
Abstract
Purpose:
Tension band wiring technique has been widely used for treating patellar fracture. Conventional techniques are associated with some complications and several modifications have been introduced to increase stabilization. The purpose of this study was to compare two different fixation techniques, the one-end and both-ends Kirschner wire bending fixation methods.
Methods:
We retrospectively reviewed patient data from 2013 to 2017, including the age, sex, body height, body weight, BMI, lesion of injury, trauma mechanism, fracture displacement and classification, type of fixation, fracture healing duration, length of follow-up, clinical results and complications. The surgical outcome was assessed using the pain score (VAS), Lysholm knee score, and knee joint ROM. Plain radiographs were used to evaluate radiographic outcomes and assess the fracture union duration and hardware complications. We performed statistical analysis to compare these two different fixation techniques.
Results:
There were no significant differences between the two groups in terms of demographic data, fracture healing duration, level of the K-wires, distance between the K-wires, or length of the K-wires over the patella length (all p > 0.05). There were significant differences in the VAS score, K-wire migration, flexion degree, ROM, and Lysholm score (all p < 0.001) between the two different fixation methods.
Conclusion:
The both-ends K-wire bending fixation method has a lower complication rate and results in a better clinical outcome than the one-end K-wire bending fixation method. This revised technique can effectively control both ends of the K-wires, thus eliminating the possibility of K-wire migration and improving the fixation stability.
Introduction
Patella fractures comprise 1% of all fractures encountered in the emergency department. When fracture fragments are displaced due to traction of the quadriceps femoris, surgical treatment is always necessary. Open reduction and internal fixation (ORIF) is indicated for fractures with displacements greater than 3 mm, an articular incongruity of 2 mm or more, or a disrupted extensor mechanism. 1 There are various methods for treating a patellar fracture, and the tension band wiring (TBW) technique has been widely used. This technique involves longitudinal Kirschner wires (K-wires) and steel wire in a figure-of-eight pattern looped over the anterior patella, converting the anterior tension forces produced by the extensor mechanism and knee flexion into compression forces at the articular surface. 2 The TBW technique provides rigid fixation and allows early mobilization, ensuring that fixation failure of patellar fractures is rare. 3,4 However, the use of the TBW technique is associated with some complications, including wire breakage and migration, postoperative loss of reduction (22–45%), 3,5 and a high rate of symptomatic implant irritation (8–48%), 6,7 with reported rates of subsequent implant removal for symptomatic hardware ranging from 10–55%. 3,5,7 Several modifications have been introduced to increase stabilization in the TBW technique, along with other techniques. Wu et al. reported a revised technique that consisted of bending of both ends of the K-wires to prevent dislodging, further improving the success rate. 8 The purpose of this retrospective study was to compare the clinical and radiographic results between patients with patella fractures who underwent TBW using two different fixation methods, the one-end and both-ends K-wire bending fixation methods.
Materials and methods
Patient characteristics
This was a retrospective cohort study of consecutive patients who underwent fixation of a patellar fracture at our institution between July 2013 and January 2017. The inclusion criteria were as follows: patients with a closed transverse fracture of the patella with a fracture fragment separation >3 mm or an articular incongruity ≥2 mm, AO/Orthopaedic Trauma Association (OTA) 34-C1 and AO/OTA 34-C2 fractures, and surgical fixation using the modified TBW technique. The exclusion criteria were an age <18 years, AO/OTA 34-C3 fractures, multiple or open fractures, avulsion fractures, periprosthetic fractures, other surgical fixations (i.e., cannulated screws, tension bands through cannulated screws, a combination of circumferential wiring, suture fixation with non-absorbable polyester, and the use of an artificial bone graft), revision surgery, and patients who were followed-up for fewer than 3 months. Using a retrospective cohort study design, patients were divided into two cohorts: a one-end K-wire bending fixation group and a both-ends K-wire bending fixation group. An Institutional Review Board approved the study (IRB protocol number 201700394B0), with a date of approval of December 11, 2017.
