
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The OF classification is a new classification for osteoporotic vertebral fractures. The aim of this study was to clarify the relationship between preoperative OF subgroups and the postoperative outcome after kyphoplasty in patients with such fractures.
Methods:
Patients who underwent kyphoplasty of a single osteoporotic vertebral fracture were included and divided into groups according to the OF subgroups. Pre- and postoperative plain radiographs were analyzed in regard to the restoration of vertebral body height and local kyphotic angle (LKA). Additionally, clinical data including pre- and postoperative Visual Analogue Scale pain scores was documented. The clinical and radiological results were compared pre- and postoperatively within groups and between groups.
Results:
A total of 156 patients from OF subgroups 2 to 4 were included (OF 2: n = 58; OF 3: n = 36; OF 4: n = 62). Patients from all groups experienced significant pain relief postoperatively (P < .001). Patients with OF 2 fractures showed a repositioning of the vertebral body height in the anterior and middle portions (both P < .001), but no significant improvement in LKA. For OF 3 and 4 fractures, there was a significant restoration of vertebral body height (P < .001 for both) and a significant improvement of LKA (P < .001 for both). The highest average restoration was noted in the OF 4 group.
Conclusions:
A higher OF subgroup is related to a higher radiological benefit from kyphoplasty. This confirms that the OF classification is an appropriate tool for the preoperative assessment of osteoporotic fractures.
Keywords
Introduction
With over 9 million cases every year worldwide, osteoporotic fractures constitute an important cause of morbidity in elderly patients.1-3 Due to the aging of populations, the number of such fractures is expected to rise even further in the coming decades, which makes their optimal treatment an important challenge in modern medicine. 4 One of the most frequent locations of osteoporotic fractures is the spine. 5 Such vertebral fractures can result in pronounced pain and even a persistent reduction of quality of life for affected patients. 6 Adverse effects on quality of life, physical function, mental health, and life-span have been reported to be related to the severity of the spinal deformity and are partly independent of pain.7-9 Therefore, efficient restoration of the fracture-related deformity seems to be fundamentally important for the achievement of optimal long-term outcomes and should be among the key factors to consider when making treatment decisions.
While conservative treatment of osteoporotic vertebral fractures may result in a good pain relief for many patients, surgical methods additionally allow for height reconstruction and stabilization of the affected vertebra. The most commonly used technique is cement augmentation using kyphoplasty, whereas unstable fractures require instrumentation. The individual treatment choice needs to take various factors into account, which comprise the configuration of the fracture. For this purpose, the German Society for Orthopaedics and Trauma has recently published a new classification of osteoporotic thoracolumbar spine fractures, the “OF classification”10,11 (Figure 1). However, the relation between OF classification and postoperative patient benefit still remains unclear and has not yet been examined.
Therefore, we conducted a retrospective cohort study to investigate the relationship between the OF classification and radiological as well as clinical outcomes after kyphoplasty by analyzing data from single-level kyphoplasties of the thoracolumbar spine.
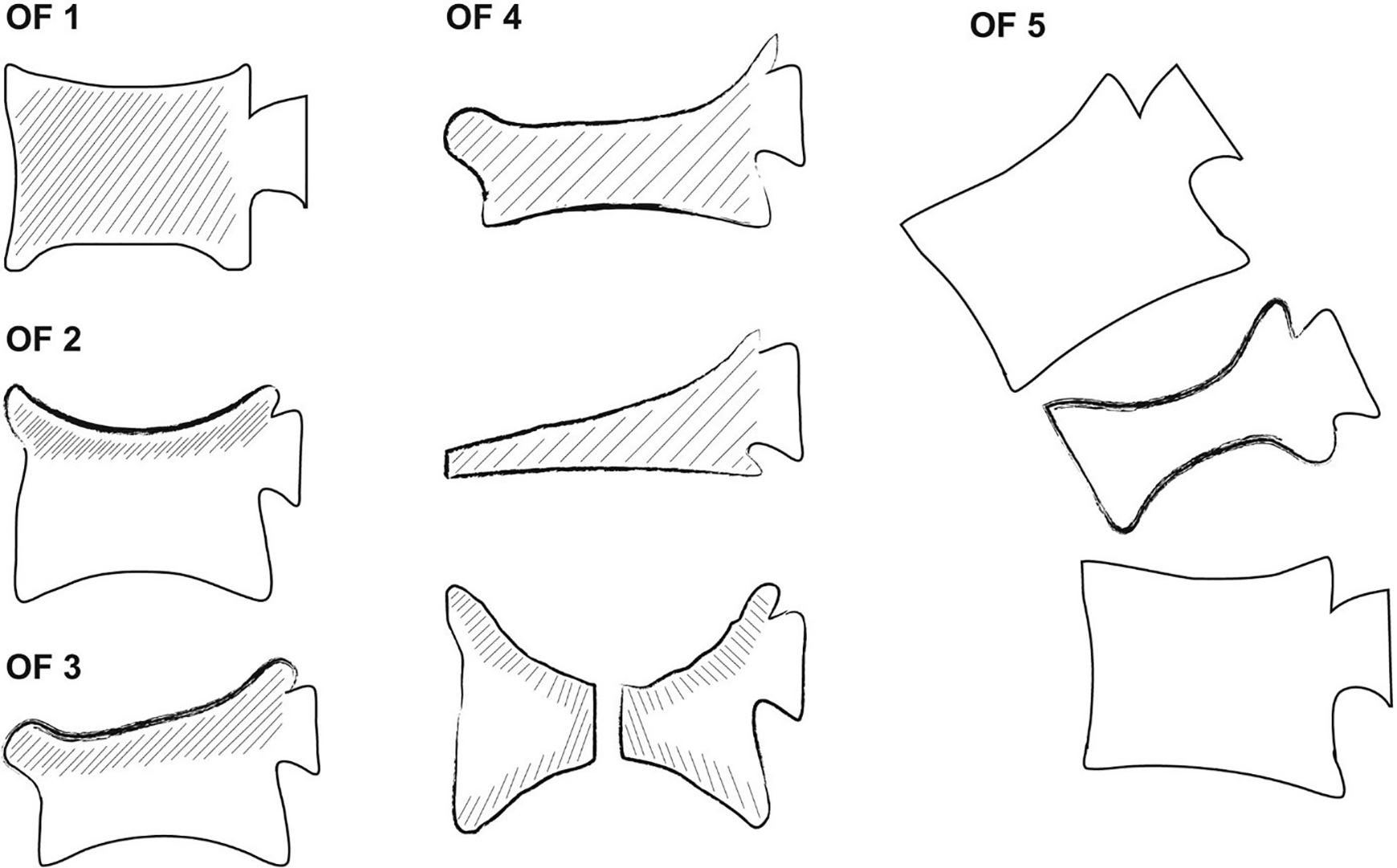
Classification of thoracolumbar vertebral fractures according to the OF classification. 10
Materials and Methods
Patients
Patients who underwent kyphoplasty of a single lumbar or thoracic vertebral fracture at our institution between January 2012 and December 2018 were eligible for this study. To limit the study to osteoporotic fractures, the main inclusion criterion was the presence of insufficiency fractures or fractures due to minor trauma (ie, atraumatic or falls from not more than normal standing height). All other fractures or neoplasia were excluded. As previous studies have shown significantly worse radiological outcomes for chronic fractures, patients without a distinct time point of symptom onset within not more than 6 weeks before the operation were excluded to avoid respective bias.9,12-15 OF 1 fractures were excluded because they have no deformation by definition, so no height restoration would be possible. 10 The included patients were divided into 3 groups according to the OF classification of the fractures.
