
Abstract
Study design
Single-centre prospective study.
Objectives
Our study aims to investigate the relationship between preoperative and intraoperative factors with VBT surgical outcomes.
Methods
This is a single-centre prospective study involving consecutive VBT patients. All patients included were followed up for >2 years postoperatively. Primary outcomes were changes in radiographic parameters from pre-operative to immediate post-operative and between subsequent follow-ups
Results
Forty-one patients (35 females, 6 males) with 53 curves were included. Preoperative curve magnitude was 49.0 ± 7.4° and improved to 17.4 ± 8.0° immediately post-op (P < 0.001), with mean correction rate at 64.6 ± 15.4%. Coronal correction rate was persistently maintained at 62.1 ± 29.0% at 2-year. Preoperative flexibility correlated with correction rate at immediate post-operatively up to 18-month (correlation coefficient (r) = 0.768 to 0.933; P = 0.002 to P = 0.044). Strength of intraoperative tensioning at upper and apical curve segments was negatively associated with correction rate up till 9-month (r = −0.409 to −0.620) but could be explained by decision to tension more in less flexible curves. Preoperative fulcrum flexibility >79.8% (i.e. 80%) predicted postoperative clinical success (AUC 0.760; P < 0.001).
Conclusion
VBT improved curve magnitude and shoulder imbalance in scoliosis with progressive spinal growth. Flexible curves were associated with persistent coronal correction, while flexibility above 80% increases chance of clinical success with minimal risk of further progression. Growth modulation was associated with skeletal immaturity.
Keywords
Introduction
Vertebral body tethering (VBT) is an alternative to traditional spinal fusion in treatment for idiopathic scoliosis. 1 Current interest in VBT lies in its fusionless nature and ability to preserve motion and spinal growth.2,3 In VBT, a flexible tether is instrumented on the convex side of the curve. Compression effect by tensioning helps achieve immediate correction while VBT is expected to allow growth modulation by the Heuter-Volkmann principle. 1 Successful coronal correction and sagittal improvement were documented in recent studies,4-7 with favourable short-to-medium term results.
However, the behavior of the tether is unpredictable and there is uncertainty on whether growth modulation occurs.2,6,7 Further, surgeons have different techniques and preferences, such as tensioning methods and screw positioning.2,4 A recent peliminary study have reported preoperative fulcrum flexibility as a predictor for coronal correction, 8 but only its relationship with the first postoperative X-ray was assessed without investigating its role in subsequent correction and sagittal plane outcomes. While curve magnitude was also reported as a determinant for postoperative correction in the same study, other intraoperative factors like segmental tensioning or positioning of vertebral screws were not accounted for. There is currently no consensus on how surgeons should modify these factors to achieve the best surgical outcomes. Hence, it is of utmost importance to address this knowledge gap and increase likelihood of favorable surgical outcomes.
Our study aims to investigate radiographic changes in VBT in terms of coronal correction, sagittal changes, spinal growth as well as assessing for any presence of growth modulation (GM). Secondary aims include (1) assessing the relationship between preoperative and intraoperative factors with postoperative coronal correction. Factors of interest include fulcrum flexibility, intraoperative tensioning, screw positioning, screw length and skeletal maturity, (2) performing subgroup analysis for patients achieving clinical success as well as those with postoperative GM, (3) analyzing VBT-specific complications and their associated predictive factors and (4) postoperative functional level assessing for presence of back pain, return-to-sports and truncal imbalance.
Methods
Study Design
This is a single-centre prospective study involving consecutive VBT patients. All patients were followed up for >2-year postoperatively. Fulcrum-bending radiographs were routinely performed in our institution for assessment of preoperative curve flexibility with reference to method described by Cheung et al. 9 Skeletal maturity is defined as Sanders stage 7b, 10 distal radius and ulnar classification-radius (DRU-R) grade 10 or DRU-ulnar (DRU-U) grade 8, 11 or proximal femur maturity index (PFMI) grade 6 (or grade 5 with concomitant Risser stage 5).12,13 Assessment of skeletal maturity with PFMI was only used when hand-wrist radiographs were not available. Postoperatively, they were followed up at 3-6 monthly intervals depending on clinical needs. Radiographic data was obtained from postoperative X-rays, while intraoperative details were retrieved directly from operative records. Details on patient mobility, presence of back pain at latest follow-up, range of motion (ROM) were collected from physiotherapy and occupational therapy records to assess for postoperative functional level. Ethical approval from the local institutional review board (IRB; Ref 23-620) was obtained before study commencement. Individual informed consent was not required.
