
Abstract
Study Design
Retrospective study.
Objectives
Pulmonary complications are among the most common non-mechanical adverse events following anterior vertebral body tethering (AVBT) for adolescent idiopathic scoliosis (AIS). While preoperative pulmonary rehabilitation (PPR) has been shown to reduce postoperative pulmonary complications in thoracic surgery, its role in AVBT has not been previously evaluated. This study aimed to assess the effectiveness of a standardized PPR program in reducing early postoperative pulmonary complications after AVBT.
Methods
A total of 185 AIS patients who underwent primary AVBT between 2011 and 2024 were retrospectively reviewed. Patients were divided into two groups based on whether they received PPR 3 weeks preoperatively (PPR group, n = 144) or not (non-PPR group, n = 41). Pulmonary complications occurring within 6 weeks postoperatively—including pleural effusion, atelectasis, and chylothorax—were recorded. Patients were also categorized according to instrumentation level (thoracic, thoracolumbar, double major curve). Associations between PPR and pulmonary complications were analyzed using Fisher’s exact test, and subgroup comparisons were performed using the Fisher–Freeman–Halton exact test.
Results
Pulmonary complications occurred in 11 patients (5.9%). The complication rate was significantly lower in the PPR group compared with the non-PPR group (3.5% vs 14.6%, P = .016). Patients who did not receive PPR had a higher risk of pulmonary complications (risk ratio 4.21; 95% CI, 1.35-13.11). No significant differences in complication rates were observed among instrumentation subgroups (P = .709).
Conclusion
AVBT is a thoracic procedure associated with pulmonary complications, and the role of preoperative pulmonary rehabilitation (PPR) in this setting has not been previously studied. In this study, PPR was associated with a lower rate of early postoperative pulmonary complications; however, due to the retrospective time-based design, causality cannot be established. Further prospective, multicenter studies are needed to clarify its independent effect.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) is defined as a spinal deformity characterized by a Cobb angle greater than 10°, after exclusion of other potential causes. 1 Treatment strategies vary according to curve severity and skeletal maturity. Among surgical options, posterior spinal fusion (PSF) remains the gold standard. 2 In contrast, anterior vertebral body tethering (AVBT), a growth-modulating technique, has been increasingly adopted worldwide. In this procedure, screws are inserted along the convex side of the curve and connected by a polyethylene tether, allowing asymmetric growth in accordance with the Hueter–Volkmann principle, thereby promoting curve correction. 3 Favorable outcomes have been reported in several studies.4,5 Nevertheless, complications have also been described. Mechanical complications such as tether breakage or curve overcorrection are the most frequently encountered, but non-mechanical complications have also been documented.6,7,8 Among the latter, pulmonary complications including pleural effusion, atelectasis, and pneumonia represent the most common group.9,10
The administration of anesthetic agents and the use of endotracheal intubation during surgery impair ciliary activity in the lungs, thereby increasing the likelihood of postoperative pulmonary complications. 11 AVBT, whether performed thoracoscopically or through thoracotomy, requires opening of the thoracic cavity. Previous studies have reported that pulmonary complications occur frequently in patients undergoing thoracotomy. 12 Such postoperative complications are associated with prolonged hospital stays and increased healthcare costs.13,14 Evidence from thoracic surgery indicates that preoperative pulmonary rehabilitation (PPR) enhances mucociliary clearance and improves diaphragmatic function.15,16 Consequently, PPR has been shown to reduce the incidence of postoperative pulmonary complications.17,18
Based on previous findings in the literature, it is hypothesized that preoperative pulmonary rehabilitation (PPR) may reduce the incidence of pulmonary complications following AVBT. The present study aimed to evaluate early postoperative pulmonary complications in AIS patients undergoing AVBT and to assess the effectiveness of PPR in preventing these adverse outcomes.
Materials and Methods
Study Design
This retrospective study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Data were obtained from the hospital database, and 185 patients (31 males, 154 females) with adolescent idiopathic scoliosis who underwent AVBT between 2011 and 2024 were included. All patients were fully informed about the study procedures, and written informed consent was obtained, outlining surgical risks and potential complications. Demographic and clinical data, including age, sex, scoliosis type, treatment plan, and pulmonary complications, were systematically recorded.
This retrospective cohort study used a pre-post (time-based) design. At our institution, a standardized preoperative pulmonary rehabilitation (PPR) program was implemented after the first AVBT cases. Patients treated before implementation did not receive PPR (non-PPR group, n = 41), while all consecutive patients treated after implementation received the standardized PPR protocol 3 weeks prior to surgery (PPR group, n = 144). Since group assignment was based on calendar time rather than randomization, the comparison is sensitive to time trend effects.
Patients were categorized into three groups according to the surgical level (thoracic, thoracolumbar, and double major curve) and into two groups according to PPR status (received vs not received). Instrumentation confined to the thoracic cavity was classified as thoracic; instrumentation extending across the diaphragm was classified as thoracolumbar; and instrumentation applied ipsilaterally to both thoracic and lumbar vertebrae was classified as double major curve.
