
Abstract
Introduction:
Hip fractures are a significant health risk in older adults and a major cause of morbidity, functional decline and mortality. Our aim was to compare clinical outcomes of older patients hospitalized in an ortho-geriatric (OG) unit to those hospitalized in an orthopedic department (OD) for surgical treatment of a hip fracture.
Methods:
A retrospective cohort study of hip fractured patients hospitalized between 2015-2016 in a single tertiary university-affiliated medical center. Included were patients aged 65 and older who had undergone hip fracture surgery and were admitted to either a geriatric or orthopedic ward.
Results:
441 patients met the inclusion criteria (195 in the OG unit, 246 in the OD); 257 were transferred to an affiliated geriatric center hospital (107 from the OG unit and 127 from the OD) for rehabilitation. Patients in the OG unit were older, more cognitively and functionally impaired and with more comorbidities. The 1-year mortality rate was significantly lower in the OD group (OR 0.32, CI 95% 0.19-0.53, p < 0.001), however, after propensity matching, the 30-day and 1 year mortality rates were similar in both groups. No difference was found in the rehabilitation length of stay between the groups. The functional independence measure improvement was similar in both groups, with a non-significant trend toward better functional improvement among OG unit patients.
Conclusions:
Despite the higher complexity of patients, worse baseline functional capacity in the OG unit, improvement after rehabilitation was similar in both groups. These results demonstrate the advantages of the OG unit in treating and stabilizing frail older adults, thus maximizing their chances for a successful recovery after hip fractures.
Level of Evidence:
Level IV
Introduction
Hip fractures are a significant health risk in older adults and a major cause of morbidity, functional decline and mortality. 1 One-year mortality rates following hip fractures are as high as 30% with only 50% of all patients returning to their previous functional status. 2,3 As the world population ages, the incidence of hip fractures continues to increase. It is estimated that approximately 1.6 million fractures per year, worldwide, will occur and double in 20 years. By 2050, the fracture rate is predicted to reach 6.3 million per year. 4,5 The importance of the geriatrician in managing hip-fractures is well known. Among the advantages are higher home discharge, lower re-hospitalization and lower post-operative delirium and depression rates. 6 -9
Studies addressing functional status outcomes of hip fracture patients following a geriatric assessment are scarce and have reported mixed results. 10 -12 The cumulative work demonstrating the advantages of a geriatric assessment for older adults with hip fractures has led many orthopedic departments to integrate geriatricians into the department. Another approach which has evolved in recent years is hospitalizing elderly patients suffering from hip fractures in acute geriatric wards, to be cared for by a multidisciplinary team including orthopedic surgeons as consultants. Several studies have reported the advantages of this strategy which include shorter waiting time for surgery, shorter hospitalization, better cost effectiveness, reduction of in-hospital mortality, better functional improvement and lower rates of re-hospitalization. 13 -15
Older adults (≥65 years) hospitalized in our medical center, diagnosed with a hip fracture are admitted either to the ortho-geriatric (OG) unit of the acute geriatric ward or to the orthopedic department (OD), based on the availability of beds and the orthopedic surgeon’s judgment in the emergency room (ER). In the OG unit, patients undergo comprehensive geriatric assessments by a multi-disciplinary team (including a geriatrician, physiotherapist, occupational therapist, dietitian, etc.) and receive a tailor-made treatment plan. The plan addresses optimal preparation for surgery, prevention, identification and treatment of major complications (e.g. delirium, pain control, dehydration, early mobilization and proper nutrition). In the OD, geriatric consultations ensue when the orthopedic surgeon deems it necessary. In this study, we aimed to retrospectively compare the demographics and clinical outcomes of older patients hospitalized in the OG unit versus older patients hospitalized in the OD for surgical treatment of a hip fracture.
