
Abstract
Study Design
Retrospective observational study.
Objectives
To determine whether the preoperative adjacent disc vacuum phenomenon (ADVP) is associated with an increased risk of adjacent vertebral fracture (AVF) after balloon kyphoplasty (BKP) for osteoporotic vertebral fractures.
Methods
The clinical and radiological data of 124 consecutive patients who underwent BKP at T11–L2 were retrospectively reviewed. ADVP was defined as radiolucent gas within the intervertebral disc space on preoperative computed tomography (CT). Patients were classified as ADVP-positive or ADVP-negative. The incidence of AVF was compared between the groups, and independent risk factors were assessed using multivariate logistic regression. Multiple imputation was performed, and propensity score matching (PSM) was used to adjust for potential confounding factors because bone mineral density data were partially missing.
Results
ADVP was identified in 48 patients (38.7%). AVF occurred in 21 patients (16.9%) and was significantly more frequent in the ADVP-positive group than in the ADVP-negative group (31.2% vs 7.9%; P < 0.01). Univariate analysis showed that the presence of ADVP and longer symptom duration were significantly associated with AVF. Multivariate logistic regression identified ADVP as an independent risk factor for AVF (odds ratio 4.97; 95% confidence interval 1.71-14.5; P = 0.003). This association remained consistent after multiple imputation and PSM.
Conclusions
Preoperative ADVP is associated with an increased risk of AVF after BKP. Incorporating the assessment of ADVP into preoperative CT evaluation may help identify patients at a higher risk of AVF.
Introduction
Osteoporotic vertebral fractures (OVFs) are among the most common fractures in older adults, and their incidence is rising with population aging. 1 OVFs can lead to persistent pain, reduced activities of daily living (ADL), 2 systemic complications, and higher mortality. 3 Early and appropriate management is therefore important.
Balloon kyphoplasty (BKP) is widely used to treat OVFs. Studies have shown that BKP provides pain relief, 4 improves ADL and quality of life, prevents vertebral deformity, 5 and may reduce mortality. 6
However, adjacent vertebral fracture (AVF) is the most frequent complication after BKP, with reported rates of 9.9%-30.8%.7-11 AVF can cause recurrent back pain and reduced ADL, and may lead to progressive local kyphosis or require additional surgery. Identifying patients at high risk for AVF is therefore clinically important. 12 Reported risk factors include low bone mineral density (BMD), intravertebral clefts, cement volume, local kyphosis, and pre-existing vertebral fractures. 9 Wilson et al showed that vertebrae augmented with polymethylmethacrylate (PMMA) are stiffer than untreated fractured vertebrae, 13 which may increase mechanical stress on adjacent levels and contribute to AVF. Beyond vertebral and cement-related factors, disc-level changes may also influence the risk of AVF. Specifically, intradiscal cement leakage has been implicated as a potential risk factor for AVF, indicating that alterations in disc biomechanics at the treated segment may predispose adjacent vertebrae to fracture. 14
The intradiscal vacuum phenomenon (VP) refers to radiolucent gas within the disc and is commonly associated with disc degeneration. 15 VP has also been observed in discs adjacent to fractured vertebrae.16-18 In the present study, we examined adjacent disc VP (ADVP) and its association with AVF after BKP. Recent studies suggest that VP may indicate both degenerative changes and spinal instability.19,20 These findings indicate that VP may reflect biomechanical stress at the affected segment and predispose the adjacent vertebrae to fracture. However, the association between ADVP and AVF development after BKP remains unclear.
We hypothesized that ADVP is associated with an increased risk of AVF after BKP. This study aimed to evaluate the association between ADVP and subsequent AVF.
Methods
Study Design and Patient Selection
We conducted a retrospective observational study across 4 institutions (1 university hospital and 3 affiliated hospitals) from April 2017 to March 2021. This study included consecutive patients who underwent BKP for OVFs.
OVFs were diagnosed based on clinical symptoms and imaging findings. Clinical symptoms include acute or subacute lower back pain, tenderness on percussion over the involved spinous process, and pain aggravated by standing or movement. Imaging findings included bone marrow edema on magnetic resonance imaging (MRI), identified mainly on short tau inversion recovery (STIR) or T1-weighted and T2-weighted sequences, and typical findings on computed tomography (CT), such as trabecular fracture lines, cortical disruption, endplate depression, or intravertebral cleft formation. Pre-existing vertebral fractures were defined as old vertebral compression fractures with sclerotic margins without bone marrow edema at the time of BKP.
The inclusion criteria were as follows: (1) BKP performed at the T11–L2 levels; (2) Minimum follow-up of 3 months; (3) Availability of preoperative CT images.
We limited the study to T11–L2 fractures because this region represents the thoracolumbar junction, where OVFs are most common, thus restricting the level of reduced anatomical heterogeneity.
The exclusion criteria were as follows: (1) Prior spinal surgery; (2) Multiple acute vertebral fractures or multilevel BKP; (3) Combined decompression or fusion procedures.
Patients with multiple acute vertebral fractures or multilevel BKP were excluded to maintain a more homogeneous cohort, because postoperative subsequent vertebral fractures in such cases may be difficult to assess in the same way as in patients with a single fractured vertebra.
This retrospective study was approved by the institutional ethics committee of our institution (Approval No. 3052). Patient consent was obtained through an opt-out process, as permitted by our institutional ethics committee.
Surgical Procedure
BKP was performed under general anesthesia using the Kyphon system (Medtronic Spine LLC, Sunnyvale, CA, USA). The patients were placed prone on a four-poster frame. A balloon was inserted into the vertebral body via a bilateral transpedicular approach and inflated under manometric control (maximum 400 psi) to restore vertebral height and create a cavity. After balloon deflation and removal, the cavity was filled with PMMA cement under low pressure. Patients were allowed to ambulate on the first postoperative day and were generally instructed to wear a thoracolumbar brace for 3 months after surgery. Thereafter, continuation of brace use was left to the discretion of the attending physician.
Patient Demographics and Operative Data
Recorded variables included age, sex, fracture level, symptom duration, presence of pre-existing vertebral fractures, follow-up duration, cement volume, postoperative osteoporosis treatment, and preoperative BMD. Postoperative osteoporosis treatment was defined as the presence or absence of pharmacological treatment after surgery. In patients who received postoperative osteoporosis treatment, medications were categorized as anabolic agents, antiresorptive agents, or other agents. Anabolic agents included parathyroid hormone analogs (teriparatide) and an anti-sclerostin antibody (romosozumab). Antiresorptive agents included bisphosphonates and denosumab. Other agents used included active vitamin D monotherapy and selective estrogen receptor modulators. Preoperative BMD was measured using dual-energy X-ray absorptiometry (DXA) and expressed as the average T-score of the lumbar spine (L1–L4) and femoral neck.
