
Abstract
Study Design
Non-inferiority randomized controlled study.
Objectives
Pedicle screws are the standard for thoracic and lumbar spine fixation. Various guidance techniques exist for optimal screw placement, among which three-dimensional (3D) navigation is regarded as one of the most accurate. The marker screw (MS) technique has been proposed as a method for defining entry points and trajectories. This study compares the accuracy of pedicle screw placement using the MS technique vs that of 3D-navigation.
Methods
The study was conducted in a tertiary center, where patients undergoing thoracic and lumbar spine pedicle instrumentation were assessed. Patients with deformities, tumors, and infections were excluded. Informed consent was obtained. Candidates were assigned to a guidance method by randomly withdrawing a sealed envelope. A computed tomography scan was obtained postoperatively, and the accuracy of pedicle screw placement was assessed and compared between the two groups. The Gertzbein and Robbins system was used to assess pedicle breach.
Results
Forty-six patients (23 MS and 23 navigation) received a total of 266 pedicle screws (146 MS and 120 navigation). Baseline demographics and surgical parameters were comparable between groups. Overall accuracy was 94.5% in the MS group vs 99.1% in the navigation group (P .04). However, MS accuracy was not inferior to navigation and within the non-inferiority margin. No neurologic or vascular complications were attributed to screw misplacement.
Conclusions
The MS technique achieved high placement accuracy with no breach-related complications. Given its safety profile, lower cost, and broader availability, the MS guidance technique represents a viable alternative.
Introduction
Pedicle screws have been the standard in spine fixation for many years.1-5 They provide reliable three-dimensional fixation that can be used for almost all spine pathologies.6,7 The screws offer immediate immobilization, rigid fixation, and reduction in the number of segments that need to be fused to treat a specific pathology. Although the screws yield excellent results in spine instrumentation, they also carry potential for complications.8-10 Pedicle screws must be completely constrained within the walls of the pedicle; a breach may lead to vascular, neurological, or other organ damage.11–13
The standard method for inserting pedicle screws involves a free-hand technique that utilizes anatomical landmarks. Various techniques were developed to assist surgeons in accurately inserting pedicle screws, such as image intensifiers, 3-dimensional generated images, navigation, and video-assisted pedicle screw insertion.14-18 These techniques also aim to reduce complications and minimize radiation exposure to the surgical team and patients.19–24
There is no consensus on the methodology for assessing the accuracy of pedicle screw insertion, as surgeons implement various approaches to report their findings. This study mentions the in/out technique and the 2-mm increment technique. The in/out technique simply grades the accuracy of pedicle screws as “in the pedicle” or “out of the pedicle.” The 2-mm increment technique utilizes a scale of 2-mm increments measured from the walls of the pedicles outward to grade the accuracy of the screw. The consensus is that any grade less than 2 mm is safe, while any grade greater than 4 mm may cause complications. 25
The aim of this study is to examine a technique that modifies the free-hand method using marker screws (MS) as guidance for pedicle screw insertion. We assessed the accuracy of this novel technique in comparison to the three-dimensional (3D) navigation technique, which is widely regarded as one of the most accurate guidance methods for pedicle screw insertion.26-29 The MS technique was previously examined in cadaveric models in 2011, with a breach rate of 5.9%, significantly lower than that of the anatomical landmark, fluoroscopy-guided, and CT-based navigation. 29
Methodology
Study Design and Participants
This study is a prospective, single-center, non-inferiority randomized controlled trial. The trial protocol was registered at ClinicalTrials.gov with the identification code: NCT04196153. The study was conducted in a tertiary care center, and institutional review board approval was obtained. Prior to recruitment, consent was obtained from the participants, including consent for clinical images. The number of screws in each arm was calculated using the equation for non-inferiority trials, cited below, for a power of 80% and a confidence level of 95%. 30 The number needed for each arm was determined to be 112 screws, with an adjusted loss to follow-up of 20%, leading to a calculated sample size of 136 screws per group. As a single-level surgery requires 4 screws to be fixed, to reach 136 screws in each arm, the maximum number of patients needed is 34 in each arm, with a sum of 68 patients if each patient got only one level to be fixed.
