
Abstract
Study Design
Prospective single-arm cohort study.
Objectives
Cervical pedicle screws (CPS) offer superior biomechanical stability compared with lateral mass screws. However, their widespread adoption is constrained by narrow pedicle safety margins and the potential risk of neurovascular injury. This study aimed to describe the rationale of a novel triad-dependent technique (TDT) for subaxial CPS placement and to evaluate its accuracy and safety.
Methods
Between May 2023 and April 2025, 63 consecutive patients undergoing posterior subaxial (C3–C6) cervical instrumentation at our institution were screened for eligibility. CPS were inserted using the TDT, which integrates individualized morphometric preoperative planning, intraoperative fluoroscopic guidance, and continuous tactile monitoring via mini-laminotomy. Postoperative CT was used to assess screw accuracy using the 2-mm breach classification. Multinomial logistic regression was performed to identify risk factors for breach.
Results
A total of 204 CPS were inserted in 41 patients. No breach was observed in 174 screws (85.3%), while 30 screws (14.7%) demonstrated breach, including 18 medial and 12 lateral violations. No neurovascular complications were observed in this cohort. Pedicle diameter <4 mm significantly increased the risk of both medial and lateral breach, while medial wall thickness showed direction-specific effects on breach risk.
Conclusions
The TDT demonstrates the feasibility of accurate and safe subaxial CPS placement. By integrating individualized morphometric planning with fluoroscopic and tactile safeguards, TDT effectively mitigates both medial and lateral breach risks and may expand the safe application of CPS fixation.
Keywords
Introduction
Cervical pedicle screws (CPS) provide the strongest biomechanical fixation for the subaxial cervical spine, offering superior pullout strength compared with lateral mass screws (LMS).1-3 Despite these advantages, the widespread adoption of CPS remains limited by narrow pedicle safety margins, which increase the risk of neurovascular injury from screw malposition. Consequently, LMS remain the standard posterior instrumentation.4,5 Nevertheless, CPS are indispensable when conventional techniques are insufficient, particularly in cases of severe osteoporosis, complex deformity, multilevel pathology, and highly unstable traumatic injuries. In such settings, CPS provide superior biomechanical stability while allowing shorter constructs.3,6-8
Following the initial clinical description of CPS fixation by Abumi et al, 9 early clinical series reported favorable outcomes with relatively low pedicle perforation rates.10-12 In contrast, cadaveric studies have demonstrated higher perforation rates, reaching up to 87.5%, with lateral breaches predominating and posing a particular risk to the vertebral artery.13,14 Lateral deviation commonly results from inserting the screw at a medial trajectory smaller than the true pedicle axis, causing deflection by the thick proximal medial cortex. 15
Early efforts to reduce lateral breaches focused on increasing mediolateral insertion angles to match the native pedicle axis.15-20 However, achieving angles exceeding 45° is technically difficult due to bulky paraspinal musculature and often requires separate paraspinal stab incisions, limiting practicality. 18 The Medial Cortical Pedicle Screw (MCPS) technique later addressed this by partially drilling the medial cortex to guide the screw along the stronger medial wall. 21 While effective in reducing lateral breaches, MCPS introduced higher medial wall violation rates, theoretically increasing the risk of spinal cord or nerve root injury.
Previous studies have described distinct technical approaches aimed at improving the accuracy of CPS placement, including individualized preoperative morphometric planning, pedicle-axis fluoroscopic guidance, and mini-laminotomy.11,12,22,23 However, when applied in isolation, these approaches do not consistently address both lateral and medial cortical breaches. Their systematic integration into a single workflow has not been previously reported.
These limitations underscore the need for a reliable CPS insertion technique that minimizes both lateral and medial breaches while remaining practical and reproducible. The triad-dependent technique (TDT) was therefore developed to address this gap by refining and integrating individualized preoperative morphometric planning, pedicle-axis fluoroscopic guidance, and continuous tactile monitoring via mini-laminotomy into a unified, structured workflow. Accordingly, this study aims to describe the rationale of the TDT and to prospectively evaluate its accuracy and safety in subaxial CPS placement, particularly in settings without advanced navigation technologies.
Patients and Methods
Trial Design and Registration
This single-center, single-arm prospective cohort study received approval from our institutional review board (17100676) and registered in advance at ClinicalTrials.gov (identifier: NCT05855642). The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants provided written informed consent before enrollment in the study.
