
Abstract
Introduction:
Patella fractures managed by fixation with metal implants often cause local soft tissue irritation and necessitate implant removal. An alternative is to utilize suture-based fixation methods. We have adopted suture and hybrid fixation in the routine management of patella fractures. Here, we compare the results of 3 fixation techniques.
Materials and Methods:
Eighty-seven eligible patients underwent patella fracture fixation over a 3-year period. As determined by fracture configuration, patients received (1) suture fixation (transosseous sutures and figure-of-eight tension banding with FiberWire), (2) hybrid fixation (transosseous FiberWire sutures and metal tension banding), or (3) metal fixation. Primary outcome measures included reoperation rate and soft tissue irritation. Secondary outcomes included surgical complications, radiological, and functional parameters.
Results:
Reoperation rate was highest for metal fixation (25/57, 43.9%) and lowest for suture fixation (2/13, 15.4%). Soft tissue irritation necessitating implant removal was the predominant reason for reoperation and was significantly less prevalent following suture fixation (1/13, 7.7%, P < .01). Hybrid fixation resulted in similar rates of soft tissue irritation (6/17, 35.3%) and implant removal (7/17, 41.2%) as compared to metal fixation. There was a significant increase in patella baja (13/17, 76.5%) and reduction in Insall-Salvati ratio (0.742; 95% confidence interval: 0.682-0.802) following hybrid fixation as compared to the other 2 fixation methods (P < .05).
Discussion:
Suture fixation results in the least amount of soft tissue irritation and lowest reoperation rate, but these advantages are negated with the addition of a metal tension band wire. Hybrid fixation also unbalances the extensor mechanism.
Conclusion:
Patients should be counseled as to the expected sequelae of their fixation method. Suture fixation is the favored means to fix distal pole fractures of the patella. An additional metal tension band loop may confer additional stability but should be applied with caution.
Introduction
Patella fractures are common, accounting for 1% of skeletal injuries. 1 In the presence of significant fracture displacement and articular incongruity, open reduction and internal fixation is the standard of care to restore quadriceps function and prevent osteoarthritis. 2 Classically, the AO-technique for patella fixation utilizes axial K-wires in combination with anterior tension banding. 3 Screw fixation, both with and without tension banding for reinforcement, is another option. 4 As a result of utilizing metallic implants, patients commonly complain of soft tissue irritation over the knee. More than one-third of patients subsequently require secondary procedures for implant removal to provide symptomatic relief. 5
Alternative operative techniques have been developed to avoid these complications. Transosseous sutures have been applied in conjunction with suture-based anterior figure-of-eight cerclage. 6,7 Extraosseous suture fixation via circumferential cerclage in combination with anterior tension banding has also been described. 8 Under controlled conditions, these studies demonstrate a reduction in implant-related sequelae and similar functional outcomes as compared to traditional fixation methods.
In response to these findings, our trauma center has adopted suture-based techniques in the routine surgical management of patella fractures. As determined by fracture configuration and stability, we treat cases of displaced patella fractures by means of pure suture, hybrid, or metal fixation. Here, we review the results of 87 patella fractures managed operatively over a 3-year period. Our primary objective was to evaluate reoperation rates for the 3 fixation methods due to symptomatic hardware and otherwise. We also evaluated for surgical complications and radiological and functional outcomes after a minimum of 6 months of follow-up.
Materials and Methods
Inclusion and Exclusion Criteria
We identified a total of 134 cases of patella fractures operated on at our trauma center for the 3-year period spanning from January 2014 to December 2016. A total of 87 patients were eligible for analysis, while 47 patients were excluded (Figure 1). Twenty-one patients were lost to follow-up prior to 6 months. Twelve patients underwent fixation in a manner other than the 3 methods described. Five cases of open fracture and 3 cases of polytrauma were excluded. Two cases had preexisting limb deformity and were excluded. Two cases had prior orthopedic procedures performed on the affected limb and were excluded. One patient was excluded due to inflammatory arthropathy and another due to delayed surgery following initial refusal of operative intervention.