The number of patients needed in each arm would be less if more than one level were fixed. Thus, 68 identical sealed envelopes were prepared and placed in the office of the chief investigator. The envelopes were prepared by a student without any of the other parties involved in the study knowing. Thirty-four mini envelopes indicated the MS technique, while the other 34 identical envelopes indicated the 3D navigation technique. Settings for both techniques were kept on stand-by on the day of the surgery with the whole team ready for any of both techniques. A mini envelope was blindly and randomly drawn by the surgeon, indicating the technique to be used the morning of the surgery.
All patients requiring pedicle screw insertion for thoracic and lumbar spine surgery at our institute since the beginning of enrollment in the study on January 1, 2021, were included, except for patients undergoing surgeries for the correction of deformities such as scoliosis and kyphosis, as the standard of care in our hospital for such cases is to use 3D navigation. Additionally, patients with infections and tumors were also excluded due to potential distortion of anatomical landmarks. The enrollment process concluded after both groups reached 136 screws on March 5, 2023 (Figure 1-CONSORT). CONSORT flow diagram
Outcome Measures
After surgery, a CT scan was performed on each patient to assess the pedicle screws. All CT scan images were reviewed by a designated neuro-radiologist who was blinded to the utilized technique. Each screw was evaluated for breach using the CT-based Gertzbein and Robbins system (GRS). 25 The GRS is a categorization system used to evaluate the placement of pedicle screws. The system measures the breach of the pedicle wall in millimeters and is classified into 5 grades: A is a breach of 0 mm, B is a breach of 2 mm, C is a breach of 4 mm, D is a breach of 6 mm, and E is a breach of >6 mm. Each pedicle was evaluated based on its superior, inferior, lateral, and medial walls. GRS grades A and B were considered acceptable while GRS grades C, D and E were considered to be severe breaches.
Moreover, patients’ demographic data (Age, Gender and BMI) preoperative laboratory parameters, intraoperative parameters, and immediate postoperative parameters were collected (Pre and Post-operative Hemoglobin, Pre and Post-operative Hematocrit Duration of Surgery, Estimated Blood Loss, Hospitalization Time and Time before Ambulation). Postoperatively, all patients were examined for complications related to screw placement. In the immediate postoperative period, all patients underwent a clinical examination after recovering from anesthesia. A full neurological examination was conducted and compared to the one performed immediately pre-operatively. Complications were monitored throughout the follow-up period.
Study Groups
Pedicle Screws Insertion Using 3D-Navigation
After posterior exposure of the thoracic and lumbar spine under neural navigation with the use of intraoperative 3D imaging quality O-arm, pedicle screws were inserted at the thoracolumbar/lumbar spine after rigid fixation of the reference frame at the spinous process above or below the level of instrumentation. This step was followed by O-arm imaging and uploading of the images to the navigation system. Pedicle screws then where inserted using navigated awl, navigated taping then navigated screwdriver (Figure 2). (A) Pedicle canulation using navigated awl. (B) Navigating tapping. (C) Pedicle screw insertion using navigated screwdriver
Pedicle Screws Inserted Using MS
After posterior exposure of the thoracic and lumbar spine, the anatomical landmarks for the insertion of pedicle screws were identified, followed by the use of a high-speed burr drill to create a pilot hole at the chosen entry point, which is the midpoint of the transverse process and lateral to the facet joint. The MS was then placed with the proposed trajectory. The inserted part of the MS typically measures 12 mm in length and 3 mm in width. Fluoroscopy was then used to obtain anteroposterior and lateral views to confirm the position of the MS. The MS indicated a pilot entry point and trajectory for the pedicle screw. At this stage, a modified free-hand technique was employed, supported by the images provided, which were used to cannulate the pedicle with the information from the two images taken for all the MS simultaneously, after which the pedicle screws were inserted. To enhance intraoperative accuracy when using the MS technique, several strategies were employed, including strict adherence to anatomical landmarks, confirmation of marker screw trajectory using orthogonal fluoroscopic views, tactile probing during pedicle cannulation, and final fluoroscopic assessment after placement of all screws. A detailed description of the technique was provided previously by Khashab et al
24
(Figure 3). (A) Exposure the posterior elements and marker screws applied through standard anatomical entry point. (B) and (C) Anteroposterior and lateral radiographs are taken after applying all marker screws to confirm the entry points and trajectories to start the insertion of pedicle screws
Statistical Analysis
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 22.0. The Pearson chi-squared test, Student’s t-test, and Fisher exact test were employed. The study was designed as a non-inferiority trial. The non-inferiority margin was prespecified as −10% (δ = −0.10), based on prior literature indicating acceptable pedicle screw accuracy above 90% and reported navigation accuracy approaching 99%. Non-inferiority was established if the lower bound of the two-sided 95% confidence interval (CI) for this difference exceeded −0.10. P-values below .05 were considered significant. A confidence interval of 95% was considered in carrying out the analysis for the non-inferiority margin.