Inclusion criteria were a diagnosis of idiopathic scoliosis during adolescence and having undergone primary AVBT surgery at our institution during the study period. Exclusion criteria included revision surgery for any reason, congenital scoliosis, intraspinal anomalies, hybrid/revision procedures involving posterior spinal fusion, and known pre-existing respiratory disorders. Primary outcome status (pulmonary complication within 6 weeks) was determined for all included patients; where secondary variables were missing, analyses were performed using available case data.
Outcomes and Definitions
The primary outcome was the occurrence of a postoperative pulmonary complication within 6 weeks of surgery. Pulmonary complications were defined as any of the following events diagnosed at the time of initial hospital admission or during any unscheduled visit and/or routine follow-up within the 6-week postoperative period: pleural effusion, atelectasis, or chylothorax.
Pulmonary complications were identified through standardized in-hospital clinical evaluation by the treatment team and the consulting thoracic surgeon. All patients underwent routine chest X-rays after chest tube removal, and additional chest X-rays and/or CT scans were performed as clinically necessary (eg, dyspnea, hypoxemia, tachypnea, respiratory distress) or as recommended by the consulting thoracic surgeon.
Definitions were as follows: Pleural effusion was defined as a recent postoperative accumulation of pleural fluid documented on chest X-ray and/or CT. Effusions were further categorized by clinical management as: observation only (no intervention), medical management (eg, supplemental oxygen and/or respiratory physiotherapy), or invasive intervention (eg, thoracentesis or pleural drainage catheter placement). Atelectasis was defined as radiographic evidence of lobar or segmental collapse on chest X-ray and/or CT, with or without respiratory symptoms, and managed with respiratory physiotherapy and/or additional supportive care as clinically indicated. Chylothorax was defined as postoperative pleural drainage (characteristic milky appearance) diagnosed by the consulting thoracic surgeon and consistent with biochemical confirmation and/or supportive clinical course (eg, response to dietary modification and/or somatostatin therapy) where available.
For transparency, clinically significant pulmonary complications were defined as any pulmonary complication associated with increased respiratory symptoms and/or care, including the need for supplemental oxygen beyond routine postoperative care, intensive care unit monitoring/transfer, bronchoscopypleural drainage, and/or hospital readmission for respiratory symptoms. We also reported a secondary consequence of pulmonary complications: thoracentesis or pleural catheter placement.
Preoperative Pulmonary Rehabilitation Protocol
Incentive spirometry 15 min Diaphragm breathing exercises 15 min Pursed-lip breathing 20 repeats Effective coughing technique 20 min
Prior to surgery, patients were instructed to practice a standardized PPR protocol for 3 weeks, with three to four sessions per day. Each session consisted of incentive spirometry (15 min), diaphragmatic breathing exercises (15 min), pursed-lip breathing (20 repetitions), and effective coughing technique (20 min), lasting approximately 45-50 min per session. Practice and technique were monitored by a physiotherapist. At the initial clinical visit, patients received detailed instructions and supervised practice to ensure each exercise was performed correctly. Patients kept a daily exercise diary, reviewed by the physiotherapist, to document practice. All patients received counseling on preoperative expectations and the importance of continuing postoperative breathing exercises.
Surgical Technique
All patients were operated on under total intravenous anesthesia in the lateral decubitus position. A double-lumen endotracheal tube was used in all cases, and the tidal volume of the ipsilateral lung was reduced during thoracic instrumentation. Patients were divided into three groups according to the surgical levels and analyzed accordingly. This grouping was based on factors such as diaphragmatic incision and the use of a double-lumen tube. It is well established that diaphragmatic incision and selective ventilation with a double-lumen tube may increase the risk of pulmonary complications. For thoracic curves, thoracoscopy was combined with a mini-open intercostal approach. For thoracolumbar curves, a mini-retroperitoneal approach was preferred to access L2 and the lower vertebral levels. The diaphragm was incised sufficiently to allow passage of sutures and was primarily repaired following fixation. Double major curves were corrected in the same session, with the procedure initiated by lumbar instrumentation. In patients undergoing AVBT for double major curves, a thoracic drainage tube was inserted in all cases, including those with bilateral procedures.
Postoperative Rehabilitation
All patients were monitored in the ward following surgery. Standard postoperative respiratory physiotherapy was initiated early postoperatively under the supervision of a physiotherapist and repeated throughout the day. Patients were mobilized on the first postoperative day and encouraged to ambulate frequently. Patients were followed under the supervision of a consulting thoracic surgeon throughout their hospitalization. Chest tube output was recorded daily, and tubes were removed once drainage decreased below 100 mL. After chest tube removal, scoliosis radiographs were obtained to evaluate correction. Patients were instructed to continue the preoperative respiratory rehabilitation program for 6 weeks after discharge. This postoperative respiratory physiotherapy program was applied similarly in both groups. A routine follow-up was scheduled at 6 weeks; however, patients experiencing respiratory difficulties at any time were advised to seek immediate medical attention.
