
Abstract
Background:
To reduce the risk of radiation exposure, we explored whether the total dorsal ramus block can be performed under ultrasound guidance. We evaluated the accuracy and effect of ultrasound-guided total dorsal ramus block for chronic low back pain.
Methods:
Accuracy of ultrasound guidance after total dorsal ramus block to the L4–L5 level was evaluated using fluoroscopy (n = 5). A second group was assigned into two groups: ultrasound-guided group (n = 19) or fluoroscopy-guided group (n = 18). The effects and adverse events were compared.
Results:
In all cases, the fluoroscopic findings revealed an accurate injection at the L5 level. Significant alleviation of pain was observed after ultrasound-guided total dorsal ramus block, and comparable effectiveness was observed with both ultrasound guidance and fluoroscopic guidance. There were no complications.
Conclusions:
The ultrasound-guided total dorsal ramus block may sufficiently block all three branches of the lumbar dorsal ramus at the targeted level resulting in significant pain reduction.
Introduction
Low back pain (LBP) is a leading cause of disability. 1 Chronic LBP (CLBP) can be defined as daily LBP for at least 3 months with a pain intensity greater than 5 on a 10-point pain scale. 2 CLBP has 9.9% point prevalence and 51.2% lifetime prevalence. 2 In more than 85% of patients with CLBP, a definitive cause or pathology cannot be found, resulting in a diagnosis of nonspecific LBP. 1,3 Suzuki et al. reported that orthopedists classified 78% of cases as “specific LBP” based on examination findings. 4 Although the injection of several blocks has been used to treat LBP, no definite treatment protocol has been established. Trigger-point injection therapy is considered for patients with trigger or tender points. 5 Miyakoshi et al. applied the total dorsal ramus block to treat CLBP and reported that blocking the entire lumbar dorsal ramus (medial, intermediate, and lateral branches) is effective in improving pain significantly compared to a trigger-point block. 6 The medial, intermediate, and lateral branches of the lumbar dorsal ramus principally innervate the three major longitudinal back muscles: multifidus, longissimus, and iliocostalis, respectively. 7,8 Furthermore, deep to the multifidus, each articular branch of the medial branch innervates the facet joints above and below it. 7,8 Administering large volumes of local anesthetics to a conventional point in the medial branch can block all three branches of the lumbar dorsal ramus. 6 However, the block requires fluoroscopy guidance. To eliminate the radiation exposure to patients and practitioners, we explored whether the procedure could be performed under ultrasound guidance or not. Furthermore, we investigated whether ultrasound guidance could yield the same effect as fluoroscopy guidance or not.
We conducted preliminary imaging and clinical evaluations of ultrasound-guided total dorsal ramus block in the present study. First, we investigated the feasibility of ultrasound in guiding the administration of an accurate block. Second, using a prospective randomized controlled study design, we compared the efficacies of ultrasound- and fluoroscopy-guided total dorsal ramus blocks in patients with nonspecific CLBP.
Materials and methods
Patients with CLBP lasting for more than 1 year without lower extremity symptoms were enrolled in the study. Computed tomography and magnetic resonance imaging were performed to rule out specific findings, such as spondylosis and osteoporosis. Exclusion criteria were previous lumbar surgery and the presence of lumbosacral transitional vertebrae. All patients had been treated with analgesics, cyclical trigger-point injections, and physiotherapy without success. Similar to a previous study, the L4–L5 level was chosen as the target level of the total dorsal ramus block in all patients. 6 The study protocol was approved by the Institutional Review Board of the study, and written informed consent was obtained from all patients.