Participant Selection
Between May 2023 and April 2025, 63 consecutive patients undergoing posterior subaxial (C3–C6) cervical instrumentation at our institution were screened for enrollment in this prospective study. All adult patients requiring posterior cervical fixation for any indication, including trauma, degenerative disease, tumor, infection, or deformity, were considered eligible. Patient-level exclusion criteria included inability or unwillingness to provide informed consent and the presence of vertebral artery anomaly or injury confirmed on preoperative computed tomography angiography (CTA), which was performed in all screened patients. Only patients satisfying all patient-level criteria proceeded to pedicle-level evaluation. Because fixation requirements varied based on the underlying pathology and surgical goals, not all subaxial pedicles (C3–C6) were intended for instrumentation in every patient. Only pedicles planned for CPS insertion, as dictated by surgical necessity, were assessed. Each planned pedicle underwent detailed evaluation using preoperative CT imaging. Pedicles were excluded from CPS insertion if they demonstrated an outer cortical diameter <3.5 mm, a pedicle fracture, or sclerotic morphology with absent cancellous tract (Figure 1). Preoperative CT examples illustrating pedicle-level and patient-level exclusion criteria. (A–B) Axial and coronal oblique CT images demonstrating a left pedicle with an outer cortical diameter <3.5 mm at its narrowest point (arrow). (C–D) Axial and sagittal CT images showing a right pedicle fracture (arrow). (E–F) Axial and coronal oblique CT images showing a sclerotic right pedicle with absence of a cancellous tract (arrow). (G–H) Axial and coronal oblique CT angiography images demonstrating a right-sided vertebral artery anomaly (arrow)
Sample Size
This study employed consecutive sampling, aiming to include all eligible patients within the specified timeframe. The minimum required sample size was determined by an a priori calculation aimed at ensuring sufficient precision in estimating the primary outcome: the TDT screw placement accuracy rate. Based on previously published accuracy rates for cervical pedicle screw placement,24-26 an expected accuracy of 85% was assumed, requiring a minimum of 196 screws to generate a 95% confidence interval with a margin of error of ±5%. The final sample size obtained through consecutive enrollment exceeded this requirement, thereby improving the precision of the accuracy estimate and supporting reliable descriptive and regression analyses.
Triad-Dependent Technique (TDT): Conceptual Overview
The TDT is based on the integration of 3 complementary components: (1) individualized preoperative morphometric analysis for pedicle viability and trajectory planning; (2) intraoperative fluoroscopic guidance to reproduce the planned entry point and trajectory; and (3) continuous tactile monitoring through a mini-laminotomy to prevent medial violation while allowing controlled medial cortical preparation. These components are applied in a complementary and integrated manner to optimize accuracy while minimizing the risk of both lateral and medial breach.
Component I: Preoperative Morphometric Evaluation and Trajectory Planning
Preoperative Morphometric Pedicle Assessment
Preoperative evaluation was based on high-resolution three-dimensional multislice computed tomography (CT) integrated with advanced surgical planning software (Horos, version 4.0.1; Annapolis, MD, USA).
27
Multiplanar reconstruction (MPR) was used to accurately realign the axial and sagittal planes, correcting for any vertebral rotation or image acquisition inaccuracies. Consecutive cross-sectional images were generated along oblique coronal planes oriented perpendicular to the true pedicle axis to identify the pedicle’s narrowest segment. At this level, the inner pedicle diameter, outer pedicle diameter, and medial cortical wall thickness were precisely measured (Figure 2). Pedicle viability was confirmed after excluding pedicles with a narrow outer diameter (<3.5 mm), fractures, or complete sclerosis with the absence of a cancellous core. Preoperative CT-based pedicle assessment and trajectory planning. (A) Sagittal multiplanar reconstruction showing alignment of the true pedicle axis parallel to the superior endplate. (B) Axial reconstruction demonstrating the true pedicle axis relative to the contralateral lamina. (C) Oblique coronal slice perpendicular to the pedicle axis at the narrowest pedicle level, used to measure the outer pedicle diameter (OPD), inner pedicle diameter (IPD), and medial wall thickness (MWT). (D) Axial planning view illustrating the planned screw trajectory (green), which is perpendicular to the ipsilateral lamina (green), and the true pedicle axis (red), which runs parallel to the contralateral lamina (red); the two intersect at the pedicle’s narrowest point
Identification of the True Pedicle Axis
The true pedicle axis was identified primarily on axial CT images and subsequently confirmed in the other planes. • Axial plane: Axial CT images were scrolled to the level of the pedicle isthmus. The MPR reference axes were rotated such that one axis passed through the geometric center of the pedicle along its longitudinal course; this axis was designated as the true pedicle axis. It was further adjusted to be parallel to the contralateral lamina, ensuring correct mediolateral alignment. • Sagittal plane: The MPR axis was fine-tuned to ensure that it passed through the pedicle center and remained parallel to the superior vertebral endplate, establishing the cranio-caudal orientation. • Coronal oblique plane: The intersection of the reference axes was confirmed to lie at the center of the cortical pedicle ring. • Final definition: The true pedicle axis was defined as the MPR axis that remained centered within the pedicle across axial, sagittal, and oblique coronal views, while being parallel to the contralateral lamina in the axial plane and to the superior vertebral endplate in the sagittal plane (Figure 2).