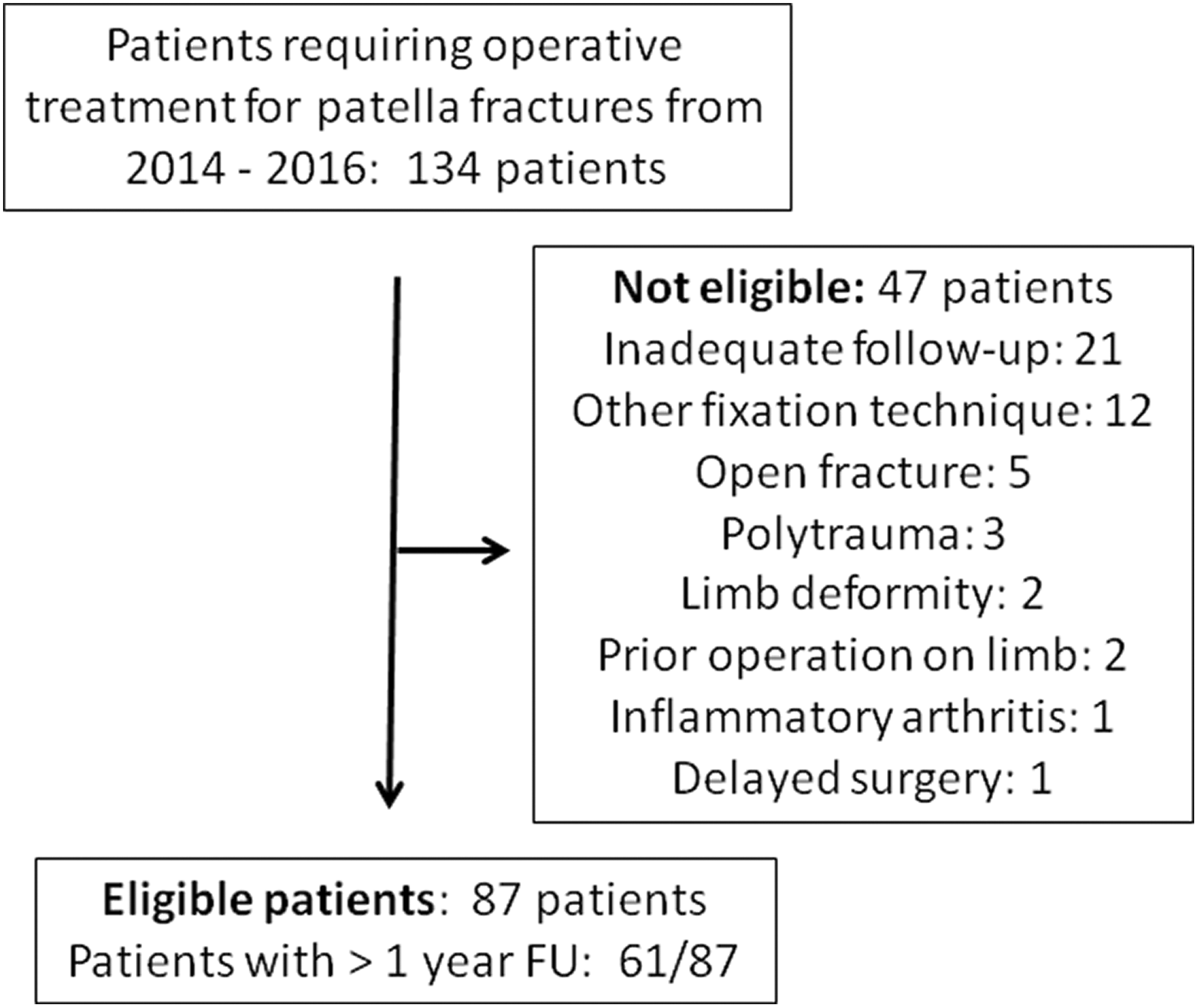
Patient eligibility and exclusion.
Patient Demographics
Of the 87 eligible patients (Table 1), there were 32 males and 55 females with an average age of 60.0 ± 15.4 years (10-89 years). A total of 13, 17, and 57 patients received fixation by means of suture, hybrid, and metal fixation, respectively. Slip and fall injury on level ground was the most common mechanism of injury, accounting for 10 (76.9%) of 13, 17 (100%) of 17, and 53 (93.0%) of 57 of patients receiving suture, hybrid, and metal fixation, respectively. A total of 9 (10.3%) of 87 patients sustained their injury while on duty. Average operation time was approximately 60 minutes and did not demonstrate statistically significant differences between groups (P = .414). A follow-up period of 12 months or more was attained in 61 (70.1%) of 87 patients and for 9 (69.2%) of 13, 11 (64.7%) of 17, and 41 (71.9%) of 57 patients receiving fixation by means of suture, hybrid, and metal fixation, respectively.
Patient Demographics.

Abbreviations: F, female; IOD, injured on duty; M, male; OT time, operation time; SD, standard deviation.
