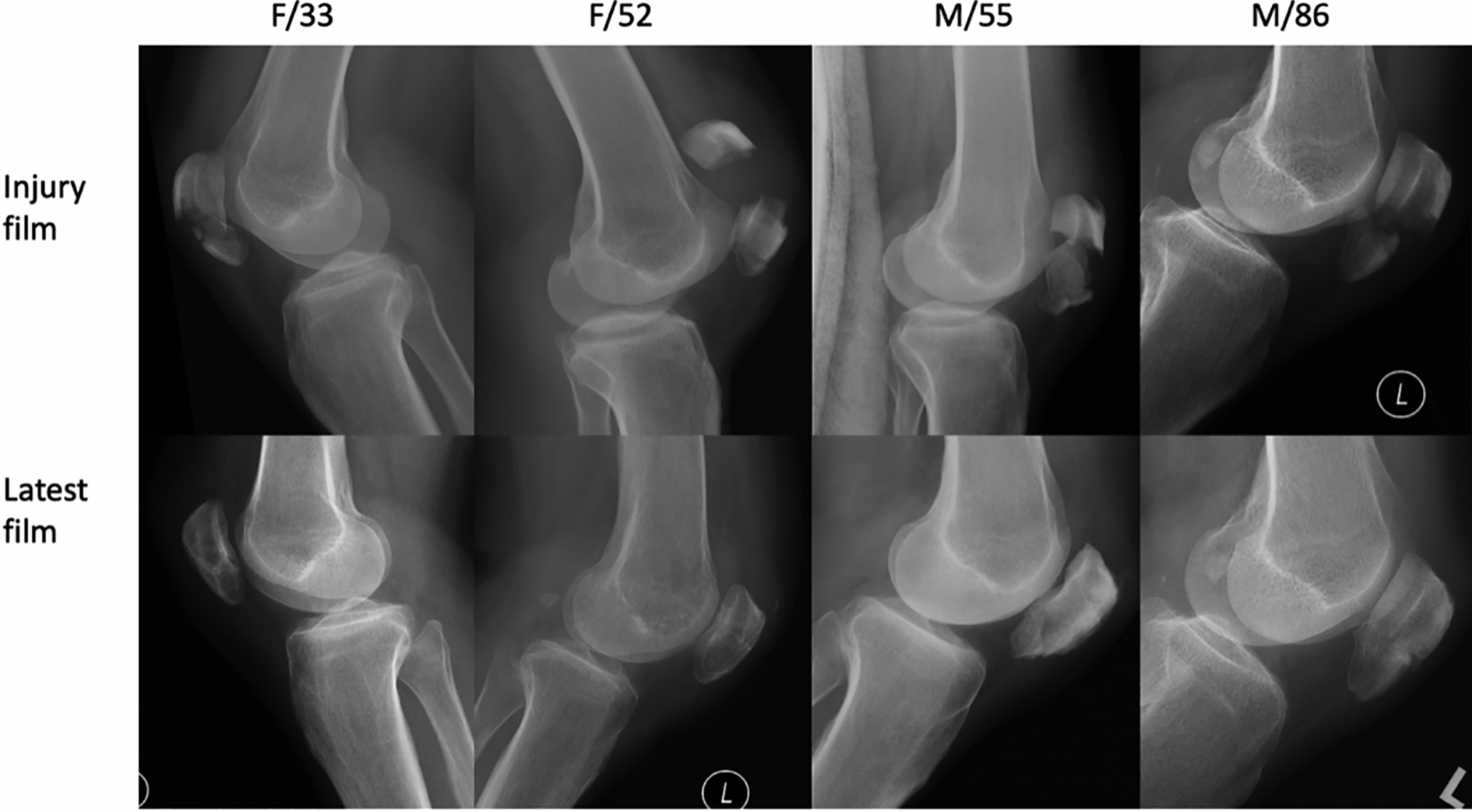
Examples of discharged patients comparing injury film and last film.
There was no wound complication noted in all the patients nor was there any knot impingement. One patient required manipulation under anesthesia (MUA) 14 months after initial surgery. During examination under spinal anesthesia, her knee range was noted to be normal, and it was surmised that her postoperative stiffness could be due to pain or reluctance to mobilize. Her knee range subsequently improved to 120° after MUA and she was discharged from long-term follow-up. There was also one patient with malunion due to poor compliance to rehabilitation protocols. None of the patients required revision surgery or elective removal of implant.
