
Abstract
Study Design
Retrospective cohort study.
Objectives
The mechanism underlying the pain relief observed following balloon kyphoplasty (BKP) to vertebral compression fractures is reported to involve stabilization of the fractured vertebrae. However, whether fixation of the vertebrae was achieved immediately after BKP has not been investigated. The purpose of this study was to assess fixation of the vertebrae immediately after BKP and whether the instability was related to visual analog scale (VAS) scores.
Methods
Thirty-eight patients with vertebrae that were evaluated on lateral roentgenkymography within 1 week after BKP were recruited. Instability was defined as a cleft observed between the cement and end plate of the vertebra in the supine position that disappeared in the sitting position, and the posterior wall height of the vertebra was reduced in the sitting position.
Results
Instability of the vertebrae immediately after BKP was observed in 17 cases. VAS scores improved in all cases, and no significant differences were observed with or without instability.
Conclusions
The mechanism of rapid pain relief following BKP was not strong fixation but some degree of stabilization or other factors. We suggest that more research is needed about the mechanism of pain relief following BKP in the future.
Keywords
Introduction
The incidence of vertebral compression fractures (VCFs) has increased in association with the rising number of patients with osteoporosis. Osteoporotic VCF disrupts the quality of life of elderly people. Many previous studies have reported satisfactory results following balloon kyphoplasty (BKP) to VCF. 1 , 2 , 3 , 4 , 5 , 6 , 7 BKP has some advantages, such as restoration of the vertebral height via reduction of the fracture, decreased risk of complications, and rapid relief of pain. In many previous reports, clinical results, including alignment, pain, safety, efficacy, and complications, have been discussed. Generally, the mechanism underlying the pain relief observed following BKP is thought to involve fixation of the fractured vertebrae. However, to the best of our knowledge, fixation of the vertebrae immediately after BKP using roentgenkymography has not been previously investigated. The questions arose whether the fixation of the fractured vertebrae was really achieved immediately after BKP and whether fixation of the fractured vertebrae really improved pain.
The purpose of this study was to evaluate fixation of the vertebrae immediately after BKP and whether the remaining instability related to pain estimated by the visual analog scale (VAS). This is the first report to investigate fixation of the vertebrae using roentgenkymography at the immediate period following BKP.
Methods
Between April 2011 and January 2013, 46 BKP procedures were performed in 43 patients with unhealed VCF at Kyushu University Beppu Hospital and Karatsu Red Cross Hospital. BKP was performed in patients whose pain caused by VCF was not relieved after adequate conservative treatment, such as the administration of appropriate analgesic drugs, bracing, and bed rest. Painful level was decided from the clinical findings, X-ray films, and magnetic resonance imaging. Low back pain at the time of body motion and percussion pain of spinous process suspected VCF as the source of pain. After an examination, lateral X-ray films in both the sitting and supine positions were obtained (Fig. 1). Preoperative instability was defined as a change in vertebral shape on lateral X-ray films obtained in both the sitting and supine positions (Fig. 2). If a vertebra exhibited instability, the vertebra was diagnosed as the source of pain. All treated cases of VCF were attributed etiologically to osteoporosis, not myeloma or metastatic spinal tumors.
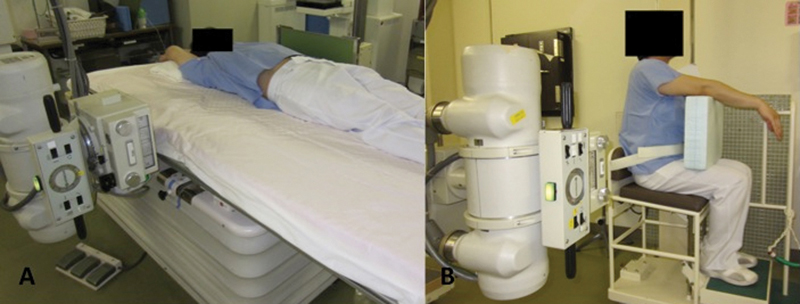
(A) Photograph showing how to perform a lateral X-ray in the supine position. (B) Photograph showing how to perform a lateral X-ray in the sitting position.