Determination of Fixation Method
Decision in regard to fixation method of the fractured patella was determined intraoperatively by the surgeon based on its configuration. Distal pole fractures were managed with pure suture fixation using transosseous sutures supplemented by a figure-of-eight anterior tension band suture, while those considered to require further stability received hybrid fixation with rigid metal tension banding to prevent anterior displacement of fracture fragments in addition to transosseous sutures. Transverse and comminuted intraarticular fractures were treated by metal fixation. For the former, we utilized the AO-technique of axial K-wires in combination with anterior tension banding. Implant configuration in the latter often necessitated additional augmentation to achieve stability as described below.
Surgical Technique
Cases were operated upon by a fellowship-trained trauma surgeon (6 surgeons) or by a senior resident under supervision. An anterior midline approach to the patella was adopted with exposure from the superior pole down to the patella tendon. Reduction was achieved with the aid of bone clips, clamps, and temporary intraosseous K-wires. For suture-based fixation (Figure 2A), 2 loops of 2-FiberWire were anchored to the patella tendon substance distally in the Krakow configuration, resulting in 4 suture limbs. Three axial transosseous tunnels spanning the proximal fracture fragment were created using 1.6-mm K-wires. A needle passer was inserted through the tunnels from proximal to distal to retrieve the suture limbs; central sutures from both loops were passed through the middle tunnel. After fracture reduction, sutures were tied over the superior pole. For pure suture fixation, 2-FiberWire was passed beneath the quadriceps insertion proximally and patella tendon distally and tightened over the anterior patella surface in a figure-of-eight configuration. For cases of hybrid fixation, 1.25-mm metal cerclage wire was utilized for the figure-of-eight anterior tension band (Figure 2B). For metal fixation of simple transverse patella fractures, two 1.6-mm transosseous axial K-wires were reinforced with 1.25 mm cerclage wire in a figure-of-eight anterior tension band configuration (Figure 2C). Comminuted fractures necessitated additional transosseous K-wires to secure individual fragments and/or circumferential cerclage wiring. Subsequent to fracture fixation, stability was noted throughout the range of passive knee motion. Torn extensor retinaculum was repaired, followed by closure of the subcutaneous and skin layers.

Schematic representation of 3 fixation techniques. A, Suture fixation. FiberWire (blue) was sutured to the patella tendon in a Krakow configuration and passed proximally through transosseous bone tunnel (dotted lines) and secured over the superior patella pole. An anterior FiberWire figure-of-eight tension band provided further reinforcement. B, Hybrid fixation. Transosseous FiberWires were reinforced by a metal-of-eight anterior tension band (silver). C, Metal fixation. Axial K-wire were reinforced with metal figure-of-eight anterior tension band. Complex fracture patterns necessitated additional intraosseous K-wire together with circumferential metal cerclage to ensure stability.
Postoperative Care and Follow-Up