Patients and Methods
Study Design
This was a retrospective cohort study of hip fractured patients hospitalized in a single tertiary university-affiliated medical center between 2015-2016. All patients aged ≥65 hospitalized in the OG unit or OD for acute hip fracture surgery, were included in the study. Exclusion criteria included patients who had not undergone hip fracture surgery, those who had experienced a trauma other than an accidental fall (such as a motor-vehicle accident) and patients with fractures which had occurred in the hospital. Data were retrieved from our center’s computerized databases and included patients’ demographics, medical history, drug prescriptions, performance status, cognitive status, routine laboratory tests, fracture type, type of surgery, post-operative complications and rehabilitation status, when available. Comorbidity burden was evaluated by the Charlson Comorbidity Index (CCI). 16 Performance status was assessed by the Katz Index of Independence for Activities of Daily Living (ADL) 17 and the Functional Independence Measure (FIM) score. Cognition was assessed by standard screening tests such as the Mini–Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA) 18 or obtained from the patient’s medical history. Complications which were evaluated included mortality, post-operative infections, cardiovascular complications, cerebrovascular events, thromboembolic events, acute kidney injury and the administration of blood products. Ethical approval was received from the local Ethics Committee of Rabin Medical Center (IRB# is 0532-17-RMC), however, in view of the retrospective nature of the study, all procedures performed were part of the routine care, thereby, there was no need for the patients’ informed consent.
Please see Strobe Checklist.
Statistical Analysis
Continuous variables are presented as mean and standard deviation (SD). Quantitative and ordinal variables (such as FIM scores) are presented as absolute and relative frequencies. The student’s t-test was used for continuous data and the Fisher exact test for categorical data. To reduce possible confounding variables between the 2 groups (OD and OG unit), a propensity score matching was performed. The Kaplan-Meier analysis measured the survival curves; the Log-Rank method compared them. All comparisons were 2 tailed. A p-value of <0.05 was considered significant. Statistical analysis was performed using the SAS (software) system.