Radiological Assessments
VP was assessed on preoperative sagittal CT images and defined as radiolucent gas within the intervertebral disc space. Patients were classified as ADVP-positive (ADVP+) if ADVP was present in 1 or both adjacent discs, and ADVP-negative (ADVP−) if absent in both (Figure 1). Assessment of the adjacent disc vacuum phenomenon (ADVP) on sagittal CT images. ADVP-positive (ADVP+) was defined as the presence of vacuum phenomenon in either the cranial or caudal adjacent disc, or in both.
Preoperative CT images were also used to evaluate intravertebral clefts, endplate fractures, and posterior wall fractures. An intravertebral cleft was defined as a linear or cystic vacuum or fluid-filled space within the vertebral body. An endplate fracture was defined as a disruption or depression of the superior or inferior endplate, and a posterior wall fracture was defined as a cortical break or retropulsion of the posterior vertebral wall. Standing lateral radiographs were routinely obtained at 1, 3, 6, and 12 months postoperatively, and annually thereafter, or whenever new back pain developed. As this was a retrospective multicenter study, the actual timing and duration of follow-up were not identical across all patients. Therefore, only patients with at least 3 months of clinical and radiographic follow-up were included in the analysis. AVF was defined as a new morphological fracture of a vertebra adjacent to the treated level. AVF was identified by reduced height of the adjacent vertebral body on plain X-ray, or by increased signal intensity on fat-suppressed T2-weighted MRI and decreased signal on T1-weighted MRI, with or without new-onset back pain.
Plain lateral radiographs obtained preoperatively, immediately postoperatively, and at the final follow-up were analyzed for radiographic assessment. The wedge angle of the fractured vertebra and the local kyphosis angle (LKA), defined by the superior endplate of the cephalad vertebra and the inferior endplate of the caudal vertebra, were measured (Figure 2A).9,21 Anterior and posterior vertebral body heights were measured, and the relative anterior height was calculated using the formula: (A) The local kyphosis including the upper and lower units = α degree. The wedge angle of the vertebral body = β degree; (B) Percentage height of the anterior wall as calculated by the following formula: [2a/(b+c)]×100. 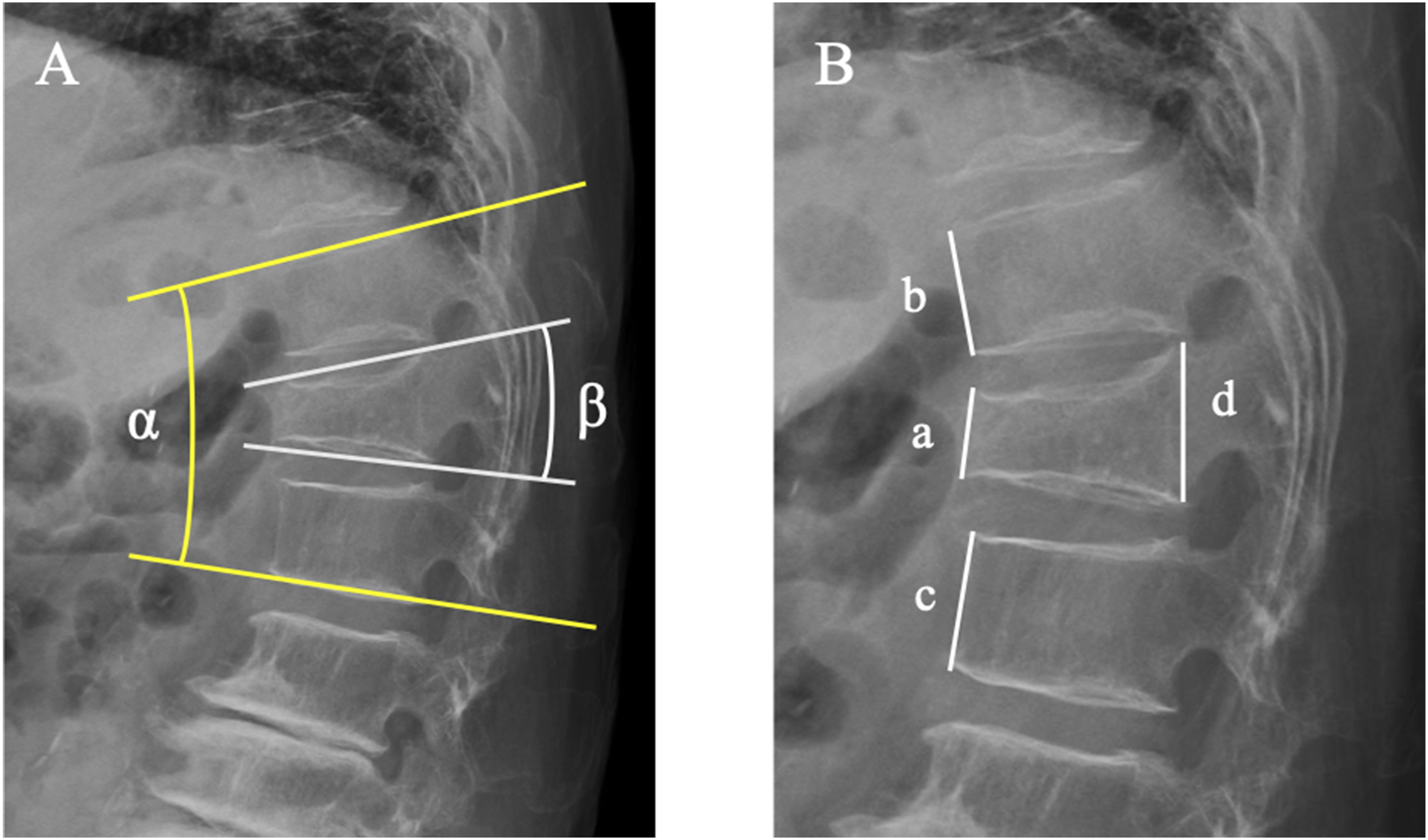
Relative anterior height = [2a/(b + c)]×100 (Figure 2B).9,21
Changes in wedge angle, LKA, and relative anterior height from immediately postoperative to the final follow-up were defined as Δwedge angle, ΔLKA, and Δrelative anterior height, respectively.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median (interquartile range), and categorical variables as counts (percentage). Comparisons between groups were performed using the Student’s t-test or Mann–Whitney U-test for continuous variables, and Pearson’s chi-square test or Fisher’s exact test for categorical variables.
Multivariate logistic regression analysis was conducted to estimate odds ratios (ORs) and 95% confidence intervals (CIs), and to identify factors associated with AVF. AVF was used as the dependent variable, and clinically relevant variables, including those that were significant in the univariate analysis, were included as independent variables.