Postoperative radiographs were taken the day after surgery. Patients were given a hinged knee brace as protection postoperatively and allowed to weight bear. In general, 0° to 90° of flexion in-brace was allowed for the first 6 weeks postoperatively. Patients were discharged after attaining sufficient independence in ambulation and toileting and given their first follow-up appointment at 2 weeks postoperatively for wound inspection. Patients were followed up every 4 to 6 weeks to monitor for functional return and clinical/radiological fracture union (Figure 3) and thereafter assessed at 3- to 6-month intervals.
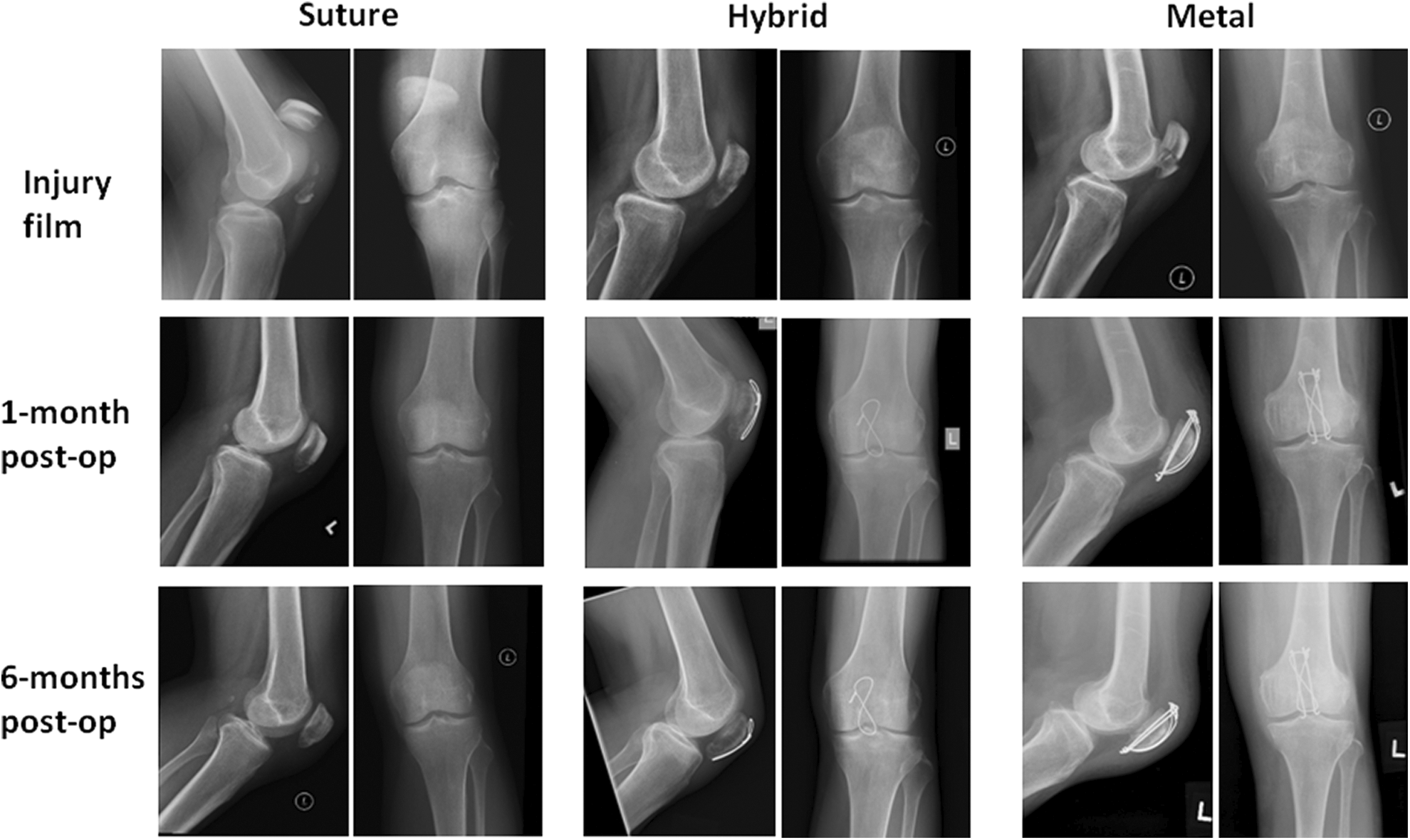
Radiographs of fixation techniques.
Outcomes Measures
The primary outcomes of this study were the reoperation rates for the 3 fixation methods and the prevalence of symptomatic hardware causing soft tissue irritation. Secondary outcomes included surgical complications (fixation failure/displacement, implant breakage/dislodgement, nonunion, infection), radiological parameters (patella baja, Insall-Salvati ratio), and knee function (return to premorbid walking status, knee range of motion). Fracture displacement was defined as an opening up of the fracture gap ≥ 3 mm compared to immediate postoperative radiographs. Nonunion was defined as failure to achieve radiological bony union at 6 months’ time. Reoperation for elective implant removal included patients scheduled for but yet to receive their surgery. Patella height was calculated by measuring the Insall-Salvati ratio of most recent lateral knee X-rays, with a value <0.8 taken as the criterion for patella baja.
Statistical Testing
Fisher exact test (1-tailed) was utilized to analyze categorical outcomes and single-factor analysis of variance for comparison of parametric outcomes (Insall-Salvati ratio, knee range of motion). Subgroup analysis was performed using 1-tailed Fisher exact test and 1-tailed t test for categorical and parametric data, respectively. Statistical significance was determined at a P value of <.05, and at P < .0167 for subgroup analysis following the Bonferroni correction.
Results
Patella Fracture Classification
A summary of the fracture configurations encountered for each fixation method according to the Speck and Regazzoni classification 9 is shown in Table 2. Simple distal pole fractures (B1) accounted for 4 of 13 and 9 of 17 of patella fractures receiving suture and hybrid fixation, respectively, while comminuted distal pole fractures (C3) accounted for 9 of 13 and 8 of 17 among the 2 groups. Comminuted intraarticular fractures (C3; 27/57) and simple transverse fractures (B2; 20/57) accounted for the majority of fractures receiving metal fixation. For cases receiving suture fixation, we observed a higher reoperation rate of 1 (25%) of 4 in simple distal pole fractures as compared to 1 (11.1%) of 9 for comminuted distal pole fractures (Table 2). Conversely, in hybrid and metal fixation methods, we observed a higher reoperation rate for comminuted fracture subtypes as compared to other configurations, accounting for 4 (50%) of 8 and 14 (51.9%) of 27 of patients, respectively. Statistical analysis failed to demonstrate a significant correlation between fracture configuration and reoperation rate (P = .538, suture fixation; P = .419, hybrid fixation; P = .529, metal fixation). Comparison of overall reoperation rate in comminuted (15/41, 36.6%) as compared to simple fracture configurations (19/46, 41.3%) across fixation methods failed to reach statistical significance (P = .409).
