
Abstract
Introduction
Lateral mass screws are widely used in the sub-axial cervical spine but have poor pullout strength and result in a screw tulip that is medial, which limits both rod passage to nearby pedicle screws and the ability to centrally decompress the canal after screw placement. True pedicle screws have the highest pullout strength, but carry neurovascular risk. The cervical pedicle inlet (CPI) trajectory is a novel technique that involves a lateral starting point similar to a true pedicle screw, but the tip of the screw stops in the dense bone at the pedicle inlet, thus limiting neurovascular risk. Prior biomechanical studies have demonstrated increased pullout strength relative to lateral mass (LM) screws, but no clinical series have been published. The purpose of this study is to provide a preliminary clinical report on the radiographic and safety profile of this novel screw trajectory.
Methods
We retrospectively reviewed 388 screws placed from C3-7 from 64 consecutive cases of cervico-thoracic fusion from a single surgeon at a single center. All patients were ≥18 years and underwent posterior cervico-thoracic fusion with navigated CPI screw placement in the sub-axial cervical spine between 2020 and 2025. Intra-operative CT scans were available on all patients and were used to classify breaches with a modified Gertzbein-Robbins scale. Screws that were completely in bone were graded as “0,” those with a 1-2 mm breach were graded as “1,” and screws with > 2 mm breach and that were removed or repositioned intra-operatively were graded as “2.”
Results
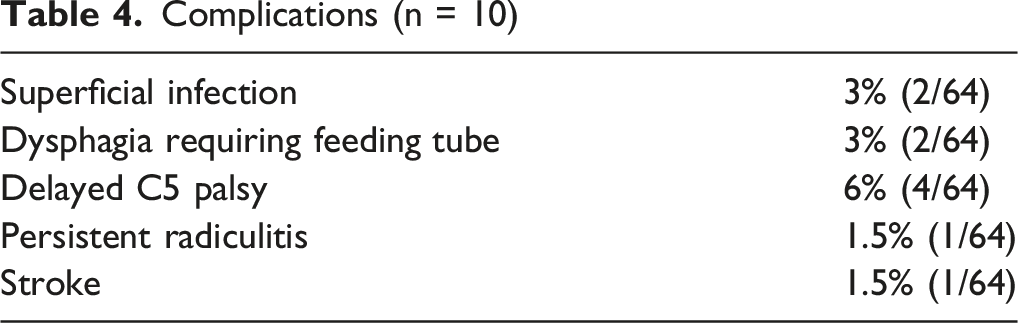
A total of 388 screws were placed. (292 CPI, 47 LM, 49 pedicle). For the CPI screws, 79% (232/292) were grade 0 (completely in bone), 18% (54/292) were grade 1 (1-2 mm breach), and 2% (6/292) were grade 2 (removed or repositioned intra-operatively). For the LM screws, 72% (34/47) were grade 0, 28% (13/47) were grade 1, and 0% (0/47) were grade 2. For pedicle screws, 61% (30/49) were grade 0, 29% (14/49) were grade 1, and 10% (5/49) were grade 2. CPI screws were more likely than LM or pedicle screws to be grade 0 (P < 0.01). Ten patients experienced some type of early post-operative complication, including delayed C5 palsy (6%, n = 4), superficial infection (3% n = 2), dysphagia (3%, n = 2), or other (3%, n = 2). There were no cases of return to OR for screw malposition or neurovascular injury related to screw placement, and no cases of CPI screw pullout or loosening within 6 months of surgery.
Conclusion
The use of navigation allows for safe screw placement along the CPI trajectory, with no recorded screw related complications. For patients with cervical pedicles that are too small to accept a true pedicle screw, the CPI trajectory is a reasonable alternative.
Introduction
Posterior cervical fusion is a widely used surgical technique for treating a variety of cervical spine pathologies, including deformity, degenerative disease, and instability.1-3 Stable fixation is essential for achieving fusion and preventing hardware-related complications, but the optimal method of screw placement remains debated.3,4 Pedicle screw fixation offers the strongest biomechanical purchase, yet its use is restricted by narrow pedicle morphology, high rates of cortical breach, and risk of neurovascular injury,1-7 Thus, surgeons need an alternative to pedicle screws because many pedicles are simply too small to allow for safe placement.