Initial analyses included all patients regardless of BMD availability due to missing data in some cases. For the subanalysis, missing BMD values were imputed using multiple imputation by chained equations (MICE), assuming that data were missing at random. The imputation model included age, sex, fracture level, time to surgery, presence of an intravertebral cleft, ADVP status, and AVF occurrence. A total of m = 100 imputed datasets were generated, each with 100 iterations. Within each imputed dataset, propensity score matching (PSM) was performed to compare outcomes between the ADVP+ and ADVP− groups. Covariates for matching included age, sex, time to surgery, presence of an intravertebral cleft, and lumbar BMD. 1:1 nearest-neighbor matching without replacement was conducted using a caliper width of 0.2 standard deviations of the propensity score logit. Covariate balance before and after matching was assessed using standardized mean differences (SMD). After PSM, AVF incidence was compared between the ADVP+ and ADVP− groups within each imputed dataset using Fisher’s exact test. Incidence was reported as the cumulative incidence (incidence proportion) during follow-up (n/N). The resulting P-values were summarized across the imputed datasets. To account for small-sample bias and potential separation after matching, Firth’s penalized logistic regression was applied to each imputed and matched dataset to estimate the association between ADVP and AVF. The effect estimates from Firth’s penalized logistic regression were descriptively summarized across imputations.
As a supplementary analysis, PSM was also performed using age, sex, symptom duration, intravertebral cleft, and preoperative LKA. Because these variables had no missing values, the analysis was conducted without multiple imputation.
All statistical analyses were performed using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). A two-tailed P-value <0.05 was considered statistically significant.