Results
Between January 2015 and December 2016, 564 hip fractured patients were hospitalized in our medical center, of whom, 441 patients met the inclusion criteria (195 in the OG unit, 246 in the OD). Baseline characteristics showed significant differences between groups (Table 1). Patients in the OG unit were significantly older, more cognitively and functionally impaired, with higher rates of polypharmacy on admission. The CCI was higher in the OG unit group, mostly due to a higher prevalence of congestive heart failure and dementia. There were no significant differences between groups in the hip fracture types, time to surgery, and type of surgery (Table 1).
Baseline Characteristics.

a Functional status according to the Katz Index of Independence of Activities of Daily Living.
b Cognitive status according to Mini-Mental State Examination.
Abbreviations: OG, orthogeriatric; OD, orthopedic department; SD, standard deviation; CCI, Charlson Comorbidity Index; DHS, dynamic hip screw; PFNA, proximal femoral nail antirotation.
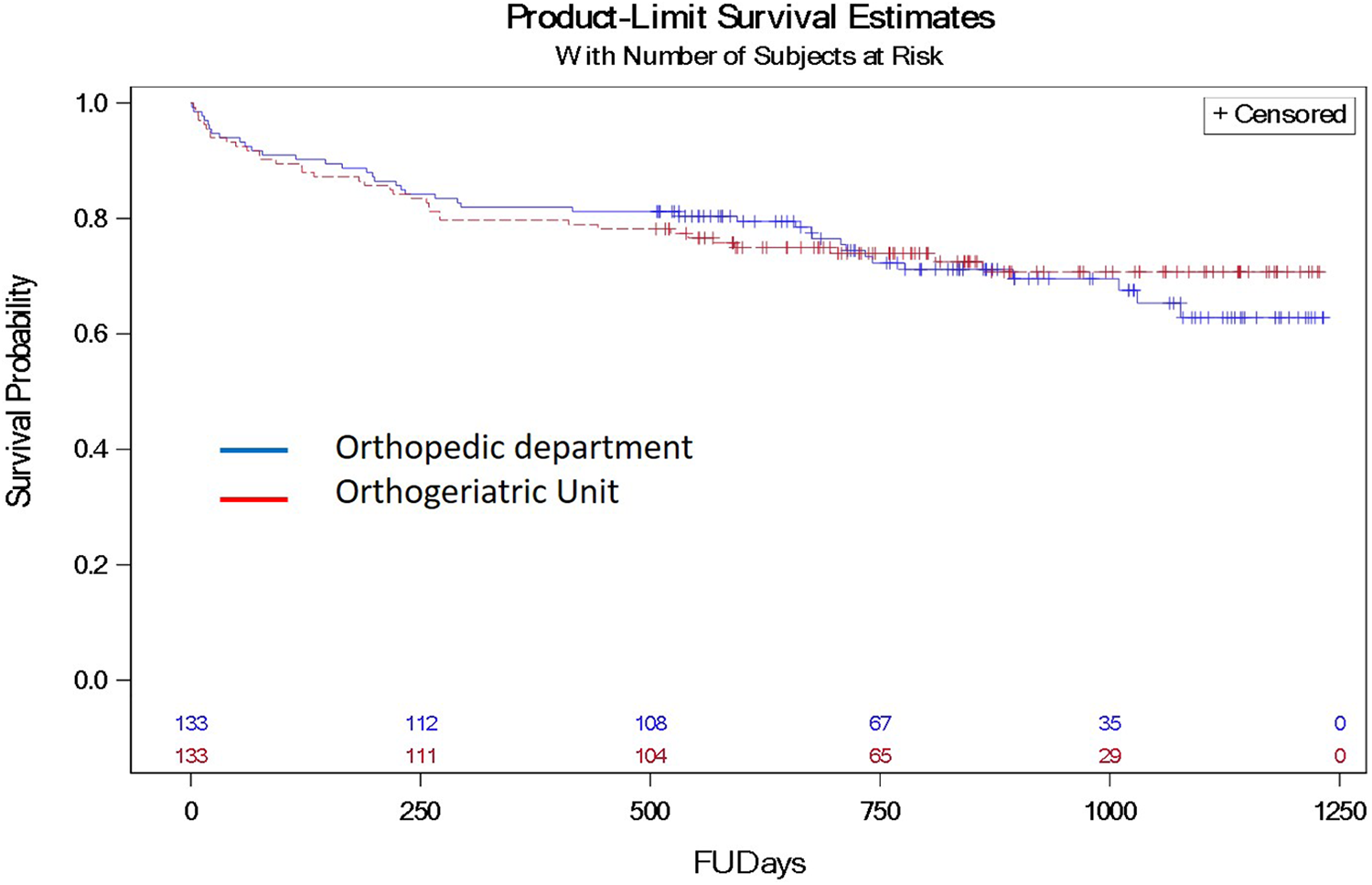
Post-operative complications differed between the groups (Table 2). Hospitalization length was significantly longer in the OG unit (12.1 ± 7.2 days vs 8.3 ± 4.5 days, p < 0.001) and there were significantly more post-operative infections and less events of acute kidney injury in the OG group (Table 2). One-year mortality rates were significantly lower in the OD group (11.8% vs 29.2%, OR 0.32, CI 95% 0.19-0.53, p < 0.001). Figure 1 shows the long-term mortality rates of the 2 groups. However, after propensity matching, the 30 day and 1 year mortality rates were similar in both groups (Figure 2). Patients in the OG group received significantly less packed cell units than the OD patients (a mean of 0.89 vs 1.29 p = 0.013). While 4% of the patients in the OD group were transferred to an internal medicine ward due to complications, all patients in the OG group remained in the geriatric department.
Post-Operative Outcomes.
