
Abstract
Introduction:
Sarcopenia and osteoporosis increase the risk of fall, resulting in fragility fracture. Intervention programme on sarcopenic hip fracture was set up in our centre.
Method:
All patients aged ≥65 admitted to Caritas Medical Centre with operatively treated hip fracture and diagnosed with sarcopenia were included. Interventions include inpatient nursing education, dietary advice, therapist assessment and structured 12-week Geriatric Day Hospital (GDH) exercise programme. Those who are not eligible for GDH training were classified as control group. Changes in relative skeletal muscle mass index (RASM), muscle strength and functional scores were measured.
Results:
There were 11 intervention and 13 control patients. Both groups of patients were noted to have improvement in RASM, knee extension power of lower limbs and functional scores. Between-group analysis showed there was more improvement in injured limb extension power in the intervention group, although it is statistically insignificant (control group: 3.585 kg, intervention group: 5.827 kg, p = 0.147). There was no statistically significant difference in the 3-month change in RASM (control group: 0.581 kg/m2, intervention group: 0.347 kg/m2, p = 0.369) and functional scores.
Conclusion:
These sarcopenic hip fracture patients may be too frail to benefit from traditional exercise treatment for sarcopenia. However, more improvement in muscle strength was observed in the intervention group although not statistically significant. Intervention programme with exercise prescription in sarcopenic hip fracture patients may have the potential to improve the lower limb muscle strength. A more intensive and longer exercise training programme with incorporation into day rehabilitation model may be needed for these frail hip fracture patients.
Introduction
Ageing is associated with progressive decline in skeletal muscle mass that may lead to decreased strength and functionality. In 1989, Rosenberg first referred this age-related decrease in muscle mass as ‘sarcopenia’, which derives from the Greek words ‘sarx’ (flesh) and ‘penia’ (loss). 1 Sarcopenia is a syndrome characterized by progressive and generalized loss of skeletal muscle mass and strength. For geriatric hip fracture patients, the prevalence of sarcopenia was found to be alarmingly high (73.6% in males and 67.7% in females) in the previous study. 2
There were different studies correlating sacropenia with physical disability and functional impairment. Janssen et al. 3 reported that the likelihood of functional impairment and physical disability is approximately twofold greater in older men and threefold greater in older women with severe sarcopenia by comparison with elderly with a normal muscle mass. Another epidemiological study conducted in Mexico also showed similar results. 4 Furthermore, Melton et al. 5 reported that sarcopenia is associated with having difficulty in walking.
Sarcopenia was also found to be associated with the increase in fall risk. Landi et al. 6 reported that sarcopenic individuals were over three times more likely to fall during a follow-up period of 2 years relative to nonsarcopenic individuals. Other studies 7,8 reported a threefold increase in fall risk in people with sarcopenia.
A number of recent studies found that sarcopenia was associated with osteoporotic hip fractures. 9 –13 There were also three other large studies correlating sarcopenia and osteoporotic fracture in general. 14 –16 For all these studies, sarcopenic patients were found to have a significantly increased risk of suffering fragility fracture. Other adverse outcomes related to sarcopenia included poor quality of life 17,18 and death. 19 –21 It also imposed significant cost on the healthcare system. 22
To prevent the negative impact of sarcopenia on hip fracture patients and to improve recovery, sarcopenia treatment is of paramount importance. There are different proposed treatment modalities in the literature, but their effectiveness was still controversial. There is increasing evidence to suggest the increase in protein intake 19,23 and progressive resistive exercise 24 –26 can increase muscle mass and strength. Both have been recommended to combat sarcopenia. A systematic review by Latham et al. 27 reported that most strength training programmes had durations of 8–12 weeks, used two to three sets of 8–10 repetitions and were performed two to three times per week. Most of the reviewed studies reported an increase in muscle strength and improvement in functional performance.
Nevertheless, the evidence concerning the efficacy of potential therapies for sarcopenia is still scarce. Currently, there is still knowledge gap for the recommended treatment of sarcopenia specifically for geriatric hip fracture patients, who may represent a different group of patients compared with the general elderly population.