Surgical details
All surgeries were performed by two orthopaedic surgeons of the same institution, and were done either by thoracoscopic or mini-open approach. Implant systems used were REFLECTTM (Globus Medical, USA) and The TetherTM (Zimvie/Highridge Medical, USA). Length of screw used was determined intraoperatively according to surgical needs (5.0 to 6.5 mm). By dividing the vertebral body into 3 equal parts on lateral view, the positioning of vertebral screw was determined as located in the anterior one-third, posterior one-third or at the centre third of vertebra. After screw insertion, the flexible tether was anchored and sequentially tightened. One common tensioning technique is to maximally tension at every level, while other surgeons may prefer only tensioning maximally at apex region, or applying minimum tensioning throughout, depending on individual patients and curve characteristics. Strength of tensioning was measured in newtons (N). Immediate intraoperative correction of coronal curve was achieved through direct compression by screw-tensioning. 2
Study Outcomes
Primary outcomes were interval changes in radiographic parameters from pre-op to immediate post-op and subsequent follow-ups at 3-6 monthly. Parameters measured included coronal curve magnitude (Cobb angle), T1-T12 kyphosis for thoracic curves, 4 L1-L5 lordosis 14 for thoracolumbar/lumbar curves, shoulder height difference, pelvic obliquity and T1-S1 spinal height. Curve correction rate (%) and the fulcrum bending correction index (FBCI) were subsequently obtained. 15 Clinical success was defined as coronal curve magnitude <30° and the avoidance of revision surgery7,16, while GM was defined as further curve correction (>5 degree (°) improvement) compared to immediate post-op. Further correction of >5° was selected as cut-off for GM given the potential 5° measurement error 17 . Postoperative clinical success and GM were each assessed separately at postoperative 2-year. Shoulder height difference was obtained by first drawing vertical lines through the posterior axillary folds, then measuring the height difference between the intersection of horizontal lines on shoulders and the vertical lines. 18 Pelvic obliquity was measured with the Osebold technique by first drawing a straight line between bilateral superior aspects of iliac crests and another line parallel to lower end of radiograph, the angle between the intersection of the two lines was obtained. 19 Absolute values for shoulder height and pelvic obliquity were used to indicate severity of imbalance.
Secondary outcomes were relationships between preoperative and intraoperative factors with coronal correction rate. Preoperative factors included curve flexibility and skeletal maturity in terms of Sanders and DRU classification. Intraoperative factors were strength of tensioning at upper/apical/lower segments, tensioning technique (maximal tensioning or not), screw positioning, screw length and immediate coronal correction. Screw positioning was defined as screw location relative to centre of individual vertebra on lateral spine radiograph (anterior, middle and posterior 1/3 of vertebral body). Subgroup analysis of patients achieving postoperative clinical success and GM were performed. The incidences of VBT-specific complications, including tether breakage, overcorrection and revision procedures were recorded. Incidences of early perioperative complications were investigated in a recent study by our institution 20 and it would be interesting to report on mid-to-long term complications specific to the procedure. Lastly, functional level was assessed by functional status (return-to-sports), any presence of back pain at latest follow-up, aesthetic concerns (rib hump/loin hump) and any truncal imbalance.
Statistical Analysis
Patient demographics, preoperative characteristics and surgical details were presented. Data normality was tested. Comparisons between radiographic parameters at multiple time-points were done with the Friedman test, while the Mann-Whitney U test was utilised to compare between two groups of continuous variables. Subgroup analysis for thoracic and thoracolumbar/lumbar curves were carried out. For sagittal profiles, patients were further subdivided according to degree of kyphosis/lordosis. Normokyphosis was defined as T1-T12 kyphosis of 15° to 40°, and hyperkyphosis and hypokyphosis as >40° and <15° respectively. 21 Normolordosis was defined as having L1-L5 lordosis of 10° to 40°, and hyperlordosis as >40°. 22 Fulcrum flexibility (%) was assessed by: (Preoperative curve magnitude –preoperative fulcrum-bending curve magnitude)/(Preoperative curve magnitude) x 100%, while correction rate (%) was assessed by: (Preoperative curve magnitude – curve magnitude at follow-up)/(Preoperative curve magnitude) x 100%. FBCI (%) was assessed by: (correction rate/fulcrum flexibility) x 100%.
Correlations of parameters were tested at each individual time-point, at 3-6 month intervals, up till post-op 2-year. We recognize that both tethered curves in a double VBT may not be completely statistically independent and any clustering effect from patients with double VBTs were controlled by implementation of partial correlation analysis whenever feasible. In such circumstances where further controlling for single vs double VBTs is not feasible, conventional correlation tests like Pearson and Spearman correlation were utilized for analysis.
For significant factors associated with postoperative clinical success and GM (eg, curve flexibility), further receiver operating characteristic (ROC) analysis was performed. The area under the curve (AUC) was calculated and optimal cut-off values were determined with the highest sensitivity and specificity. Binary logistic regression with bootstrapping was done after controlling for single/double VBTs, in order to further investigate relationship between flexibility and clinical success, and between GM and flexibility respectively. Odds ratio (OR) and 95% confidence intervals (CI) were presented.
For complication anaylsis, any potential correlations between preoperative/intraoperative factors with tether breakage and overcorrection were tested. Tether survival was assessed by Kaplan-Meier survival analysis. Despite the number of relationships assessed, the authors decided to report unadjusted P-values to avoid missing potential significant relationships, owning to the exploratory nature of our study. 23 Statistical significance was set at P < 0.05. All statistics were generated with SPSS statistics (v29.0; IBM, USA).