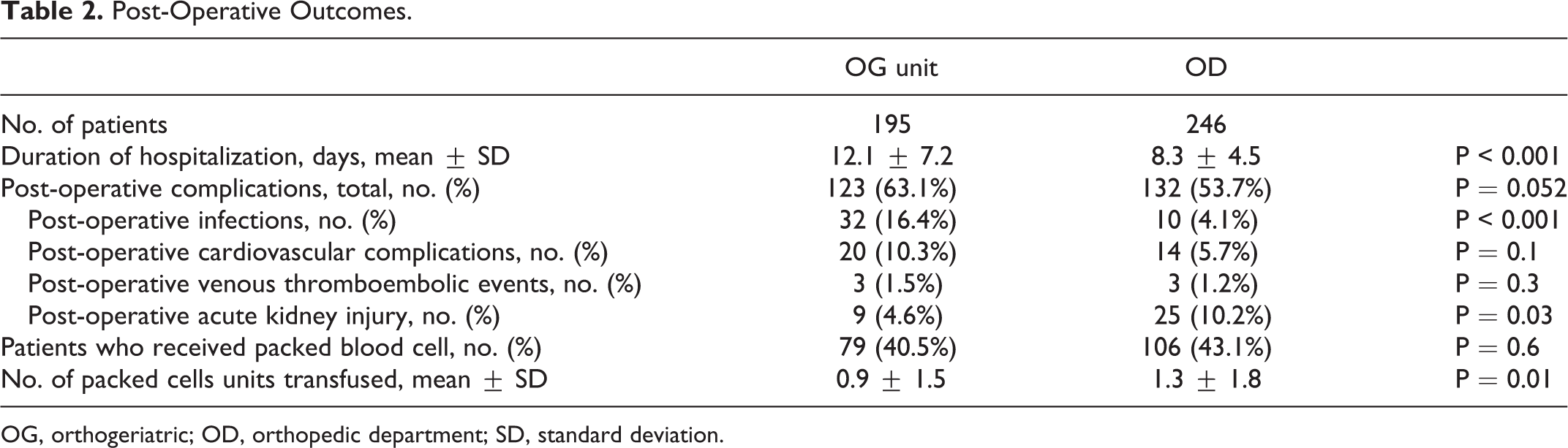
OG, orthogeriatric; OD, orthopedic department; SD, standard deviation.

Patient survival estimations after hip fracture surgery (FUDays- follow up days), according to hospitalization unit (p < 0.001).
Patient survival estimations after hip fracture surgery, according to hospitalization unit, after propensity matching.
Of the 441 patients included in the study, 257 were transferred to an affiliated nearby geriatric rehabilitation center (107 from the OG group and 127 from the OD group) with the remaining 284 patients released to non-affiliated rehabilitation institutions or continued their rehabilitation at home and were, therefore, lost to follow-up. There was no significant difference in the length of stay (LOS) at the rehabilitation center between groups. Both motor and total FIM scores were lower in the OG group with similar improvement in both groups (Table 3). A matching propensity score was performed for age, functional status, cognitive status, morbidity burden (CCI) and number of medications. One hundred and thirty-three patients remained in each group (Table 4). The incidence of complications did not change after matching, i.e. kidney injury remained more common in the OD group, infections more common in the OG unit. Differences in blood packed cell unit transfusions even heightened after matching. After propensity score matching for referrals to an affiliated rehabilitation center, 68 patients remained in each group. No statistical differences were found in the outcomes between the groups. There was a trend toward better functional improvement among patients from the OG unit, but did not reach statistical significance (Table 5).
Rehabilitation Outcomes.
