
Abstract
Background:
It is important to investigate the level of physical function impairment before fracture to predict mortality after hip fracture. This study aimed to examine the predictive factors associated with mortality depending on prefracture physical function impairment among Korean elderly patients.
Methods:
We included 1841 patients aged 65 years and older with hip fractures using osteoporosis-related hip fracture network data from 15 university hospitals in South Korea. The collected data included sociodemographic, nutritional, disease-related, and fracture- and surgery-related factors. For the degree of prefracture physical function impairment, ambulatory ability was classified into community, household, and nonfunctional ambulators. Binominal logistic regression was used to identify the predictive factors for mortality.
Results:
Analysis showed that mortality rate at the first follow-up after hip fracture was 4.9%, and most patients (77.7%) were community ambulators before fracture. Sociodemographic (older age, male sex), nutritional (low body mass index, low albumin level before surgery), and fracture- and surgery-related (nonsurgical management, complications after surgery) factors significantly predicted mortality, depending on the prefracture ambulatory status.
Conclusions:
This study emphasizes that nutritional assessment and management as interdisciplinary interventions from hospitalization to follow-ups should be performed to lower malnutrition and mortality risk. Therapeutic management for comorbidities negatively affecting surgery outcomes should be prioritized to reduce postoperative complications and mortality. Surgical treatment should be encouraged if it aligns with the therapeutic goals, even in poor health status.
Introduction
The prevalence of hip fracture is increasing with the increase in the elderly population. 1,2 However, hip fracture surgery is associated with functional deterioration 3,4 as well as high mortality and morbidity 5,6 in elderly individuals. After hip fracture surgery, the rates of inpatient, 30-day, 90-day, and 1-year mortality in all age groups were 3.3% 7 , 11% 8 , 3.7% 5 , and 20% 8 , respectively; on the other hand, recent studies reported that 1-year mortality in the elderly is much higher, ranging from 27% to 34%. 8,9 The high mortality among elderly individuals with hip fractures has been attributed to demographic factors such as age, sex, body mass index (BMI), and residence status before fracture 5,7,8,10 –15 ; disease-related factors such as general health status, cognitive impairment, and comorbidity; 6 –8,10,12 and fracture- and surgery-related factors such as type of fracture, nonsurgical management, time from fracture to surgery, and postoperative delirium. 6,10,12
Prefracture physical function impairment has been identified as a predictor of 6-month mortality after surgery. 6,13,14 Most elderly adults with hip fractures have osteoporosis and multiple comorbidities, 15 and osteoporosis, with its close association with sarcopenia, increases the risk for hip fracture. 16,17 In a previous study, 18 mortality was significantly higher among elderly patients with hip fractures accompanied by sarcopenia and physical function impairment than among those with hip fractures accompanied by sarcopenia and various other comorbidities, highlighting the importance of physical function impairment. Because elderly individuals with more severe physical function impairment before fracture develop more catastrophic functional impairment after fracture, 19 it is essential to examine the degree of prefracture physical function impairment to predict mortality after hip fracture. 18
However, prefracture physical function impairment has a greater effect on postoperative physical functional recovery than on postoperative mortality, 20 and few studies have examined predictive factors for mortality. 13 Therefore, whether elderly individuals with physical function impairment before fracture are actually more likely to affect mortality after hip fracture remains unclear. Considering that physical function impairment is a major determinant of mortality in advanced age, 18 the assessment of ambulatory status to identify physical function impairment is likely to be reasonable and rather easier to evaluate visually. Moreover, as most prior studies were performed in Western countries, there are racial and cultural differences between their subjects and Korean elderly patients. These differences, in addition to the varying health-care environments and systems across countries, give rise to the need for additional studies to verify the external validity of the factors found to affect mortality. In addition, studies on mortality after hip fracture in Korean elderly patients 12,21 were conducted on a small number of subjects from a single hospital. Examining mortality after hip fractures among the elderly would ultimately contribute to lowering the mortality and developing better intervention strategies.
In this context, this multicenter study aimed to examine the predictive factors associated with mortality in relation to the level of prefracture physical function impairment among Korean elderly patients. The findings of this study would serve as a foundation for developing ongoing interventions that can lower mortality.
Materials and methods
Study design and ethical considerations
This multicenter prospective cohort study was approved by the institutional review board (KNUH 2014-07-008-001), and written consent was obtained from all patients before the study.