Results
Patient Characteristics
Patient Demographics and Operation Details
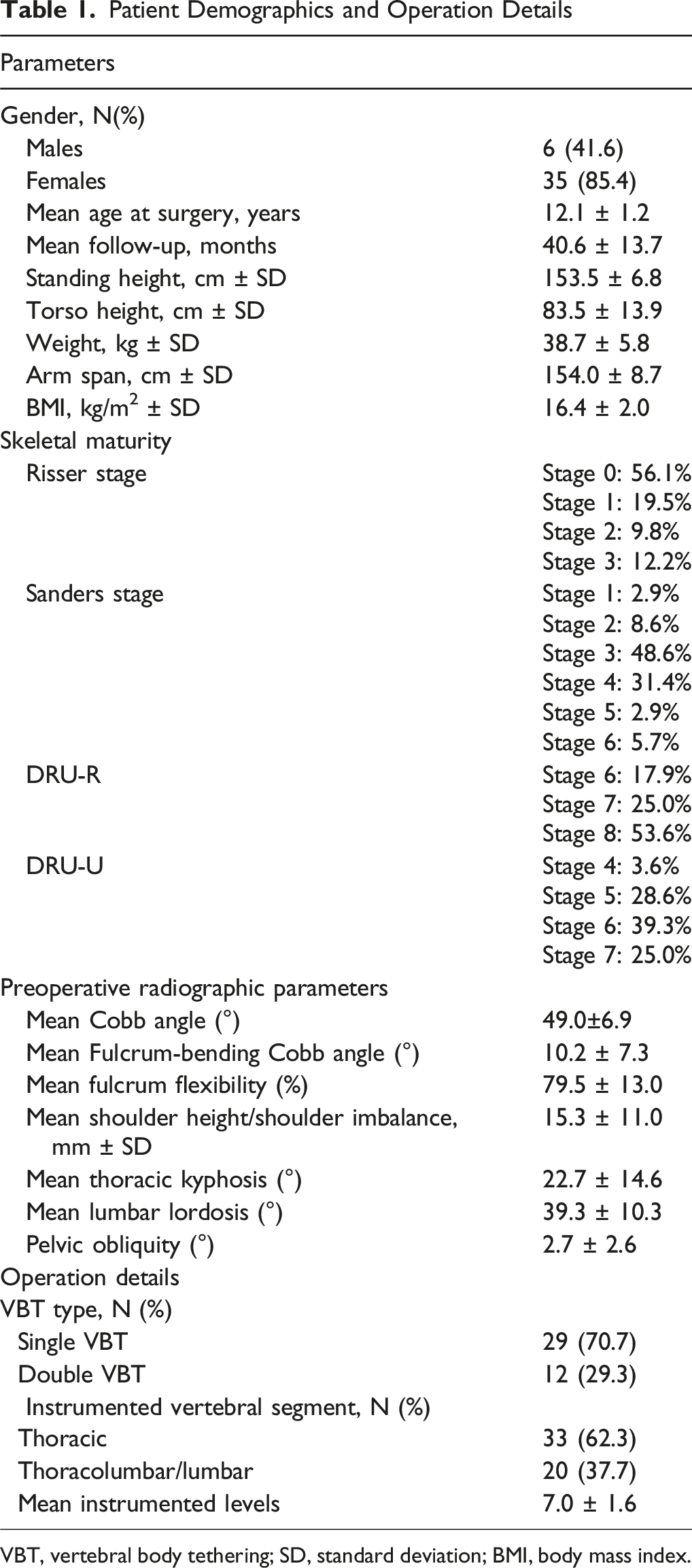
VBT, vertebral body tethering; SD, standard deviation; BMI, body mass index.
Trends of radiographic Parameters
Changes in Radiological Parameters Across Follow-Ups
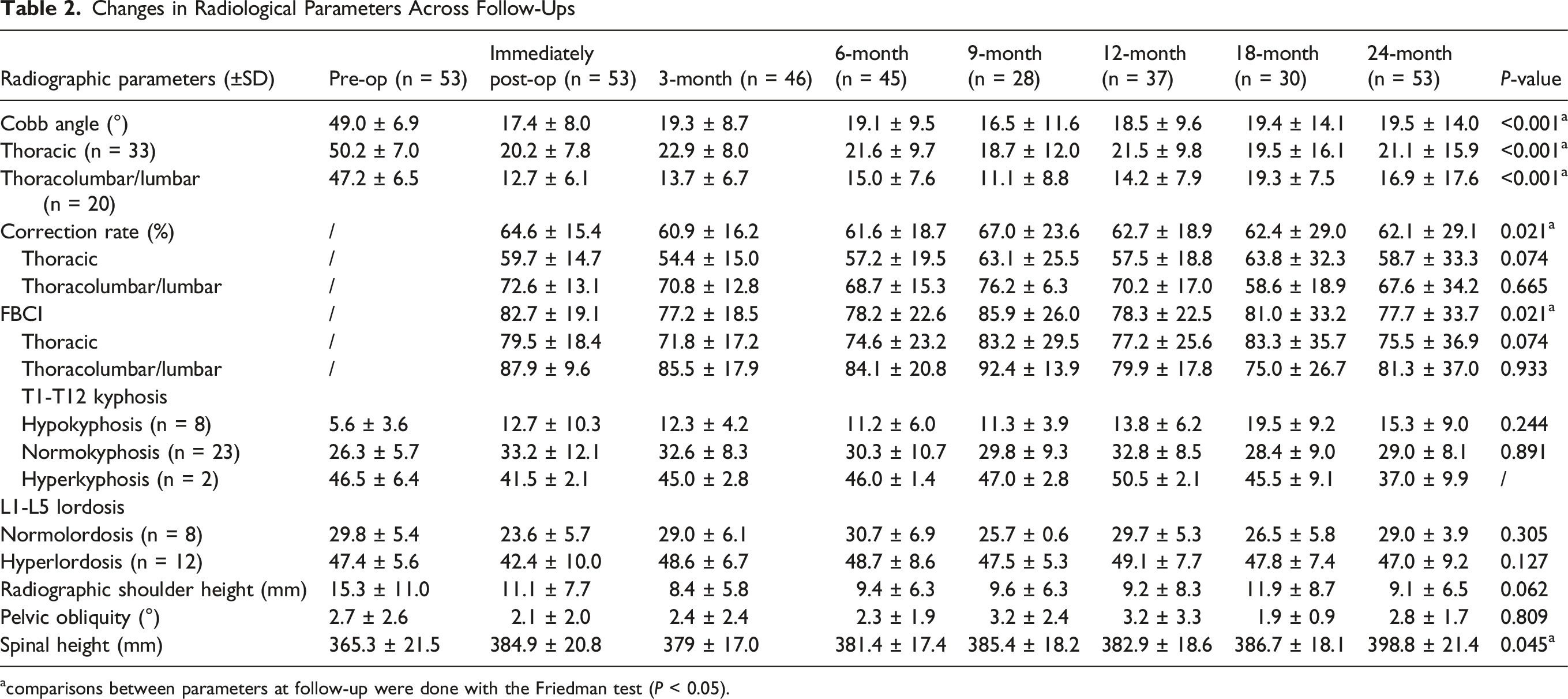
acomparisons between parameters at follow-up were done with the Friedman test (P < 0.05).