Surgical Procedure
All patients were treated in the same standardized manner. The patients were placed in a prone position and received kyphoplasty using a bipedicular approach with biplanar C-arm imaging guidance under general anesthesia. The balloons were inserted and inflated up to a maximum pressure of 300 PSI until they made contact with either of the endplates or until complete restoration of the vertebral body height occurred. The polymethylmethacrylate cement was then allowed to cure until it reached a toothpaste-like viscosity and then used to fill the cavity. All patients stayed in a prone position for at least 15 minutes after cement administration to allow the cement to set.
Radiographic Parameters
Two independent raters not related to the surgeries (SB and ZH), who received special training regarding the measurement of radiological spinal parameters, independently evaluated the vertebral body height in the anterior, middle, and posterior portions as well as the local kyphotic angle (LKA) of the fractured vertebra on pre- and postoperative radiographs for all patients. In order to minimize the risk of systematic bias, we used the mean values from both measurements in statistical analyses. The height of the fractured vertebra was calculated as the relative height compared to the mean height of the nearest unfractured vertebrae proximally and distally to minimize the influence of varying magnifications. Subsequently, the difference between pre- and postoperative relative vertebral body height and between pre- and postoperative LKA were calculated to assess the repositioning that was achieved through kyphoplasty of the fractured vertebra. Example measurements are depicted in Figure 2.
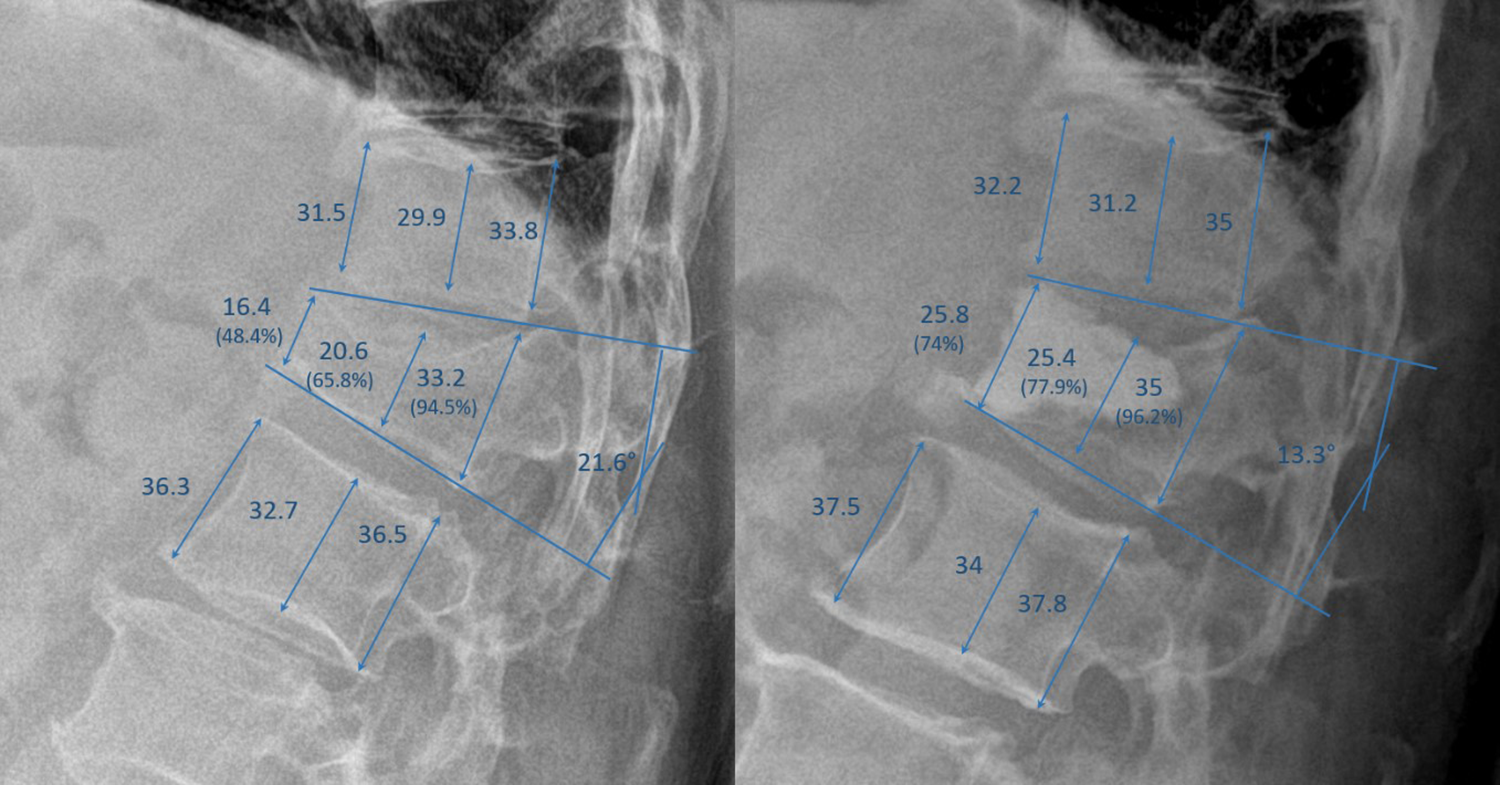
Measurement of radiographic parameters on pre- (left) and postoperative (right) radiographs from a 64-year-old patient with a fracture classified as OF 3. The restoration was 25.6% for the anterior portion, 4.8% for the middle portion, 1.8% for the posterior portion, and 11.7° for the local kyphotic angle.