This study adhered to the STROBE statement (Supplemental Table).
Results
Patient Characteristics
Among the 209 patients who underwent BKP during the study period, 34 treated at levels outside T11–L2, 7 without CT evaluation, 25 with follow-up shorter than 3 months, 12 with prior spinal surgery, 6 with multiple acute vertebral fractures, and 1 who underwent combined fusion surgery were excluded (Flowchart, Figure 3). Consequently, 124 patients (54 men and 70 women) were included in the analysis. The mean age at surgery was 79.65 ± 8.34 years, and the median follow-up was 12.00 months (IQR, 6.00-12.00 months; range, 3.00-16.00 months). The treatment levels were distributed as follows: T11, 8 patients; T12, 39 patients; L1, 55 patients; and L2, 22 patients. Perioperative complications were also reviewed. Cement leakage was observed in 14 patients (11.3%); however, no symptomatic cement leakage or revision surgery was observed. In addition to the missing BMD values in 37 patients (29.8%), no other variables had missing data. A flowchart of patient selection. 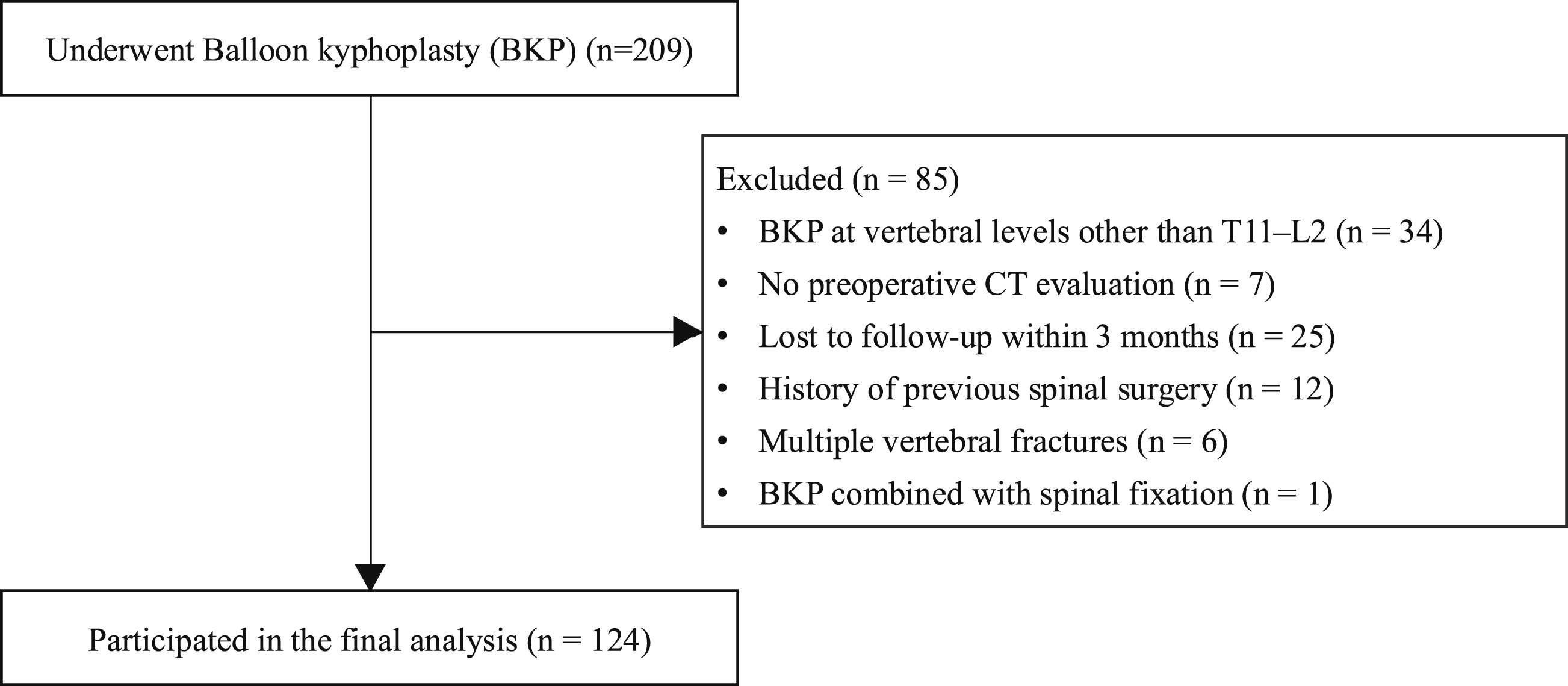
Patients Demographics (N = 124)
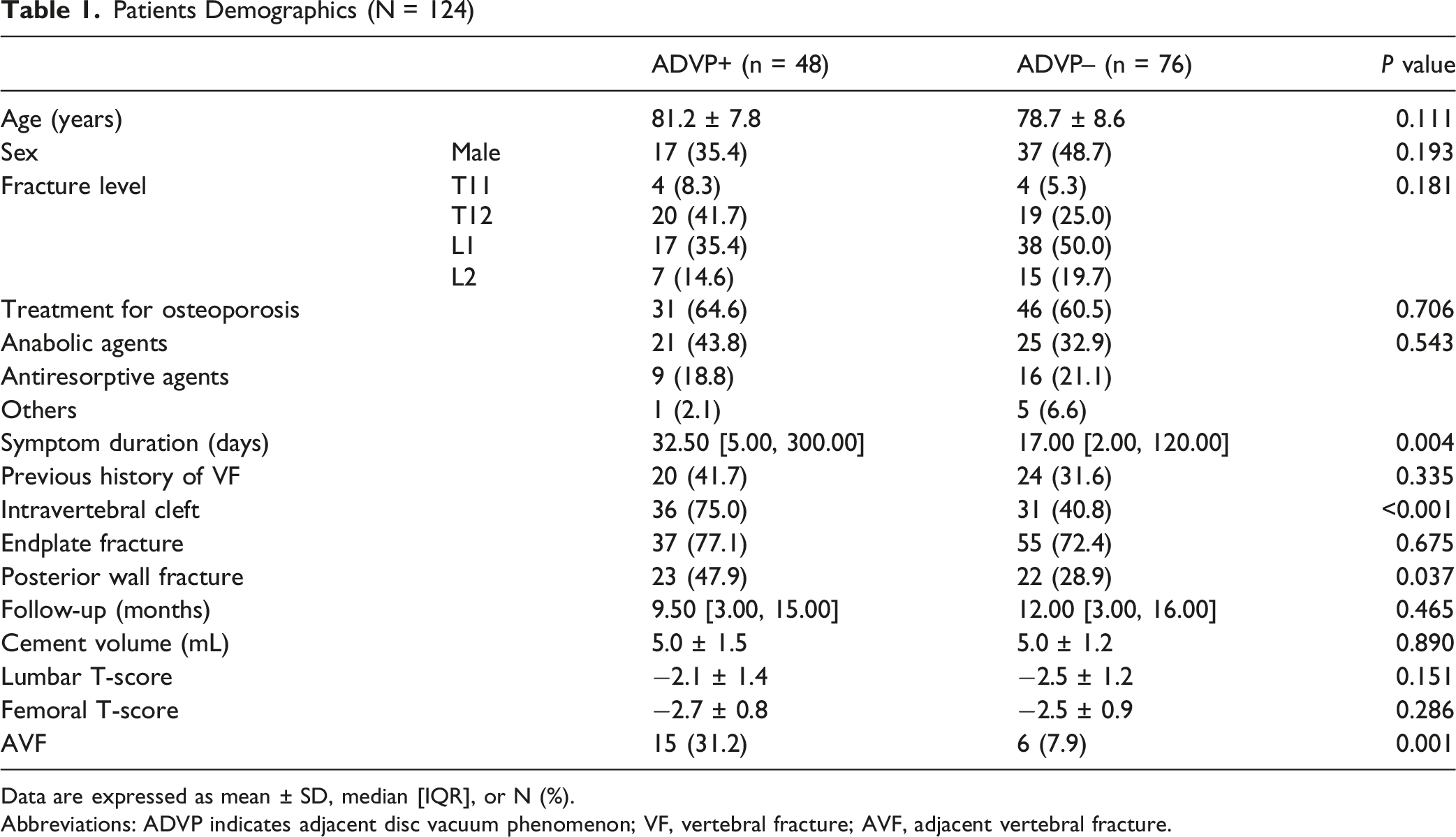
Data are expressed as mean ± SD, median [IQR], or N (%).
Abbreviations: ADVP indicates adjacent disc vacuum phenomenon; VF, vertebral fracture; AVF, adjacent vertebral fracture.
Association Between the Location of Adjacent Disc Vacuum Phenomenon (ADVP) and the Location of Adjacent Vertebral Fracture (AVF)
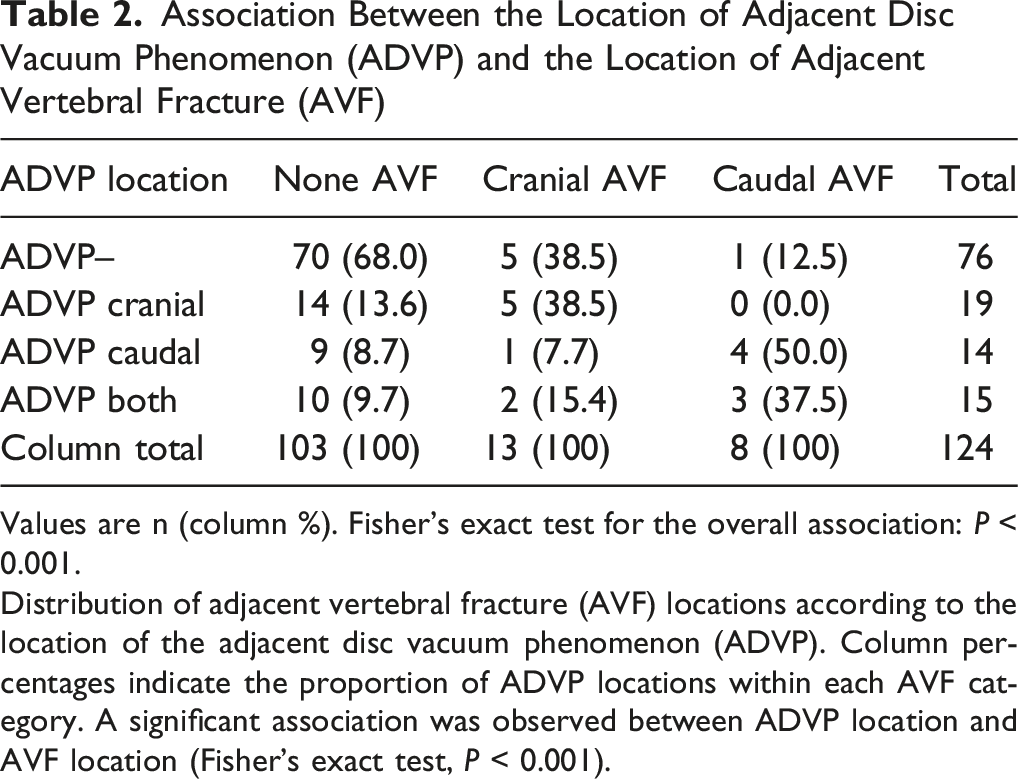
Values are n (column %). Fisher’s exact test for the overall association: P < 0.001.
Distribution of adjacent vertebral fracture (AVF) locations according to the location of the adjacent disc vacuum phenomenon (ADVP). Column percentages indicate the proportion of ADVP locations within each AVF category. A significant association was observed between ADVP location and AVF location (Fisher’s exact test, P < 0.001).