Relationship Between Factors and Coronal Correction
Relationship Between Preoperative Factors With Coronal Correction Rate
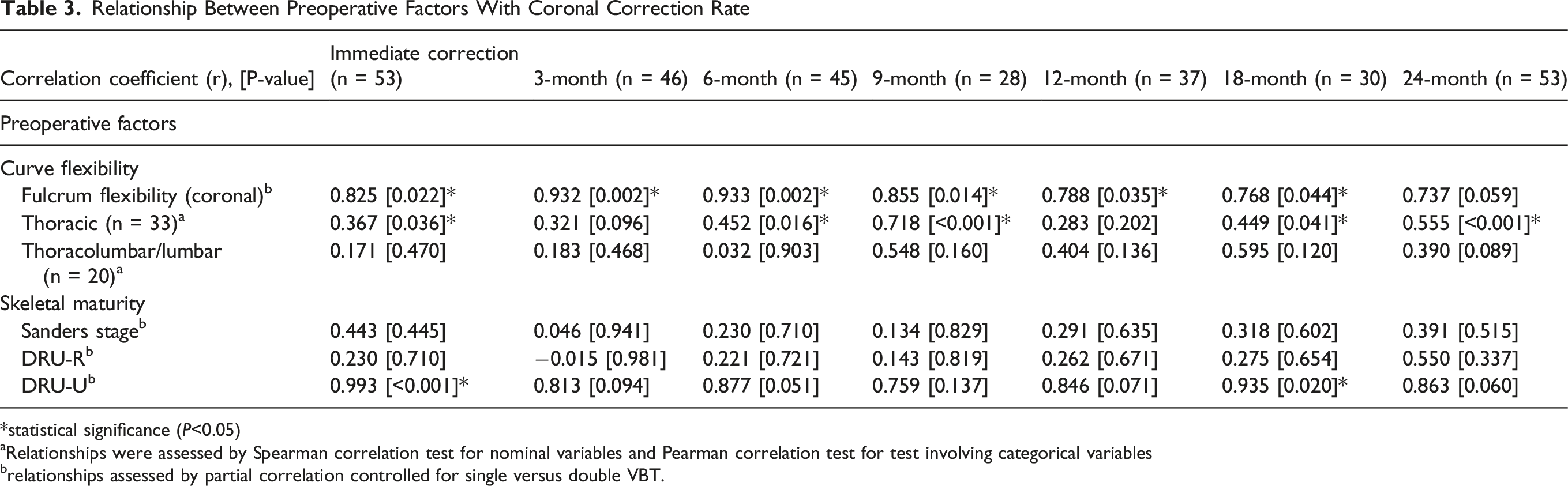
*statistical significance (P<0.05)
aRelationships were assessed by Spearman correlation test for nominal variables and Pearman correlation test for test involving categorical variables
brelationships assessed by partial correlation controlled for single versus double VBT.