Clinical Parameters
Clinical data on patient characteristics and the course of treatment was obtained from medical records. To guarantee complete datasets for all patients, clinical data was only analyzed until the day of discharge. These data included age, sex, interval between injury and surgery, osteoporosis medication, pain on a Visual Analogue Scale (VAS) at rest and in motion (1 day preoperatively and 2 days postoperatively), use of analgesics according to the World Health Organization (WHO) Analgesic Ladder (1, nonopioid analgesics; 2, nonopioids + weak opioids; 3, nonopioids + strong opioids; assessed 1 day preoperatively and 2 days postoperatively), body mass index (BMI), and first day of full postoperative mobilization. The mean volume of bone cement was 6.4 (±2) mL.
Statistical Analysis
Patient characteristics are presented as mean values with standard deviation or percentages, as appropriate. Baseline characteristics between the 3 different groups were compared using a one-way analysis of variance (ANOVA). Differences between pre- and postoperative parameters within the groups were compared using a paired t test for parametric variables or a Wilcoxon test for nonparametric variables. The radiological repositioning between the 3 groups was compared by one-way ANOVA with post hoc analysis according to Games-Howell.
Results
Study Population
We identified 492 patients who were treated by kyphoplasty at our institution between September 2012 and December 2018. A total of 156 patients were included for further analysis according to our predefined inclusion and exclusion criteria (Figure 3). Of these patients, 58 were classified as OF 2, 36 as OF 3, and 62 as OF 4. The identified patients with OF 4 fractures all had a loss of integrity of the vertebral frame structure, as patients from the other 2 OF subgroups (vertebral body collapse or pincer-type fractures) are regularly treated by spinal instrumentation at our institution. No patient with an OF 5 fracture was identified. In all patients the indication was persistent pain despite intensive conservative treatment. Baseline characteristics of the study population are presented in Table 1. Apart from the body height (P = .013), the baseline characteristics did not significantly differ between the 3 study groups. There were 67 patients who had thoracic fractures (Th5: 4, Th6: 5; Th7: 2; Th8: 8; Th9: 6; Th10: 4; Th11: 15; Th12: 23), and patients 89 had lumbar fractures (L1: 36; L2: 18; L3: 15; L4: 13; L5: 7). The average time of discharge was 4.9 (±6.1) days postoperatively.
Baseline Characteristics of the Study Population.
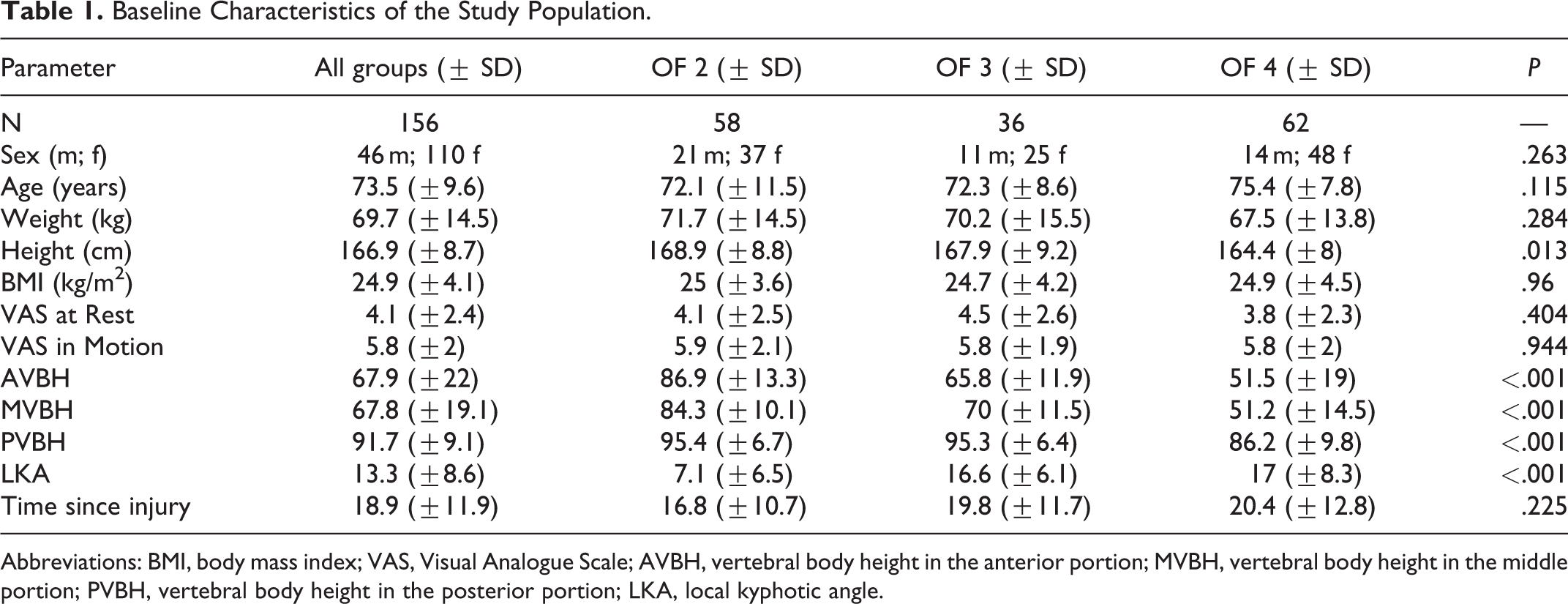
Abbreviations: BMI, body mass index; VAS, Visual Analogue Scale; AVBH, vertebral body height in the anterior portion; MVBH, vertebral body height in the middle portion; PVBH, vertebral body height in the posterior portion; LKA, local kyphotic angle.