Results
The trial recruited 46 participants: 28 were females (16 in the navigation group and 12 in the MS group) and 18 were males (7 in the navigation group and 11 in the MS group).
Group Demographics, Surgical Details, and Hospital Course
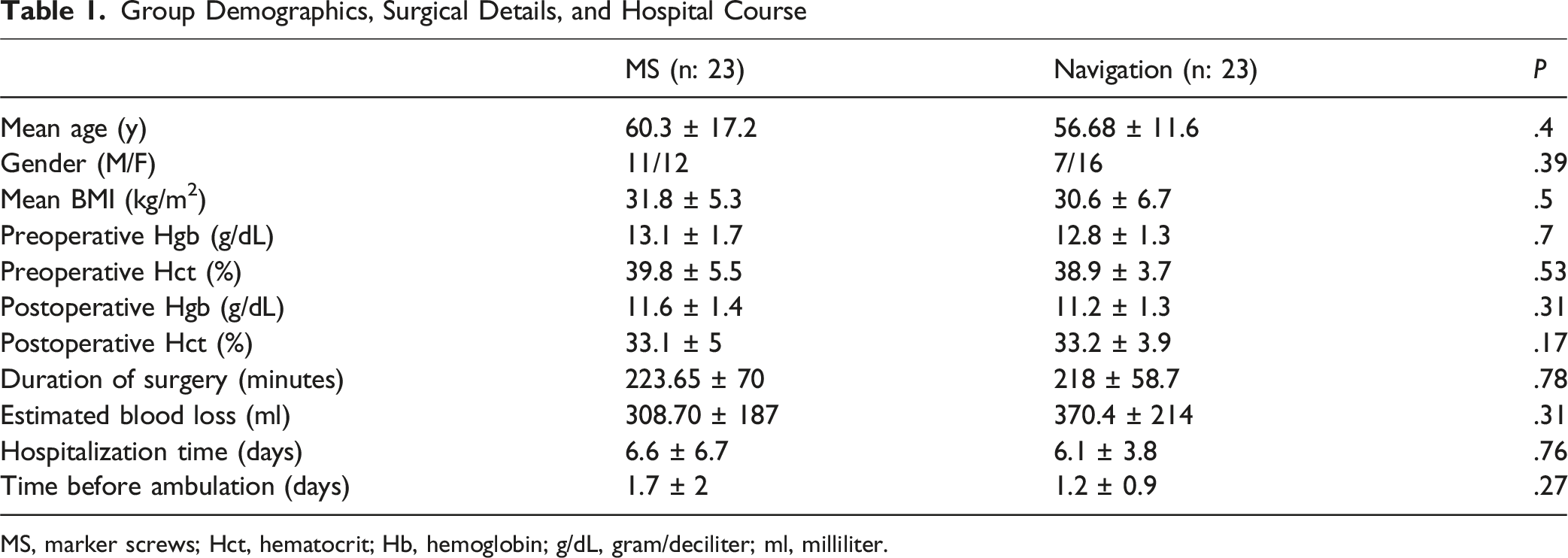
MS, marker screws; Hct, hematocrit; Hb, hemoglobin; g/dL, gram/deciliter; ml, milliliter.