Protocol 1
Five patients were enrolled to evaluate the accuracy of the ultrasound-guided total dorsal ramus block. There were three men and two women, with an average age of 72 years (range, 62–80 years). The patient was placed in the prone position on the fluoroscopy table with a pillow under the abdomen to decrease lordosis. A convex ultrasound Noblus probe (Hitachi, Tokyo, Japan) was placed at approximately the fifth lumbar level. The corresponding spinous, superior articular, and transverse processes were identified. The target point was set at the junction of the L5 superior articular process and the transverse process 6 (Figure 1). We confirmed the accurate position of the ultrasound-guided puncture using fluoroscopy. After correct needle placement and absence of blood aspiration were confirmed, 4.0 mL of mepivacaine 1% (Carbocaine; AstraZeneca, London, UK) mixed with 1.0 mL of Iotrolan (Isovist 240; Schering, Berlin, Germany) was gradually injected on each side in one patient, and 5.0 mL of mepivacaine 1% was injected on each side in four patients. During the injection, cranial rotation of the needle bevel was maintained to maximize the cranial spread of the solution. After bilateral administrations, the patient received contrast media to undergo an X-ray scan and was evaluated for the spread of the drug. Pain at rest and during motion in maximum flexion and extension was evaluated using a 100-mm visual analog scale (VAS) before and 30 min after the block.
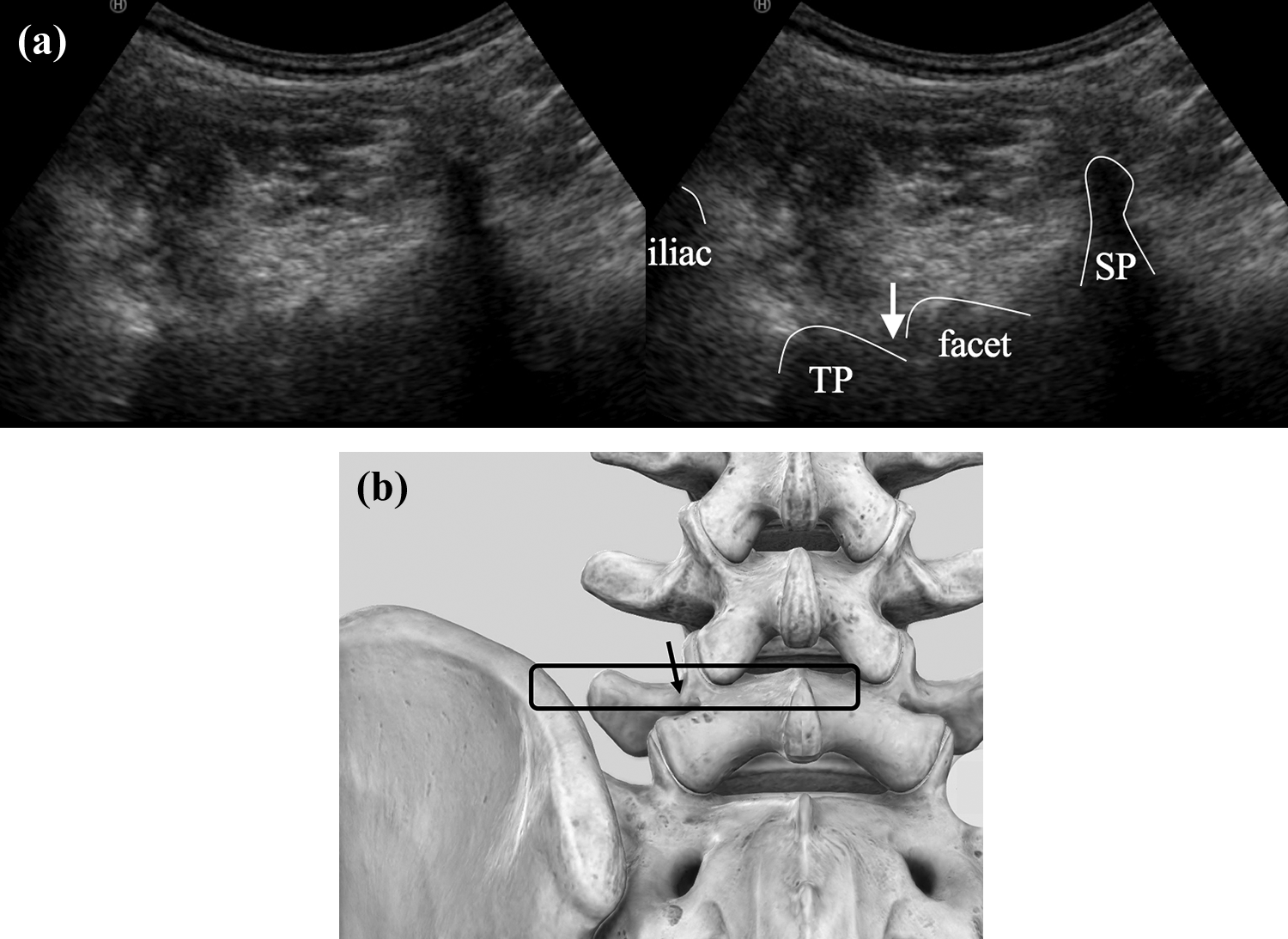
(a) Ultrasound axial image. The probe is initially placed at the level of fifth lumbar vertebra spinous process (or interspinous space) and transverse process. Placement is clearly identified via the arrow on the image. (b) The square indicates the position of the probe. The arrow indicates the position of the needle (image courtesy of Complete Anatomy). SP: spinous process or interspinous space; TP: transverse process.
Protocol 2
The aim of this protocol was to evaluate the effect of the ultrasound-guided total dorsal ramus block using a prospective, randomized controlled trial. Thirty-seven consecutive patients, different from those in protocol 1, were enrolled (13 men and 24 women; mean age, 76 years; range, 46–90 years). They were alternately assigned to two groups: ultrasound-guided (US group; n = 19; six men and 13 women; mean age, 74 years) or fluoroscopy-guided (FS group; n = 18; seven men and 11 women; mean age, 79 years) group. Both groups received the bilateral total dorsal ramus block with 5.0 mL of mepivacaine 1% on each side following the method of protocol 1.