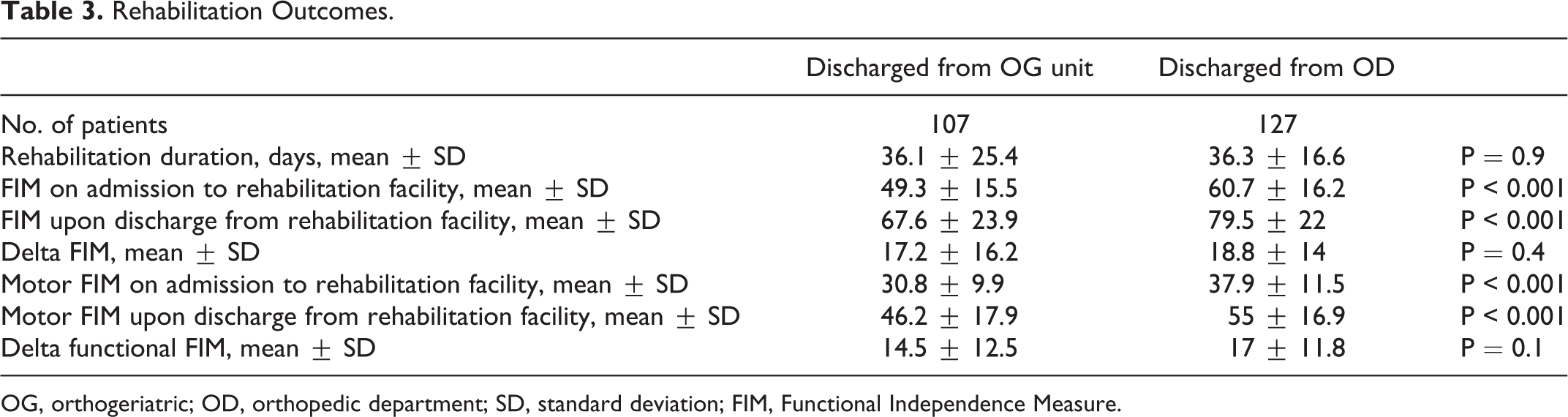
OG, orthogeriatric; OD, orthopedic department; SD, standard deviation; FIM, Functional Independence Measure.
Outcomes After Propensity Score.

OG, orthogeriatric; OD, orthopedic department; SD, standard deviation.
Rehabilitation Outcomes After Propensity Score.

OG, orthogeriatric; OD, orthopedic department; SD, standard deviation; FIM, Functional Independence Measure.
Discussion
Herein, we present outcomes for hip fractured patients who had undergone a surgical intervention and were admitted to an OG unit versus an OD. In 1993, Antonelli et al. found an increased surgical intervention rate, reduced mortality and hospital LOS following a geriatric assessment for older adults in orthopedic wards [6]. Subsequently, more studies reported positive outcomes following geriatric consultations, such as less delirium 7 and lower depression rates, 8 lower discharge rates to long term care facilities 19 and improvement in basic functional status. 8,20 However, other studies did not discern these advantages. 10,21 A systematic review and meta-analysis by Grigoryan et al. found a significant reduction in hospital mortality and LOS in patients hospitalized in OG units, 9 The authors emphasized the need for more data due to the large heterogeneity and lack of variables such as time to surgery, delirium, and functional status limiting the ability to interpret the studies, 9 The cumulative work demonstrating the advantages of a geriatric assessment for elderly patients with hip fractures has led to several models of collaborative orthopedic and geriatric treatments, 9 The optimal model is yet to be determined.
Our study demonstrated a higher 1-year mortality rate in patients who were admitted to the OG unit, mainly due to major baseline differences between the 2 groups, as proved by the loss of statistical significance after the propensity score adjusted for age, functional status, cognitive status, morbidity burden (CCI) and number of medications. Patients in the OG unit were significantly older, more debilitated, more cognitively impaired, with higher CCI scores and were prescribed more chronic medication. Within a year, despite their worst baseline characteristics, mortality in the OG group was 29.2% compatible with other published studies. 22 In contrast, mortality rates in patients admitted to the OD were significantly lower (11.8%). These differences are best explained by a strong selection bias, perhaps due to the tendency of the ER physicians to direct older and sicker patients to the OG unit.