Determination of the Planned Screw Trajectory
The planned screw trajectory was defined relative to the previously identified true pedicle axis and determined using a stepwise multiplanar approach (Figure 2). • Sagittal plane: The planned trajectory was aligned with the true pedicle axis and adjusted to remain parallel to the superior vertebral endplate, thereby maintaining appropriate cranio-caudal orientation. • Axial plane: The axial trajectory was designed to originate just medial to the center of the lateral mass and advance toward the pedicle at an angle perpendicular to the ipsilateral lamina. To determine this orientation, a reference line was drawn along the long axis of the ipsilateral lamina. A second line was then constructed perpendicular to this laminar reference, defining the planned axial trajectory. This trajectory was deliberately less steep than the native true pedicle axis but was designed to intersect it precisely at the pedicle’s narrowest point, thereby ensuring passage through the safest central osseous corridor. • Coronal oblique plane: the planned trajectory was required to pass through the medial half of the cortical pedicle ring.
Medial Cortical Preparation Strategy
The proximal segment of the planned trajectory was designed to engage the medial pedicle wall. The preoperatively measured medial wall thickness guided the anticipated extent of controlled medial cortical preparation, a key component of the triad-dependent technique aimed at minimizing lateral breach risk while preserving medial wall integrity. Medial walls measuring >2 mm were interpreted as permitting a greater degree of controlled thinning under intraoperative monitoring, as detailed in Component III.
Component II: Intraoperative Fluoroscopic Guidance
A pedicle-axis fluoroscopic view was obtained by rotating the C-arm until the pedicle appeared as a cortical ring. This view was used to confirm that the entry point, placed just medial to the center of the lateral mass, 1-2 mm inferior to the superior articular facet, lay within the medial half of the pedicle ring. A 2-mm high-speed burr was used to penetrate the cortical bone at the selected entry point. During pedicle preparation, lateral fluoroscopy was used to maintain cranio-caudal alignment parallel to the superior vertebral endplate (Figure 3A and B). Intraoperative steps of the triad-dependent technique. (A) Pedicle-axis fluoroscopic view showing the pedicle as a cortical ring, confirming that the entry point lies within its medial half. (B) Lateral fluoroscopic view verifying cranio-caudal alignment of the planned pedicle trajectory during cannulation. (C) Schematic illustration demonstrating the orientation of the burr in the axial plane to match the planned trajectory. The burr is positioned perpendicular to the ipsilateral lamina and guided by a 90-degree dissector, with its short arm flush against the lamina and the burr shaft aligned parallel to the long arm. (D) Intraoperative photograph demonstrating a mini-laminotomy exposing the medial pedicle wall, with a hook dissector providing continuous tactile feedback during tract preparation using a 2-mm burr. (E) Schematic illustration depicting controlled burr advancement with incremental medial cortical thinning, continuously monitored through tactile feedback via the mini-laminotomy using a ball-tipped hook to detect early cortical compromise and prevent medial breach
Component III: Continuous Tactile Monitoring and Controlled Cortical Preparation
Medial cortical preparation was performed using a 2-mm high-speed burr. In the axial plane, The burr was directed medially at an angle perpendicular to the ipsilateral lamina. This orientation was estimated intraoperatively using a 90-degree dissector, with the short arm resting flush against the ipsilateral lamina and the burr aligned parallel to the long arm of the dissector (Figure 3C). Cranio-caudal alignment was maintained under lateral fluoroscopic guidance.
A focused mini-laminotomy was created at the instrumented level to provide direct tactile access to the medial pedicle wall while preserving posterior element stability. Controlled, incremental pressure was applied to thin, but not perforate, the medial cortex. The extent of medial cortical thinning was determined preoperatively based on the measured medial pedicle wall thickness and was continuously monitored intraoperatively through direct tactile feedback via the mini-laminotomy. A hook dissector was maintained along the medial pedicle wall throughout the procedure to detect early cortical compromise and prevent unintended medial deviation (Figure 3D and E). In cases where the preoperatively measured medial wall thickness exceeded 2 mm, a 2.5-mm burr was selectively used to allow additional controlled medial cortical thinning. This step was performed only after confirming that the initial tract created with the 2-mm burr was intact, with no evidence of medial or lateral cortical breach on tactile assessment and direct visualization.