Surgical procedures
All patients received a single dose of a first-generation cephalosporin antibiotic for antimicrobial prophylaxis within 60 minutes of incision. Under general or spinal anesthesia, patients were placed on the operating table in the supine position with a pneumatic tourniquet inflated to 300 mmHg. A longitudinal midline skin incision was made. The intra-articular hematoma from the knee joint was drained and the blood clot and soft tissue from the fracture site were removed. The fracture surface was refreshed and the fragments reduced with a clamp. A lateral patellar arthrotomy was made, and the articular surface of the patella was palpated to maintain reduction. Two 2-mm K-wires (Mizuho, Tokyo, Japan) were inserted in parallel from the proximal pole to the distal pole of the patella while bending the knee. The distance between them was 10–20 mm, and both had to be prevented from penetrating through the articular surface. A cerclage wire (Zimmer, Warsaw, IN, USA) of 1.2-mm in diameter was threaded through both ends of the two K-wires to form a figure-of-eight tension band at the anterior side of the patella. With full extension of the knee, the cerclage wire was tightened. In the one-end K-wire bending group, the upper ends of the K-wires were bent into hooks past 90° and the ends of the K-wires were cut. Finally, the lower ends of the K-wires were cut and the upper ends were reversed by 180° to face downward and buried beneath the quadriceps tendon (Figure 1), then the wound was closed with drain insertion. In the both-ends K-wire bending group, the procedure was the same as that for the one-end bending group, with the exception that both ends of the K-wires were bent into hooks at both poles of the patella. After cutting off the excess K-wires, both ends were reversed downward and buried in the quadriceps and patella tendon (Figure 2).

Tension band wire fixation with one end bending K-wire method. (a) and (b), Preoperative radiograph of a 50-year-old man who had a displaced transverse patella fracture. (c) and (d), Postoperative radiograph showing the proper placement of the wire and Kirschner wire in AP and lateral view.

Tension band wire fixation with both ends bending K-wire method. (a) and (b), Preoperative radiograph of a 63-year-old woman who had a displaced transverse patella fracture. (c) and (d), Postoperative radiograph showing the proper placement of the wire and Kirschner wire in AP and lateral view.
Postoperative management and evaluation
Postoperatively, intravenous antibiotics (cephalosporin) were given for 1 day. Patients in both groups were prescribed a similar postoperative rehabilitation program. An elastic bandage was used for 2 weeks after surgery to reduce hematoma of the knee and prevent deep vein thrombosis in all patients. Under supervision of physiotherapists, static quadriceps exercises, straight-leg raising, and progressive knee joint flexion were initiated as early as possible. Protected weight-bearing with crutches was advised until the fracture had healed. The knee was immobilized with splint protection until ambulation at around 6 weeks postoperatively depending on the degree of comminution and the surgeon’s decision. Patients were followed-up at the outpatient department until union of the fracture or until further surgical intervention was carried out. The results of clinical and radiographic evaluations were recorded. Medical charts of both groups were reviewed to obtain demographic information, including age, sex, body height, body weight, body mass index (BMI), history of diabetes mellitus, smoking status, American Society of Anesthesiologists (ASA) class, injury time, mechanism, and side of the lesion. Follow-up records included the duration of follow-up, pain score (VAS), knee joint range of motion (ROM), Lysholm knee score, complications, and the time of implant removal. The clinical data was assessed at the last outpatient department or the second surgery for removal of implant. Radiographic images (anteroposterior and lateral views of the knee) were studied to assess the initial fracture type, displacement, implant position, and healing duration. The Orthopedic Trauma Association (OTA) system was used to classify each fracture. Evaluation of the implant position included the level of the K-wires (superficial level: level of the K-wires anterior to the center of the patella; deep level: in the center at a deeper position of the patella), distance between the K-wires, and ratio of the lengths of the K-wires and the patella (Figure 3).

The distance between the K-wires (a), and the ratio between the K-wires (b) and the patella length (c).