Participants and data collection
The study used osteoporosis-related hip fracture network data from 15 university hospitals, for a total of 2043 adults aged ≥50 years who had hip fracture by low-energy trauma, excluding pathological fracture and motor vehicle accident-related fracture between August 2014 and May 2016. After excluding 196 adults aged <65 years and 6 adults with incomplete medical records, a total of 1841 patients were enrolled in this study. Data were collected immediately after admission, during surgery, postoperatively, and at the first follow-up after discharge. Subject assessment and data collection were conducted according to the guidelines at each of the 15 university hospitals.
The collected data included patient gender, age, prefracture residence status, degree of prefracture physical function impairment, BMI, preoperative albumin levels, dementia, number of comorbidities, general health status, fracture location, cause of fracture, companion fracture, refracture, type of surgery, time from admission to surgery, surgical management, operation time, estimated blood loss, length of stay (LOS) in hospital, postoperative complications, and mortality in the first follow-up. Prefracture residence status was categorized into home, nursing home, hospital, and others, and data were collected from the elderly patients and their caregivers by a trained interviewer in each university hospital. For the degree of prefracture physical function impairment, ambulatory status was assessed by a trained interviewer according to the guideline by Koval et al., 22 which classified individuals into community, household, and nonfunctional ambulators, on the basis of seven ambulatory abilities. In a recent study, 19 Salpakosk et al. mentioned that it is important for even ambulators with walking limitations to walk around the community to maintain physical function. This may be in line with our assumption that community ambulators with even walking aids have a lower mortality risk than others. Therefore, we assessed the elderly patients on the basis of the following criteria: one point for community ambulator to walk indoors and outdoors either independently or with an assistive device; two points for household ambulator to walk indoors, independently or with an assistive device; and three points for nonfunctional ambulator to not walk at all with even an assistive device. BMI and albumin levels were measured to assess nutritional status. The presence of dementia was determined based on Diagnostic and Statistical Mental Disorders, 5th edition 23 criteria. The number of comorbidities was determined by reviewing medical records and by interviewing the patients and caregivers. General health status was assessed using the American Society of Anesthesiologists (ASA) score. Fracture location, cause of fracture, companion fracture, and refracture were determined by reviewing medical records. Type of surgery, time from admission to surgery (days), operation time, and estimated blood loss were determined from the operative records. For the postoperative hospitalization period, data on LOS in hospital were collected from medical records. Information on whether surgery was performed and the presence of postoperative complications was also collected from medical records and recorded as “yes” or “no.” At the first follow-up after discharge, mortality was determined based on outpatient visit or via telephone inquiry and recorded as “yes” or “no.”
Statistical analysis
All analyses were performed using SPSS 25.0 software (Chicago, Illinois, USA). Categorical variables were presented as real numbers and percentages, and continuous variables were presented as means and standard deviations. Differences between survivors and deceased patients were compared using the t-test and χ 2 test. For the identification of predictive factors of mortality and the influence of the degree of prefracture physical function impairment, we entered all variables that were significantly associated in bivariate analysis into a binominal logistic regression. In the logistic regression analysis, the first category was set as the reference variable for categorical variables. Statistical significance was set to 5%.
Results
A total of 1841 individuals were enrolled in this study and consisted of 1431 (77.7%) community ambulators, 343 (18.7%) household ambulators, and 67 (3.6%) nonfunctional ambulator (Table 1). The mean ages were 79.77 ± 7.05, 79.05 ± 6.94, 82.40 ± 6.91, and 81.66 ± 6.41 years for the total participants and the community, household, and nonfunctional ambulators, respectively. Most patients lived at home before fracture in all groups. The mean BMI (21.97 ± 3.44 kg/m2) and the albumin level (3.56 ± 0.57 g/dL) were the highest for the community ambulators. The mean number of comorbidities was the highest at 3.31 ± 1.78 for the nonfunctional ambulators. More than half of the household and nonfunctional ambulators had an ASA score higher than 3. Among the nonfunctional ambulators, 29.9% of patients were diagnosed with dementia before fracture.
Baseline characteristics of total participants.

M ± SD, mean ± standard deviation; BMI, body mass index; ASA, American society of anesthesiologists; LOS, length of stay.
Fracture location, reason of fracture, companion fracture, and types of surgery were similar between the groups. The refracture rate was the highest at 16.4% for nonfunctional ambulators. The average time from admission to surgery was about 3.31 days for community ambulators, compared to about 5.09 and 4.81 days for household and nonfunctional ambulators. Of the total participants, 1.8% did not undergo surgery. Operation time, LOS in hospital, and postoperative complications were the lowest for community ambulators. A total of 91 patients (4.9%) died by the first follow-up, and mortality was the highest among nonfunctional ambulators 11.9%.