Discussion
A braided tape-shaped polyblend suture was used in place of traditional steel wires due to their high-tensile strength, while at the same time, foregoing the disadvantages of steel wires. 11 The tensile strength of FiberTape by Arthrex® was greater than 540 N compared to 494 N of 18-gauge steel wires. 12,13 The diameter of an 18-gauge steel is 1.02 mm, while the width of FiberTape is 2 mm. Previous studies revealed the pull through force of FiberTape was roughly 189 N during testing with cadaveric infraspinatus and subscapularis tendons, and mode of failure was due to suture pull through. 14
Contrary to traditional fixation method, our surgical technique involves repairing the retinaculum on both sides of patella prior to fixation. Not only does this prevent bone loss, it also optimizes the configuration of bony fragments before application of the FiberTape, thus allowing for easier and more precise fixation. In addition, as our technique does not require insertion of K wires or reduction forceps, a smaller wound that is just adequate for retinaculum repair can be created, thus minimizing postoperative wound pain for the patient. In our study group, we noted that a wound just 1 cm longer than the longitudinal length of the patella is sufficient for the procedure. The concept of prefixation retinaculum repair and its benefits can be illustrated particularly in cases of comminuted patella fractures. In the case of a 36-year-old patient admitted after a road traffic accident, preoperative computed tomography scan (Figure 4) showed a severely comminuted displaced fracture pattern with at least six fragments along with multiple small satellite fragments. His operation lasted 75 min. After fixation and postoperative physiotherapy, he was discharged 4-month post-injury with a healed fracture on X-ray and good knee ROM (Figure 5).
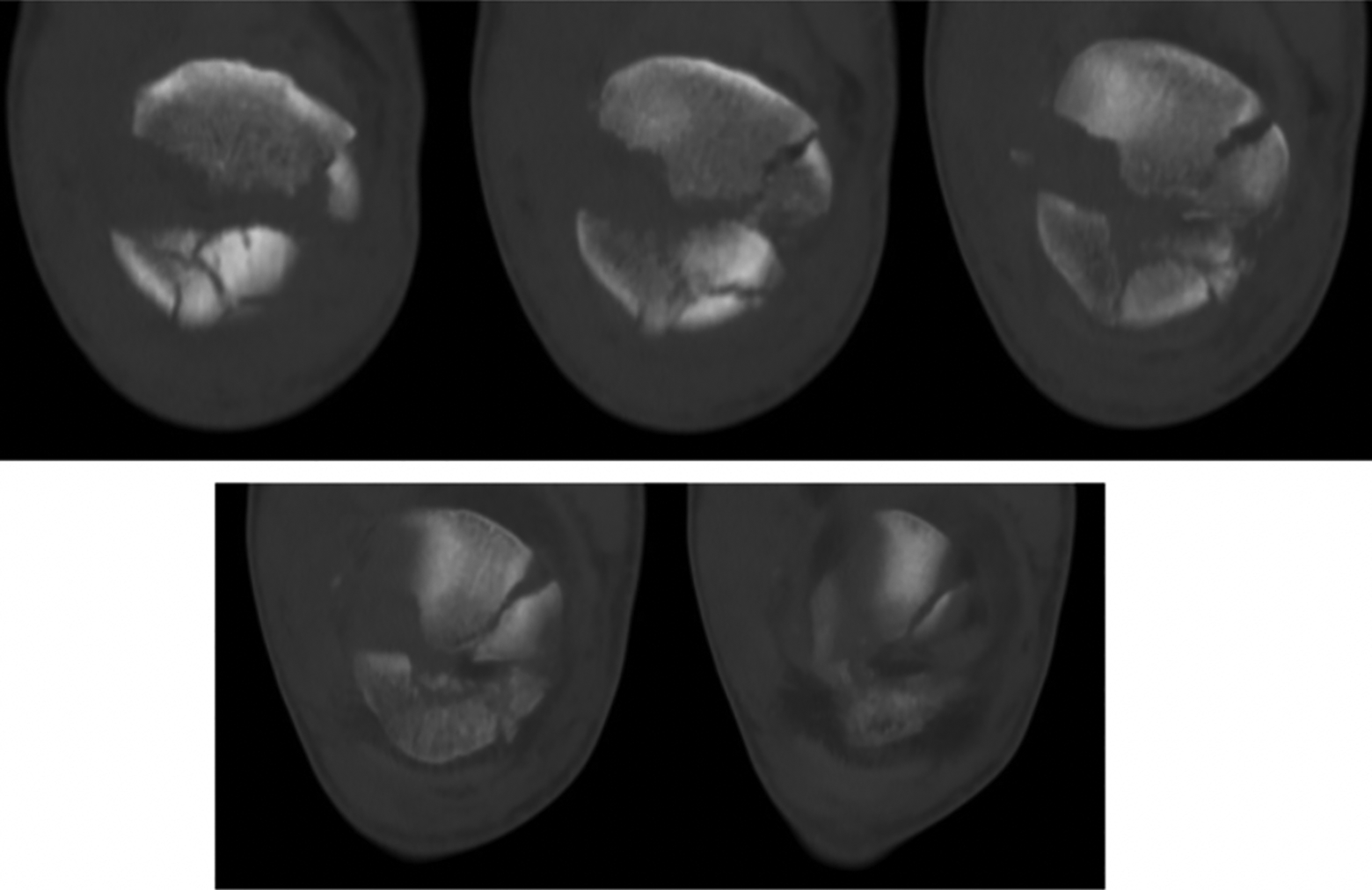
Preoperative CT scan of a 36-year-old patient with comminuted fracture right patella. CT: computed tomography.