Pain was evaluated using VAS at the following time points: before each treatment; 0.5, 3, and 12 h after each treatment; and 1, 3, 5, and 7 days after each treatment. 6 Defining a minimal clinically important difference (MCID) ≥4 as effective, 9 we compared the proportion of effective interventions between the two groups. Patients were also examined for the occurrence of adverse events.
Data analysis
All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). 10 The two-way analysis of variance was performed to evaluate the role of the treatment at different time points. Fisher’s protected least significant difference was used as the post hoc test for multiple comparisons. Paired or unpaired t-tests were used for comparisons between the two groups. A p value <0.05 was considered statistically significant.
Results
Accuracy and infiltration of injections
In protocol 1, for one patient who underwent the dorsal ramus block under ultrasound guidance, X-ray revealed that the radiocontrast dye had spread over the junction of the superior articular and transverse processes of both L4 and L5 bilaterally, where the medial branches of the L3 and L4 dorsal rami are located.
Puncture at the L5 level was confirmed in all five patients. The analysis of patient-reported pain scores on VAS showed a definite improvement after the total dorsal ramus block. VAS revealed that the rest and motion pain had significantly decreased after the block (mean ± standard deviation, 66.0 ± 18.2 to 25.0 ± 10.0, 71.0 ± 18.8 to 20.0 ± 7.1, respectively; p < 0.05). There were no complications, signs of nerve root block, or other neurological symptoms.
Comparison between ultrasound- and fluoroscopy-guided blocks
The differences in age and sex between the US and FS groups were not statistically significant. VAS scores had significantly reduced after the treatment in both groups (Figure 2; p < 0.0001). No significant difference in pain reduction was observed between the US and FS groups. In both groups, significant pain reduction continued for 7 days. Eleven (57. 9%) patients in the US group and 10 (55.6%) patients in the FS group had MCID ≥4, with no statistically significant difference. There were no complications, signs of nerve root block, or other neurological symptoms.