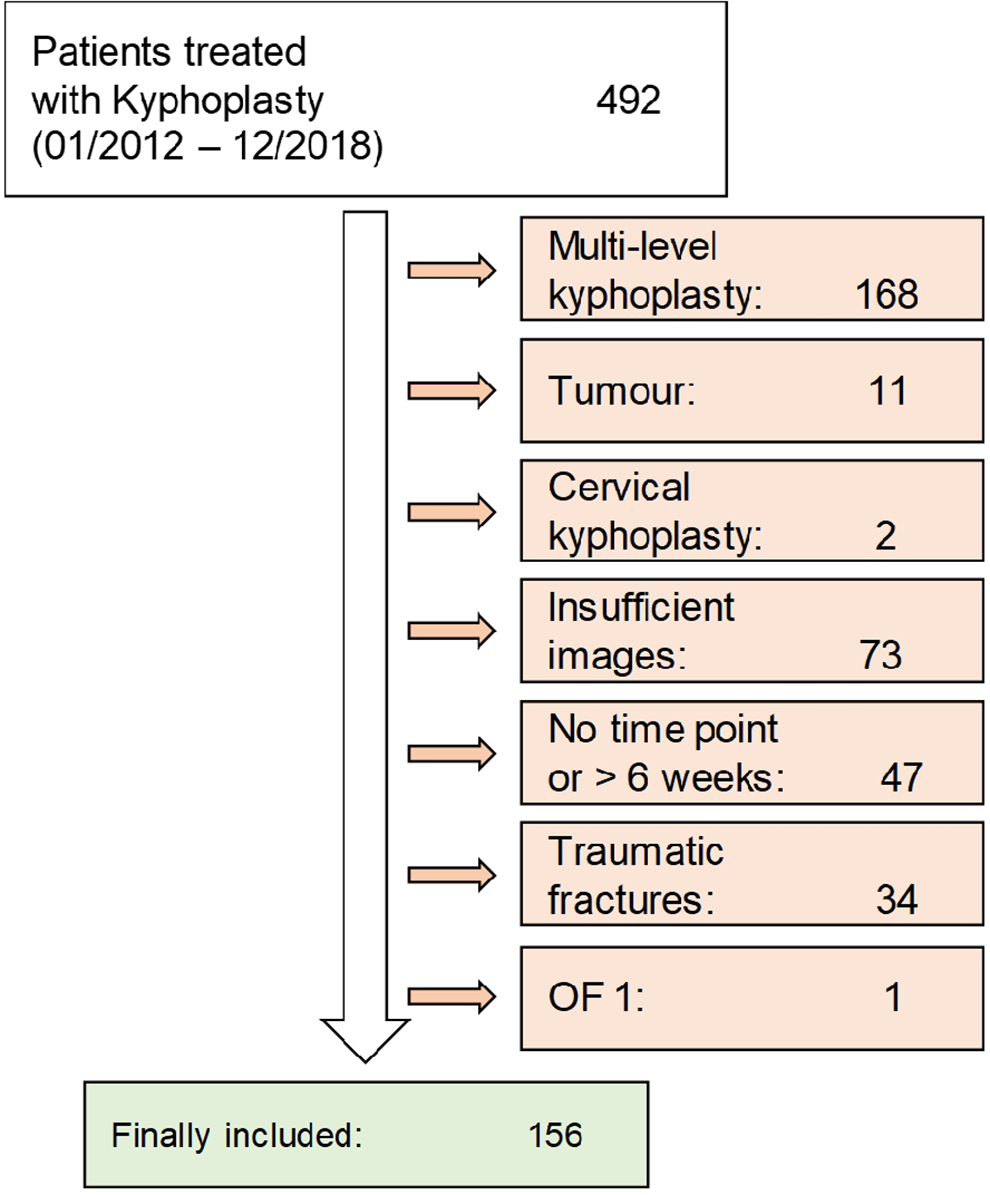
Study flowchart.
Radiological Outcome After Kyphoplasty
For the whole patient cohort as well as for patients classified as OF 4, there was a significant improvement in all measured radiological parameters—that is, anterior vertebral body height (AVBH), middle vertebral body height (MVBH), posterior vertebral body height (PVBH), and LKA—postoperatively (Table 2). In patients with OF 3 fractures, there was a significant correction of AVBH, MVBH, and LKA, whereas only AVBH and MVBH changed significantly in the OF 2 group. On average, the LKA could be corrected by 4°, ranging from 0.9° (OF 2) to 6.7° (OF 4) depending on the fracture classification. The posterior vertebral body height restoration was lower than the changes in other parameters in all groups, but still reached significance for the whole patient collective as well as the OF 4 group. In addition, 17/58 patients (29.3%) from the OF 2 group, 18/36 patients (50%) from the OF 3 group, and 46/62 patients (74.2%) from the OF 4 group had a restoration of ≥10% in relation to the height of the adjacent vertebrae in the anterior portion. An LKA correction of ≥5° was achieved in 10/58 (17.2%) patients with OF 2 fractures, 12/36 (33.3%) patients with OF 3 fractures, and 36/62 (58.1%) patients in the OF 4 group. Interrater reliability was generally high (intraclass correlation coefficient for preoperative measurements: AVBH 0.97; MVBH 0.96; PVBH 0.89; LKA 0.974; for postoperative measurements: AVBH 0.92; MVBH 0.88; PVBH 0.8; LKA 0.95).
Restoration of Vertebral Body Height and Local Kyphotic Angle.