The pilot hole was assessed circumferentially using a ball-tipped feeler, after which the tract was tapped to the appropriate diameter. Standard polyaxial screws were inserted with continued tactile monitoring. Final screw position was confirmed using anteroposterior and lateral fluoroscopic views.
For clarity, the procedural workflow is summarized as follows: Preoperative CT-based planning defines the true pedicle axis, a patient-specific trajectory, and the anticipated extent of medial cortical thinning. Intraoperatively, the planned entry point is reproduced using pedicle-axis fluoroscopic guidance. A pilot tract is created using a high-speed burr, followed by controlled medial cortical preparation under continuous tactile monitoring through a mini-laminotomy. Cranio-caudal alignment is maintained using lateral fluoroscopy. Final verification includes tract assessment with a ball-tipped probe to confirm the absence of cortical breach, followed by screw insertion with continued tactile monitoring and fluoroscopic confirmation of final screw position using anteroposterior and lateral views.
Outcome Measures
The primary outcome was screw placement accuracy. Secondary outcomes included the incidence of screw-related complications and the identification of risk factors for pedicle breach. Screw accuracy was evaluated on high-resolution three-dimensional MSCT obtained immediately postoperatively. All screws were assessed for pedicle breach and subsequently classified according to the 2-mm increment system based on the Gertzbein–Robbins classification. 28 Screws were graded as follows: Grade 0, no breach; Grade 1, a breach of <2 mm; Grade 2, a breach of 2-4 mm; and Grade 3, a breach of >4 mm. Grades 0 and 1 were considered clinically acceptable. Assessment and classification were performed by 2 investigators who independently assessed each screw 3 times for pedicle breach prior to comparison of results. Discrepancies were adjudicated by the principal investigator. Blinding to vertebral level, side, and surgical indication was not feasible due to their inherent visibility on postoperative CT imaging.
Statistical Analysis
Data were analyzed using GraphPad Prism for macOS version 9.5.0 (GraphPad Software, San Diego, CA, USA). Continuous variables were presented as mean ± standard deviation, and categorical variables as frequencies and percentages. Multinomial logistic regression analysis was performed to identify potential risk factors for pedicle breach. Intraobserver and interobserver reliability for breach classification were assessed using agreement rates and Cohen’s kappa (κ) statistics. A P value <0.05 was considered statistically significant.
Results
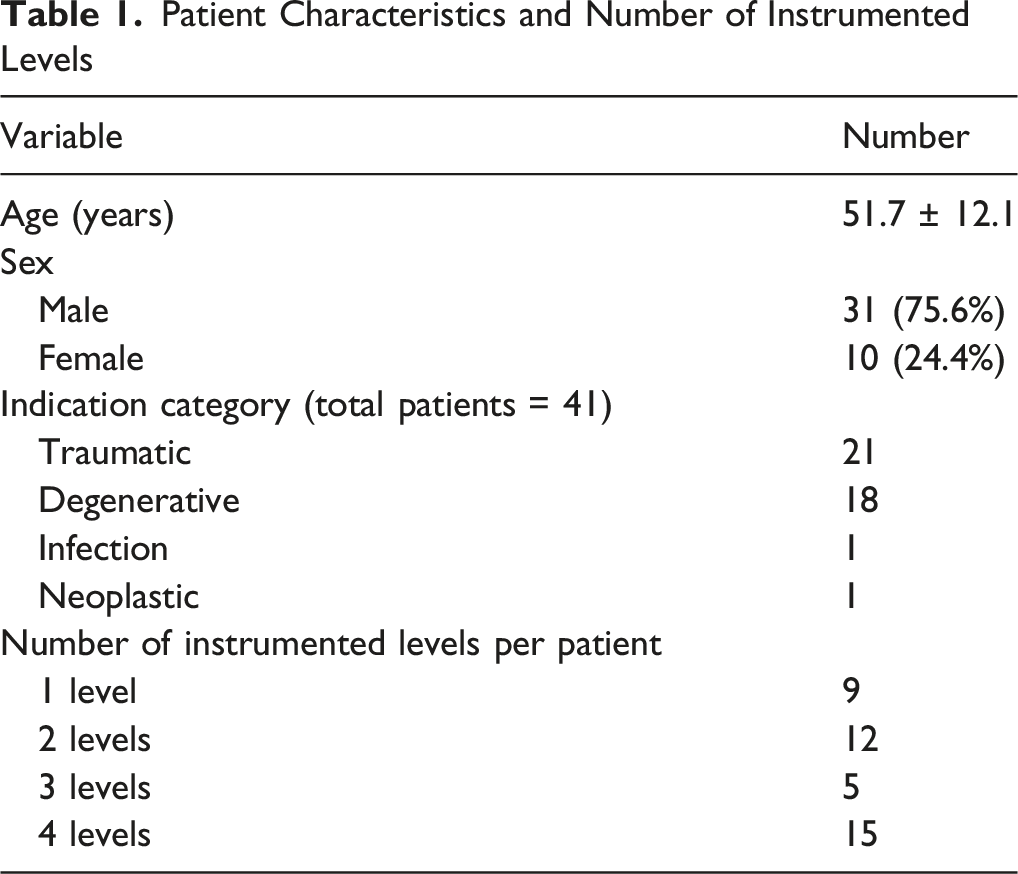
Patient Characteristics and Number of Instrumented Levels
Level-Specific Distribution of Planned, Excluded, Converted, and Inserted Cervical Pedicle Screws
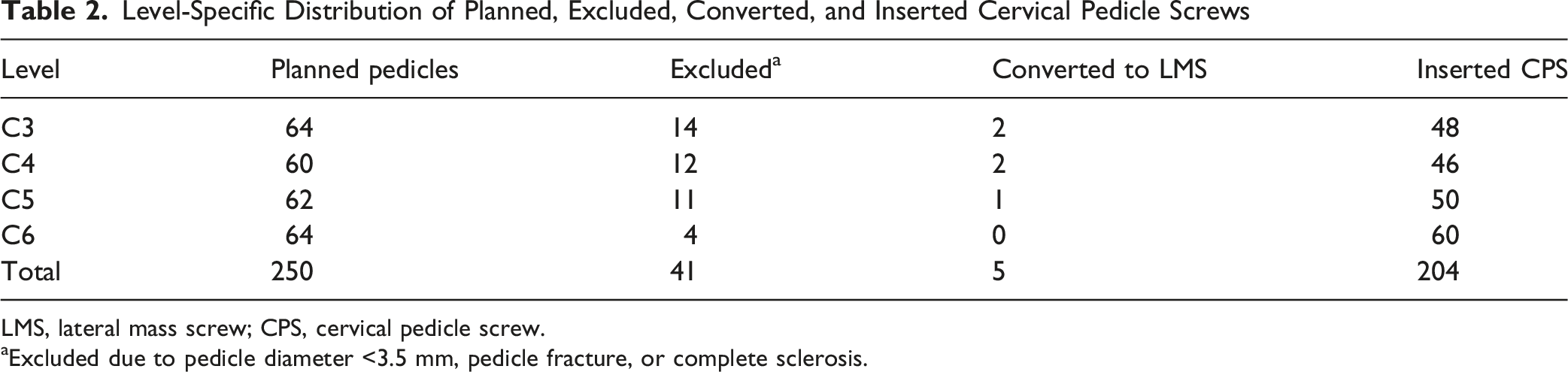
LMS, lateral mass screw; CPS, cervical pedicle screw.
aExcluded due to pedicle diameter <3.5 mm, pedicle fracture, or complete sclerosis.

Flow diagram of patient screening and pedicle inclusion