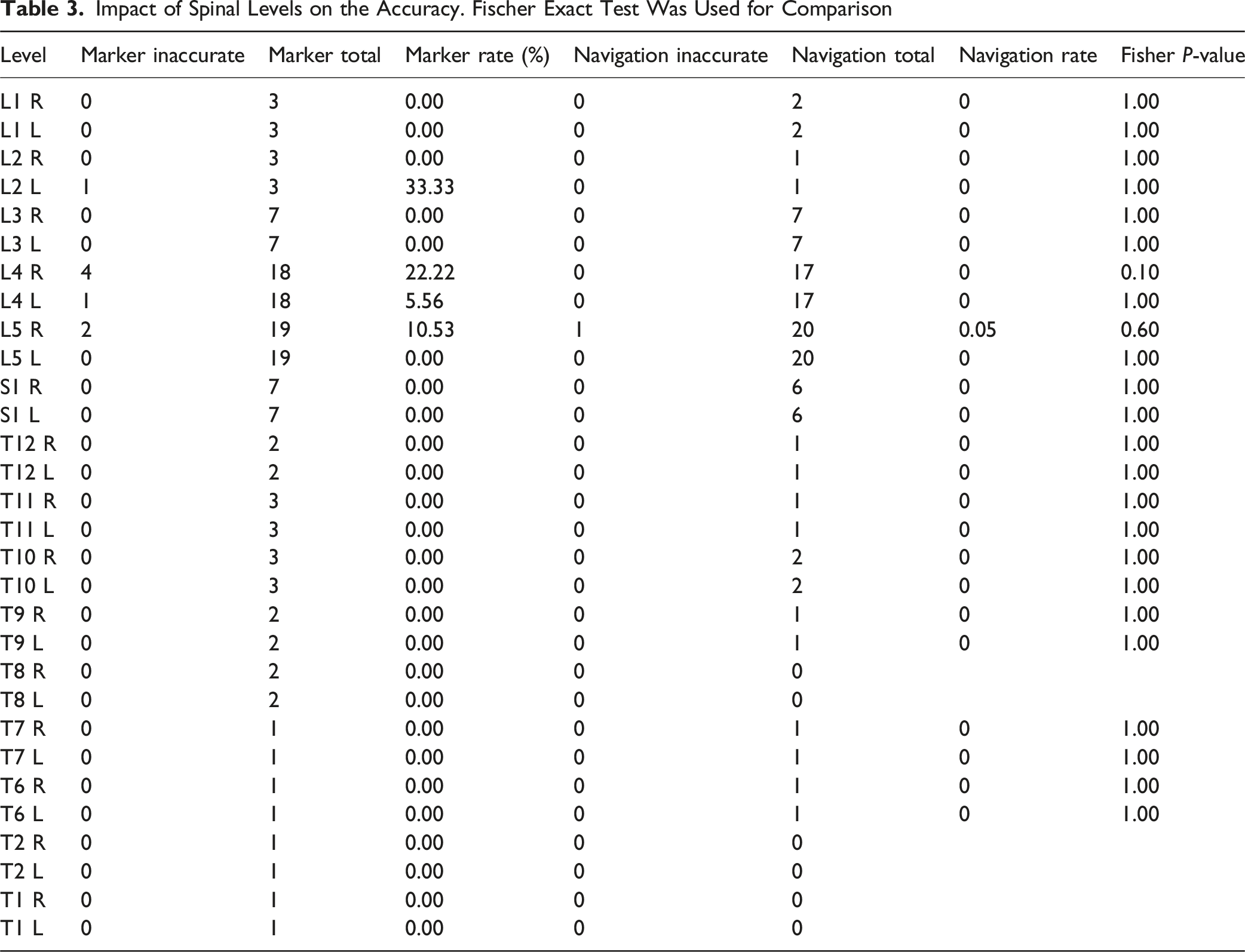
The Navigation technique showed an accuracy of 99.17% (119 accurate screws out of 120), while the Marker Screws technique showed an accuracy of 94.52% (138 accurate screws out of 146). The Navigation arm shows significantly higher accuracy with Fisher’s exact test (P: .043).