Outcome measures
The primary outcome was early failure of fixation, which was defined as a loss of reduction of fracture displacement greater than 2 mm as compared with the immediate postoperative image, necessitating revision surgery. Fracture healing was defined as a patient having no pain or tenderness, the ability to walk independently, and evidence of trabecular bone growth across the fracture line. 8 Nonunion was defined as a fracture that had not healed 1 year after treatment or loss of fragment reduction and bony healing being impossible. 8 The secondary outcomes were implant loosening without loss of reduction, infection, implant failure due to trauma, and the need for implant removal. Implant loosening was defined as K-wire migration and K-wire loosening or breakage, with loss of the tension band effect. We defined cases of infection as those requiring intravenous antibiotics, involving the bone, joint, and/or implants, or requiring surgical irrigation and debridement.
Statistical analysis
All continuous data were expressed in terms of the mean and standard deviation of the mean. One-way analysis of variance (ANOVA) was performed to assess differences between groups when the Levene test for homogeneity of variances was not significant (p < 0.05); otherwise, the Mann–Whitney U test (two groups) was used. The Least Significant Difference test was performed as a post-hoc pair-wise analysis of the Kruskal–Wallis test. The generalized linear model for repeated measures with Sidak correction for multiple comparisons was performed to examine differences in scores at different follow-up points. The non-parametric Pearson’s Chi-square test evaluated by the Exact method was performed to investigate the relationships between group variables. For all tests, p < 0.05 was considered significant. Statistical analysis was carried out using Statistical Package for the Social Sciences (SPSS) software version 15.0 (SPSS Inc., Chicago, USA).
Results
Demographic data
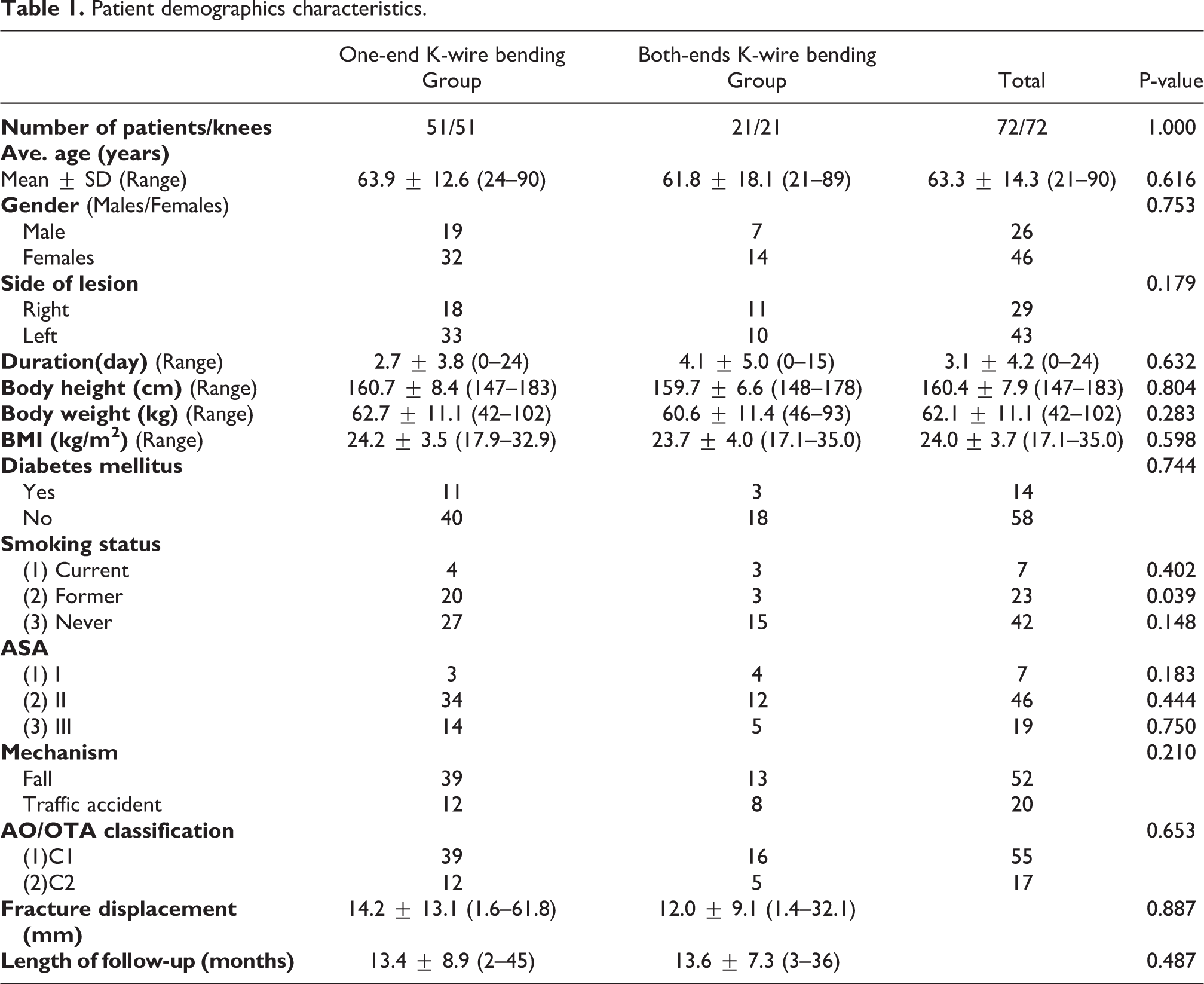