The traditional alternative has been lateral mass (LM) screws, which have a long history and excellent safety profile,1,3,4 but limited biomechanical strength.2,3,5 Furthermore, the medial tulip head of the lateral mass screw makes passage of a rod more difficult in constructs where both pedicle and lateral mass screws are nearby (Figure 1). Lastly, the medial tulip head limits the opportunity for placement in MIS or percutaneous cases, and can interfere with central decompression of the canal after the implant is placed.
4
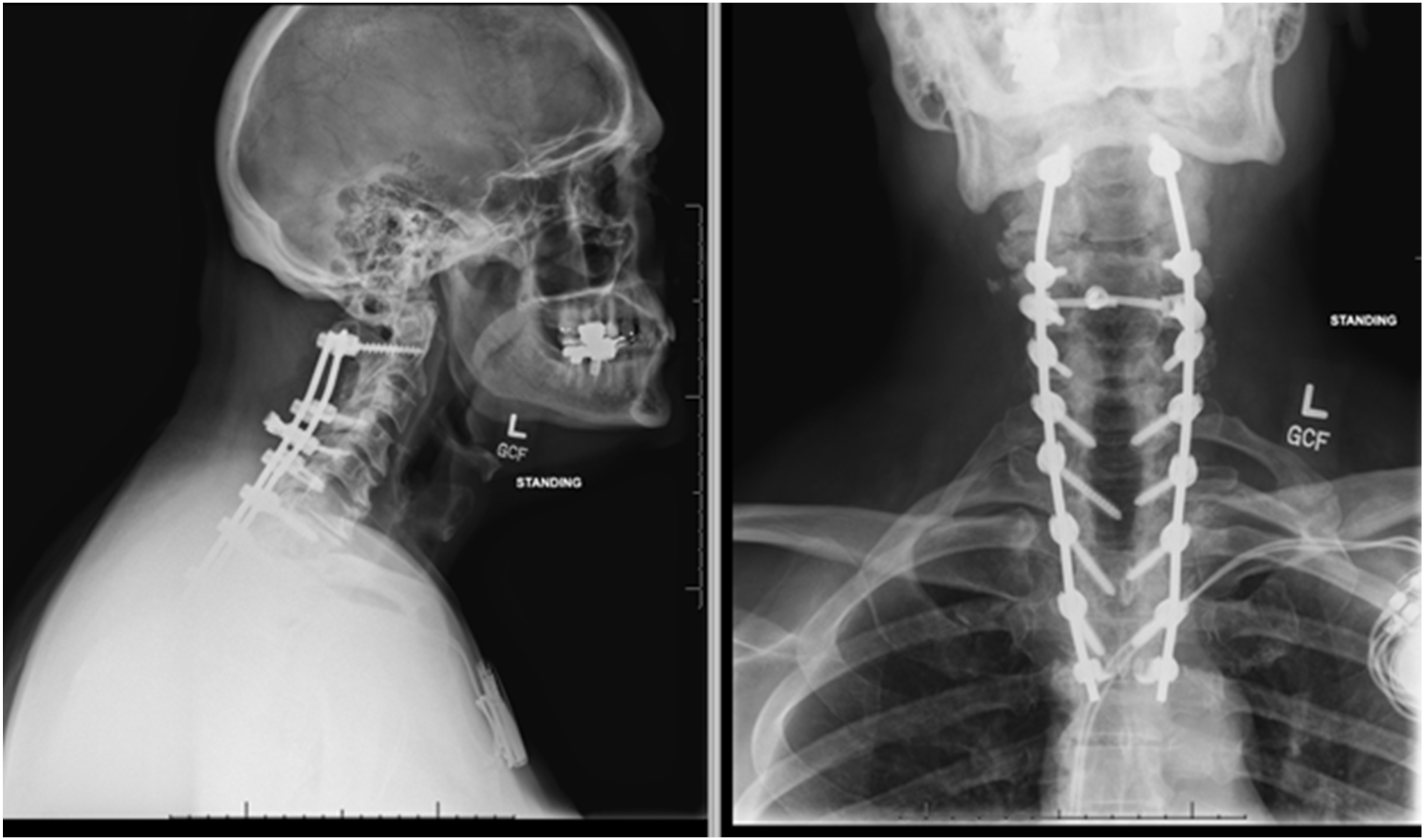
Pre-operative lateral (left), post-operative lateral (center), and post-operative AP radiograph showing cervicothoracic fusion with C2 and Thoracic pedicle screws, and sub axial (C4-6) pedicle inlet screws. C3 and C7 are un-instrumented to decrease implant density
The cervical pedicle inlet (CPI) screw trajectory (Figure 2) has been proposed as an alternative technique that balances safety and strength by targeting the dense bone of the pedicle inlet for screw purchase, but avoids the neurovascular risk associated with traversing the pedicle.2,4 Furthermore, the lateral tulip position facilitates rod passage in long constructs (Figures 1 and 3). Early biomechanical investigations suggest that CPI screws offer enhanced pullout strength and lower risk of malposition compared with conventional constructs.