The difference in screw placement accuracy between the MS and navigation techniques was −4.6%. The 95% confidence interval for this difference ranged from −8.7% to −0.6%. Because the lower bound of the CI remained above the predefined non-inferiority margin of −10%, the MS technique met the criterion for non-inferiority (Figure 4). A bell chart comparing both techniques accuracy rates to the pre-determined non-inferiority margin
The number of screws inserted in the MS arm of the study was 146 screws. The number of screws inserted in the 3D navigation arm of the study was 120 screws, with the highest number of screws inserted at the levels L5 (38 screws in the MS arm and 40 in the Navigation arm), L4 (36 screws in the MS arm and 34 in the Navigation arm), and S1 (14 in the MS arm and 12 in the Navigation arm) (Figure 5). Number of screws inserted according to the spinal level
Distribution of Breaches According to the Affected Pedicle Wall
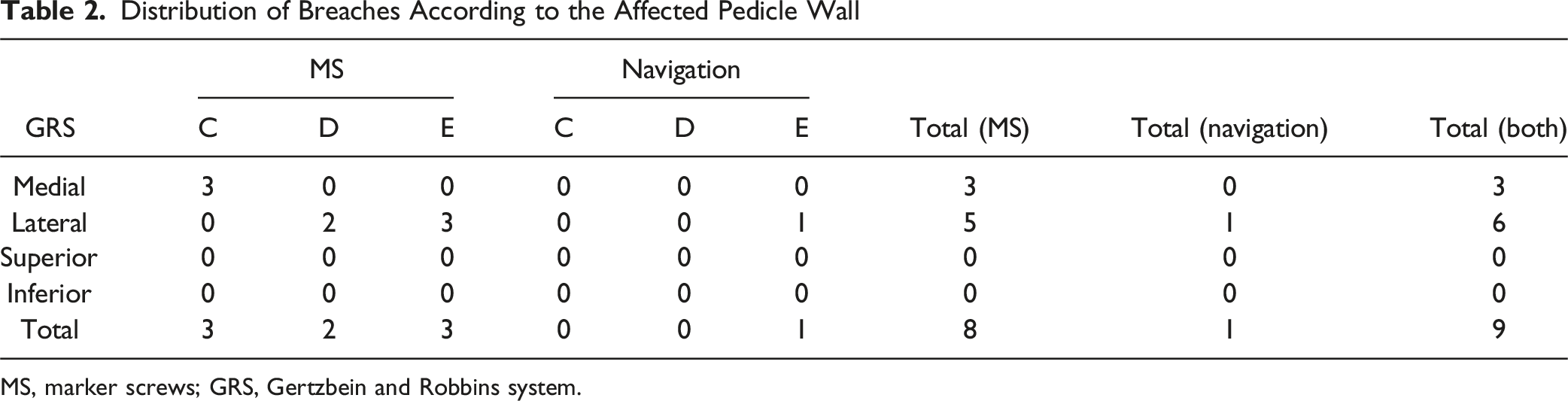
MS, marker screws; GRS, Gertzbein and Robbins system.
Comparing severe breaches between the two techniques showed no statistical significance.
There were 3 (medial wall) breaches in the Marker Screws arm and 0 in the Navigation arm. The difference between the two arms is not statistically significant (Fisher’s exact P: .13).
Impact of Spinal Levels on the Accuracy. Fischer Exact Test Was Used for Comparison
There were no patients that were taken to OR for revision surgery. No complications related to screw breaches were reported during the study period.
Discussion
The establishment of 3D spine fixation through pedicle screws has revolutionized the field of spine surgery, however, complications arising from mispositioning screws may result in neurological damage and vascular injury, which are significant concerns in spinal surgery. In this study, we introduce a modified free-hand technique utilizing MS to enhance accuracy and safety. This method shows promise for improving outcomes in spinal fixation techniques.
The pedicle screw insertion using the free-hand technique has demonstrated a wide range of accuracy in the literature, from 71% to 98%.31–33 This variability can be attributed to different techniques utilized and variations in surgical skills and experience. Our current findings indicate that the use of MS not only improves visualization but also enhances tactile landmarks, reducing the risk associated with malpositioning of pedicle screws, using the traditional free-hand technique although, recent advancements have introduced navigational technologies that offer improved accuracy, achieving rates above 95% however, these techniques necessitate additional equipment and often increase operational costs and exposure to ionizing radiation for both the surgical team and the patient. 34 In contrast, the modified MS free-hand technique retains the cost-effectiveness of traditional methods while providing accuracy comparable to those of navigated techniques.