In this study, hip fracture patients diagnosed with sarcopenia were enrolled in an integrated intervention programme and to see whether their muscle mass and functional status will improve after the treatment. The proposed training programme was a multidisciplinary training programme involving occupational therapist and physiotherapists, which was based on the current training programme in Geriatric Day Hospital (GDH) and unified to a 12-week programme.
The objective of this study was to evaluate the effectiveness of the integrated physical training programme on geriatric hip fracture patients with sarcopenia. Our hypothesis was that the use of an outpatient integrated physical exercise programme consisting of progressive resistance training exercise and nutritional supplement is effective in treating sarcopenia in hip fracture patients and improves recovery.
Methods
Design and setting
This is a prospective non-randomized study to evaluate the effect of an integrated programme on geriatric hip fracture patients with sarcopenia. All patients aged 65 or above admitted to Department of Orthopaedics and Traumatology of Caritas Medical Centre from 1 July 2015 to 31 December 2018 with operatively treated hip fracture and diagnosed with sarcopenia were included. Assessment was carried out within 2 weeks of admission and was repeated 3 months later. The study protocol was approved by the Kowloon West Cluster Clinical Research Ethics Committee.
Inclusion criteria
All patients aged 65 or above admitted to Department of Orthopaedics and Traumatology of Caritas Medical Centre with operatively treated hip fracture and diagnosed with sarcopenia were included. Operations for geriatric hip fracture were defined as a patient-episode with ICD-9-CM procedure code of 81.52, 51.51, 81.40, 79.15, 79.35 or 78.55. The diagnosis of sarcopenia was based on previous Consensus report of the Asian Working Group for Sarcopenia 28 with relative skeletal muscle mass index (RASM) below cut-off value of 7 kg/m2 in men and 5.7 kg/m2 in women.
Exclusion criteria
We selected the cases with relatively good premorbid ambulatory status and metal status to cope with the training programme. To improve dual-energy X-ray absorptiometry (DXA) accuracy in diagnosing sarcopenia, we excluded those patients with a huge metallic implant. We excluded other causes that will affect the treatment of sarcopenia, for example, malnutrition, diabetes mellitus on insulin and renal impairment. Pathological fractures and complication of surgery were excluded as these may affect the rehabilitation progress. The exclusion criteria are listed below. Age above 99 Hong Kong Montreal Cognitive Assessment below 22 scores Major joint replacement surgery over contralateral side (total hip replacement, total knee replacement and hip hemiarthroplasty) Modified functional and ambulatory category (MFAC) below 5 in the previous 6 months Mini nutritional assessment below 11 or serum albumin below 21 g/L Diabetes mellitus Pathological hip fracture or cancer disease in active phase or undergoing treatment (radiotherapy or chemotherapy) Renal impairment with glomerular filtration rate less than 40 mL/min/1.73 m2 Cut-out of internal fixation device requiring further surgery Poor compliance to physical exercise training programme attending less than 12 sessions
Division of group
Eligible patients with sarcopenia were divided into intervention group or control group. Those who were not within the GDH catchment areas or refused GDH training were classified as control group. Others were divided into intervention group.
Intervention
All patients will receive conventional 3 weeks in-patient rehabilitation programme, consisting of daily walking training exercise, self-care training, pain relief treatment, hip mobilization and strengthening, physical mobility and ambulatory training as well as education for hip precaution and fall prevention strategy. All patients will receive high protein diet (1.2–1.5 g/kg/day) throughout the stay in orthopaedic rehabilitation ward. Education and dietary advice will be given to patient upon discharge.
For intervention group, apart from the conventional 3 weeks in-patient rehabilitation programme, the patients will receive an extra 12-week integrated physical training programme with sessions twice weekly (24 sessions in total) in GDH. The programme includes progressive upper and lower limb strength training. The content of progressive upper and lower limb strength training includes four resistance exercises (two for upper limb and two for lower limb). The muscle groups for upper limb are biceps and wrist flexors, whereas for lower limb are gluteus maximus and quadriceps. Each muscle group should be trained for a total of three sets with 12 repetitions per set and a rest interval of 2 min in between. 27 The number of physical exercise training sessions that patient attended would be recorded.