Patella Fracture Classification (Speck and Regazzoni). 9

Reoperation Rate and Soft Tissue Irritation
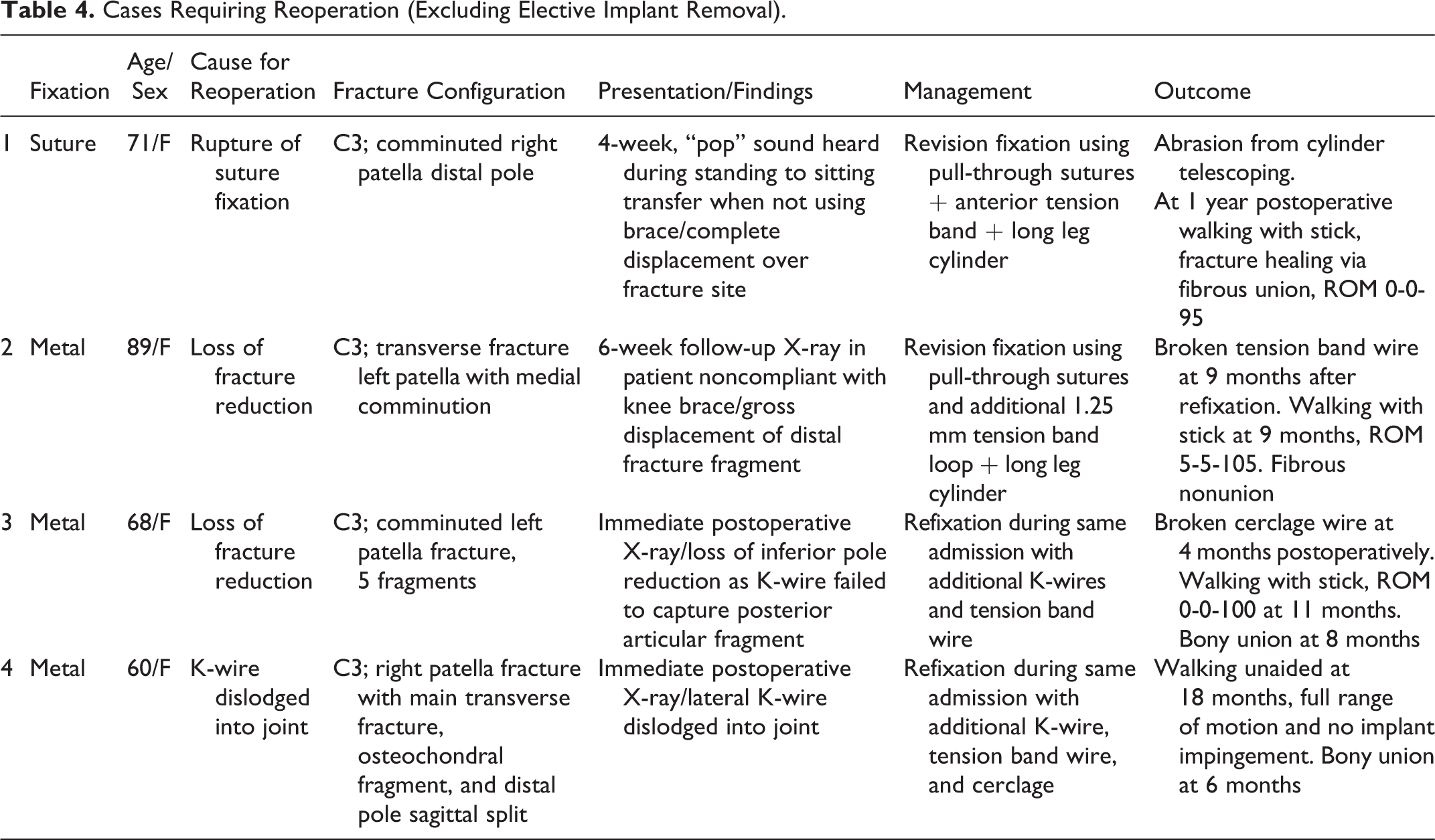
Overall, 34 (39.1%) of 87 of patients received reoperations after initial fracture fixation (Table 3). Reoperation rates were lowest following suture fixation (2/13, 15.4%), followed by hybrid (7/17, 41.2%) and metal fixation (25/57, 43.8%), without discernible statistical difference (P = .165). Elective implant removal was the predominant cause for reoperation and was arranged for 1 (7.7%) of 13, 7 (41.2%) of 17, and 22 (38.6%) of 57 of patients receiving suture, hybrid, and metal fixation, respectively, and differences failed to reach statistical significance (P = .0786). In the suture fixation subgroup, the second case of reoperation was resultant from suture rupture and fracture displacement necessitating refixation. The 3 cases of reoperation from other causes among the metal subgroup were due to gross loss of fracture fixation in the immediate and delayed postoperative period, as well as a dislodged K-wire noted following immediate postoperative X-rays. A summary of the details regarding the cases of reoperations excluding those that were scheduled for elective implant removal is listed in Table 4.