Studies comparing various insertion techniques have consistently shown that while image-guided navigation improves screw placement accuracy, the technique may not significantly reduce complication rates compared to those of well-executed free-hand techniques. 23 Our study supports this notion by demonstrating that MS-guided techniques can yield similar results to those of navigated methods without the complexities associated with imaging technologies and radiation exposure. A systematic review reported the accuracy of the free-hand technique to be between 69% and 94%. With fluoroscopy assistance, the accuracy was reported to be between 28% and 85%. The accuracy of fluoroscopy navigation was reported to be between 81% and 92%, while CT navigation achieved an accuracy of 89% to 100%. 34 The MS technique described in this study had an accuracy of 94.52%, which is in the higher range compared to that of the aforementioned techniques.
Keeping in mind that the MS technique relies mainly on x-Xray and comparing it to the navigation system which is an advanced technology that incurs costs for establishment, maintenance, and continuous personnel training, the feasibility of the MS technique appears clearly. These costs of the Navigation technique are not always feasible for all institutions performing spine surgeries. Also, when comparing radiation exposure between the two techniques, the MS technique requires only a few X-ray shots, whereas the 3D or CT imaging needed for navigation. Although the MS technique may theoretically involve lower radiation exposure to patients and reduced costs compared with navigation-based systems, it may have increased radiation dose to surgent in compare to navigation. Moreover, radiation dose and cost analyses were not performed in this study.
Although complications could be devastating when pedicle screws are utilized10,35 the complication rates are low, rendering the use of pedicle screws in thoracic and lumbar spine surgery safe for achieving the intended clinical goals. This risk underscores the importance of improving surgical techniques to enhance both accuracy and safety. The complications that may arise from inserting pedicle screws range from minor breaches of the pedicle wall to more severe complications, such as injuring neural elements, which can lead to paraplegia with or without loss of sphincter control. Inserting long screws may disturb major blood vessels, causing bleeding that could be life-threatening. 26
In this study the lateral pedicle wall was most affected in both techniques, showing how the two techniques were comparable. Spine surgeons are particularly concerned that breaches of the medial pedicle wall carry a high potential for unwanted neurological complications. This concern might explain why the lateral wall was the most affected in this study.
All screws that were suspected of being misplaced during surgeries in both arms through fluoroscopy were revised intra-operatively, although none of the reported breaches in this study in both arms were detected intraoperatively with fluoroscopy as intraoperative fluoroscopy may have limited sensitivity for detecting certain pedicle breaches, particularly small medial or lateral cortical violations. 26 The rate of severe breaches C, D and E was 3.4% which is comparable to the literature. 31
Furthermore, an important advantage of the MS technique lies in its educational value and suitability for surgical training. Unlike navigation technique, which may reduce reliance on anatomical landmarks, the MS technique reinforces fundamental principles of pedicle anatomy, entry point selection, and trajectory planning. This is particularly relevant for residents and junior spine surgeons, as it facilitates the development of tactile feedback and spatial understanding that are essential for safe free-hand instrumentation.
Although the MS technique has an inherent learning curve, this characteristic may be advantageous rather than detrimental in training environments. Under appropriate supervision, trainees can progressively refine their skills while maintaining acceptable accuracy and safety. In this study, most screws were placed by trainees under senior supervision, yet accuracy remained high and without complications, supporting the feasibility of this technique as both a primary and backup method in spine surgery training programs.
The navigation technique relies on the stable positioning of reference tools throughout the surgery. The reference tool is typically attached to a bony structure (usually the spinous process) proximal or distal to the levels intended for fixation. Breakage of the bony structure to which the reference tool is attached, or minor changes in the reference frame position due to being nudged by the surgeons or during the movement of the bulky O-arm, may cause inaccuracies in the positioning process. Any change in the position of the reference will result in faulty positioning. Surgeons trained solely in the navigation technique might find detecting incorrect entry points and trajectories challenging. In contrast, surgeons with extensive knowledge of anatomical structures and reference points for placing spine instrumentation may have a better sense of when navigation systems have deviated from accuracy. Surgeons trained in both free-hand and modified free-hand techniques, such as the MS technique, may be better equipped to perform surgeries when technology fails for any reason.