A 48-year-old male patient with traumatic cervical spinal cord injury (Frankel grade B) following a motor-vehicle accident. (A) Preoperative sagittal T2-weighted MRI demonstrating cervical canal compromise with intramedullary hyperintensity cord signal, cord swelling, and disruption of the posterior ligamentous complex. (B) Preoperative sagittal CT showing fractures of the C4, C5, and C6 spinous processes. (C–D) Postoperative anteroposterior and lateral radiographs demonstrating C3–C6 posterior cervical pedicle screw fixation and decompressive laminectomy. (E–H) Postoperative axial CT images at the C3, C4, C5, and C6 levels, respectively. All screws are Grade 0 (no breach) except the left C4 pedicle screw in (F), which demonstrates a Grade 1 (<2 mm) lateral cortical breach (arrow). (I–J) Right and left oblique coronal CT reconstructions confirming accurate screw positions; the Grade 1 (<2 mm) lateral breach of the left C4 pedicle screw is again evident (arrow) in (J), without any clinical sequelae

Bail-out scenario with conversion to lateral mass screw following intraoperative pedicle fracture. (A) Axial CT image demonstrating fracture of the medial wall of the right C4 pedicle (red arrow) occurring during screw insertion despite an initially intact tract, which was directly visualized through the mini-laminotomy. Based on intraoperative tactile feedback, the pedicle screw was abandoned, and a lateral mass screw was placed. The contralateral (left) C4 pedicle screw demonstrates ideal positioning without cortical breach (Grade 0). (B) Sagittal CT image (right side) showing fracture of the inferior wall of the right C4 pedicle (red arrow). (C) Sagittal CT image (left side) demonstrating optimal screw positioning at C4–C7. (D) Right coronal oblique CT image confirming the medial wall fracture of the right C4 pedicle. (E) Left coronal oblique CT image confirming accurate placement of pedicle screws at C4–C7 without cortical violation
Regarding screw placement accuracy, of the 204 screws inserted, 174 screws (85.3%) demonstrated no breach, while 30 screws (14.7%) exhibited a breach, including 18 medial and 12 lateral breaches (Figure 7). Breach frequency varied by vertebral level, with C3 showing the highest breach rate, followed by C4 and C5 whereas C6 demonstrated the lowest (Table 3). Based on the 2-mm increment rule, 190 screws (93.1%) were classified as clinically acceptable, defined as Grade 0 (no breach) or Grade 1 (<2 mm breach) (Table 4). Interobserver agreement was 93.4% (mean κ = 0.76), and intraobserver agreement was 91.8% (mean κ = 0.72), indicating good reliability. Importantly, no vascular or neurological complications were observed in this cohort. Representative examples of cervical pedicle screw breaches. Postoperative axial and coronal oblique CT images illustrating different grades and directions of pedicle screw breach (arrows indicate the site of cortical violation). (A–B) Grade 1 (<2 mm) medial cortical breach of the left C4 pedicle screw. (C–D) Grade 2 (2-4 mm) medial cortical breach of the right C3 pedicle screw. (E–F) Grade 2 (2-4 mm) lateral cortical breach of the right C4 pedicle screw. (G–H) Grade 3 (>4 mm) lateral cortical breach of the right C3 pedicle screw. None of the illustrated breaches were associated with neurovascular complications Accuracy and Breach Distribution of Cervical Pedicle Screws by Level and Side Accuracy of Cervical Pedicle Screws According to the 2-mm Increment System