Surgical Outcomes.
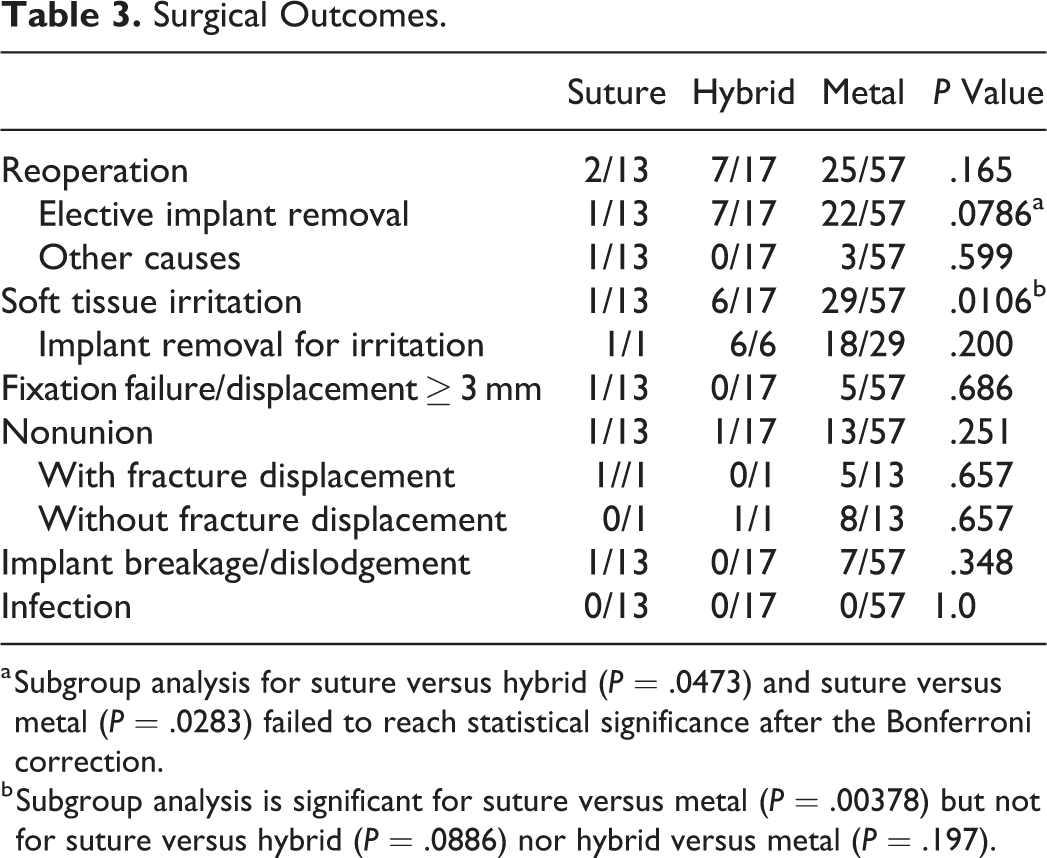
a Subgroup analysis for suture versus hybrid (P = .0473) and suture versus metal (P = .0283) failed to reach statistical significance after the Bonferroni correction.
b Subgroup analysis is significant for suture versus metal (P = .00378) but not for suture versus hybrid (P = .0886) nor hybrid versus metal (P = .197).
Cases Requiring Reoperation (Excluding Elective Implant Removal).