Outcome measures
The outcomes we measured were based on the definition of sarcopenia proposed by the European Working Group on Sarcopenia in Older People in 2010 29 and Consensus report of the Asian Working Group for Sarcopenia, 28 which include the presence of low muscle mass with low muscle strength or low physical performance. The primary outcome of this study was the change in muscle strength, which was measured as isokinetic knee extension. Other secondary outcomes include the change in body composition and functional outcome. Clinicians and therapists assessed all study subjects within 2 weeks after admission and at 3 months later, thus two sets of data were collected.
The outcomes were assessed as follows:
Muscle strength—Isometric knee extension
Maximal isometric knee extension strength was assessed for both limbs with a fixated hand-held dynamometer (JAMAR hand dynamometer). The patients were seated on an examination couch with their arms crossed, theirs knees at a 90° angle and their upper limb fixed with a strap to the examination couch during testing. The transducer was positioned under a fixation belt that was fastened to the examination couch. After familiarization with the procedure, the patients would perform three voluntary isometric knee extensions for each limb with strong verbal encouragement, separated by a minimum of a 30-s pause. Among the three trials of exertion, maximal isometric strength in kilogram (kg) would be registered 30 (Figure 1).

Measurement of isometric knee extension muscle strength.
Body composition—RASM
Appendicular and whole-body lean body mass will be measured by DXA. Appendicular skeletal muscle mass will be normalized by size (sum of lean muscle mass in upper and lower limb/square of body height). 31
Functional outcome—The elderly mobility scale
The elderly mobility scale (EMS) by Smith was devised for assessing mobility in frail, elderly people, and contains seven items considered essential for performing the basic activities of daily living. These items include transfer, gait, and balance tasks, scored from 0 (totally dependent) to 20 (representing independent mobility in the hospital environment). 32
Functional outcome—The modified functional and ambulatory category
The modified functional and ambulatory category (MFAC) is a seven-point Likert-type scale (I–VII) that is used to classify a patient’s walking capacity with or without walking device. Gait is divided into seven categories, ranging from no ability to walk and requires manual assistance to sit or is unable to sit for 1 min without back or hand support (MFAC I) to the ability to walk independently on level and non-level surfaces, stairs and inclines (MFAC VII). 33
Functional outcome—The modified Barthel index
Modified Barthel index measures performance in activities of daily living in 10 areas of functioning, which include feeding, grooming, dressing, transfer, toileting, bathing, walking, stairs climbing, bowel and bladder control. The score is on a scale of 0–100, where 100 indicates total independence and 0 indicates total dependence. 34
Statistical analysis
Data analysis was performed with SPSS (Windows version 20.0; IBM Corp, Armonk, New York, United States). Mann–Whitney U-test was used for data analysis. Results with a p-value of <0.05 were considered statistically significant.
Results
During the study period, 123 patients were identified as having geriatric hip fracture. Eighty-nine of them were diagnosed of sarcopenia. Sixty-five patients were excluded because of the exclusion criteria listed above or loss to follow up. For the remaining 24 patients, 13 patients did not fall into GDH catchment area or refused GDH training, they were the control group. The other 11 patients who received regular GDH training were the intervention group.
There were 13 patients in the control group and 11 patients in the intervention group. The mean age in the control group was 78.7 and the intervention group was 81.5. Female-to-male ratio in the control group was 9:4 and the intervention group was 8:3. All patients were discharged back to home after rehabilitation. Baseline characteristics of both groups of patients are listed in Table 1. There was no significant difference between two groups (p > 0.05).
Baseline characteristics of patients with fragility hip fracture.