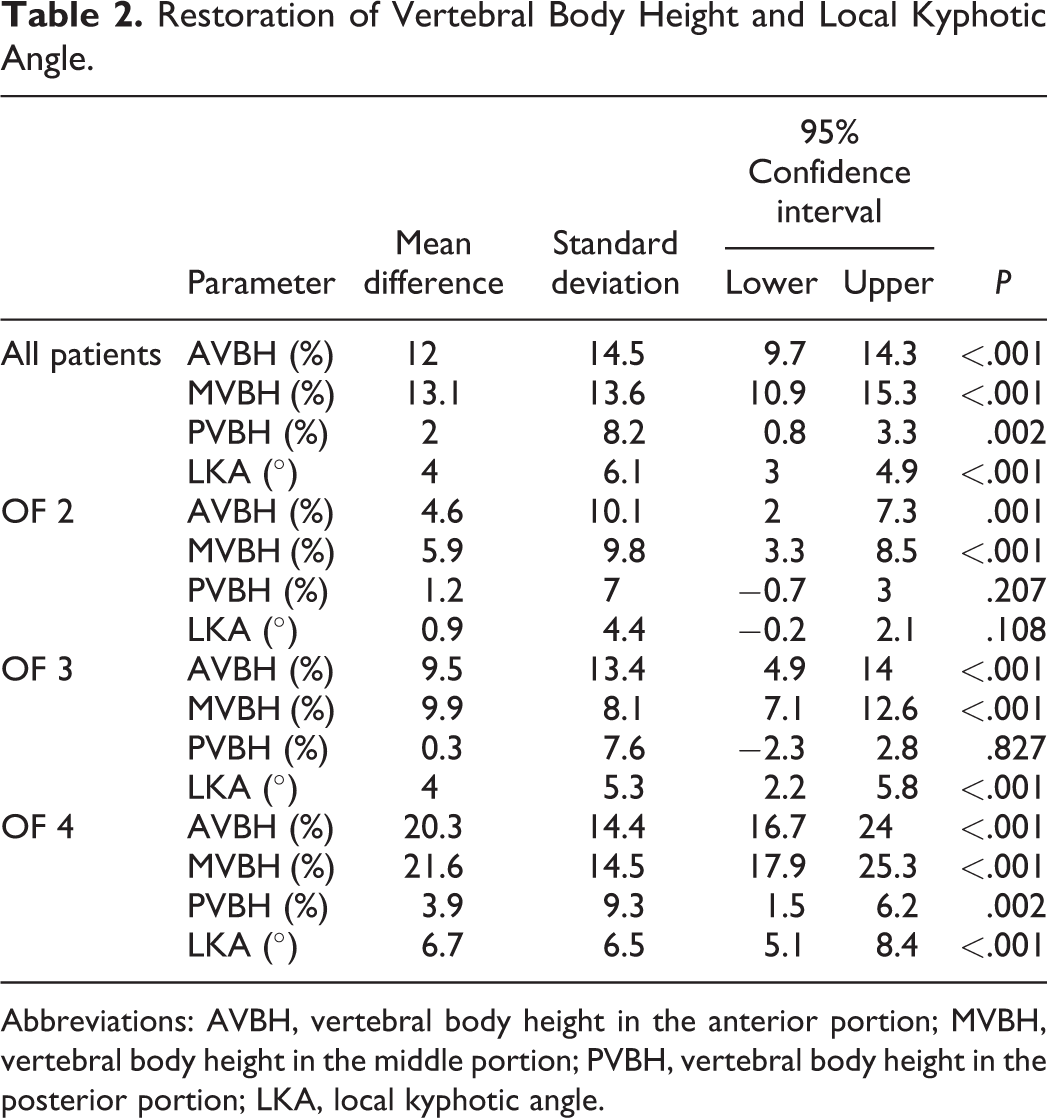
Abbreviations: AVBH, vertebral body height in the anterior portion; MVBH, vertebral body height in the middle portion; PVBH, vertebral body height in the posterior portion; LKA, local kyphotic angle.
Clinical Outcome After Kyphoplasty
Patients from all groups had significant pain reduction at rest (each P < .001) and in motion (each P < .001) 2 days postoperatively (Figure 4).
In the whole patient cohort and among patients with OF 4 fractures, the use of analgesics according to the WHO Pain Ladder was significantly reduced at both 2 days postoperatively (all patients: P = .012; OF 4: P < .046) and at the time of discharge (all patients: P < .001; OF 4: P = .004). In the OF 2 group, the use of pain analgesics was only significantly reduced at the time of discharge (P = .001), but not on the second postoperative day (P = .131). In contrast, the OF 3 group only showed a trend toward a lower use of analgesics without significant changes at either time point (2 days postoperatively: P = .357; discharge: P = .177).
A total of 150 out of 156 patients (96.2%) were fully mobilized (or reached their preoperative level of mobility in case of preexistent disability) within 1 day after surgery and 100% of patients were fully mobilized within 5 days. Twenty-three patients (14.7%) had cement leakage on postoperative radiographs (n = 6 for OF 2, n = 8 for OF 3, and n = 9 for OF 4 subgroup), but none of the affected patients required any further intervention. One patient (0.6%) was monitored in the intensive care unit postoperatively due to respiratory insufficiency (from OF 4 group), but recovered without any sequelae. None of the patients had spinal infections or fatal complications during the hospital stay. The risk for any of these complications was 15.3% for the whole cohort.
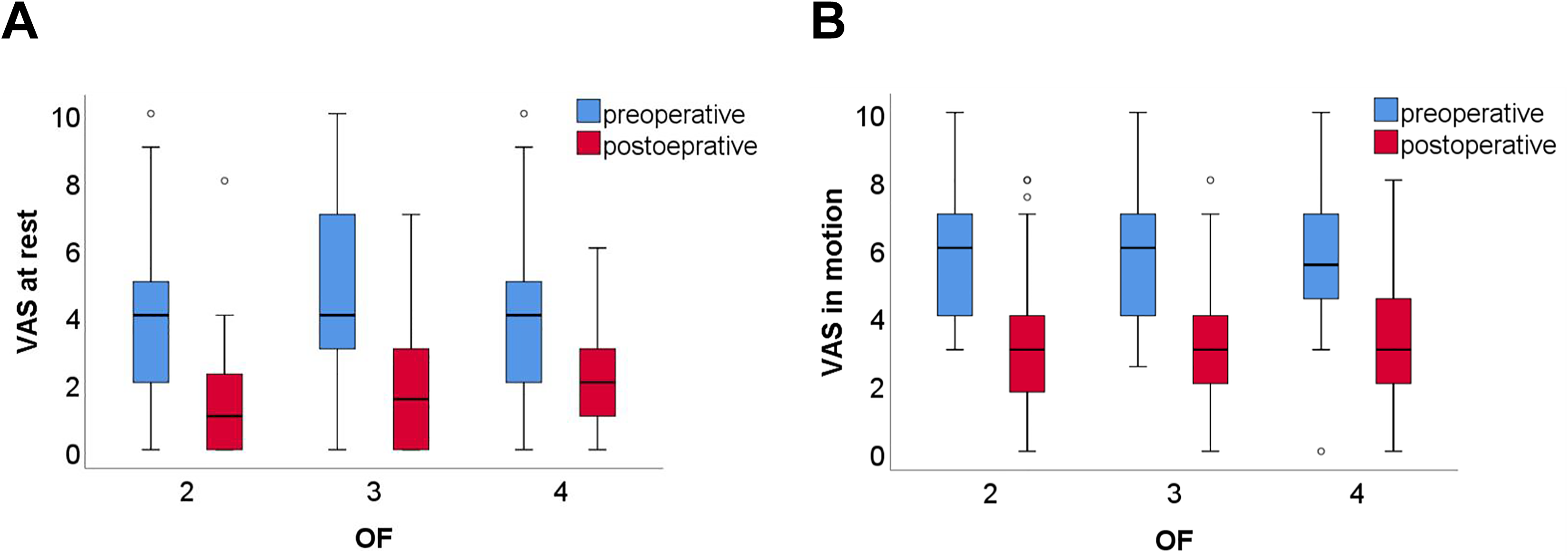
Pre- and postoperative VAS scores at rest (a) and in motion (b) depending on OF classification.