Incidence of AVF and Multivariate Logistic Regression Analysis
Baseline Characteristics by Adjacent Vertebral Fracture (AVF) Status
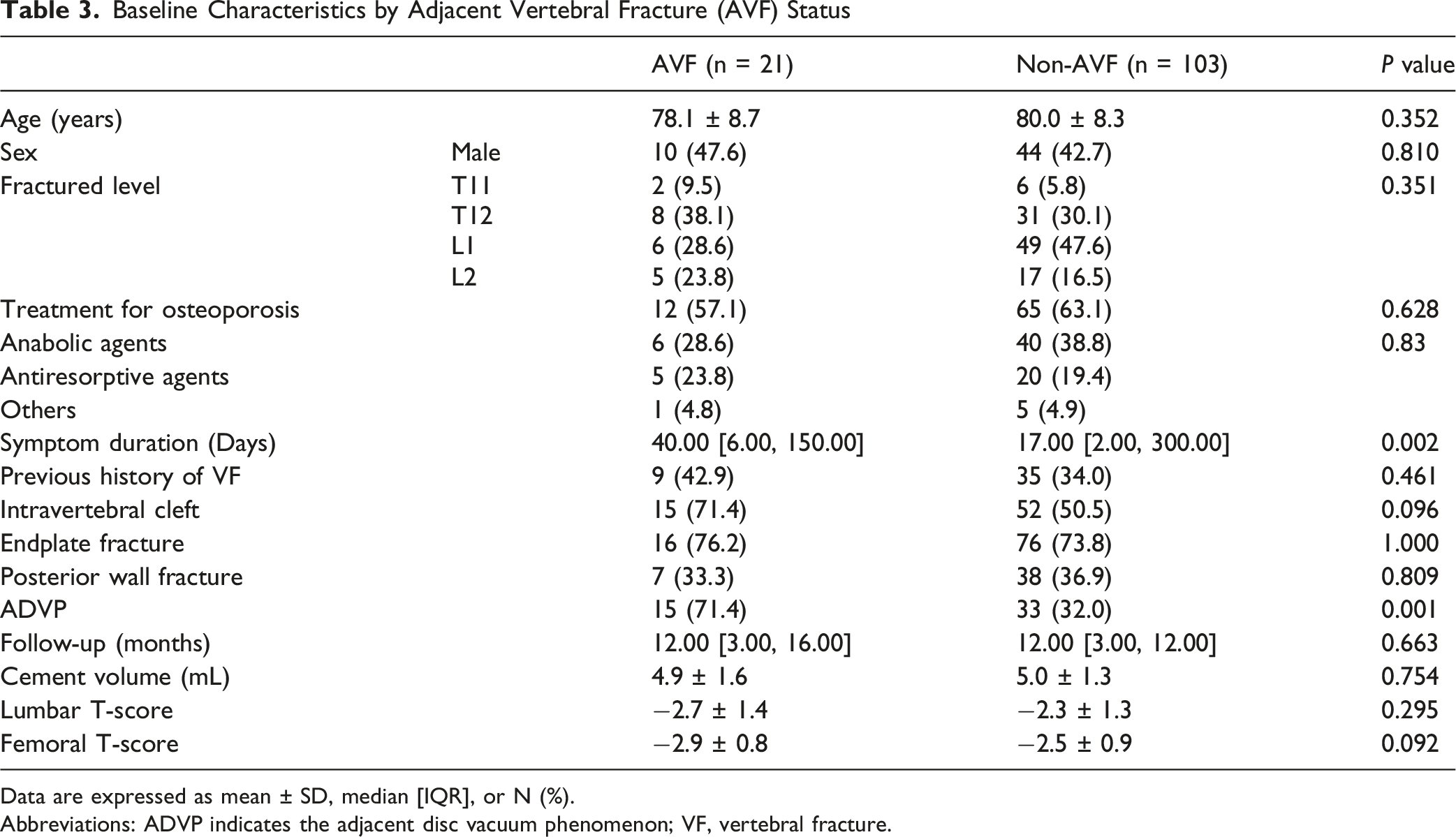
Data are expressed as mean ± SD, median [IQR], or N (%).
Abbreviations: ADVP indicates the adjacent disc vacuum phenomenon; VF, vertebral fracture.
Multivariable Logistic Regression Analysis for Adjacent Vertebral Fracture
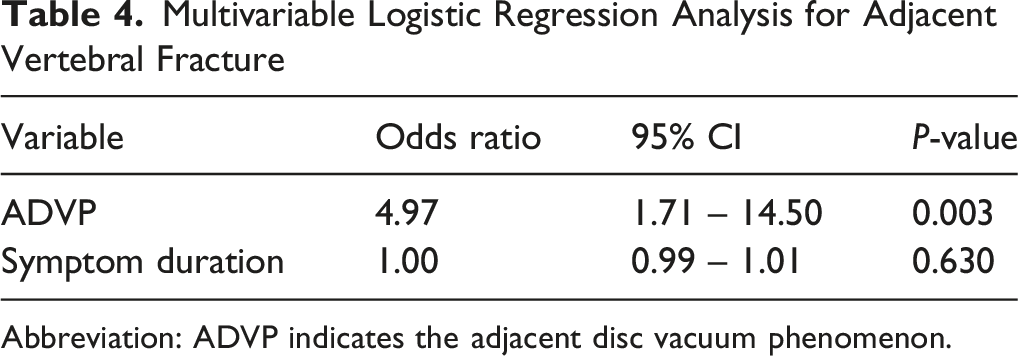
Abbreviation: ADVP indicates the adjacent disc vacuum phenomenon.
In sensitivity analyses, ADVP remained significantly associated with AVF after adjustment for intravertebral cleft (OR 4.67, 95% CI 1.58-13.80, P = 0.005) and after adjustment for femoral T-score in a complete-case analysis of 87 patients (OR 6.83, 95% CI 1.90-24.60, P = 0.003) (Supplemental Tables 1 and 2).