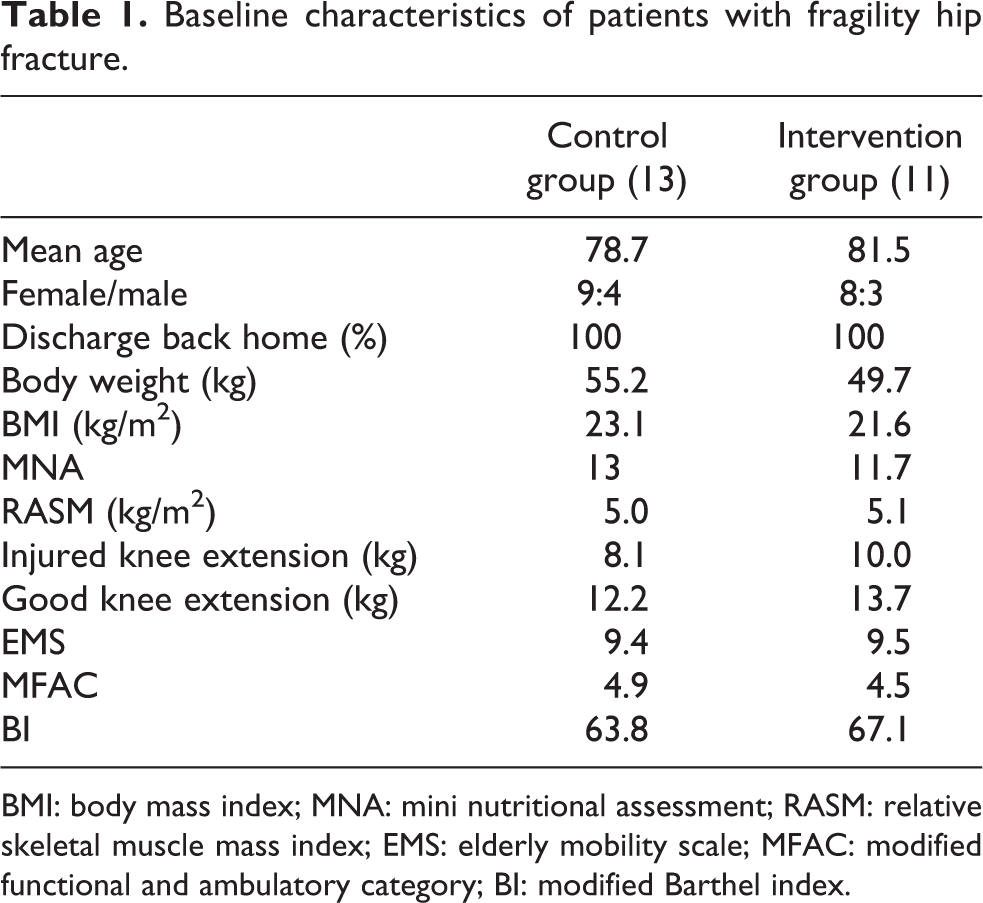
BMI: body mass index; MNA: mini nutritional assessment; RASM: relative skeletal muscle mass index; EMS: elderly mobility scale; MFAC: modified functional and ambulatory category; BI: modified Barthel index.
Muscle mass, muscle strength and functional performance were measured accordingly. All patients had improvement in RASM, limb extension power and all functional scores (MFAC, EMS and BI) throughout 3 months. Between-group analysis showed more improvement in knee extension power of injured limb in intervention programme group with 5.827 kg increment while the mean difference was 3.585 kg increment in the control group, although it is statistically insignificant (p = 0.147). The mean difference in RASM between discharge and 3-month is 0.581 kg/m2 increment in the control group and 0.347 kg/m2 increment in the intervention programme group (p = 0.369). There was no statistically significant difference in the improvement of functional scores (Table 2).
Average changes in muscle mass, muscle strength and functional scores after 3 months.