Table 2 presents the association between mortality and patient characteristics. Among the total participants, sociodemographic factors significantly associated with mortality were gender and age. Nutritional characteristics associated with mortality were BMI and albumin level. Disease-related characteristics significantly associated with mortality were the number of comorbidities, ASA score, and dementia. Fracture- and surgery-related factors included surgical treatment, operation time, and postoperative complications. In the community ambulators, age as a sociodemographic factor was associated with mortality. Nutritional and disease-related characteristics significantly associated with mortality were albumin level and the number of comorbidities. Fracture- and surgery-related factors included time from admission to surgery, surgical treatment, and postoperative complications. In the household ambulators, gender, BMI, number of comorbidities, ASA score, surgical treatment, and postoperative complications were associated with mortality. Companion fracture was associated with mortality in the nonfunctional ambulators.
Relationships between mortality and patients’ characteristics.

BMI, body mass index; ASA, American society of anesthesiologists; LOS, length of stay.
a χ 2 test.
b t-test.
c p < 0.05.
d p < 0.001.
e p < 0.01.
The variables significantly associated with mortality were entered in a logistic regression model to identify predictive factors for mortality (Table 3). The results showed that gender, age, BMI, albumin level, and postoperative complications were significant predictive factors for mortality among the total participants. Male gender (odds ratio (OR) 1.81, confidence interval (CI) 1.07–3.04) and older age (OR 1.05, CI 1.01–1.08) resulted in an increased risk of mortality. Low BMI (OR 1.72, CI 1.04–2.84) and albumin level (OR 2.87, CI 1.75–4.70) were associated with higher risks of mortality. Absence of complications after surgery (OR 0.14, CI 0.08–0.23) were observed to decrease the risk of mortality. In the community ambulators, the results showed that older age (OR 1.05, CI 1.00–1.10), low prefracture albumin level (OR 3.57, CI 1.84–6.94) were predictive factors to increase mortality, whereas absence of complications after surgery (OR 0.13, CI 0.06–0.25) were decreased predictive factors for mortality. Male gender (OR 2.51, CI 1.11–5.67), in addition to low BMI (OR 1.98, CI 0.92–4.27), nonsurgical treatment (OR 0.06, CI 0.01–0.25), and complications after surgery (OR 0.20, CI 0.08–0.46), was a predictive factor for mortality among patients who were household ambulators before surgery. There were no predictive factors for mortality among nonfunctional ambulators.
Binomial logistic analysis of mortality according to prefracture ambulatory status.
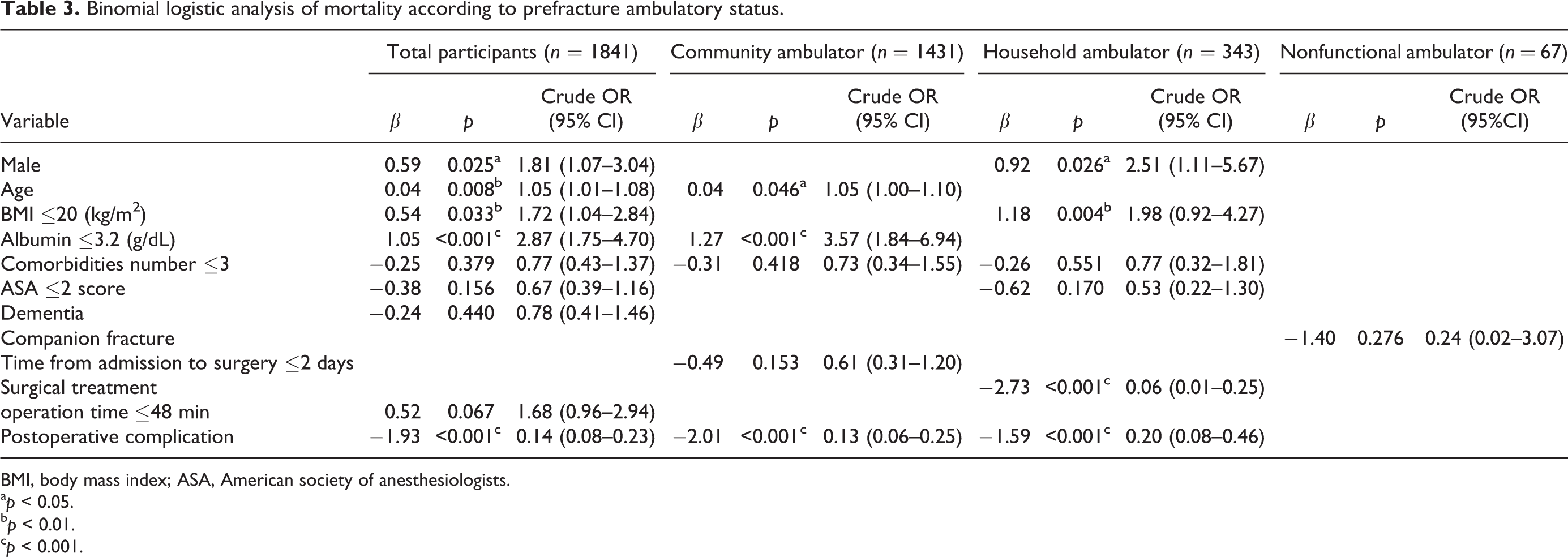
BMI, body mass index; ASA, American society of anesthesiologists.