Relationship Between Intraoperative Factors With Coronal Correction Rate
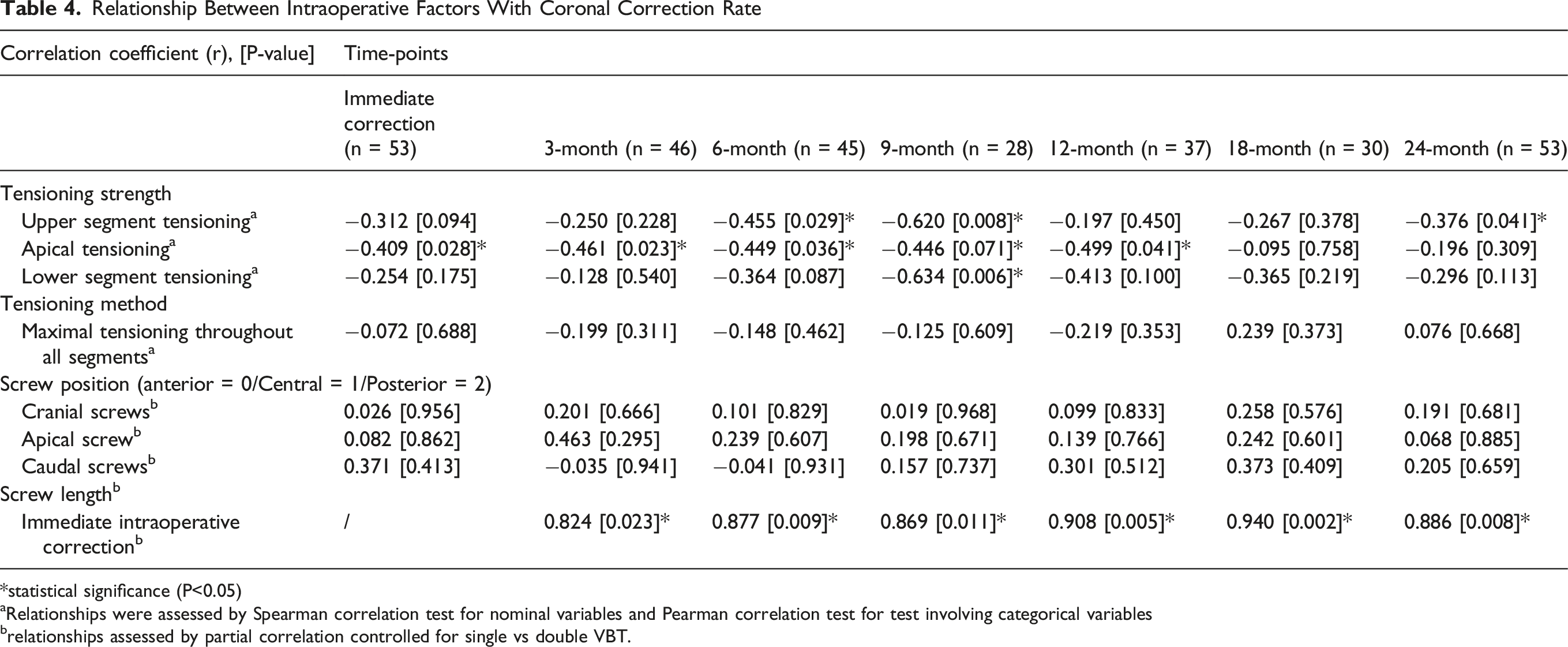
*statistical significance (P<0.05)
aRelationships were assessed by Spearman correlation test for nominal variables and Pearman correlation test for test involving categorical variables
brelationships assessed by partial correlation controlled for single vs double VBT.
Subgroup Analysis
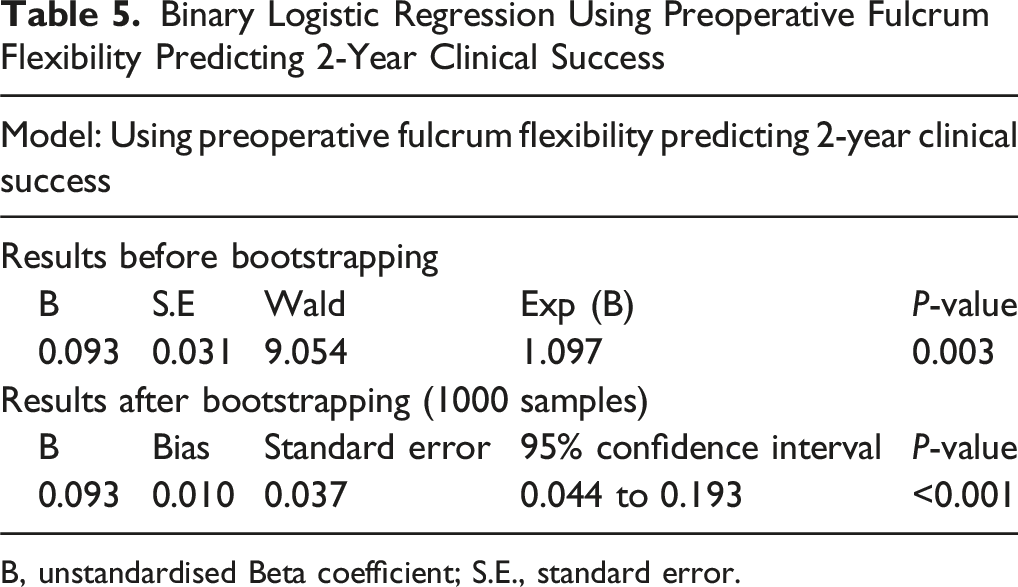
Clinical success: Thirty-five curves (66.0%) had magnitude <30° and did not require revision surgery at 2-year postoperatively (clinical success). Patients achieving clinical success had higher preoperative fulcrum flexibility compared to those without (71.0% vs 83.9%; P < 0.001). Presence of clinical success was associated with higher pre-op flexibility (r = 0.494; P < 0.001). With ROC analysis (Figure 1), utilising pre-op flexibility to predict presence of clinical success with area-under-curve (AUC) of 0.760 (P < 0.001), yielding optimal cut-off of 79.8% (sensitivity 0.78, specificity 0.69). Binary logistic