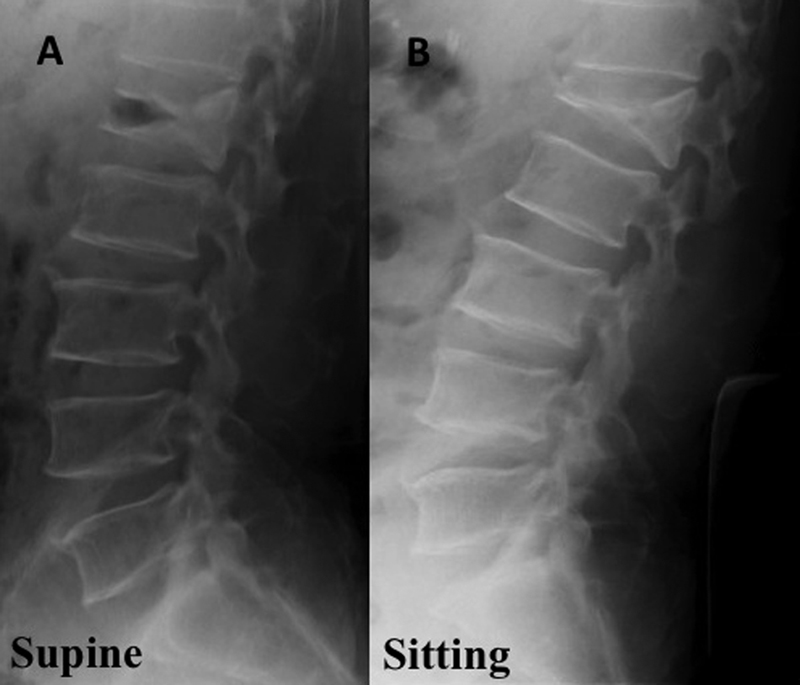
(A) Lateral X-ray taken in the supine position before balloon kyphoplasty (BKP). The intravertebral cleft can be observed. (B) Lateral X-ray taken in the sitting position before BKP. The intravertebral cleft has disappeared.
BKP was performed under general anesthesia for one vertebra in each surgery. Two bone tamps/balloons were inserted into the vertebral body under image guidance using a bilateral approach. The balloons were inflated to expand the vertebral body to create a cavity and reduce the fracture deformity. After completing these procedures, the balloons were deflated and removed, and the cavity was filled with cement with an appropriate level of viscosity until the cement touched the end plate under image guidance.
Thirty-eight of the 46 vertebrae that had been evaluated on lateral roentgenkymography within 1 week after BKP were assessed. We classified fracture type into wedge, crush, and biconcave. Wedge-type fracture occurred in 31 cases, crush-type fracture in one case, and biconcave-type fracture in six cases.
BKP was performed at T7–10 in three cases, T11–L2 in 32 cases, and L3–5 in three cases. The mean age at surgery was 81 years (56 to 97 years). The average duration from the onset of pain to surgery was 6 months (0.5 to 29 months). Postoperative instability was defined as the following two points using lateral X-ray films obtained in both the sitting and supine position. First, a cleft was observed between the cement and end plate of the vertebra in the supine position that disappeared in the sitting position. Second, the posterior wall height of the vertebra was reduced in the sitting position (Fig. 3). The degree of instability was estimated by three orthopedic surgeons using lateral roentgenkymography, and only a consensus of views was judged to be the final assessment. The degree of lordosis of the fractured vertebra was assessed according to the upper and lower end plate angles measured using lateral X-ray films obtained in the sitting position. The correction angle was calculated as the difference in the degree of pre- and postoperative lordosis.
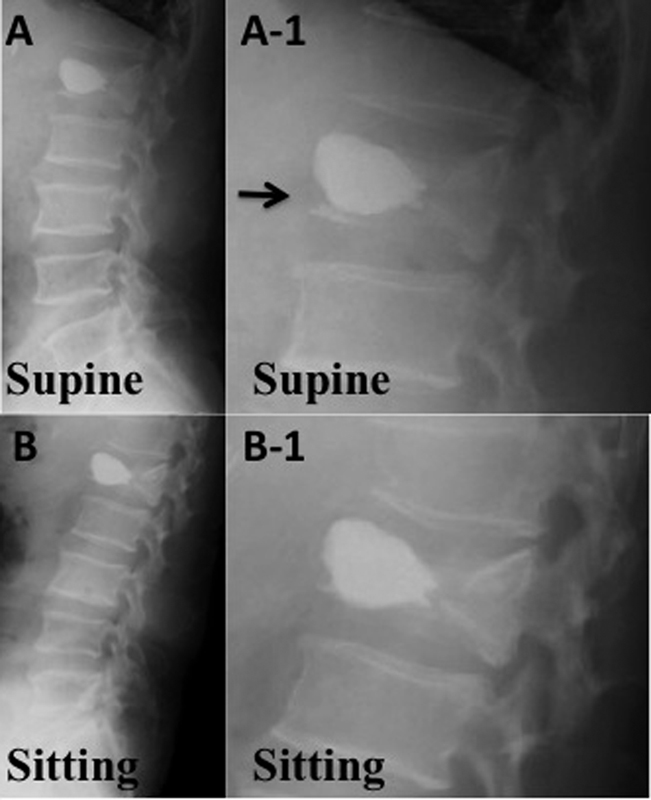
(A) Lateral X-ray taken in the supine position after balloon kyphoplasty (BKP). (A-1) Magnified X-ray that focuses on the treated vertebra. The black arrow indicates the presence of a cleft between the cement and the end plate. (B) Lateral X-ray taken in the sitting position after BKP. (B-1) Magnified X-ray that focuses on the treated vertebra. The cleft between the cement and end plate previously observed in the supine position has now disappeared.