Radiological Assessments
Comparison of Radiographic Parameters
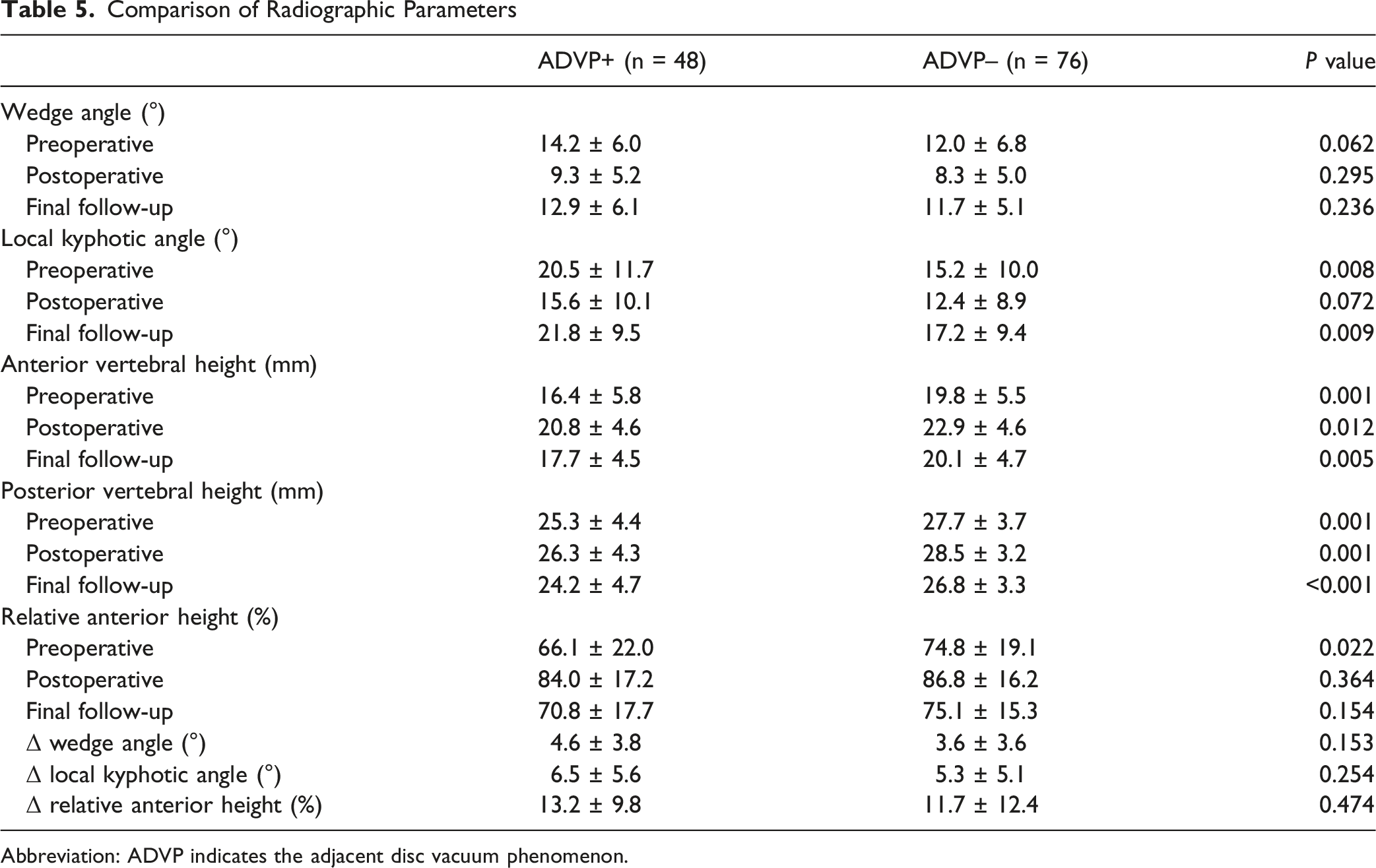
Abbreviation: ADVP indicates the adjacent disc vacuum phenomenon.
There were no significant differences in the Δwedge angle (P = 0.15), ΔLKA (P = 0.44), or Δrelative anterior height (P = 0.25).
Multiple Imputation and PSM
Baseline Characteristics of the Representative Patients After Propensity Score Matching
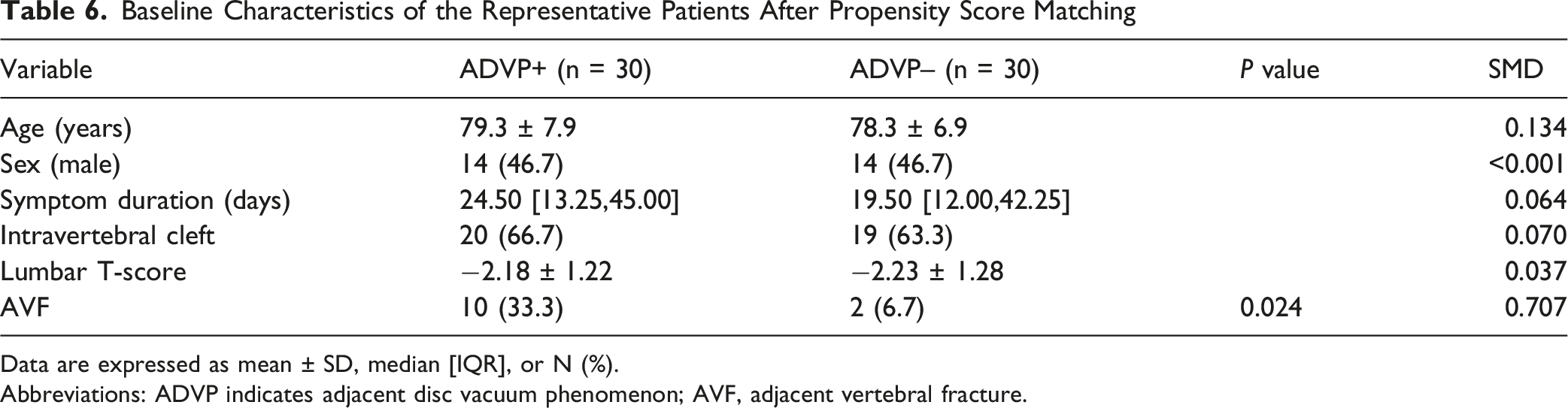
Data are expressed as mean ± SD, median [IQR], or N (%).
Abbreviations: ADVP indicates adjacent disc vacuum phenomenon; AVF, adjacent vertebral fracture.
Distribution of Adjacent Vertebral Fracture Incidence Across 100 Imputed Datasets
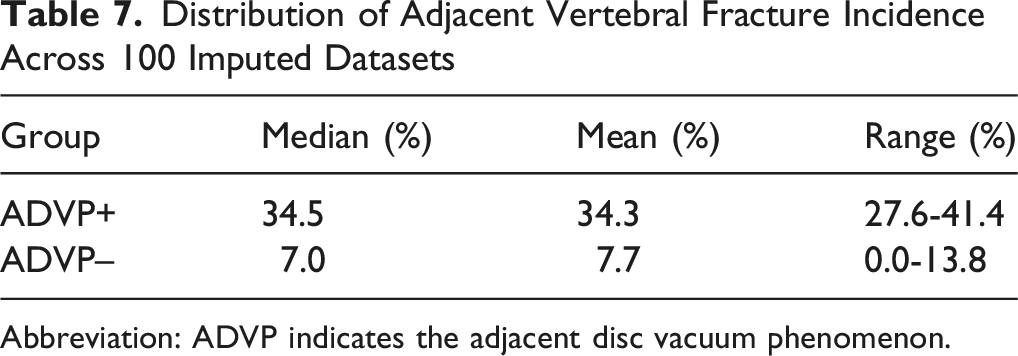
Abbreviation: ADVP indicates the adjacent disc vacuum phenomenon.