Multinomial Logistic Regression Identifying Predictors of Pedicle Breach Type

Reference outcome, no breach; RRR, relative risk ratio; CI, confidence interval. Bold values indicate statistically significant results (P < 0.05).
Discussion
CPS provide the strongest biomechanical stability in the subaxial cervical spine. However, their adoption remains limited by narrow pedicles and proximity to the vertebral artery and neural structures. Traditional freehand and modified methods have struggled to consistently avoid pedicle wall violation. The TDT was developed to address these limitations by integrating 3 elements: individualized multiplanar morphometric planning, fluoroscopic guidance, and tactile medial-wall protection through a mini-laminotomy. This study prospectively evaluated TDT accuracy and identified predictors of breach direction.
Entry-point and trajectory-angle selection are central determinants of CPS accuracy and safety. Morphometric studies consistently demonstrate that the native pedicle transverse angle (PTA) in the subaxial cervical spine ranges from 45° to 55°.22,29 Accurate screw placement along this anatomic axis would therefore require a far-lateral entry point at the lateral vertebral notch combined with a steep medial inclination exceeding 45°. 15
The traditional technique described by Abumi et al 9 uses an entry point lateral to the midpoint of the lateral mass but medial to the lateral notch, with a medial inclination of approximately 25-45°. In an early report by Abumi et al, a relatively low perforation rate of 6.9% was observed in 159 screws. 10 However, subsequent studies have shown less consistent accuracy. In a large multicenter series by the Abumi group (Hojo et al), involving more than 1000 screws, the overall perforation rate increased to 14.8%, with lateral breaches accounting for 79.7% of misplacements, posing a particular risk to the vertebral artery. 30 This predominance of lateral perforation has been attributed to lateral deflection of the screw by the thick proximal medial pedicle cortex when the entry point is medial to the notch and the trajectory is shallower than the native pedicle transverse angle. 15
To better align screw placement with pedicle morphology, several authors advocated far-lateral entry point combined with steep medial angulation (45-55°).15-20 Techniques such as that described by Pan et al reduced lateral perforations. However, the overall perforation rate remained relatively high (19.6%). 20 In addition, achieving such steep angulation requires extensive dissection or separate stab incisions, increasing morbidity and limiting practicality. 18
More recently, medialized entry-point strategies, including MCPS technique, were introduced to reduce lateral breaches while allowing shallower trajectories. Although effective in limiting lateral deviation, these techniques substantially increased medial perforations. Mahesh et al 21 reported an overall perforation rate of 19.93% in 577 screws, with 74.8% of breaches occurring medially, underscoring the vulnerability of the medial cortex when screws are advanced medially.