regression showed that higher preoperative fulcrum flexibility predicted postoperative clinical success (OR 1.097; 95% CI 1.045 to 1.213; P = 0.003) with significance level P < 0.001 after further bootstrapping (1000 samples). (Table 5). ROC curve of preoperative fulcrum flexibility predicting postoperative clinical success at 2-year Binary Logistic Regression Using Preoperative Fulcrum Flexibility Predicting 2-Year Clinical Success B, unstandardised Beta coefficient; S.E., standard error.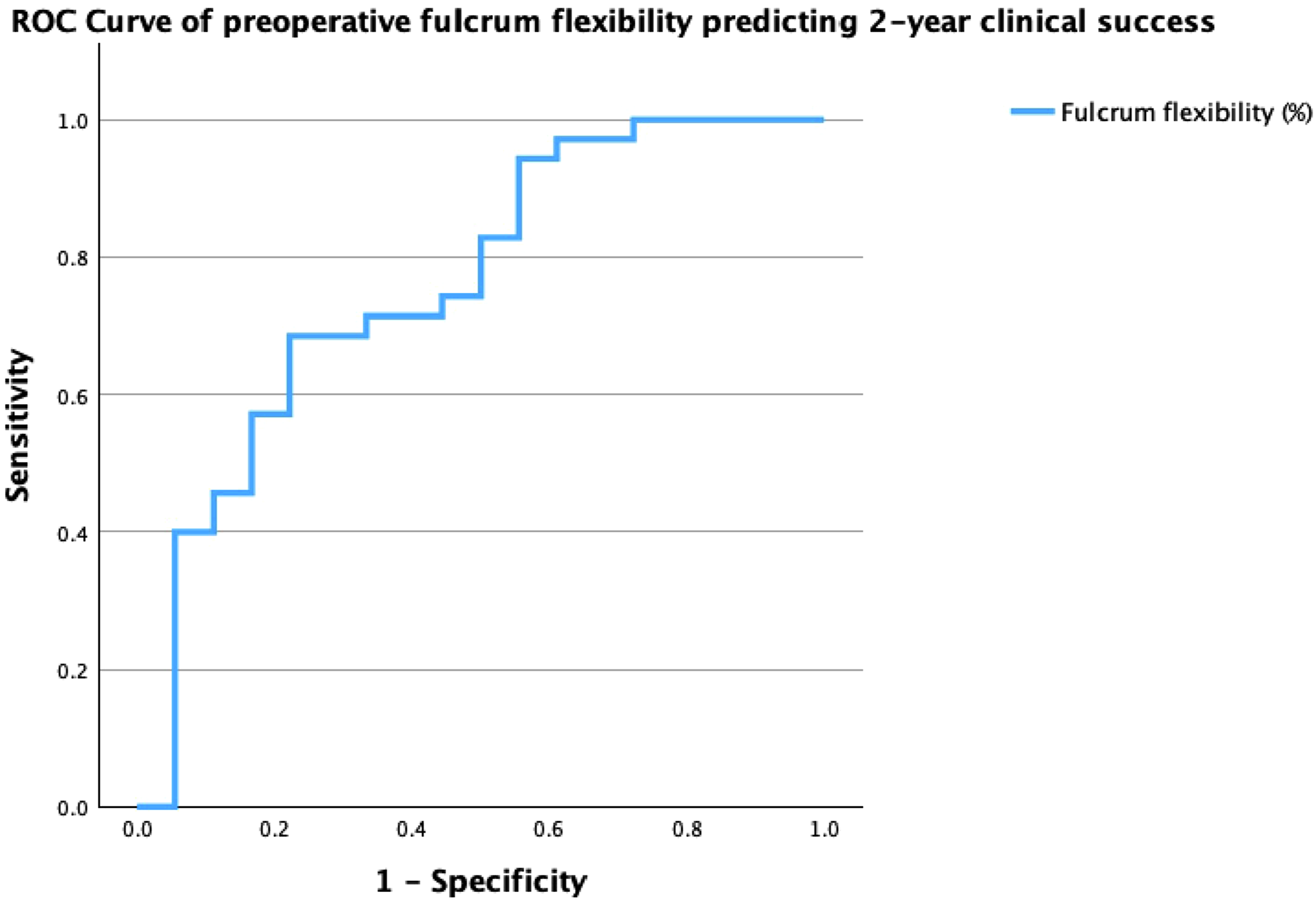
Growth modulation: Twelve curves (22.6%) exhibited GM, with 4 curves showing progressive curve improvement at subsequent follow-ups. Other curves generally exhibited pattern of initial curve progression over initial 3-6 months followed by progressive curve improvement. Higher fulcrum flexibility trended towards GM but not statistically significant (r = 0.270, P = 0.076). GM was associated with preoperative Risser stage ≤2 (r = 0.301; P = 0.047), and was also associated with postoperative clinical success (r = 0.343; P = 0.023).