Implant-related soft tissue irritation was reported in 1 (7.7%) of 13, 6 (35.2%) of 17, and 29 (50.8%) of 57 patients receiving suture, hybrid, and metal fixation, respectively. Statistical significance was demonstrable upon comparison of the 3 groups (P = .0106), with subgroup analysis identifying that soft tissue irritation was specifically reduced in suture versus metal fixation (P = .00378). Implant removal was requested for all cases of suture (1/1) and hybrid fixation (6/6) with soft tissue irritation, with the source of impingement being from a prominent FiberWire knot in the suture subgroup. In contrary, only 18 (62.1%) of 29 of patients receiving metal fixation with subsequent soft tissue irritation decided for implant removal. To account for the total of 7 patients with implant removal in the hybrid fixation subgroup, an additional asymptomatic patient requested removal. To account for the 22 patients with elective implant removal among the metal fixation subgroup, 2 patients were asymptomatic and requested removal. Another 2 patients were noted to have K-wire dislodgement subsequent to fracture healing upon follow-up X-rays and agreed for implant removal.
Other Surgical Outcomes
A total of 1 (7.7%) of 13, 0 of 17, and 5 (8.7%) of 57 of patients receiving suture, hybrid, and metal fixation, respectively (Table 3) demonstrated gross fixation failure (details in Table 4) or significant fracture displacement, with no statistically significant difference between groups (P = .686). Nonunion was demonstrated in 1 (7.7%) of 13, 1 (5.9%) of 17, and 13 (22.8%) of 57 of patients receiving suture, hybrid, and metal fixation, respectively. All 5 patients in the metal subgroup with fixation failure/displacement concomitantly had nonunion. The cases of nonunion among suture and hybrid subgroups resulted from a failure to maintain anatomical reduction. There was no statistical difference between fixation methods for fixation failure/displacement (P = .686) or nonunion (P = .251).
Implant breakage and dislodgement was encountered in 1 (7.7%) of 13, 0 of 17, and 7 (12.2%) of 57 patients receiving suture, hybrid, and metal fixation, respectively. For the suture subgroup, this occurred as a result of FiberWire rupture during sitting to standing transfer. Among the metal fixation subgroup, 3 patients had broken cerclage wiring, 2 patients had backing out of axial K-wires, 1 patient had dislodgement of an axial K-wire into the joint, and 1 had a broken figure-of-eight anterior tension band wiring. Differences between the 3 treatment subgroups failed to reach statistical significance (P = .348). There were no cases of infection among our patient population.
Radiological and Functional Outcomes
A total of 4 (30.8%) of 13, 13 (76.5%) of 17, and 25 (43.9%) of 57 of patients receiving suture, hybrid, and metal fixation, respectively (Table 5), demonstrated patella baja, with statistical significance demonstrable between groups (P = .0234). Subgroup analysis specifically revealed a significant increase in the number of cases with patella baja following hybrid fixation as compared to suture fixation (P = .0159). Similarly, difference in patella height as measured by the Insall-Salvati ratio (Figure 4) demonstrated statistical significance (P = .0154). Subgroup analysis was significant (P = .00351) for a reduction in patella height in hybrid (0.742; 95% confidence interval [CI]: 0.682-0.802) as compared to suture fixation (0.882; 95% CI: 0.802-0.962) and significant (P = .00949) between hybrid and metal fixation (0.830; 95% CI: 0.795-0.866).
Radiological and Functional Outcomes.

Abbreviation: CI, confidence interval.
a Subgroup analysis was significant for suture versus hybrid (P = .0159) but not for hybrid versus metal (P = .0173) nor suture versus metal (P = .294) after the Bonferroni correction.
b Subgroup analysis was significant for suture versus hybrid (P = .00351) and hybrid versus metal (P = .00949) but not for suture versus metal (P = .113).

Insall-Salvati ratio. Comparison of Insall-Salvati ratio from 3 fixation methods. Error bars = mean ± SEM. **P < .01.
Functional outcome was assessed by means of walking status and knee range of motion upon final follow-up. Return to premorbid walking status was achieved in 12 (100%) of 12, 14 (86.5%) of 16, and 43 (78.2%) of 55 of patients receiving suture, hybrid, and metal fixation, respectively (P = .166). One patient each was excluded from analysis among the suture and hybrid groups because of unknown premorbid walking status, and 2 excluded from the metal fixation group due to insufficient documentation in regard to their postoperative progress. There was no difference in the number of patients with extension lag ≥10° (0/12, 3/16, 3/51; P = .172) between the 3 groups, nor in the average angular deficit from full extension (P = .151). Similarly, differences between treatment groups were insignificant with regard to patients with flexion range ≤90° (0/12, 0/16, 2/51; P = .999) and in the average passive flexion range (P = .749). Due to incomplete documentation of knee range of motion, one patient each from the suture and hybrid groups as well as 6 patients from the metal fixation group was excluded from analyses.