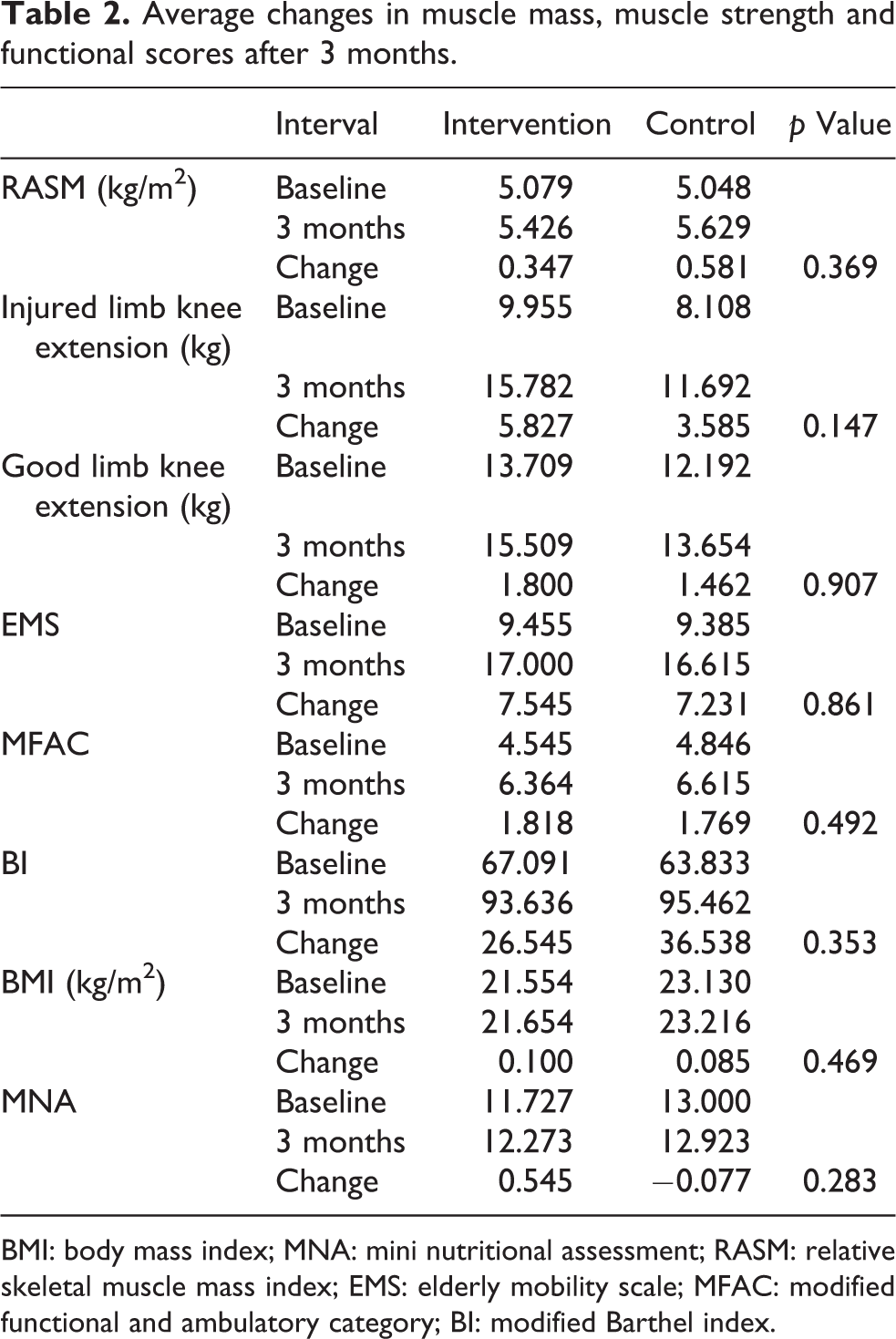
BMI: body mass index; MNA: mini nutritional assessment; RASM: relative skeletal muscle mass index; EMS: elderly mobility scale; MFAC: modified functional and ambulatory category; BI: modified Barthel index.