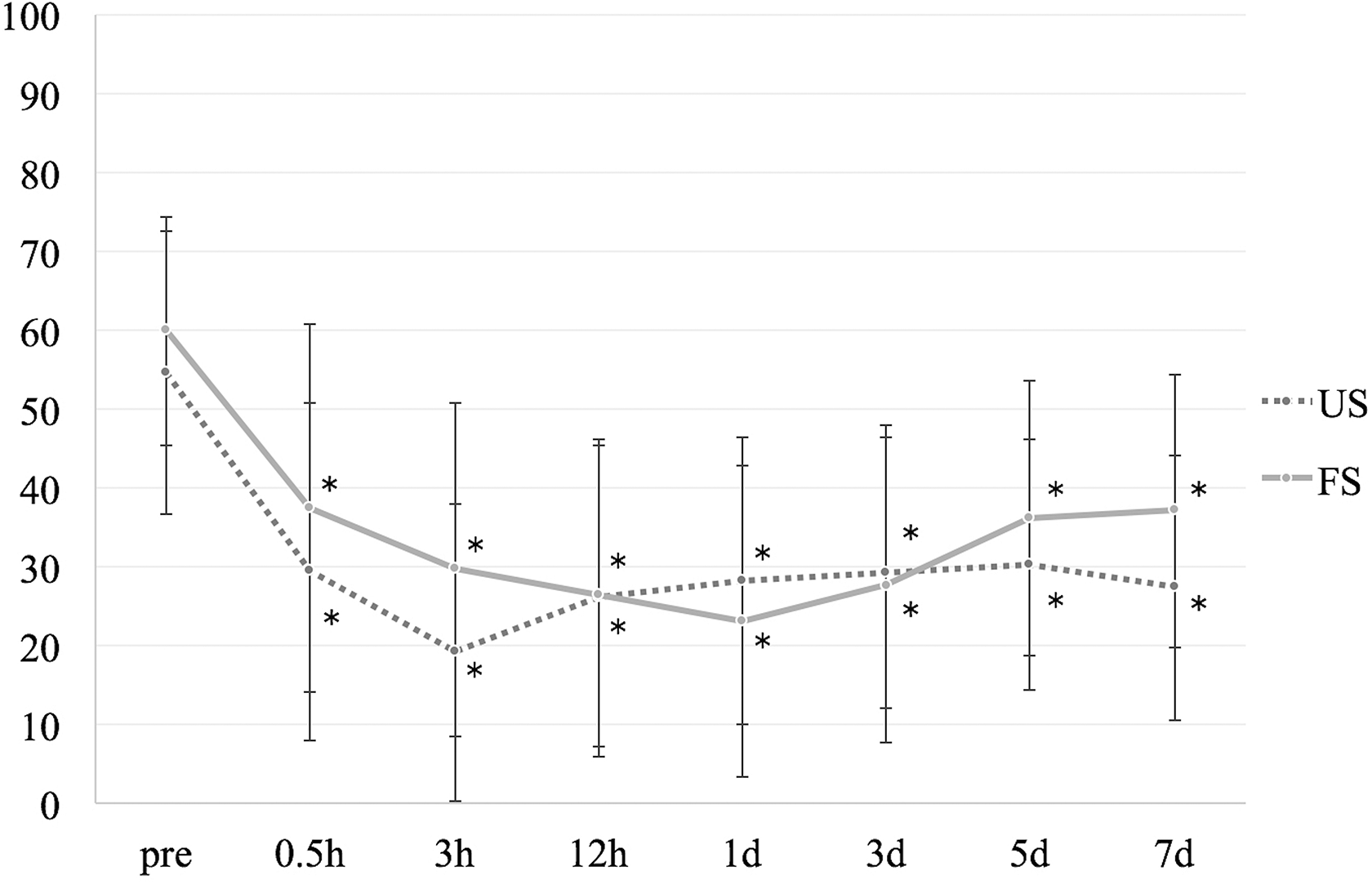
Changes in pain after the ultrasound- and fluoroscopy-guided total dorsal ramus blocks. Pain significantly reduced after the treatment. No significant differences in pain was observed between US and FS groups. *p < 0.0001. US: ultrasound-guided group; FS: fluoroscopy-guided group.