The TDT was designed to reconcile the limitations of these prior strategies. TDT employs a medialized entry point at the midpoint of the lateral mass and a planned trajectory aligned perpendicular to the ipsilateral lamina, typically inclined less than 35°. Although shallower than the native PTA, this trajectory is planned to intersect the true pedicle axis precisely at the pedicle’s narrowest point, ensuring passage through the safest central osseous corridor. Accurate identification of the entry point is facilitated intraoperatively using a pedicle-axis fluoroscopic view. While Yukawa et al 12 selected the center of the pedicle ring in the pedicle-axis view as the entry point and used a 30-35° medial inclination, their choice of a central-ring entry point geometrically corresponds to a more lateral entry and would normally require a steeper angle to align with the native axis. In TDT, the entry point is deliberately positioned within the medial half of the cortical ring, consistent with the planned medialized starting point, allowing the use of a shallower trajectory while still converging with the true pedicle axis.
Because medialized entry points are inherently associated with an increased risk of medial breach, TDT incorporates a mini-laminotomy to enable continuous tactile monitoring of the medial pedicle wall during drilling, probing, tapping, and screw insertion. The protective value of mini-laminotomy is supported by prior studies: Park et al 23 reported no medial breaches among 78 screws, Celikoglu et al 31 demonstrated predominantly lateral perforations in a series of 227 screws, and Ludwig et al 14 showed that laminotomy increased accurate intrapedicular placement from 12.5% to 45% while reducing critical breaches compared with morphometric freehand techniques.
In a subset of narrow pedicles, minimal emergence of screw threads through the medial cortex was observed intraoperatively. These limited breaches were accepted when the exposed threads were clearly separated from the neural structures, providing confidence that the violation was minor and clinically safe. Huang et al 32 demonstrated that a measurable medial buffer exists between the medial pedicle wall and the cord, with a mean distance of 6.56 ± 2.10 mm, which may help explain the absence of neurological complications in the present series. Overall, mini-laminotomy appears to enhance procedural safety not only by reducing the incidence of medial breach but also by limiting breach severity and ensuring adequate separation from critical neural structures.
When benchmarked against prior strategies, the TDT achieved a low overall breach rate of 14.7% with a balanced distribution of deviations (5.9% lateral and 8.8% medial). This pattern reflects effective control of both dominant modes of screw deviation. By medializing the entry point, reducing the required medial inclination, and combining controlled medial cortical preparation with continuous tactile monitoring, TDT minimizes lateral breach risk without increasing medial violation.
The multinomial regression analysis identified key anatomical determinants of breach direction during CPS insertion. Pedicle diameter <4 mm significantly increased the risk of both medial and lateral breaches (P = 0.001 and P = 0.020), confirming that narrow pedicles provide a very limited osseous safety margin for accommodating a 3.5-mm screw. This finding is consistent with morphometric studies by Karaikovic et al, 22 who demonstrated that the inner pedicle diameter at C3–C6 averages only 2.6-2.9 mm, making cortical engagement unavoidable even with ideal technique. Consequently, any deviation from the intended trajectory in these narrow pedicles readily results in cortical violation.
Medial wall thickness showed a direction-specific effect on breach risk. A thin medial cortex (<1.5 mm) significantly increased medial breach risk (RRR 5.85, P = 0.003), whereas a thick medial cortex (>2.0 mm) increased lateral breach risk (RRR 7.98, P = 0.008). This reflects the biomechanical balance between over-thinning a thin cortex, which predisposes to medial violation, and under-preparing a thick cortex, which allows lateral deflection. Prior morphometric studies report substantial variability in medial cortical thickness (1.2-2.0 mm in Panjabi et al 33 ; 2.3-2.7 mm in Sakamoto et al 15 ), a pattern that was also observed in our study (1.3-2.4 mm), underscoring the need for individualized preoperative measurement to guide cortical preparation.
Vertebral level further influenced accuracy, with C6 screws demonstrating a significantly lower risk of lateral breach (RRR 0.13, P = 0.042), consistent with larger pedicle dimensions, while age, sex, and laterality showed no significant associations (P > 0.05), underscoring that anatomical rather than demographic factors govern CPS accuracy.
Regarding intraoperative conversions to lateral mass screws, 5 planned CPS insertions required conversion. Three conversions were due to medial wall fracture occurring during screw insertion despite an intact initial tract, which was directly visualized through the mini-laminotomy. The remaining two conversions were undertaken following intraoperative identification of lateral breach, indicated by a tract length shorter than that planned on preoperative CT, and safe redirection of the tract was not feasible. Conversions occurred at C3 (n = 2), C4 (n = 2), and C5 (n = 1), with no conversions at C6. These findings are comparable to those reported by Park et al, 34 who observed a 7.8% conversion rate, with conversions occurring predominantly at the upper subaxial levels (C3–C5). Collectively, these data underscore the importance of meticulous preoperative planning and continuous tactile feedback in maintaining procedural safety during CPS insertion, particularly at anatomically constrained levels.