Influence of OF Classification on Height Restoration
One-way analysis of variance revealed significant differences among the 3 groups in regard to the restoration of vertebral body height in the anterior and middle portion as well as the correction of the local kyphotic angle (Table 3). Direct comparison using post hoc analysis showed a significantly higher restoration of AVBH, MVBH, and LKA for OF 4 compared to OF 2 fractures. When comparing OF 4 and OF 3 fractures, there was significantly better restoration of AVBH and MVBH as well as a trend toward a better restoration of PVBH and LKA for the OF 4 group. Between OF 2 and 3, the only significant difference was a better restoration of LKA for the OF 3 group, while AVBH and MVBH showed a trend toward a better restoration as well (Table 4). An overview of the postoperative restoration of LKA and vertebral body height in the different groups is depicted in Figure 5.
ANOVA Comparing the Restoration of Vertebral Body Height and Local Kyphotic Angle Between the Different Groups.
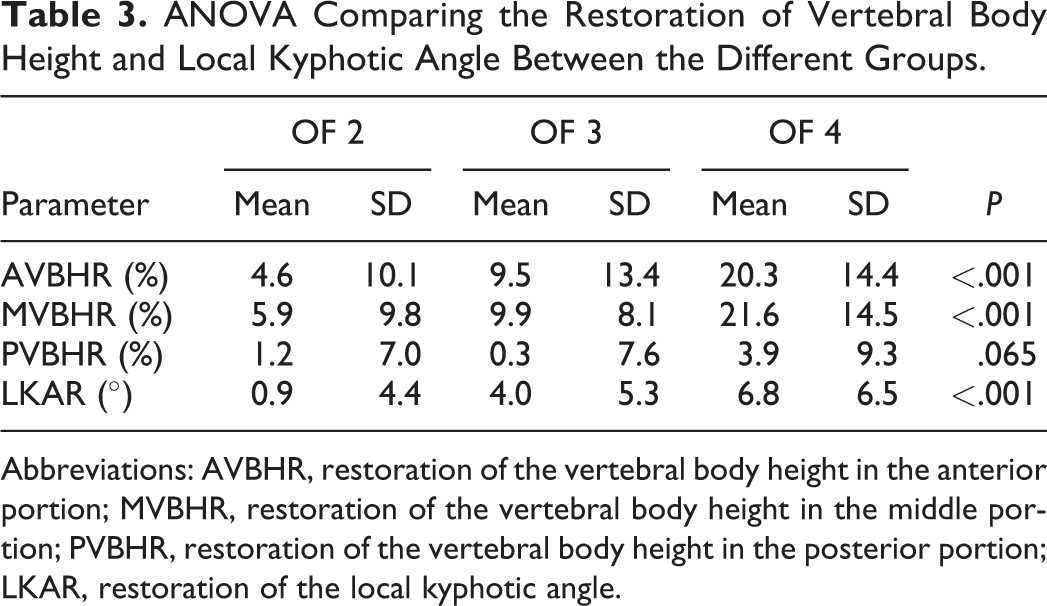
Abbreviations: AVBHR, restoration of the vertebral body height in the anterior portion; MVBHR, restoration of the vertebral body height in the middle portion; PVBHR, restoration of the vertebral body height in the posterior portion; LKAR, restoration of the local kyphotic angle.
Post Hoc Analysis Directly Comparing the Restoration of Vertebral Body Height and Local Kyphotic Angle Between Groups.