VBT-specific Complications
Overall incidence for tether breakage was 32.1% (17/53; 9 thoracic and 8 thoracolumbar/lumbar curves). By Kaplan-Meier analysis, breakage-free survival at 12-month, 24-month and 36-month were 98.1% (95% confidence interval (CI) 94.4 to 100.0%), 84.5% (95% CI 74.7 to 94.3%) and 57.3% (95% CI 40.7 to 73.9%) respectively (Figure 2A). Thoracolumbar/lumbar curves were at greater risk of tether breakage (2-year survival 78.5% vs 87.9%; log-rank test P = 0.020) with hazard ratio of 2.69 (95% CI 1.00 to 7.22) (Figure 2B). Regarding curves with tether breakage (n = 17), there was a slight but statistically insignificant curve progression of 3.7 ± 3.4° (P = 0.197) and 6.8 ± 1.5° (P = 0.104) at 6-month and 12-month post-breakage respectively. Most tether breakages (11/17; 64.7%) occurred caudal to the curve apex (lower segments). 6 breakages (35.3%) occurred at the curve apex, while one lumbar curve had breakages both cranial and caudal to curve apex (both upper and lower segments). We did not find any significant correlations between fulcrum flexibility with incidence of tether breakage. 2A, Graph showing tether breakage-free survival in VBT curves; 2B, Graph showing tether breakage-free survival of thoracic vs thoracolumbar/lumbar curves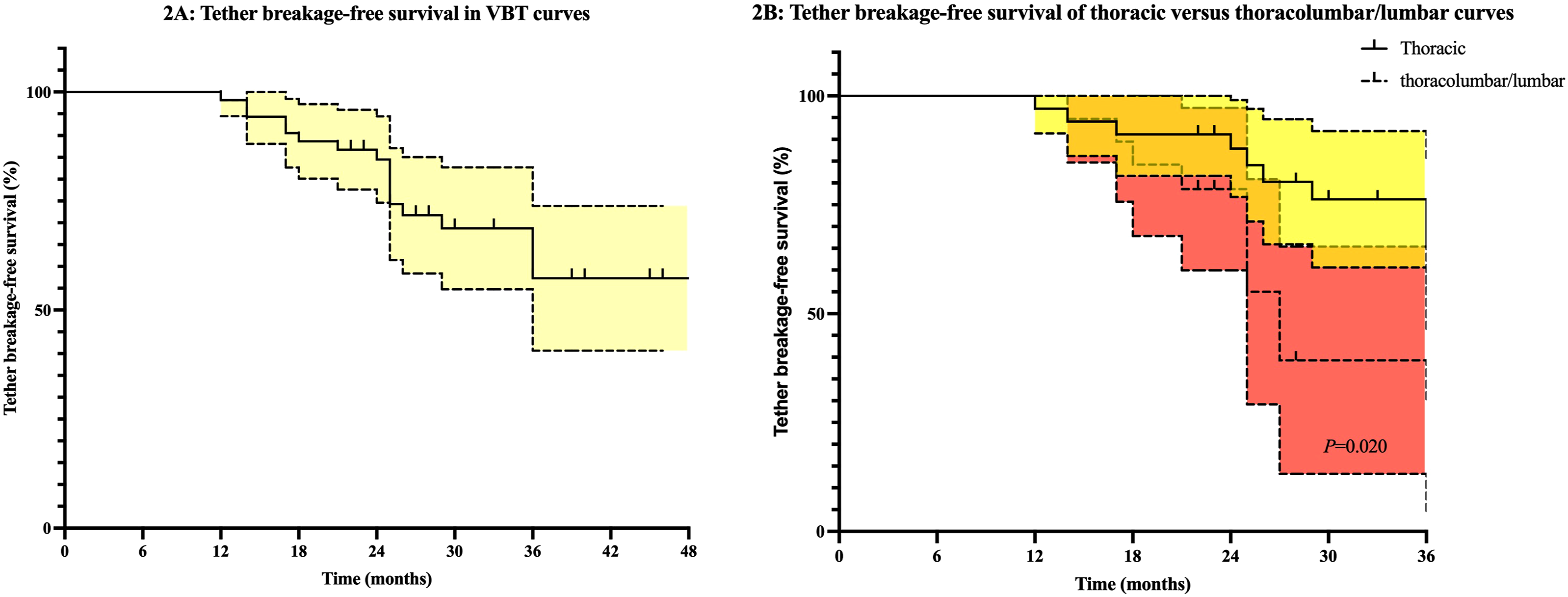
Six patients (14.6%) required revision surgery at mean 29.2 ± 12.2 months (range: 24 to 54). Amongst them, two required conversion PSF due to primary thoracic curve deterioration and one other had PSF for T10-L3 deterioration. Another patient had upper untethered thoracic (T2-5) deterioration, ultimately requiring T2-L3 PSF. A total of 4 instrumented curves in 3 patients had overcorrection (excessive growth modulation from −3.4 to −36.8°), with 2 patients ultimately requiring removal of implants after 2-year.
Postoperative Functional Level
Only 2 patients complaining of mild back pain at final follow-up, with others all asymptomatic. Twenty-six patients (63.4%) had retrievable physiotherapy/occupational therapy assessments. Five patients were frequent sports players, with one returning to competitive sports (rugby). Ten patients has mild residual thoracic humps while only two had mild loin humps. Six patients had mild truncal shifts. None had problems with walking, balancing and ADL.
Discussion
Our study demonstrated that VBT improved curve magnitude and shoulder imbalance in scoliosis, while simultaneously allowing for progressive spinal growth. Flexible curves were associated with persistent coronal correction, while flexibility above 79.8% (i.e. 80%) increases chance of subsequent clinical success. GM occurred in 22% of patients and was associated with skeletal immaturity. Less flexible curves warranted more intraoperative tensioning but did not directly contribute to postoperative correction.
Majority of curve correction was achieved intraoperatively in VBT,5,6,24,25 while a proportion of patients achieved further curve correction post-index operation (growth modulation). It was reported by Catanzano et al that progressive thoracic curve improvement occurred in half of the patients. 26 Most flexibility of the curve was taken up during intraoperative correction, as reflected from the immediately post-op FBCI (>80%).8,9,15 Thoracic kyphosis was mildly increased in hypokyphotic patients. This echoed with findings from Baroncini et al, which also reported restoration of normokyphosis in preoperative hypohyphotic patients. 4 Direct compression by instrumentation on anterior column might explain this kyphotic effect. The most significant advantage of VBT undoubtedly relied on its ability to preserve growth and range-of-motion. Progressive increase in spinal height was demonstrated throughout and previous literature also reported spinal growth was allowed to occur at an expected rate with VBT. 27 Overall imbalance was improved with significant decrease in postoperative shoulder height difference, and was reported to be comparable to PSF. 28 Previous studies documented a 30% decrease in shoulder height, implying the potential of spontaneous proximal thoracic curve correction after VBT. 29 Pelvic obliquity was more or less unchanged throughout our study, it should be noted most pelvic obliquity in a healthy AIS cohort results from leg-length discrepancy and was not corrected by scoliosis surgery.