2
However, only limited case reports exist of their use, and to our knowledge there are no prior case series in open cervico-thoracic constructs.
4
This study aims to address this knowledge gap by presenting the radiographic results in patients undergoing multi-level posterior cervico-thoracic fusion from a single surgeon at a single center. Diagram of pedicle inlet screw trajectories. The screw starts on the supero-lateral aspect of the lateral mass and ends with the tip in the dense bone of the pedicle inlet. Green lines represent possible trajectories for reaching the pedicle inlet AP and lateral radiographs showing pedicle inlet screws placed from C4-6 bilaterally. The screw tulips line up with pedicle screws placed at C2 and in the thoracic spine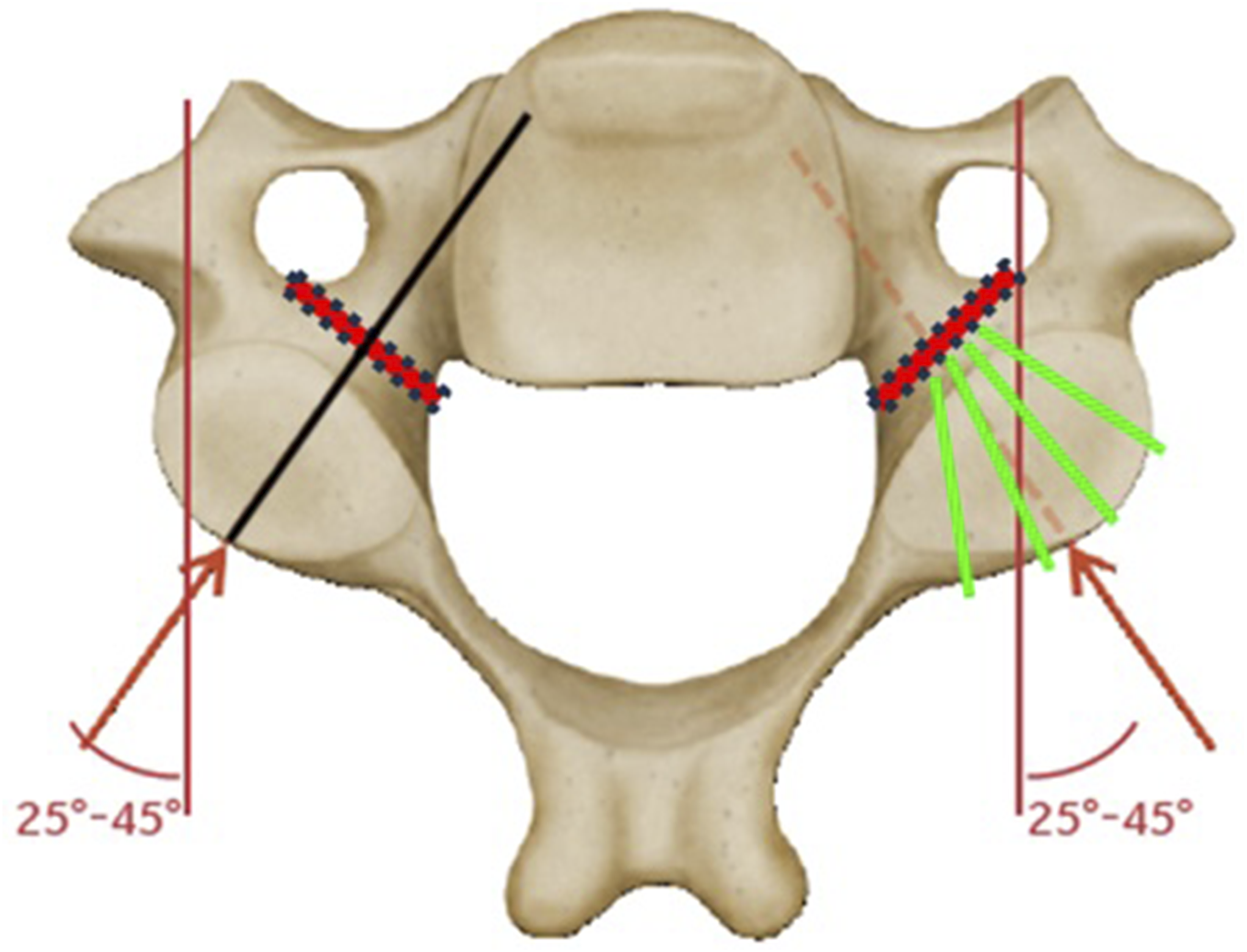
Methods
Study Design and Patient Selection
We conducted a retrospective review of prospectively collected data from patients who underwent posterior cervicothoracic fusion using the cervical pedicle inlet (CPI) screw trajectory between 2020 and 2025 at a single institution. Inclusion criteria were: age ≥18 years, cervical or cervicothoracic fusion for degenerative or deformity indications and availability of intraoperative O-arm 3D imaging to confirm screw trajectory. Patients were excluded if surgery was performed for trauma, fracture, or infection. In all included cases, the CPI screw trajectory was used for at least one level in the sub-axial spine (C3-7).