The presence of backache before and after BKP was evaluated using VAS. Postoperative complications were also investigated. Differences in the mean VAS scores of the instability (IG) and stability (SG) groups were analyzed using the t test. Differences in the mean amount of cement and the correction angle between the IG and SG groups were also analyzed using the t test.
Results
Strong fixation immediately after BKP was not achieved in a total of 17 vertebrae. There was no difference in the incidence of instability by vertebral fracture type. The VAS scores improved in all cases, regardless of the presence of instability. No significant differences were observed in the preoperative VAS scores, postoperative VAS scores, or cement volume between the IG and SG groups (Table 1). There were no significant differences in the mean correction angle between the IG and SG groups.
Preoperative VAS Scores, Postoperative VAS Scores, and Cement Volume of the Instability and Stability Groups
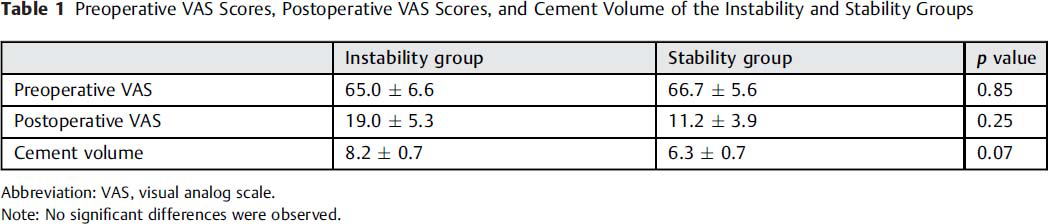
Abbreviation: VAS, visual analog scale.
Note: No significant differences were observed.
Regarding complications, 13 adjacent vertebral fractures occurred within 1 month, seven of which achieved bone union following conservative treatment, five remained under observation, and one was treated with BKP. One case of surgical site infection occurred and was successfully treated with antibiotics. No major perioperative complications were observed, such as compression of the spinal cord or pulmonary embolism caused by extravasation.
Discussion
Previous studies have reported that BKP is a good procedure for treating VCF due to its efficacy and safety. These reports primarily discussed the clinical results of BKP, including alignment, pain, safety, efficacy, and complications. In general, the mechanisms underlying the pain relief observed following BKP are thought to involve stabilization of the fractured vertebrae. Indeed, Wang et al reported that intravertebral instability at the cleft site disappeared following the injection of cement. 7 In that study, intravertebral instability was assessed using standing lateral radiographs only. At first glance, the clefts were filled with cement, and the instability appeared to have resolved. However, when assessing fixation, the use of images of lateral X-ray films obtained in both the sitting and supine positions is required. Indeed, in the present study, 17 vertebrae (45%) did not exhibit fixation on lateral roentgenkymography immediately after BKP. The number of cases of instability occurring immediately after BKP was larger than we had expected.
Why did a total of 17 vertebrae not achieve fixation? In general, it is thought that injection of an insufficient amount of cement causes persistent instability after BKP. However, in the present study, there were no significant differences in the cement volume between the IG and SG groups. Furthermore, contact between the polymethyl methacrylate and end plate was confirmed on X-ray images at the end of surgery in all cases. Even patients in whom adequate filling of the intervertebral clefts was confirmed during surgery demonstrated instability on lateral roentgenkymography immediately after BKP. BKP may not be able to achieve strong fixation immediately.
The effectiveness of BKP for treating osteoporotic VCF was demonstrated in the present as well as previous studies. The VAS scores improved immediately after BKP in all cases, and there were no significant differences in the scores between the IG and SG groups. Reduction of instability or fixation was achieved via cement injection. Toyone et al reported that changes in the vertebral wedging rate from a supine to a standing position are associated with back pain. 8 Even if fixation was not achieved following BKP, the reduction of instability alone may have improved the VAS scores. In the present study, the rate of improvement in the SG group was superior to that observed in the IG group. There were no significant differences due to the small number of cases, although significant differences may appear in the future. To obtain further information regarding the association between persistent instability and the VAS score, additional studies of large groups of patients over long follow-up periods should be performed.
Conclusions
BKP might not be able to gain strong fixation immediately. The mechanism of rapid pain relief following BKP was not achieved by strong fixation but by some degree of stabilization or other factors. We suggest that more research is needed to elucidate the mechanism of pain relief following BKP in the future.
Disclosures
None