Discussion
This study describes the single largest cohort of patients receiving operative intervention for patella fractures as well as suture-based fixation methods. Prior related studies are limited by small sample sizes 8 and standardized to individual surgeons. 6,7 In applying suture-based fixation across our institution, we substantiate the advantages of pure suture fixation. Specifically, in the management of distal pole fractures, we establish that utilization of hybrid fixation nullifies the benefits of pure suture fixation in preventing implant-related complications while significantly reducing patella height.
Implant-related soft tissue irritation resulting in anterior knee pain and subsequent need for implant removal is the most common complication following metal fixation. The prevalence of such sequelae should be discussed with patients in order to temper expectations. Meta-analysis with regard to surgical management of transverse patella fractures 1 demonstrates that in general, 25% to 42% of patients receiving metal fixation experienced suboptimal results and postoperative pain/irritation. Following on, counts of hardware removal were reported to range from 5% to 100%. The study with the lowest reported rate of irritation and subsequent implant removal utilized a cannulated screw and cable construct, which was demonstrated to be superior to the traditional modified tension band technique. 4 Alternatively, utilization of suture-based techniques also results in a marked reduction in soft tissue irritation 10 and lessens the need for reoperation. 7 Fixation with biodegradable materials is another approach, but not as widely available or feasible. 11 The reduced incidence of soft tissue irritation was apparent in this work upon comparison of suture and metal fixation groups. Surprisingly, incidence of soft tissue irritation in the hybrid subgroup approached that of the metal subgroup and was more than 4-fold that observed in patients receiving suture fixation alone. From our observation, the source of irritation in patients with metal hardware is often from the prominent terminal wire loop originating from the anterior tension band, which we fail to avoid when utilizing the hybrid fixation technique.
Our overall incidence of nonunion at 6 months among patients receiving metal fixation (13/57; 22.8%) was elevated as compared to rates reported in existing literature. 12 Likely contributory factors in our cohort included the significant number of comminuted fractures (27/57; 47.4%), together with our criterion of achieving radiological bony union at 6 months despite many cases being asymptomatic with good function likely resultant from fibrous union having been achieved within this period of time. Incidence of nonunion and fixation failure among patients receiving suture and hybrid-based fixation was lower as compared to patients receiving metal fixation. In congruency with our rationale of using a metal tension band wire to confer additional stability, none of the cases receiving hybrid fixation had gross failure or significant displacement. Nevertheless, excellent rates of union and maintenance of reduction have been described following pure suture fixation, with a mean time to union of 9 weeks. 13 Biomechanically, FiberWire has been demonstrated to have a higher load to failure than stainless steel. 14
Concerning fractures of the distal pole, suture-based techniques avoid the complications associated with partial patellectomy in relation to affecting patella height and impairing knee biomechanics. 7 However, we found a significant decrease in patella height following hybrid fixation. We hypothesize that a reduction in patella tendon length and excursion resulting from the use of locking sutures over the tendon substance, together with the metal tension band cutting through the quadriceps muscle substance to cause elongation and weakening, served to unbalance the extensor mechanism. Following metal fixation, intraosseous axial K-wires may impede progressive anterior translation of the tension band wire but are absent in the hybrid fixation construct.
An obvious limitation of our study is in the heterogeneity of fracture configurations. Results should not be interpreted as a direct comparison between 3 different surgical options, as we have predominantly utilized suture-based techniques for tackling distal pole fractures and metal fixation for intraarticular fractures. The comparatively small numbers of fractures receiving suture and hybrid fixation likely contributed to the study being underpowered. Judicious trends in outcomes such as reduced reoperation rates for implant removal in suture compared to metal fixation (P = .0283) as well as suture compared to hybrid fixation (P = .0473) failed to reach statistical significance after the Bonferroni correction and therefore should be interpreted with caution. Our study is lacking in detailed functional evaluation and patient-related outcome measures, as well as in a rehabilitation protocol to guide bracing requirements postoperatively.
Conclusion
In summary, all means of fixation achieved acceptable outcomes. Our results allow us to counsel patients and manage their expectations on the prevalence of soft tissue irritation and reoperation with respect to fixation method. Concerning clinical decision-making, our study encourages pure suture as opposed to hybrid fixation for patella fractures involving the distal pole. Although a supporting metal tension band loop in addition to transosseous sutures may confer additional stability, this technique should be utilized with caution as incidence of soft tissue impingement and reoperation is elevated. Further assessment and follow-up is required to determine whether the significant reduction in patella height consequent to hybrid fixation results in functional impairment and early osteoarthritis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.