a p < 0.05.
b p < 0.01.
c p < 0.001.
Discussion
In contrast to the extensive literature on age, gender, and disease-related factors associated with mortality in elderly patients with hip fractures, few studies have investigated physical function impairment in relation to mortality. In this study, we identified the predictive factors for mortality in the total patients and identified the predictive factors for mortality after classifying the patients according to the degree of prefracture physical function impairment. Mortality rate at the first follow-up was 4.9%, and most patients (77.7%) were community ambulators before fracture.
In our study, gender and age were predictive factors for mortality for the entire elderly patient cohort. Age 5,6,8,12 and male gender 5,6,8,10,12 are well-known factors associated with mortality, and the results of our study were consistent with those of other studies. Prefracture residence status was not associated with mortality; although this contradicts some previous reports, 6 –8 it is similar to the findings of a study that analyzed 1-year mortality after hip fracture among elderly persons living in nursing homes in Korea. 21 In our study, the vast majority of the elderly patients lived in their homes before fracture, and only a few of them lived in a nursing home or a hospital. In addition, although living in a nursing home is a factor that increases mortality in other countries, the same is not evident in Korea, suggesting that differences in policies and environmental factors may be present. Thus, future studies should compare and analyze the differences in mortality between elderly persons living in nursing homes in Korea and other countries.
In an analysis of the predictive factors affecting mortality among the total population, low BMI and albumin level, and complications after surgery were also significant predictive factors for mortality. Contradictory results pertaining to the association between nutritional status and mortality were reported in previous studies. Whereas a prior study 13 reported that BMI and albumin level were not significantly associated with 6-month mortality in elderly patients (aged >85 years) with hip fracture, another study 6 reported that elderly patients with a BMI >30 kg/m2 showed a higher 12-month mortality, contrary to our findings. In the present study, mortality was clearly higher among elderly patients with poor nutritional status, similar to the findings of a previous study of 2517 elderly inpatients in which early mortality was 1.56 times more common among the nutritional risk and malnutrition groups. 24 Most elderly persons with hip fractures (60–70%) are malnourished 17 ; however, few studies have investigated the association of nutritional status with mortality. These findings emphasize the need for interdisciplinary interventions that include nutritional assessment and management from hospitalization to follow-ups to reduce malnutrition and mortality.
Although all disease-related factors were associated with mortality, these were not significant factors for mortality. This result was in contrast with previous findings. 8,11,12,25,26 In contrast to our study, all previous studies investigated 12-month or longer-term mortality after fracture and surgery. In another study, 5 the sample was limited to elderly patients who underwent total hip replacement for a hip fracture, and comorbidities and preoperative status had significant effects on 90-day mortality after surgery. Hence, this study also involved a different sample and follow-up period for mortality. Further studies should be performed to specifically identify the comorbidities in elderly patients with hip fractures and to examine the severity to predict mortality.
Except complications after surgery, fracture- and surgery-related factors were not predictive of mortality. Although the results pertaining to type of fracture and surgery were similar to previous findings, 8,25,26 a meta-analysis review study 6 reported that femur neck fracture was associated with a significantly higher mortality than other types of proximal femur fractures, necessitating additional studies on the type of fracture. Time from admission to surgery of 2 days was also not a predictor of mortality among the participants. These results contradicted a previous study 12 indicating that patients who had surgery within 2 days had significantly lower mortality rates than those who did not. We did not identify the specific reasons for surgery delay. However, therapeutic management might have preceded surgery, considering that most patients had more than two underlying diseases and three ASA scores. Examination and treatment of comorbidities affecting surgery may be necessary before surgery. 12 Further studies are needed to determine the effect of time from admission to surgery on mortality. Mortality was considerably lower among elderly patients who had no complications after surgery, as reported in previous studies. 8,26 Complications after surgery are intimately associated with age and comorbidities in elderly patients with hip fractures. 26,27 Although factors associated with complications are not preventable, the therapeutic management of comorbidities affecting negatively surgery outcomes should be prioritized to reduce postoperative complications and mortality.