The accuracy achieved with TDT (85.3%) aligns with, and in some instances exceeds, the performance of freehand and even navigation-assisted techniques reported in systematic reviews. In the most recent and largest review, Irmak et al 35 analyzed more than 14,000 screws and reported mean accuracy rates of 83.0% for non-navigated techniques (freehand and fluoroscopy), 82.5% for navigation-guided placement, and 95.8% for 3D-printed template techniques. Notably, this represents a shift from earlier systematic reviews and meta-analyses, including those by Kosmopoulos et al, 24 Mahmoud et al 25 and Tarawneh et al, 26 in which navigation consistently outperformed non-navigation techniques (navigation accuracy 87.5-99.2% vs 80-91.3% for freehand or fluoroscopy-based methods). The more recent convergence in accuracy likely reflects the broader adoption of freehand technique with the cumulative learning-curve effect.
In contrast, reported navigation accuracy in the cervical spine varies widely, with pedicle violation rates ranging from as low as 2.7% to as high as 63.2%. 35 These discrepancies primarily arise from the intrinsic mobility of the cervical spine: even subtle changes in vertebral alignment during reduction maneuvers, tissue retraction, or screw insertion can desynchronize navigation data from real-time anatomy.36-38 Beyond accuracy variability, navigation also carries practical limitations, including time-consuming intraoperative registration, high acquisition and maintenance costs, and limited availability in many centers.12,38
Template-guided techniques continue to demonstrate the highest accuracy (95.8%) but their routine use is restricted by the need for 3D printing, sterilization requirements, restricted availability, and impracticality in emergency settings. 35
Importantly, navigation and template-guided systems cannot replace fundamental surgical principles such as tactile feedback, real-time judgment, and the ability to recognize and correct trajectory deviations intraoperatively; rather, they should be viewed as adjuncts to sound surgical technique. 39 Conceptually, the TDT is designed as a surgeon-controlled primary strategy that may be complemented by navigation or template guidance in selected cases. In such settings, preoperative morphometric planning and mini-laminotomy remain central to safety, while fluoroscopy may be reduced or partially replaced by advanced guidance technologies, potentially lowering radiation exposure.
The novelty of the TDT lies in its structured integration and refinement of 3 essential safety mechanisms within a single reproducible workflow. Specifically, the technique combines (1) individualized morphometric planning to define a patient-specific safe corridor, (2) pedicle-axis fluoroscopic guidance to accurately reproduce the planned entry point and trajectory, and (3) continuous tactile monitoring via mini-laminotomy to provide real-time feedback and prevent medial cortical violation. By integrating these elements within a unified framework, the TDT minimizes both lateral and medial breaches, thereby addressing the principal limitations of prior free-hand techniques. In addition, the TDT does not require advanced navigation systems or patient-specific templates, making it applicable across a wide range of surgical settings, including resource-limited environments. This may facilitate safe CPS placement in settings without access to advanced navigation technologies, thereby broadening its clinical applicability. However, certain technical considerations should be acknowledged. The approach requires familiarity with multiplanar CT-based planning and includes an additional step of mini-laminotomy, which may increase operative time and blood loss. A learning curve should be anticipated, particularly in mastering multiplanar CT-based planning and intraoperative execution.
Limitations
Certain limitations must be acknowledged. This was a single-arm, single-center investigation performed by an experienced surgeon, which may limit generalizability and underestimate the learning curve required to adopt the TDT. No direct comparison was made with navigation-assisted insertion or other freehand techniques, and long-term clinical outcomes were not assessed. The analysis was conducted at the screw level without explicit modeling of within-patient clustering, which may have influenced variance estimates. Procedural parameters, including fluoroscopy time, screw-specific insertion time, and intraoperative blood loss, were not planned to be collected in this study. We anticipated that per-screw assessment would not be feasible and that aggregate values would be substantially confounded by the heterogeneous study population and variability in the number of pedicles instrumented across patients. Future prospective studies with more homogeneous cohorts and standardized instrumentation levels are warranted to accurately quantify these technique-related metrics and to evaluate their clinical relevance, particularly the potential impact of pedicle-axis views on radiation exposure.
Conclusions
The TDT demonstrates the feasibility of accurate and safe subaxial CPS placement by integrating individualized morphometric planning, fluoroscopic guidance, and tactile feedback via mini-laminotomy. This strategy may enhance accuracy by effectively reducing both medial and lateral breach risks while maintaining procedural safety; no neurovascular complications were observed in this cohort despite the identified breaches. These findings support the potential role of TDT to broaden the safe adoption of CPS across diverse cervical pathologies and surgical environments.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines and approved by the institutional review board of the authors’ affiliated institution (17100676).
Consent to Participate
All participants provided written informed consent before enrollment in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.