Seventy-two patients were involved in this retrospective study (26 males, 46 females). The majority of the fractures resulted from a direct contusion caused by falling (52 patients), followed by traffic accidents (20 patients). Patients were classified into two groups: a one-end K-wire bending fixation group (51 patients with a mean age of 63.9 ± 12.6 years, range, 24–90 years) and a both-ends K-wire bending fixation group (21 patients with a mean age of 61.8 ± 18.1 years, range, 21–89 years). Demographic information of both groups is reported in Table 1. The constituent proportions of gender, mechanism, fracture side, anesthesia risk (ASA), smoking status, history of diabetes mellitus, and AO classification were consistent between the two groups, with no significant differences (p > 0.05). Furthermore, no significant statistical differences existed in the mean age (p = 0.616), BMI (p = 0.598), time from injury to surgery (p = 0.632), fracture displacement (p = 0.887), and follow-up duration (p = 0.487) between groups.
Patient demographics characteristics.
Clinical results
Regarding the VAS pain score (Table 2), the mean score for the one-end and both-ends K-wire bending fixation groups was 2.0 ± 0.5 and 0.8 ± 0.7, respectively (Table 2), demonstrating a significant difference (p < 0.001). Compared with the one-end K-wire bending group, the both-ends K-wire bending group gained more significant flexion and total ROM. The mean extension values were 1.5 ± 2.9° in the one-end K-wire bending group and 0.7 ± 1.8° in the both-ends K-wire bending group, with no significant difference (p = 0.344). The both-ends K-wire bending group had an average flexion of 133.3 ± 7.5°, which was better than that in the one-end K-wire bending group (118.4 ± 15.4°, p < 0.001). The both-ends K-wire bending group had an average total ROM of 132.6 ± 7.8°, which was better than that of the one-end K-wire bending group (117 ± 15°, p < 0.001). The Lysholm score was significantly better in the both-ends K-wire bending group (90.6 ± 3.6) than in the one-end K-wire bending group (83.3 ± 5.0, p < 0.001).
Clinical results of the two groups.

Radiological results
Radiographic union occurred at a mean of 3.4 months post-surgery in both groups. The mean fracture healing duration for the one-end K-wire bending group was 3.7 ± 2.5 (range, 1–13 months), which was similar to that in the both-ends K-wire bending group (3.0 ± 1.2, range, 1–7 months; p = 0.828). The level of the K-wires, distance between the K-wires, and K-wires length over patella length did not differ between the two groups of patients (Table 3).
Radiological results of the two groups.