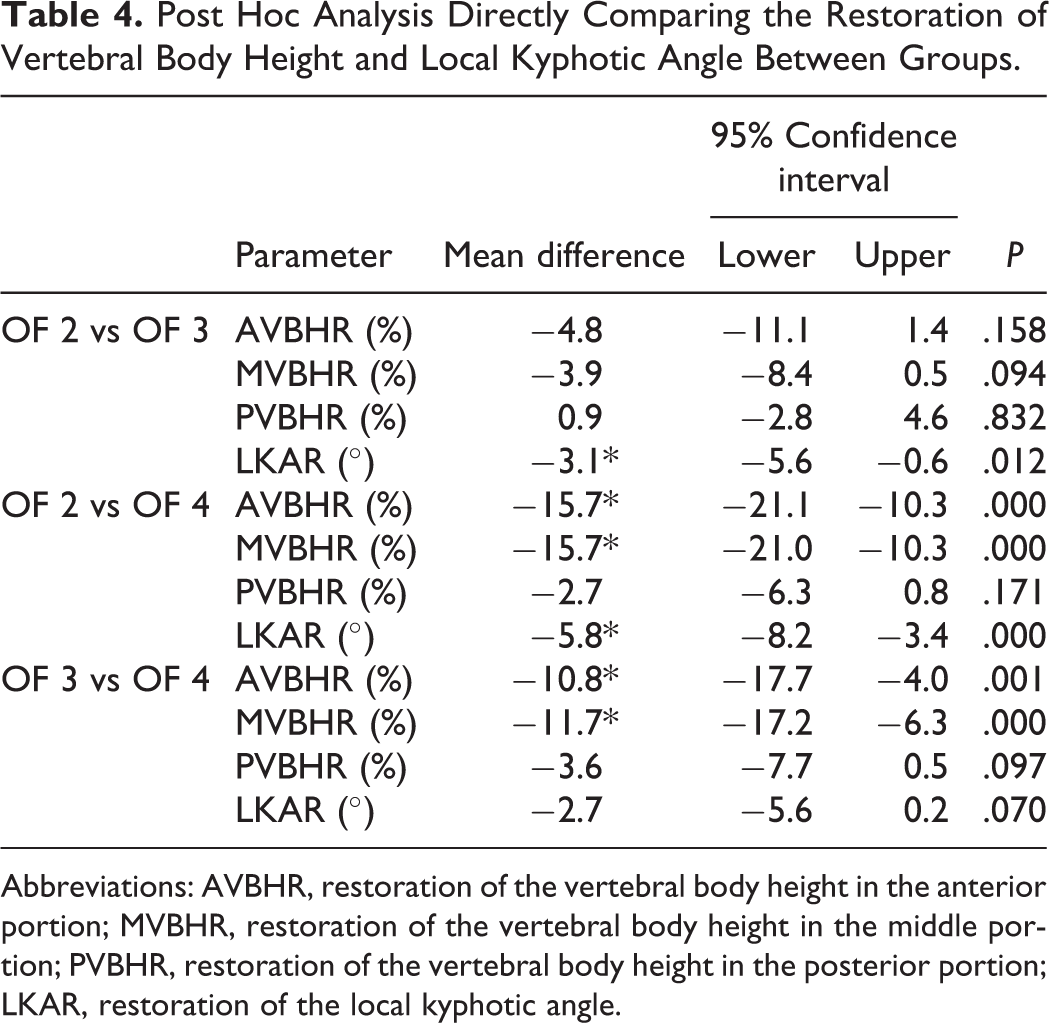
Abbreviations: AVBHR, restoration of the vertebral body height in the anterior portion; MVBHR, restoration of the vertebral body height in the middle portion; PVBHR, restoration of the vertebral body height in the posterior portion; LKAR, restoration of the local kyphotic angle.
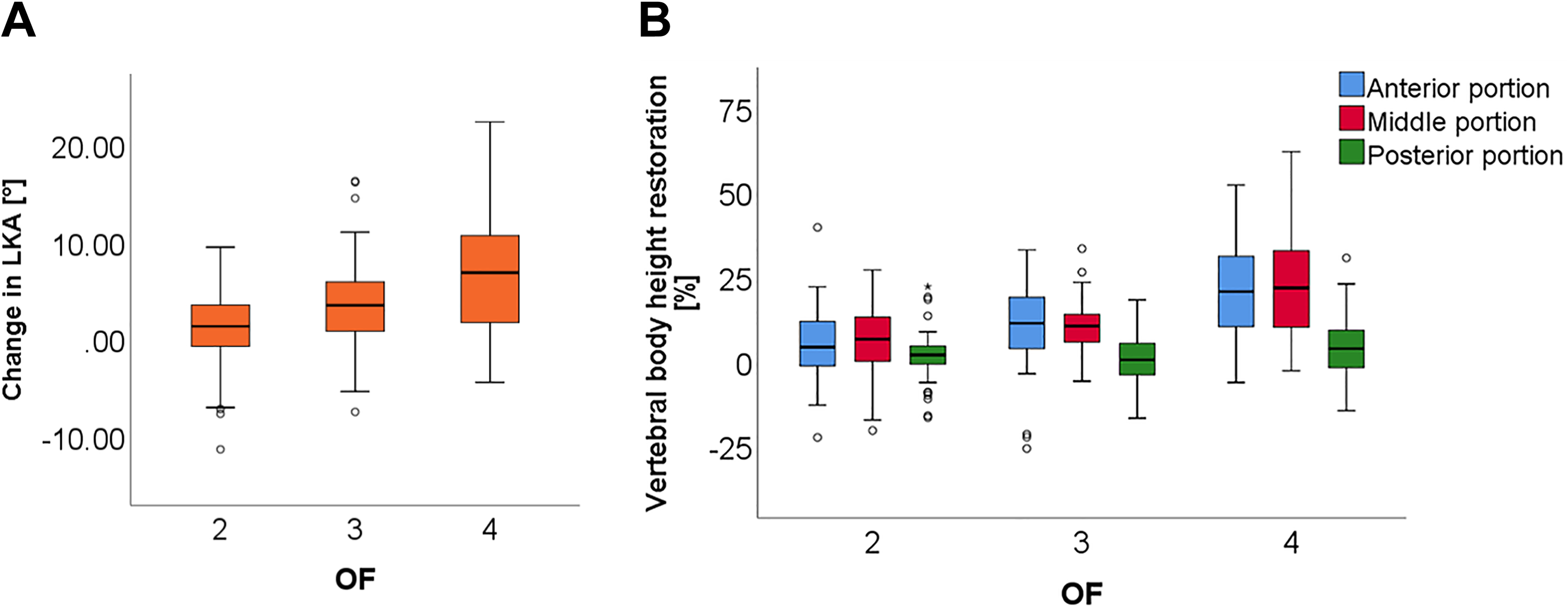
Postoperative changes in local kyphotic angle (a) and vertebral body height (b) depending on OF classification.
Discussion
The OF classification is a rather new classification that was first published nationally in 2017, followed by international publication 1 year later.10,11 In the respective publications, the authors state that “it remains unclear whether this classification will be of any prognostic value.” 10 To the best of our knowledge, the present study is the first investigation of the relation between preoperative OF subgroups and postoperative clinical and radiological patient outcomes. In general, we were able to demonstrate that a higher OF classification is related to a better restoration of vertebral body height and local kyphotic angle.