Utilizing MS is considered safe when considering injuring neural components and if they were inserted in a wrong level; the neural canal is 20 mm away from the entry point of a pedicle screw and the usually utilized MS are 12 mm in length, with regard to they being inserted in the wrong level as proven by the control anteroposterior and lateral views they could just be removed and the pilot hole sealed by bone wax as no actual anatomical disturbance occurs and no disturbance of the facets or other vital structures.
Overall, our results suggest that the MS technique is not only viable but might be advantageous in the current landscape of spinal surgery, in which balancing precision, cost, and safety is crucial. As we move forward, further investigating the long-term outcomes associated with this technique across varied surgical contexts and patient populations will be essential.
Navigation become central in minimally invasive spine surgery (MIS) due to limited exposure, however MS technique can be utilized through minimally invasive exposure as described in previous study by Khashab et al. 24 Although MIS was not a part of this study in hands, when MS is utilized in MIS the same standard skin marking is made utilizing an image intensifier. A mark is placed 1 cm lateral to the lateral pedicle wall after the levels intended to be fixed are marked. Instead of utilizing a longitudinal slit for each screw, a single longitudinal incision is made no longer than 1 inch when a single level is intended to be fixed. Special sequential tubular dilators are then used to establish an intramuscular corridor utilizing the Wiltse approach. The posterior elements are then exposed showing the pars, the transverse processes and the facets. The anatomical landmarks are used to insert he MS and then the image intensifier is used to obtain the AP and Lateral views needed for the modified free hand technique for the pedicle screws insertion.
Some limitations specific to the MS technique include a learning curve, as the technique relies on the free-hand method for instrumentation, the difficulties that would incur in case of altered anatomy, as the MS technique depends on anatomical landmarks, in altered anatomy, such as in severe deformities, tumors, and infections, its accuracy may be potentially reduced, these pathologies were not included in this study. Lastly, osteoporotic bone may challenge MS utilization, as the pins may have poor purchase, and pilot holes may risk fractures of weakened bony elements, such as facets, the pars interarticularis or transverse process. Also, limitations of the current study include its single-center design, the limited range of included pathologies, and the outcome of the breaches, which, despite not being clinically significant, may require a larger sample size to detect significant differences and outcomes.
Directions for future research include investigating the accuracy of the MS technique across a wider range of spinal pathologies, including deformities and tumors, precise measurements of radiation exposure, which was not part of this study, accurate cost analysis, and studies with larger samples in multicenter settings.
Conclusion
The MS technique provides a comparable accuracy, feasible, and less costly alternative to the 3D navigation technique for pedicle screw placement. MS carries a lower risk of potential complications, including reduced radiation exposure for both surgeons and patients. Additionally, the technique offers excellent teaching and learning potential that can serve as a backup technique in case of loss of accuracy or technical failure of the 3D navigation system.
The marker screw technique demonstrates comparable accuracy to three-dimensional navigation for thoracic and lumbar pedicle screw placement while remaining within the predefined non-inferiority margin. The technique is safe, feasible, and broadly applicable, with potential advantages related to availability, workflow, and surgical training. The MS technique may serve as a valuable alternative or adjunct to navigation, particularly in training environments and in settings where advanced navigation systems are not readily available.
Footnotes
Ethical Considerations
Institutional review board approval was obtained for King Abdullah International Medical Research Centre Study. Approval number (RJ19/107/J). Informed consent was signed by participants willing to be included.
Consent to Participate
Participants have signed informed consent accepting participation in the study.
Author Contributions
Conceptualization: MAK, ME, MMA RAA. Methodology: MAK, ME, MMA RAA. Software: ME. Data curation: MMA. Formal analysis: ME and MMA. Writing—original draft preparation: MAK, MMA and ME. Writing—review and editing: MAK, ME, MMA RAA. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author (MMA) upon reasonable request.