Complications
The complication rates were 36/51 (70.6%) in the one-end K-wire bending group and 2/21 (9.5%) in the both-ends K-wire bending group, showing a significant difference (p < 0.001) (Table 4). With regard to the primary outcome, four patients (7.8%) in the one-end K-wire bending group (Figure 4) and one patient (4.8%) in the both-ends K-wire bending group had loss of reduction; these patients were treated with revision TBW surgery. Six patients (11.8%) in the one-end K-wire bending group had nonunion, as compared with none in the both-ends K-wire bending group. Regarding the secondary outcomes, implant loosening without loss of reduction was observed in 28 patients (54.9%) in the one-end K-wire bending group (Figure 5) and none in the both-ends K-wire bending group (p = 0.001). Three patients in the one-end K-wire bending group and 1 patient in the both-ends K-wire bending group experienced implant failure due to new trauma; all received revision surgery. Two patients in the one-end K-wire bending group had a postoperative infection, as compared with none in the both-ends K-wire bending group. The patients who sustained an infection were successfully treated with superficial wound debridement and oral antibiotics. In the one-end K-wire bending group, 34 patients (66.7%) underwent elective implant removal, as compared with 15 (71.4%) in the both-ends K-wire bending group (p = 0.694).
Complications of the two groups.


Postoperative (a and b) and postoperative 3 months (c and d) radiograph of one case in the group of Tension band wire fixation with one end bending K-wire method. That encountered K-wire loosening with loss of fracture reduction.

Postoperative (a and b), postoperative 3 months (c and d), and postoperative 6 months (e and f) radiograph of one case in the group of Tension band wire fixation with one end bending K-wire method. The fracture got bone union; however, the K-wires were loosening progressively with time. The prominent K-wires cause irritation pain and lower functional score than the group of Tension band wire fixation with both ends bending K-wire method.
Discussion
The tension band wiring (TBW) technique is one of the most common surgical fixation methods for patella fracture. 9 It converts the anterior tension forces into compression forces at the articular surface through the extensor mechanism. 10 –12 The modified AO tension band technique has been widely used for transverse patellar fractures and has been shown to provide relatively stable fixation in many biomechanical and clinical studies; 13 however, many postoperative complications have been reported, including broken wires, loosening of K-wires causing irritation, and fixation failure. 14 Choi et al., Meena et al., Tamaki et al., and Kalia et al. reported cases of symptomatic migration of broken K-wires and wires used for patellar fixation to the popliteal fossa in 2008, 2013, 2015, and 2016, respectively. 15 –18 Wang and Lee and Sharma et al. reported cases of locking knee symptoms secondary to the migration of a broken patella wire into the knee joint. 19,20 A broken wire has also been reported to have migrated from the patella into the proximal tibia and the dorsolateral side of the foot. 21,22 Broken wires from the patella, besides lying in the soft tissue envelope around the knee joint, have even been reported to have migrated to the heart. 1 Due to the surface of the K-wire having no threaded sectors to fix to the bone, and the K-wire in the modified AO tension band technique being under traction by the quadriceps in the knee joint, loosening of K-wires is the main complication of TBW fixation of patella fractures. The technique of K-wire insertion has not been described in detail, and usually only one end of the K-wires is bent. 23 Several new fixation techniques have been shown to improve the stability and eliminate complications. Wu’s modified TBW technique, reported in 2001, is one of the simplest and most effective methods. 8 This revised technique comprises bending of both ends of the K-wires, which can more effectively control the K-wires, thus eliminating the possibility of wire migration and improving the fixation stability. The purpose of the present study was to investigate the clinical and radiographic results in patients with patella fractures who underwent TBW using two different fixation methods, the one-end and both-ends K-wire bending fixation methods.
Previous studies have compared the outcomes of these two surgical techniques. In 2011, Eggink and Jaarsma reported a case series of 60 patients with a follow-up period of 2–8 years. 24 They divided the patients into three groups, as follows: group 1, TBW with parallel K-wires proximally bent; group 2, TBW with parallel K-wires proximally and distally bent; and group 3, de-tensioning cerclage wiring fixing the patella to the tibial tuberosity. There were no significant differences in functional scores between patients treated with the different surgical techniques. In our study, the both-ends K-wire bending group had a significantly lower VAS pain score and a better Lysholm score. The reason for this may be the fact that the complication rate in the one-end K-wire bending group was higher in our series (70.6%) than in the previous study (51.2%), and that in the both-ends K-wire bending group was lower in our series (9.5%) than in Eggink’s study (61.5%). With regards to knee ROM, there was no significant difference between the patients undergoing different types of surgery in Eggink’s study. In our study, there was no significant difference between the two groups in extension. In both groups, patients had these fixed flexion deformity maybe due to the bending wire buried in the quadriceps tendon. However, we found that the both-ends K-wire bending group had more significant flexion and a greater total ROM than the one-end K-wire bending group. The reason for this was that 28 patients (54.9%) in the one-end K-wire bending group experienced the complication of implant loosening without loss of reduction, most of which was due to K-wire migration. These complications may cause patients to suffer from pain when moving and could delay the rehabilitation program with prolonged splint protection. As in Eggink’s study, no significant differences were found in the radiological outcomes between the two surgical groups in our series.