Postoperative X-rays of patient with comminuted fracture.
The two strands of FiberTapes were sequentially laid over the anterior surface of the patella. With the application of two parallel and offset strands of FiberTape, maximum tension force could be evenly distributed over a wider surface area. By doing so, it prevents the sutures from cutting into bone. The utilization of FiberTape also allows for more precise placement of the sutures. Compared to passage of steel wires through patella and quadricep tendon using a cannulated needle, FiberTape was tied to the end of a strand of 2-0 Nylon suture with a large curved needle which was hand-guided through the respective tendons. This allows for easier manipulation and adjustment of the final position of the FiberTape.
Other advantages of this technique include the elimination of removal of implant due to skin impingement. As no patient experienced knot impingement, there are no foreseeable cases requiring “removal of implant” from the patient pool at this juncture. In addition, FiberTape does not display fatigability. This reduces the possibility of implant failure seen by breakage of metal wires.
Finally, contrary to fixation with metallic wires, this novel technique may be applied not just for simple or comminuted patella fractures but at the same time may be an effective fixation method for distal pole fractures. As mentioned before, our technique does not require transosseous suturing as seen in traditional methods of distal pole fracture fixations. In our study, the mean operation time for the three patients with distal pole fractures was 81.3 min, while the average healing time on X-rays on follow-ups was 1.7 months. The average knee ROM on their latest follow-up was 0–120°.
The tightness of the knot tied during fixation being a surgeon-dependent process may be a foreseeable disadvantage in this new technique. To not sacrifice the integrity of fixation, sequential tightening of the sutures (while maintaining position of knot with an artery forceps) is recommended to gain maximum strength, while ensuring that the suture is fitted on the patella.
A postoperative extension knee brace and hinge knee brace was given as a precaution. While some surgeons may choose to allow free range for a patient’s knee after fixation with a steel wire, the extension knee brace given in our protocol is crucial for wound resting and fracture healing. This was demonstrated in the patient with malunion as he immediately resumed free range after discharge from hospital. His fracture alignment was unable to be maintained on his first follow-up X-ray. Option of fixation revision was offered but he defaulted subsequent follow-ups and his condition could not be further assessed.
While patella fracture fixation using an “invisible” technique is not a novel entity, there exists little data regarding fixation using FiberTape as a nontransosseous fixation suture. In a similar design by Camarda et al., 15 their group used one strand of number 5 FiberWire nonabsorbable suture in the figure-of-eight fashion through the quadriceps and patella tendons, while another number 5 FiberWire as a circumferential cerclage. They also saved the order of retinaculum repair till after fracture fixation. According to their data, all 17 treated patients had a healed fracture by 3 months, with an average healing time of roughly 9.2 weeks. A slight loss of reduction (<4 mm) were also noted in two patients 4 weeks after surgery. One patient required MUA due to noncompliance to rehabilitation protocol, and the same patient required elective removal of the FiberWire due to a superficial infection, possibly due to implant-related soft tissue irritation. Our data might be similar in terms of healing time and one patient requiring MUA. However, our overall fracture fixation failure rate is lower when comparing these two techniques. Despite having one patient displaying malunion due to noncompliance to rehabilitation protocols, none of our other patients had loss of reduction postoperatively or had any wound complications requiring removal of implant. As number 5 FiberWire has a diameter of only 0.98 mm 13 compared to the width of 2 mm in FiberTape, one might surmise that having two strands of FiberTape provides a stronger construct when holding the reduced fracture in figure-of-eight fashion, thus contributing to the difference of having no additional patients experiencing loss of reduction in our study. More testing is required, however, to identify any differences in the rate of wound complications between FiberTape and FiberWire.
Despite having a small population pool, our results have shown that fixation with a high-tensile strength tape-shaped suture is an equally effective method of patella fracture fixation. With eliminated complications pertaining to fixation with steel wires, this novel technique may also minimize potential need for complication-related revision surgeries as seen with traditional tension band wiring. Even though data collection for this study ended in September 2018, this procedure is still performed at our center in the hopes that having a larger population sample may provide a more definitive conclusion in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.