Previous literature suggested that more flexible curves was associated with more curve correction in the first erect post-op X-ray. 8 Our study further consolidated this relationship by demonstrating flexibility was also associated with subsequent correction rate up till 2-year. Consensus on intraoperative tensioning was not achieved but previous techniques described ideal tensioning should be able to obtain intraoperative correction <20° and parallel apical disks. 2 Generally, surgeons tend to increase segmental tensioning when more rigid curves are encountered. Compared to rigid curves, desirable correction in more flexible curves could be sufficiently obtained even with less tensioning per segment, possibly explaining the inverse relationship we observed between tensioning and correction. Hence, the observed relationships could merely be a reflection of common surgeon practice. Although our results did not favor a particular tensioning technique, tensioning more at the apex and less at peripherals was shown to decrease risk of screw pull-out in addition to optimizing correction in previous studies. 30 Hence, over-tensioning for more correction might not be necessary in more flexible curves, given the risks of more aggressive tensioning on increasing stress on screw-tether junction and potential for tether breakage. 31 Previous studies have shown that peripheral screws positioned posterior relative to apex could help achieve cord-tensioning effect, allowing for correction and derotation4. In contrast, screw placement did not seem to impact correction in our study.
Our study reported strong correlation between higher preoperative fulcrum flexibility and achieving clinical success, which was not demonstrated previously. We hypothesize that flexible curves are more amendable to tensioning forces exerted on the concave side of the curve during growth, hence are more prone to resisting further curve deterioration. Further GM is enabled by asymmetrical spinal growth, associated with concave vertebral height gain as well as spinal growth. 32 Differenital growth was shown to be more pronounced in instrumented major thoracic curves, while overall total spinal growth remained unchanged despite asymmetrical growth. 27 Bernard et al recommended smaller initial intraoperative correction in patients with Risser stages 0-2 and smaller preoperative curve magnitude, allowing for more growth modulation postoperatively. 33 GM was more frequently reported in skeletally immature patients,17,34 which resonated with our findings. In patients with preoperative flexibility >80%, there is greater chance of postoperative clinical success, which should be conveyed during preoperative counselling. It should also be noted that clinical success is not guaranteed despite having higher rates of treatment success in patients with more flexible curves (AUC 0.760), these should be conveyed in preoperative counselling to adjust patient expectations.
Tether breakage occurred in 32.1% of our patients, and documented occurrence can be up to 50% at 36-month. 35 Although curve deterioration was insignificant post-tether breakage, it was reported that breakage during the first 12-month resulted in consistent loss of coronal correction. 36 Dominant failure mode in tether breakage occurs at the screw-tether junction and higher failure rates were associated with higher compression force at initial correction. 31 However, our results failed to demonstrate the relationship between tensioning and incidence of breakage. Overcorrection only occurred in three patient, with recent studies suggesting lower BMI and skeletal immaturity to be critical predictors. 37
Our study provided insight on optimal surgical techniques like screw positioning and tensioning to aid surgeons in achieving improved outcomes. Strengths of our cohort included consistent 2-year postoperative follow-up and all patients attaining skeletal maturity at final follow-up. Study limitations included single-centre nature limiting size of our study cohort. With only 41 patients, secondary analysis might be underpowered (subgroup analysis for thoracic and lumbar curves). Moreover, the incompleteness of intraoperative documentation (only 46%) of tensioning variables limited further factor controlling during correlation analysis. This should be acknowledged and the effect of tensioning should be assessed in future studies. A multi-centre study would be required in the future to obtain desirable curve number for analysis, verifying relationships observed here. Potential advantages of our single-centre study included less variability in patient demographics and surgeon preferences. The inclusion of patient-reported outcome measures like Scoliosis Research Society-22 revised (SRS-22r) questionnaire would provide more comprehensive evaluation of treatment success, given that the aims of VBT surgery is preservation of mobility and function. Lastly, we were unable to accurately assess for spinal ROM as these were not systematically quantified in follow-up assessments. Some patients had private physiotherapy appointments and had no retrievable reports.
Conclusion
VBT allows for persistent curve correction, especially in flexible curves. Additional benefits of VBT included improvement in shoulder balance and preservation of progression spinal growth. Preoperative fulcrum flexibility >80% effectively predicted postoperative clinical success and these curves were unlikely to progress after index operation. Surgical success was highly correlated with presence of GM, which was associated with preoperative Risser stage ≤2.
Footnotes
ORCID iDs
Ethical Considerations
Ethics approval was obtained from the institutional review board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (IRB reference number: UW23-620).
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PWHC received funding for this work from the University of Hong Kong (HKU Seed Fund, #2302101719), JPYC received funding from the Li Shu Fan Medical Foundation Professorship in Orthopaedic Surgery.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ICMJE COI statement
All authors have no conflicts of interest to disclose.