Results of Pooled Firth’s Penalized Logistic Regression After Multiple Imputation and Propensity Score Matching
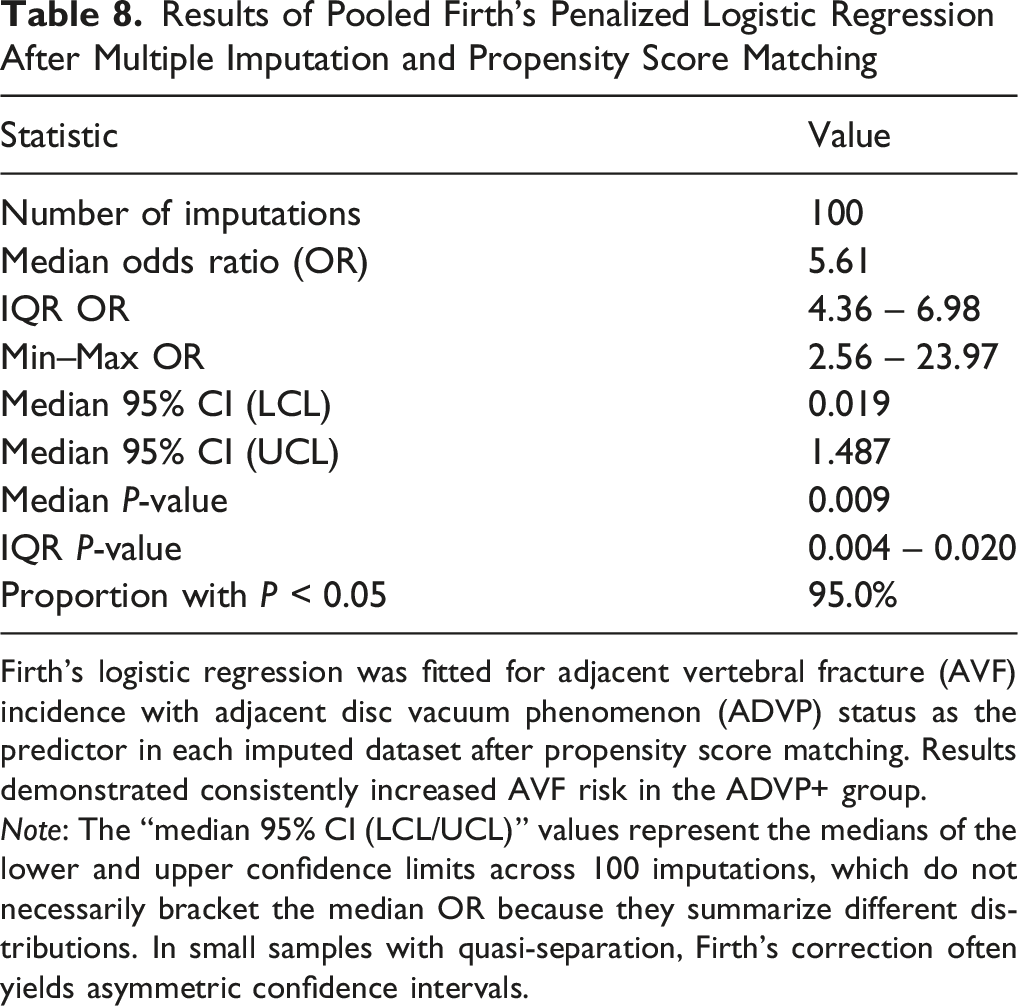
Firth’s logistic regression was fitted for adjacent vertebral fracture (AVF) incidence with adjacent disc vacuum phenomenon (ADVP) status as the predictor in each imputed dataset after propensity score matching. Results demonstrated consistently increased AVF risk in the ADVP+ group.
Note: The “median 95% CI (LCL/UCL)” values represent the medians of the lower and upper confidence limits across 100 imputations, which do not necessarily bracket the median OR because they summarize different distributions. In small samples with quasi-separation, Firth’s correction often yields asymmetric confidence intervals.
Because patients with ADVP+ tended to show greater baseline deformity, an additional PSM analysis, including preoperative LKA, was performed. In the matched cohort, the incidence of AVF remained higher in the ADVP+ group than in the ADVP− group (29.0% vs 9.7%), although the difference was not statistically significant (Supplemental Table 3).
Discussion
This study is the first to show that preoperative ADVP is a risk factor for AVF after BKP. AVF occurred more frequently in patients with ADVP, with an approximately five-fold increase in risk compared with those without ADVP. This association remained significant after adjustment for confounders and was robust across propensity score–matched analyses and sensitivity analyses using multiple imputation and Firth penalized logistic regression. These findings indicate that preoperative CT evaluation of ADVP may help identify patients at a higher risk of AVF following BKP.
AVF is the most common complication following BKP, with reported incidence rates as high as approximately 30%.7-11 In this study, AVF occurred in 16.9% of all patients, increasing to 31.2% among those with adjacent disc VP, higher than previously reported incidence rates. Multivariate logistic regression confirmed ADVP as an independent risk factor for AVF, and this association persisted in propensity score–matched analysis. Prior studies have identified several AVF risk factors, including age, 10 female sex, low BMD, 22 local kyphosis, 7 thoracolumbar junction fracture, pre-existing vertebral fractures, 9 intravertebral instability, symptom duration, and intravertebral cleft. 12 However, few studies have specifically examined adjacent intervertebral discs. Our results demonstrate that ADVP contributes to AVF risk even after adjusting for confounders, and the location of ADVP corresponded to the level at which AVF occurred. These findings suggest that ADVP may serve as a useful preoperative predictor of AVF. Recent studies have also suggested that the condition of the adjacent discs may be relevant to AVF after vertebral augmentation. Tao et al reported that more advanced adjacent disc degeneration, assessed using the Pfirrmann grade, was associated with AVF after percutaneous kyphoplasty. 23 Takano et al also observed a higher prevalence of ADVP in patients with AVF after BKP than in those without AVF, although the difference did not reach statistical significance. 24 These findings, which are consistent with our results, suggest that the condition of the adjacent intervertebral disc may be involved in the development of AVF. In this context, our findings support the potential value of ADVP as a simple preoperative imaging marker for risk stratification after BKP.