In 2017, Hsu et al. investigated the factors affecting the outcomes of modified TBW techniques in transverse patellar fractures, 25 and demonstrated that placing the tension band wire close to the patella and over the middle third of the patella decreased the rates of major loss of reduction and implant breakage. Similar results were obtained with bilaterally or proximally bent K-wires. These results were due to the location of the TBW differing between the two groups. In the present study, there was no significant difference in the location of the tension band wiring between the two groups; however, the both-ends K-wire bending group had a better clinical outcome and fewer complications.
The primary outcome of the TBW technique applied for the fixation of patellar fractures was deemed satisfactory in our study, as in other studies. 3,4 Six patients (8.3%) experienced implant failure with loss of reduction and six patients (8.3%) had nonunion. Regarding the secondary outcomes, postoperative infection was rare in our study, with only two patients in the one-end K-wire bending group suffering infection. In prior studies, 3,26 –28 the incidence of postoperative infection after fixation of patellar fractures ranged from 3% to 10%, which was similar to the overall incidence of 2.8% in our study. Four patients (5.6%) in our series suffered implant failure due to a new trauma, all of whom underwent revision TBW surgery with the both-ends K-wire bending technique. We interpret this complication as arising due to lack of patient compliance with postoperative splint protection. Even though a previous study 29 showed that TBW for patella fractures is suitable for enabling early ROM, the purpose of postoperative splint usage is to protect the implant, not guard against failure due to new trauma.
Forty-nine patients (68.1%) in our study underwent a second surgery for implant removal, which was a higher rate than in other studies, in which the rate of implant removal for symptomatic hardware ranged from 0% to 50%. 2,6,30 –32 This may be due to the high complication rate of K-wire migration in the one-end K-wire bending group and the traditional concepts of Chinese people, who are concerned about the presence of hardware in their body. The both-ends K-wire bending technique was not related to hardware prominence or implant removal. We measured the ratio of the K-wire length over the patella length on lateral X-ray films, and there was no significant difference between the two groups (p = 0.126). Although various biomechanical and clinical studies have demonstrated that the K-wires in the tension band technique can be replaced with cannulated screws or non-absorbable polyester, 33 –35 which have a greater strength of fixation and a lower complication rate owing to pain caused by hardware, cannulated screws are more rigid than K-wires, so the dynamic compression effect will be reduced if they are used in the tension band technique. 23
In order to critically analyze the differences between the two K-wire bending techniques, we excluded patients with type AO/OTA 34-C3 comminuted fractures, in whom additional K-wire fixation or circumferential wiring would have been applied.
There were several limitations of this study. First, it was a retrospective study. Second, the number of patients was relatively small in the two groups, which limited the power of the study and restricted our ability to identify independent factors predictive of suboptimal functional outcomes. Third, many orthopedic surgeons with different levels of experience, varying surgical techniques, and differing rehabilitation programs were involved in this study, which may have had an effect on the study outcomes. Therefore, more high-quality, double-blinded randomized controlled trials with greater case numbers are needed in order to confirm the advantages of Wu’s modified TBW technique.
Conclusion
When treating displaced patella fractures with Wu’s TBW technique, the both-ends K-wire bending fixation method results in a lower complication rate and a better clinical outcome than the one-end K-wire bending fixation method. This revised TBW technique can effectively control both ends of the K-wires, thus eliminating the possibility of K-wire migration and improving the fixation stability.
Footnotes
Acknowledgement
The authors thank Ya-Ju Yang, BS, for assistance with statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.