Selection of Screw Type
The author used true pedicle screws at the C2 and thoracic levels, 8 and these screws were not included in the analysis. In addition, the author typically leaves several of the sub-axial cervical levels un-instrumented to decrease implant density, and thus the total number of screws placed is less than the number of levels in the construct. CPI are typically placed in the sub-axial cervical spine from C3-6 (Figure 3). In these locations, the cervical pedicle size is often quite small, with prior systematic reviews indicating that 20-40% of cervical pedicles are not accessible. In the author’s practice, cervical pedicle screws are placed from C3-6 rarely, and only when specific criteria are met. These include: a pedicle diameter larger than 4 mm in diameter, vertebral artery contained in the foramen with no aberrancy or encroachment on the pedicle, and when the wound is shallow such that the lateral-to-medial trajectory of the pedicle is not impeded by the soft tissue envelope. The intra-operative CT scan is assessed for these criteria at each level, and if the pedicle is accessible, a true pedicle screw is placed. 9 If the pedicle is unsafe, or even borderline, then the author errs on the side of safety and places a CPI screw. Typical CPI screw lengths were 14-18 mm, and 3.5 mm in diameter. The intra-operative CT scans were used to verify that the case included CPI trajectories, and only cases with sub-axial CPI screws from C3-6 were included in this cohort. In the early part of the senior author’s practice adopting this technique, lateral mass screws would also be mixed into the construct. This is no longer standard practice, but these screws were also included in the analysis presented here to provide a point of comparison.
Surgical Technique
The patient is positioned prone with a Mayfield head holder and prepped and draped in the usual fashion. After a standard midline exposure, a reference frame is attached to the thoracic spinous process. The O-Arm (Medtronic, Memphis, TN), is used to obtain an intra-operative CT scan and the Stealth Navigation System (Medtronic, Memphis, TN) is registered to the patient anatomy. After appropriate verification of registration accuracy, screws are placed in the following fashion: The