The participants were divided according to their prefracture ambulatory status to identify the predictive factors associated with mortality in each group. In the community ambulators before fracture, older age, low albumin level before surgery, and complications following surgery were significant predictive factors for mortality. Meanwhile, gender, low BMI, nonsurgical treatment, and postoperative complications were predictive factors for mortality subject to intervention in the household ambulator group. While older age was not a predictive factor, male gender was a predictive factor in the household ambulator group. The considerably higher mortality rate among men in this group may be attributable to the fact that male patients with more comorbidities were already in poorer condition before fracture compared with female patients. 28 The severity of these comorbidities would have had an adverse effect on their prefracture physical function status, 29 which might reflect considerable mortality risk. Therefore, the gender of the patient should be considered when predicting mortality in the elderly with more severe physical function status before fracture. Older age was a predictive factor in the community ambulators and should be considered to predict mortality in this group.
Low albumin was a predictive factor for the community ambulators, while low BMI was a predictive factor for the house ambulators. Nutritional indicators including BMI and albumin are likely to increase mortality. However, a previous study reported 30 that partial nutritional indicators create difficulties in accurately identifying nutritional status. Correct nutritional assessment must be considered to identify whether nutritional status is an exact predictive factor for mortality. Nonsurgical treatment was a predictive factor among household ambulators, similar to results in a previous study. 10 Patients with severe comorbidities inevitably cannot undergo surgical treatment. 10 Clinicians should emphasize the importance of surgery and encourage it among elderly patients and caregivers if it aligns with therapeutic goals, even though patients are in poor health. Our study could not identify whether nonsurgical treatment was a factor affecting mortality among total and community ambulators because the number of nonsurgical treatments was relatively small in these groups. This study suggests that further research is needed on nonsurgical treatment to increase mortality.
There are no factors associated with mortality in nonfunctional group in this study. Previous studies 15,16 have reported that physical function impairment itself significantly affects mortality; however, few studies identified predictive factors for mortality in elderly patients with the most severe physical function impairment. A possible explanation is that the number of nonfunctional ambulators included in this study was relatively very small and especially, <10 of them died, which might restrict accurate analysis. In the future, it is necessary to evaluate the mortality in patient with nonfunctional status.
There are several limitations in this study. Firstly, our findings may have low objectivity and internal validity because prefracture functional impairment was determined solely on the basis of ambulatory status. Secondly, the follow-up period varied across patients, with the study period limited from admission to the first outpatient follow-up. Thirdly, we could not specifically examine the types and severity of comorbidities, and the results pertaining to mortality in relation to comorbidity should be interpreted with caution. Finally, enrolled patients with hip fracture were treated in university hospitals, causing selection bias. However, this study is the first multicenter study, to the best of our knowledge, to analyze mortality, and it is expected to contribute to identifying mortality and predictive factors among Korean elderly patients with hip fractures. Furthermore, by classifying patients according to the degree of prefracture physical function impairment, our study has implications in making treatment plans.
Conclusions
This study found that mortality rate in the first follow-up after hip fracture was 4.9% and 77.7% of elderly patients were community ambulators before fracture. Sociodemographic (older age, male sex), nutritional (low BMI, preoperative low albumin level), and fracture- and surgery-related (nonsurgical management, complications after surgery) factors significantly affected mortality depending on the prefracture ambulatory status. Therefore, the factors that were found to affect mortality should be reflected in treatment plans, and controllable factors should be actively managed to reduce mortality. This study emphasizes that controllable factors affecting mortality should be actively managed. Nutritional assessment and management as interdisciplinary interventions from hospitalization to follow-ups should be performed to lower malnutrition and mortality risk. Therapeutic management for comorbidities negatively affecting surgery outcomes should be prioritized to reduce postoperative complications and mortality. Surgical treatment should be encouraged if it aligns with the therapeutic goals, even in poor health status.
Footnotes
Acknowledgements
We thank Dr. Jae Suk Chang, Dr. Jae-Kwang Hwang, Dr. Kwang-Hwan Jung, Dr. Beon Jung Kang, Dr. Ji Wan Kim, Dr. Ki-Choul Kim, Dr. Tae-Young Kim, Dr. Young-Kyun Lee, Dr. Kyung-Sun Park, Dr. Yong-Geun Park, Dr. Hyun-Chul Shon, Dr. Sang-Heon Song, Dr. Kyu-Hyun Yang, for their assistance with the collection of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT, and Future Planning (NRF-2017R1C1B5075973).