Discussion
The present study showed that the ultrasound-guided total dorsal ramus block was an accurate and safe procedure with demonstrated clinical effectiveness in the treatment of CLBP. The facet joints and surrounding muscles at the targeted level showed sufficient loss of pain with the ultrasound-guided total dorsal ramus block, 6 resulting in significant pain reduction after treatment. The effect lasted 1 week and improved CLBP in the short term. The ultrasound-guided total dorsal ramus block carries no risk of exposure to radiation and can be performed in most clinical settings.
Spine surgeons have experienced more chances of exposure to radiation in recent years because of the various minimally invasive, fluoroscopy-assisted surgical procedures, such as percutaneous pedicle screw insertion, 11,12 oblique lateral interbody fusion, and extreme lateral interbody fusion. 13,14 According to previous reports that investigated the surgeon’s radiation exposure dose during these procedures, the radiation doses were within the level of the safe occupational exposure risk. 15 –17 However, surgeons performing minimally invasive spine surgeries may be exposed to much greater radiation levels during fluoroscopy-assisted surgical procedures than during other, non-spinal musculoskeletal procedures. 17 Myelography, radiculography, and root blocks, which are commonly performed by spine surgeons in Japan, also involve the use of radiation.
The International Commission on Radiological Protection lays down recommendations and guidelines for occupational radiation exposure. 18 The normal occupational dose limits are 20 mSv/year for effectiveness, 150 mSv for the lens of the eye, and 500 mSv for the skin or hands. The effective doses during myelography alone were 0.01 mSv with a torso and neck protector, 0.02 mSv with a torso protector alone, and 0.10 mSv without either protector per examination. The effective doses during radiculography and root block were 0.00 mSv with a torso and neck protector, 0.01 mSv with a torso protector alone, and 0.03 mSv without either protector per examination. 19 In this study, the exposure dose was not measured; however, an equivalent exposure dose was expected. By doing this under ultrasound guidance, these radiation exposures can be eliminated, ensuring reduced exposure to both the practitioner and patient.
Other benefits of ultrasound guidance are as follows: (1) Real-time continuous visualization of needles and the avoidance of damaging important structures, for example blood vessels. The blood vessels around the nerve roots are branching from or anatomizing with the spinal arteries. (2) Real-time observation of flow of the injecting solution by tuning on the power Doppler mode of ultrasound to assess the flow during injection. (3) The integrity and characteristics of the muscles passing through the needle overlying the facets and transverse processes can also be assessed; a major example related to CLBP is fatty changes in the multifidi.
This is the first prospective randomized study comparing the effectiveness of the ultrasound-guided total dorsal ramus block with the conventional fluoroscopy-guided total dorsal ramus block. However, this study had a few limitations. First, the clinical evaluation in this study was only conducted with respect to the change in reported pain. The evaluation of therapeutic interventions for LBP requires exploring other domains of the patient’s quality of life. Second, most participants in this study were elderly patients with spinal degenerative changes, such as facet joint osteoarthritis and intervertebral disc degeneration. Effects in young patients should also be evaluated because the younger population with less degenerative changes might show a more sustained improvement. Finally, the present study was designed to block the L4–L5 level because this level is most frequently involved in lumbar spine disorders. 20,21 For the treatment of LBP, the selection of the level to be treated is performed arbitrarily. 22,23 However, further studies are required to test the effects of the ultrasound-guided total dorsal ramus block on other lumbar levels.
This preliminary study evaluated the use of the ultrasound-guided dorsal ramus block for CLBP. The results of this study showed that the procedure may have sufficiently blocked all three branches of the lumbar dorsal ramus at the targeted level, resulting in significant pain reduction. This study encourages us to start comprehensive clinical trials in order to elucidate the relevance of this technique in the treatment of CLBP.
Footnotes
Acknowledgement
The authors thank Dr Hiroyuki Kodama for help with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.