navigated clawfoot is used to identify the starting point, typically on the supero-lateral aspect of the lateral mass (Figure 2), and the point is marked with the burr. A navigated drill, set at a depth of 14 mm, is used to cannulate a track towards the pedicle inlet (Figure 4). A ball-point probe palpates the track, which should be solid throughout in bone. If the endpoint is soft then navigation accuracy is re-assessed. A 3.0 mm navigated tap is used to tap the full length of the screw track into cortical bone, which is typically 16-18 mm. The track is palpated again, and if the endpoint is soft then a shorter screw length is chosen. A 3.5 mm screw is then placed. After placement of all implants, the O-Arm is brought back in for a verification spin and the screw positions are closely scrutinized. Screws with less than 1-2 mm of cortical breach are left in place. For screws with > 2 mm of cortical breach, the surgeon assessed the intra-op CT scan for an alternative bony corridor. If the bony anatomy allowed, a new screw was placed. If no safe corridor remained, the screw was removed and left out of the construct. A description of each removed or repositioned screw was recorded by the radiographic reviewers. Axial CT scan showing pedicle inlet trajectory which stops short of critical neurovascular anatomy at the mouth of the pedicle (L) compared to a true pedicle screw (R) which traverses into the vertebral body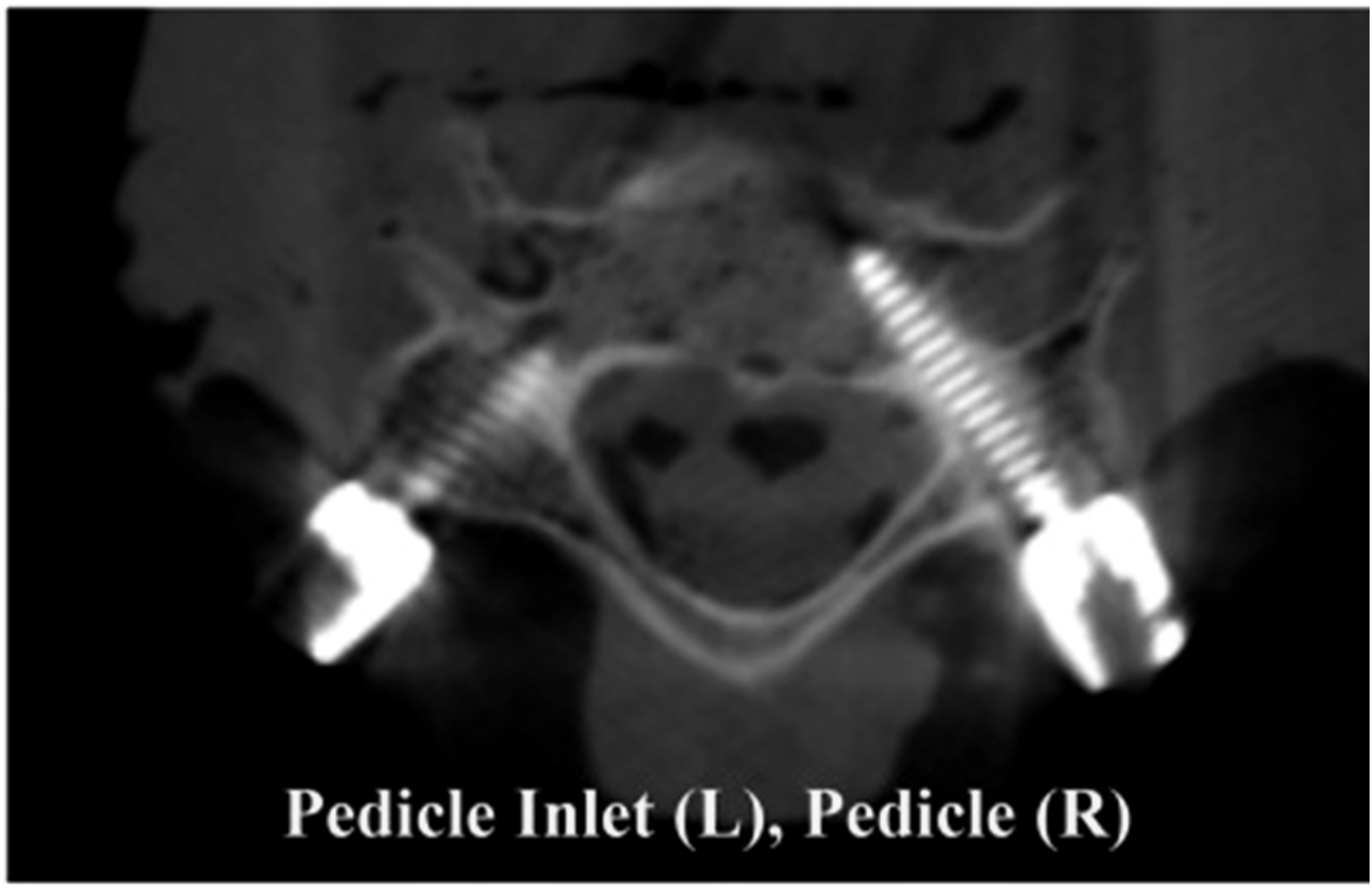
Data Collection
Demographic variables included patient age, sex, and body mass index (BMI). Surgical variables included number of levels fused, levels instrumented, and number of screws placed. Surgical indications were also recorded.
The primary outcome of interest was the prevalence of CPI, LM, and pedicle screw breach/malposition. We also collected information on intraoperative screw repositioning rate, and peri-operative mechanical complications within 6 months of surgery; including screw loosening, rod breakage, and need for return to OR for screw related complications. Given the purpose of this study is to report on the initial safety and feasibility of CPI screw placement, we did not report long term follow-up measures such as patient reported outcomes, alignment outcomes, or pseudarthrosis rates.