Overall, the available literature on kyphoplasty suggests good clinical outcomes and a low risk of complications. 16 This is confirmed by the results of our study. Patients from all groups reported a significant pain reduction already on the second postoperative day. Additionally, there was a general trend toward a lower use of analgesics in all groups, which reached significance at both investigated time points (second postoperative day and at discharge) for the whole collective and patients from the OF 4 group as well as on the day of discharge for the OF 2 group. The only group in which the differences were not significant was the OF 3 group. However, it should not be concluded that the OF 2 groups benefits less from kyphoplasty in regard to the consumption of analgesics. The OF 3 group included fewer patients than the other 2 groups (n = 36 vs n = 58 and n = 62, respectively), so these differences may be due to lower statistical power in this group. The finding that kyphoplasty reduces the consumption of painkillers is of particular interest for our population of osteoporotic patients, as these are mostly elder patients, in which polypharmacy is common. 17 Polypharmacy has been shown to be an important risk factor for morbidity and mortality, so that a reduction of analgesics may contribute to better long-term outcomes even irrespective of the direct effects on pain or the sagittal profile of the spine. 18
Regarding the effects of kyphoplasty on spinal alignment, our study showed a good reposition for OF 3 and OF 4 fractures. Good repositioning of the local deformation has been shown to be directly correlated to the correction of the global sagittal profile of the spine and is therefore fundamental for a positive clinical outcome. 19 In the OF 2 group, there was a small restoration of the vertebral body height in the anterior and middle portion, which was however much lower than for the other 2 groups and did not result in a relevant improvement of LKA. This is in line with the recommendation by the developers of the OF classification, who recommend a primarily conservative treatment in patients with OF 2 fractures.10,20 Still, also for these patients kyphoplasty should be considered as a treatment option in cases of persistent pain under conservative therapy, as recommended by current guidelines.21,22 However, the mean height restoration through kyphoplasty is rather low for OF 2 fractures with an LKA correction of only 0.9° and unlikely to have relevant clinical impact. Therefore, vertebroplasty may be considered as an alternative for these patients with respect to a cost-benefit rational. Patients with OF 4 fractures had significantly higher benefit than the other 2 groups in regard to radiological outcomes. This confirms the existing recommendations based on the OF classification, according to which a surgical treatment should be considered for these fractures. 20 The radiological outcomes of OF 3 fractures were between OF 2 and 4 fractures in our study and showed a significant restoration of both vertebral body height and local kyphotic angle, which was less pronounced than in the OF 4 group. Again, this is in line with the recommendations, which consider both surgical and conservative treatment options for this group. 20
However, it should be noted that kyphoplasty might not be the appropriate surgical treatment for all patients with OF 3 or OF 4 fractures. Although the selected patients from our cohort showed good results after kyphoplasty, some patients with OF 3 or OF 4 fractures might need instrumented stabilization, depending on the fracture stability and specific morphology. 20 This is particularly relevant for the OF 4 group, which comprises “loss of integrity of the vertebral frame structure,” “vertebral body collapse,” and “pincer-type fractures.” At the institution where the study was conducted, fractures with a loss of integrity of the vertebral frame structure are regularly treated using kyphoplasty and therefore appear in this study as the OF 4 subgroup. However, we believe that fractures with vertebral body collapse or pincer-type fractures are not suitable for kyphoplasty and should rather be treated using instrumented stabilization. As described in the methods section, patients with such fractures who received instrumented stabilization were excluded from this study and do not appear in the further analysis.
Despite our efforts for a rigorous methodology, the study has some limitations. It is based on a retrospective analysis without prospective randomization, which may introduce a selection bias. Still, the baseline characteristics suggest good comparability of the different groups. The only parameter that differed between the groups was the patient height. One possible explanation might be the higher loss of vertebral body height in the OF 3 and OF 4 groups, which results in a higher loss of body height. In our study, we aimed to investigate patients with osteoporotic fractures. For this purpose, we imposed strict criteria and only included patients with insufficiency fractures or minor trauma. However, it is possible that additional patients had an underlying osteoporosis despite adequate trauma. Although the OF classification also applies to those patients, they were not included in our study. Results of DXA (dual-energy x-ray absorptiometry) scans were not included in this study. We decided against including them because most DXA scans of our patients are performed in an ambulant setting after discharge and were therefore not available for this retrospective analysis. Instead, we limited our study to insufficiency fractures and fractures due to minor trauma, which have been shown to have a similar prognostic value for future fractures as low t scores.23-31 Besides, it should be kept in mind that DXA itself has significant weaknesses as a screening tool, as the results are strongly influenced by degenerative changes in facet joints or calcified aorta and therefore prone to underestimate the prevalence of osteoporosis. 32 Despite these known limitations, DXA remains the current standard for the diagnosis of osteoporosis and should be part of the routine osteoporotic workup for any patient with vertebral insufficiency fractures or fractures due to minor trauma. No OF 5 patients were identified for our study, so no conclusions in regard to this group can be drawn from our study. This was due to the fact that OF 5 fractures are classified as fractures with distraction or rotation and show substantial instability by definition. 10 Hence, these fractures always require an instrumented stabilization instead of kyphoplasty. Thus, the lack of OF 5 fractures in our cohort is actually an indicator of adequate surgical indications. Finally, our study only involved short-term follow-up until the day of discharge, which occurred at 4.9 days after surgery on average. Studies with longer follow-ups will be needed to determine whether the better local restoration also translates into a higher long-term benefit for patients with OF 3 and OF 4 fractures. Existing literature reports that the loss of quality of life, physical function, mental health, and life-span due to vertebral fractures is related to the severity of the spinal deformation and partly independent of pain.7-9 Therefore, it seems likely that our results are highly applicable for the estimation of long-term results.
In conclusion, we could demonstrate that patients in a higher preoperative OF subgroup show a higher postoperative benefit in regard to radiological parameters after kyphoplasty. These results confirm that the OF classification is an adequate tool for the classification of vertebral fractures and an important factor to consider when deciding on conservative versus surgical treatment. Patients with OF 2 fractures show a rather small radiological benefit, so an initial conservative treatment approach seems appropriate. Deformities caused by OF 3 and well selected OF 4 fractures can be relevantly restored by kyphoplasty, so surgical treatment should be considered for these patients.
Footnotes
Acknowledgments
Dr Palmowski is a participant in the BIH-Charité Junior Clinician Scientist Program funded by the Charité—Universitätsmedizin Berlin and the Berlin Institute of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the local institutional review board (EA1/203/18).