Discussion
Numerous studies had demonstrated the benefit of sarcopenia training programme with progressive resistive exercise and nutritional supplement. 24 –27 Even in the frail elderly population, recent studies by Yamada et al. 35 and Theou et al. 36 also showed positive effects in preventing frailty progression and disability. Exercise in frail individuals increases functional performance, balance, walking status and reduce fall. In a recent randomized controlled trial by Singh et al., 37 they demonstrated a year of resistance exercise in frail persons following hip fracture reduced mortality, nursing home admissions and ADL dependency. Sylliaas et al. 38 report the effect of prolonged strength training in older patients after hip fracture. The programme comprised four exercises, performed at 80% of maximum capacity, took place at either therapist sessions or home-based programme and 24 weeks after index fracture. The intervention group showed significant improvements in strength, gait speed and gait distance, instrumental activities of daily living and self-rated health.
In this study, all hip fracture patients received inpatient nutritional supplement, nursing education, therapist assessment and training after hip fracture operation. Improvement in muscle mass, muscle strength and functional recovery was noted in all hip fracture patients with sarcopenia after discharge from ward. In between-group analysis, there was more improvement in lower limb muscle strength in intervention group although it is not statistically significant. A larger sample size may be able to prove the statistical significance. The similarity of improvement in functional scores between two groups was likely due to ceiling effect of EMS, BI and MFAC measurements. There was also no significant difference in the change in the muscle mass.
Comparing with previous studies on exercise training programme on community dwelling sarcopenic elderly, 37 results were suboptimal in our hip fracture population. There were several potential reasons for these not so encouraging results. Hip fracture patients were found to be frail older adults with a fall history, weight loss, low physical activity, cognitive decline and depression in other studies. 39 These are all poor prognostic factors in recovery. The demographics of patients were also different. Caritas Medical Centre is located in Sham Shui Po, which is ranked third in poverty rate among 18 districts in Hong Kong in 2017. 40 Many patients in Caritas Medical Centre came from elderly centre and had poor social support. Our patients may be too frail to benefit from the resistive exercise training after hip fracture. Other potential reasons were the limited frequency and short duration of GDH training. A more intensive and longer duration of muscle training programme such as 12 months may be required to build up muscle mass and strength in such a frail patient population.
There are limitations for the design of this study. First, this study was not a randomized control trial. The study design was limited due to the public system of Hospital Authority and relatives’ unwillingness to bring patients to GDH for training. Second, this study was limited due to its small sample size. Many patients were too frail with multiple medical illnesses and were excluded according to the exclusion criteria. Third, the duration of GDH training was also very limited. Another factor is we cannot control the actual protein intake after the patients were discharged from the hospital. This is especially true in our geographic region, where the proportion of social underprivileged elderly is high.
This study showed the potential of exercise programme for sarcopenic hip fracture patients to improve muscle strength. Further studies with a larger sample size are necessary to identify any potential benefit for resistive exercise training programme. The frequency of the exercise training should increase and the duration of the programme should be extended to 12 months to visualize any potential benefits. One of the proposed ideas is to enhance the post-discharge care by incorporation of sarcopenia intervention, which includes nutrition support and exercise programme, into a new ‘day rehabilitation’ model. With day rehabilitation, patients can have more frequent muscle training and follow-up. It also has the benefit of shorter hospital stay and more engagement in training with family support.
In this study, we hope to show that just a short period of training was not enough for this group of frail elderly. We would like to urge the government to put in more resources to extend the rehabilitation of hip fracture patients. Moreover, we would like to raise awareness of the community about the importance of a long period of training. With the potential assistance of other non-governmental organizations, a more standardized long-term programme can be established for the treatment of sarcopenia.
Conclusion
Hip fracture patients with sarcopenia may represent a special group of sarcopenic individuals that are resistant to traditional exercise treatment. Further studies are needed to investigate the potential benefits of intensification and extension of rehabilitation training programme for this group of frail patients on sarcopenia treatment. The idea of incorporation into day rehabilitation programme should be considered.
Footnotes
Acknowledgement
We would like to thank our physiotherapists, occupational therapists and also colleagues in Geriatric Day Hospital in assisting us to conduct this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.