Screw breaches were classified using a modified Gertzbein-Robbins 10 scale applied to intraoperative O-arm imaging. Grade 0 was defined as the screw completely contained within the bone with no cortical breach. Grade 1 was defined as cortical breach </ = 1-2 mm. Grade 2 was defined as cortical breach >2 mm requiring repositioning. For comparison, we also graded all lateral mass and pedicle screws placed in these cases. We defined a CPI screw as any screw that starts on the lateral portion of the lateral mass and was directed medially toward the mouth of the pedicle, but did not traverse into the vertebral body. A lateral mass screw was defined as starting medial on the lateral mass and being directed laterally away from the neurovascular anatomy. A pedicle screw was defined as any screw that traversed the pedicle and entered the vertebral body. Screw grading was performed by a fellowship trained spine surgeon who was not involved in the index surgery. For an assessment of reliability, a second reviewer independently graded the screw accuracy, and inter-observer correlation coefficients were calculated.
Statistical Analysis
All statistical analyses were performed using SPSS version 28.0 (IBM Corporation, Armonk, NY). Continuous variables were summarized as means ± standard deviation, and categorical variables as frequencies and percentages. Descriptive statistics were used to determine the prevalence of screw breach, repositioning, mechanical and biologic failure, and postoperative complication rates.
Results
Demographics
Demographics
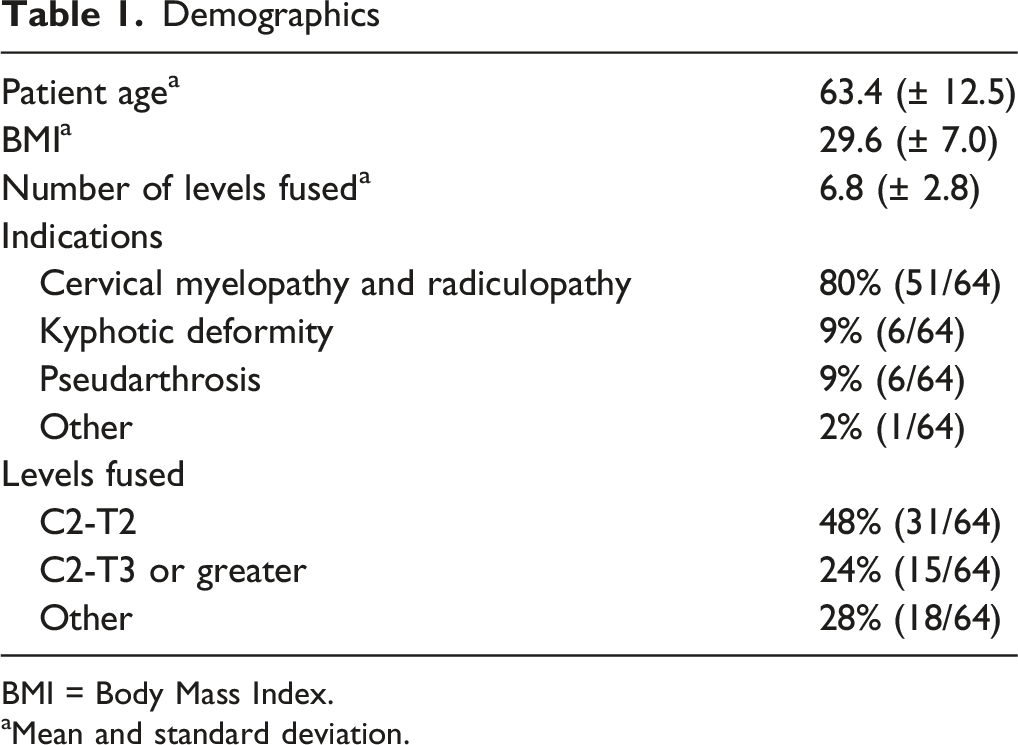
BMI = Body Mass Index.
aMean and standard deviation.
Overall Breach Rates and Screw Accuracy
CPI Screw Grading* versus Lateral Mass and Pedicle Screw Grading

CPI = cervical pedicle inlet: mm = millimeter. *Modified gertzbein-robbins scale.