In the ADVP+ group, greater preoperative local kyphosis, larger wedge angles, and reduced vertebral body height indicated more advanced vertebral collapse. However, ADVP itself was not associated with postoperative changes in vertebral collapse or kyphosis. Previous reports indicate that local kyphosis may worsen after BKP, 8 and that injury to the disc–endplate complex may contribute to postoperative deformity progression. In our cohort, segments with ADVP exhibited more severe preoperative deformity, whereas both groups showed similar changes in wedge angle and local kyphosis. One possible explanation is that vertebrae with ADVP had limited potential for further progression due to advanced collapse at the time of surgery. In this context, ADVP may primarily function as a radiological marker of advanced vertebral deformity and disc–endplate complex failure rather than as a direct driver of postoperative kyphotic progression.
VP has been strongly associated with intervertebral disc degeneration. 25 CT-detected VP is associated with reduced disc height, higher Pfirrmann grades, and intradiscal fluid accumulation on MRI.26-28VP has also been associated with angular instability 19 and abnormal vertical motion. 20 PMMA-augmented vertebrae exhibit greater stiffness than untreated fractured vertebrae; consequently, disc degeneration and segmental hypermobility may increase mechanical stress on adjacent vertebrae and contribute to AVF. 13 The finding that the ADVP site (cranial, caudal, or both) corresponded to the level at which AVF occurred supports the concept that ADVP reflects localized biomechanical overload at the adjacent segment. Clinically, ADVP in the cranial disc may preferentially increase the risk of cranial AVF, whereas ADVP in the caudal disc may predispose patients to caudal AVF.
Previous studies have explored the mechanisms underlying ADVP formation after vertebral fractures. Schömig et al reported that endplate injury may contribute to delayed VP development. 18 In this study, patients in the ADVP+ group had a longer symptom duration. VP may not manifest immediately after a fracture but may instead develop gradually over time. Previous studies by Hijikata and Takahashi have also reported delayed surgery as a risk factor for AVF, and progressive VP formation, reflecting ongoing disc degeneration, may be part of this process.9,12 In this study, patients with ADVP had a longer interval between injury and surgery, as well as higher rates of posterior wall fracture and intravertebral cleft. ADVP may develop progressively after a fracture as disc degeneration and segmental instability progress. Progressive VP formation, reflecting ongoing disc and endplate degeneration, may represent a key intermediate step in this pathological pathway. Although symptom duration was associated with AVF in the univariate analysis, this association was attenuated after adjustment for ADVP. This finding may suggest that symptom duration partly reflects fracture chronicity or severity-related changes that overlap with ADVP, rather than representing a clearly independent predictor.
This study had several limitations. First, the number of AVF events was limited, resulting in reduced statistical precision in the multivariable analysis, as reflected by the relatively wide confidence interval for ADVP. Therefore, the magnitude of this association should be cautiously interpreted. Residual confounding among severity-related variables also cannot be completely excluded. Larger studies are required to confirm these findings. Second, the follow-up was limited to a minimum duration of 3 months. Although most AVFs occur within 2 months after BKP, 29 late-onset AVFs could not be evaluated. In addition, the follow-up duration was not uniform across patients. Because subsequent vertebral fractures after vertebral augmentation are time-dependent events and have been evaluated using time-to-event methods in previous studies, heterogeneous follow-up periods may have influenced event detection in our cohort.30,31 Although no significant between-group difference in follow-up duration was observed, we did not explicitly adjust for time-at-risk or perform time-to-event analysis. Moreover, because patients were routinely instructed to wear a thoracolumbar brace for the first 3 months after surgery, clinical and radiological outcomes may not have fully manifested in those with a shorter follow-up. Therefore, the reported AVF incidence should be interpreted with caution, and future studies with longer and more uniform follow-up and time-to-event analyses are warranted. Third, BMD data were missing in 29.8% of the patients. Although multiple imputations were performed, some residual confounding factors cannot be excluded. In addition, although postoperative osteoporosis treatment data were added to the present analysis, detailed information regarding treatment timing, duration, and adherence was not fully incorporated, and confounding factors related to osteoporosis management may still have remained. Nevertheless, the association between ADVP and AVF remained consistent across propensity score–matched analyses and Firth logistic regression models. Whether ADVP size or extent contributes to AVF risk, and how ADVP relates to disc degeneration severity, such as Pfirrmann grade, remains unclear. Fifth, all radiological assessments, including ADVP, AVF, and angle measurements, were performed by a single observer, and inter-observer reliability was not evaluated. Finally, due to the cross-sectional study, it was not possible to determine whether ADVP developed as a consequence of fracture or reflected pre-existing degenerative or alignment-related changes. Longitudinal imaging studies are required to clarify the temporal sequence of ADVP development.
Conclusion
ADVP is associated with an increased risk of AVF after BKP. Incorporating the assessment of ADVP into preoperative CT evaluation may help identify patients at a higher risk of AVF and inform clinical decision-making and perioperative management. Prospective studies with larger cohorts and longer follow-up periods are warranted to validate these findings and clarify the contribution of ADVP-related disc and segmental changes to AVF development.
Supplemental Material
Supplemental Material - Association Between Adjacent Disc Vacuum Phenomenon and Adjacent Vertebral Fracture after Balloon Kyphoplasty for Osteoporotic Vertebral Fractures: A Retrospective Multicenter Study
Supplemental Material for Association Between Adjacent Disc Vacuum Phenomenon and Adjacent Vertebral Fracture after Balloon Kyphoplasty for Osteoporotic Vertebral Fractures: A Retrospective Multicenter Study by Kento Okamoto, Ryota Kimura, Michio Hongo, Yuji Kasukawa, Kazunobu Abe, Fumihito Kasama, Kyoko Nomura and Naohisa Miyakoshi in Global Spine Journal
Footnotes
Acknowledgments
We thank Teiichiro Yamazaki for his assistance with the statistical analyses.
Ethical Considerations
This study was approved by the Institutional Review Board of Akita University (approval number: 3052).
Consent to Participate
Informed consent was obtained from the patients for participation in this study using an opt-out approach in accordance with our institutional policies.
Author Contributions
Conceptualization, K.O., R.K., Y.K., M.H.; methodology, K.O. and R.K.; validation, K.O.; formal analysis, K.O., K.N.; investigation, K.O., K.A., F.K.; writing—original draft preparation, K.O.; writing—review and editing, K.O., and R.K.; visualization, K.O.; supervision, K.N., N.M.; project administration, R.K.; All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Additional Identifying Information
This study was conducted at 4 institutions: Akita University Hospital, Yuri Kumiai General Hospital, Akita Kousei Medical Center, and Omagari Kousei Medical Center.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.