Several differences in postoperative complications were observed. An acute kidney injury was more common in the OD. A possible explanation is a rigorous practice at the OG unit that includes early identification of high-risk patients, improved fluid balance management and cessation of nephrotoxic drugs. Infectious complications were more frequent in the OG unit, predominantly urinary tract infections. Due to the retrospective nature of the study, it is possible that these results were biased due to the under-diagnosis of infections in the OD and over-diagnosis in the OG unit. Moreover, patients in the OG unit had a higher comorbidity burden and were frailer, putting them at a higher risk for infections. Continuity of care is another strong confounder: approximately, 4% of OD patients were transferred during hospitalization to an internal medicine department in order to treat complications, i.e. infections. All patients in the OG unit were treated within the unit until stable enough to be discharged.
LOS was shorter in the OD mainly due to a shorter waiting time for transferring to rehabilitation; due to administrative reasons in our medical center, orthopedic patients were transferred quicker to a rehabilitation facility. Another possible reason is the complexity of the patients in the OG unit leading to longer stabilization periods post-operatively. Patients in the OG unit usually spend one night in the OD, post-op, which is probably the main reason packed cell transfusions are more common in the OD. Stricter adherence to the guidelines for blood products transfusions in the OG unit, may have also contributed to the differences.
Despite the higher complexity of the patients with worse baseline functional capacity in the OG unit, improvement after rehabilitation was surprisingly similar in both groups. We believe this demonstrates the advantages of hospitalizing the patient in an OG unit where treatment and stabilizing frailer, older adults maximizes their chances for a successful recovery after hip fracture surgery. After performing a matching propensity score, mortality rates were similar in both groups, suggesting no significant advantages for hospitalization in the OD. Differences in the incidence of complications remained significant after matching, probably as a result of different treatment approaches and quality of care. After matching, a non-significant trend for better rehabilitation results in the OG unit patients was found. Statistical significance was not reached; however, patient numbers were small. Larger scale studies are needed to shed more light on this issue.
Limitations
The main limitation of this study stems from its retrospective nature. The study was conducted in a single medical center with a unique clinical approach. The distribution of patients between the OG unit and the OD was not random, it was influenced by clinical decisions and available hospital beds at each given time, which led to major baseline differences between the 2 groups. Due to these significant differences, a matching propensity score was performed, allotting only a relatively small sample size. In addition, data regarding rehabilitation outcomes were unavailable for almost 50% of the patients, making the sample size even smaller. With these limitations in mind, despite performing the propensity score, some hidden confounders (such as poor nutritional status), might have added to the bias in disfavor of the OG patients. An ortho-geriatric unit receiving pre-operative hip fractured patients directly from the ER is still rare and therefore, relevant data are scarce. The best treatment modality for the complex, frail geriatric patient is still unclear, rendering this study relevant and clinically important.
Conclusion
This study contributes to the premise that hospitalization within the OG unit offers the older hip fractured patient, a significant contribution regarding pre- and post-operative evaluation and care. We believe our model optimizes the complex geriatric patient’s chances for better recovery and rehabilitation. There is a definite need for larger scale, randomized studies in order to shed light on the question of an optimal treatment setting for hip fractured frail elderly patients.
Supplemental Material
Supplemental Material, sj-docx-1-gos-10.1177_2151459320986299 - Characteristics and Outcomes of Hip Fracture Patients Hospitalized in an Orthogeriatric Unit Versus an Orthopedic Department: A Retrospective Cohort Study
Supplemental Material, sj-docx-1-gos-10.1177_2151459320986299 for Characteristics and Outcomes of Hip Fracture Patients Hospitalized in an Orthogeriatric Unit Versus an Orthopedic Department: A Retrospective Cohort Study by Yulia Bugaevsky, Yochai Levy, Avital Hershkovitz, Irena Ocheretny, Adaya Nissenholtz, Lisa Cooper, Yaara Leibovici Weissman, Avraham Weiss, Steven Velkes and Yichayaou Beloosesky in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Authors’ Note
Yulia Bugaevsky and Yochai Levy contributed equally to this work.
Acknowledgments
The authors thank Mrs. Phyllis Curchack Kornspan for her editorial services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.