Grade 2 Screws
All screws with more than 2 mm of breach that risked endangering neurovascular structures were identified intra-operatively on the check spin with the O-arm and were revised (Table 2). There were no such cases of LM screws. Two 0.7% (2/292) CPI screws were breached more than 2 mm into the vertebral foramen, and each was removed with no arterial injury, and no case of stroke from screw placement. 1.4% (4/292) of the CPI screw were breached more than 2 mm into the neural foramen. Of these, 3 were removed, and 1 was exchanged to a shorter screw, with no case of neural injury from CPI screw placement. 10% (4/49) of the pedicle screws were breached more than 2 mm into the vertebral foramen. Each of these was removed and converted to a pedicle inlet screw by replacing with a shorter screw in the same tract. There was no arterial injury in any case and no case of stroke from pedicle screw placement. 1 pedicle screw was breached more than 2 mm into the neural foramen and was removed from the construct with no post-operative deficit.
Interrater Reliability
Interrater Reliability Breach Agreement
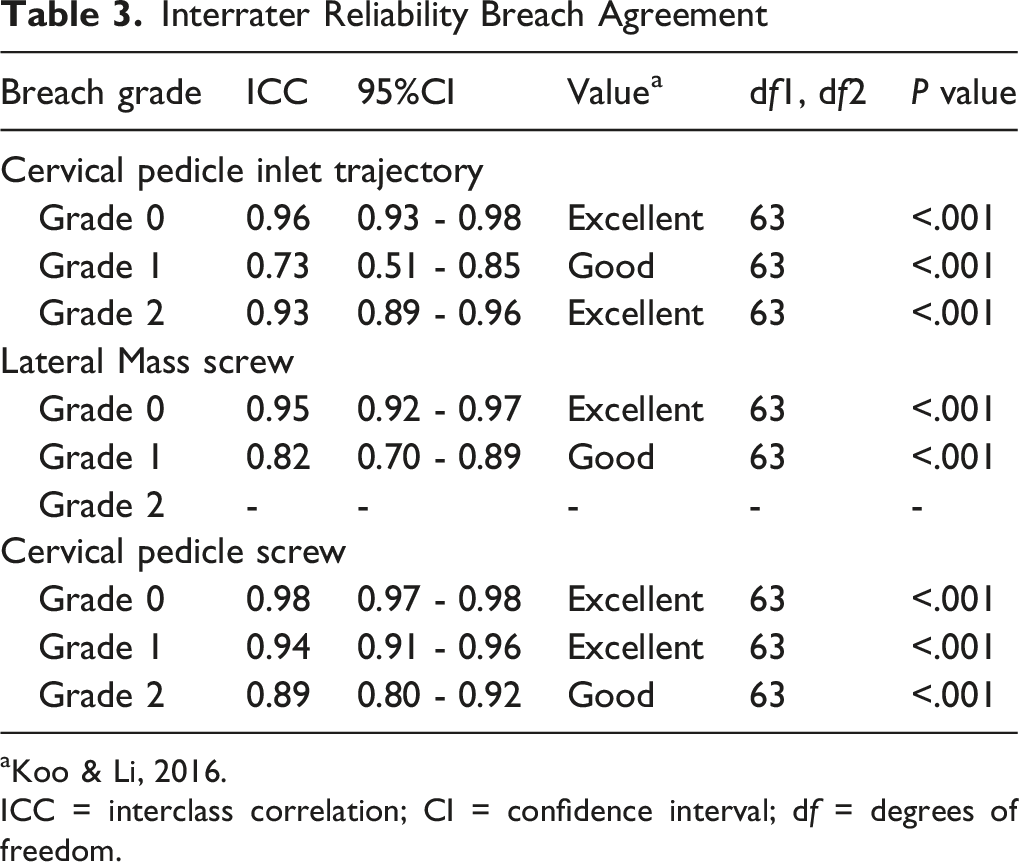
aKoo & Li, 2016.
ICC = interclass correlation; CI = confidence interval; df = degrees of freedom.
Complications
Complications (n = 10)
Discussion
Both lateral mass screws and cervical pedicle screws are in widespread use, but each trajectory carries drawbacks. The cervical pedicle inlet trajectory is a novel approach with a trajectory similar to that of a traditional pedicle screw, but that stops in the dense bone at the mouth of the pedicle (the pedicle inlet). By stopping short of the critical neurovascular structures, we suspected that the screws would have a low rate of malposition and clinical complications. Overall, we found that with navigation assistance, 98% of screws were placed with <2 mm of cortical breach, and there were no cases of return to OR for screw related complications. Several of our findings merit further discussion.
While pedicle screws are known to have the strongest biomechanical fixation, many surgeons remain concerned about the neurovascular risks. A recent systematic review found that sub-axial pedicle screws had a 17% rate of malposition, and that neurovascular complications occurred in up to 24% of cases due to screw malposition (average of 1.2%, range 0-24%). 11 In our own series, 10% (5/49) pedicle screws were malpositioned more than 2 mm and required intra-operative revision or removal. Thus, it is clear that the pedicle is not accessible in a significant number of patients. In contrast, we found that 98% of CPI screws were placed without a clinically significant cortical breach, which compares favorably against both the 83% rate historically reported for pedicle screws, 11 as well as the 90% rate observed here in our series. Furthermore, there were no cases where a CPI could not be placed, which is in contrast to true pedicle screws where a small diameter pedicle, or aberrant vertebral arteries are frequent obstacles. 11 Neither of these are obstacles to CPI screw placement, because the screw stops short of the critical neurovascular anatomy (Figure 4).
Lateral mass screws are the traditional alternative to pedicle screws. In our series, no lateral mass screws required intra-operative repositioning. This fits with the well-known and longstanding history of safety for this screw type. However, biomechanical studies have consistently shown poor quality fixation in the lateral mass. 2 Furthermore, the medial tulip head of a lateral mass screw can create challenging rod bends (Figure 1) and may limit the ability to perform central decompression after the screws are placed. A prior biomechanical study from our group indicated that the CPI screw had a 51% improvement in pullout strength compared to lateral mass screws. This clinical series builds on those prior cadaveric results by demonstrating clinical feasibility, with no screw related complications and demonstrates that the navigated CPI trajectory is a reasonable alternative to LM screws.
All of the screws in this series were placed with O-Arm assisted Stealth navigation (Medtronic). In spite of the navigation aid, 6 of 292 (2%) CPI screws were found to have more than 2 mm cortical violation and were deemed necessary for revision. 1 was exchanged for a shorter screw, and 5 were left out of the construct, with no return to OR or neurovascular complication attributable to screw placement. Navigation is necessary for placement of the CPI screw because the screw tip is directed to the mouth of the pedicle, and while the trajectory could be determined with fluoro or the use of a laminotomy and palpation, the length of the screw would be impossible to determine without the navigation aid. We believe that that these results indicate that navigation guidance makes the trajectory safe and clinically feasible, and the 2% malposition rate compares favorably against the historical rate of 17% with pedicle screws, 11 and 8% rate from our series. However, the malposition represents the fact the cervical spine is highly mobile which can lead to navigation inaccuracy, and emphasizes the importance of taking a check spin before leaving the OR. We would stress that the check spin is a critical element for safety and recommend that screws malpositioned >2 mm be removed or revised intra-operatively.
This study does have several limitations. We do not have any information about patient reported outcomes or long-term follow-up rates to determine fusion status or mechanical failure of these constructs. The purpose of this manuscript was to demonstrate the anatomic and clinical feasibility of the CPI trajectory as a first of its kind report. We anticipate future studies to report on those factors.
Overall, 2% of navigated CPI screws required intra-operative revision for malposition. No patient had a return to OR or clinical complication from screw malposition, and these results are favorable compared to cervical pedicle screws, which have a higher malposition rate. Furthermore, unlike sub-axial pedicle screws which can only be placed with favorable anatomy, CPI screws can be placed in the vast majority of sub-axial cervical levels because the tip of the screw stops short of the critical neurovascular anatomy. Thus, the CPI screw represents a reasonable alternative to pedicle screws in the sub-axial cervical spine. Furthermore, the lateral CPI tulip head allows for easier rod passage in long constructs and allows for central neurologic decompression after instrumentation, which are advantages relative to lateral mass screws. We intend for this preliminary report to increase awareness of this novel technique. Future clinical series regarding the long-term outcomes, and the applicability to minimally invasive approaches, will be useful in proving the clinical efficacy of the CPI trajectory.
Footnotes
Ethical Considerations
Institutional Review Board approval was obtained for this study from the University of Minnesota Institutional Review Board (STUDY00026021). Informed consent was waived due to the retrospective design and de-identification of patient data.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
CM declares institutional grant/research support from Mizuho OSI, NuVasive, Orthofix, and SI Bone. RC, BA, SR and KO have nothing to disclose.