Statistical Analysis
All statistical analyses were performed using SPSS Statistics (version 26.0). Descriptive statistics were calculated for all demographic and clinical variables. Continuous variables were summarized as mean ± standard deviation (SD), and categorical variables were summarized as numbers and percentages. Intergroup comparisons for continuous variables were performed using the independent samples t-test (or Mann-Whitney U test when distribution assumptions were not met). Categorical variables were compared using the Pearson chi-square test when expected cell counts were sufficient; otherwise, Fisher’s exact test was applied. The primary association between preoperative pulmonary rehabilitation (PPR; yes/no) and postoperative pulmonary complications (yes/no) was assessed using Fisher’s exact test. Differences in complication rates between instrumentation types (thoracic, thoracolumbar, double major curve) were assessed using an exact test for RxC tables (Fisher-Freeman-Halton exact test). Effect sizes were reported as risk ratios (RR) and/or odds ratios (OR) along with 95% confidence intervals (CI). Because the total number of outcome events was small (n = 11), multivariable regression or propensity-based adjustment was not performed to avoid model overfitting; therefore, results are presented as unadjusted associations. All tests were two-sided, and P < .05 was considered statistically significant.
Results
During the study period, 241 AVBT cases were reviewed for eligibility. Ten cases that did not represent primary AIS AVBT procedures (eg, non-AIS diagnoses and/or miscoded cases), seven patients who underwent hybrid surgery involving posterior spinal fusion, and five patients who underwent revision AVBT were excluded. Additionally, four patients were excluded due to documented pre-existing respiratory disorders. After applying these pre-defined clinical exclusions (n = 26), 215 cases remained. Finally, 30 more cases were excluded due to the inability to determine the primary endpoint within the 6-week postoperative period (eg, follow-up outside our institution or incomplete postoperative documentation). Therefore, the final analytical cohort comprises 185 patients.
In the final analytical cohort (n = 185), the mean age was 12.44 years (range, 8-18), and the majority were female (83.2%). Preoperative pulmonary rehabilitation was performed on 144 patients (77.8%), while 41 patients (22.2%) did not receive any preoperative pulmonary rehabilitation.
Baseline Characteristics of Patients by Preoperative Pulmonary Rehabilitation Status
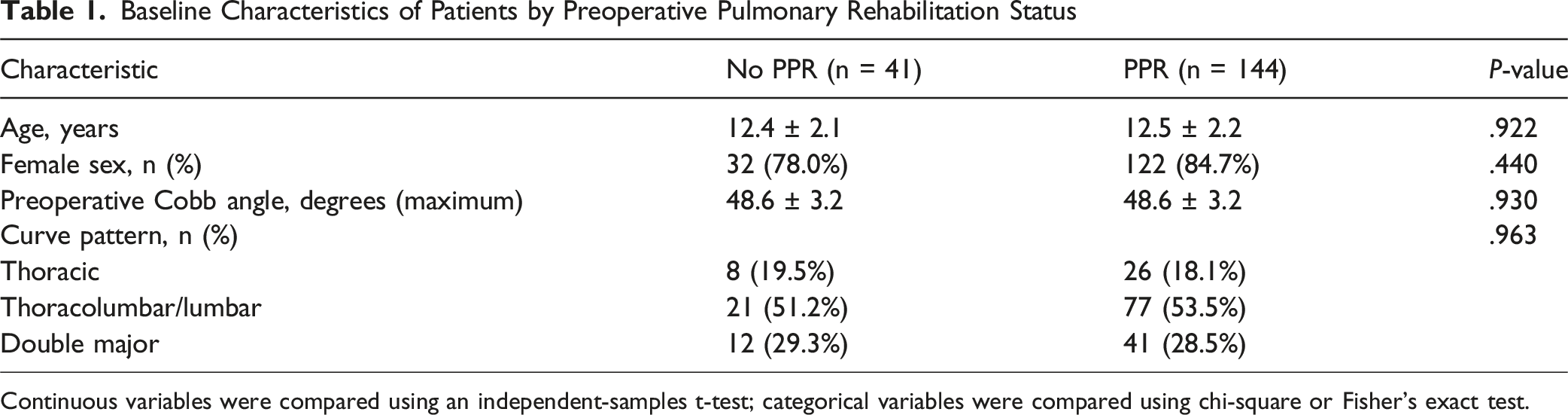
Continuous variables were compared using an independent-samples t-test; categorical variables were compared using chi-square or Fisher’s exact test.
Relationship Between Pulmonary Rehabilitation and Pulmonary Complications

P-value from Fisher’s exact test.
Relationship Between Instrumentation Type and Postoperative Complications

P-value from Fisher–Freeman–Halton exact test (RxC exact test).
Six patients in the group that did not receive PPR treatment experienced pulmonary complications. Four of these patients developed pleural effusion, and two developed atelectasis. Two of those with pleural effusion were in the thoracolumbar group, one was in the double major curve group, and one was in the thoracic group. Symptoms of respiratory distress were observed in six patients, with two cases presenting at a milder level of severity. The patients’ diagnoses were made based on chest X-rays and follow-up examinations. In one patient in the double major curve group, the content of the drainage from the chest tube changed after oral intake, and the patient was diagnosed with chylothorax. This patient’s oral intake was discontinued, and IV nutrition was started along with somatostatin treatment. Pleural effusion was observed in one patient at the fourth week after discharge. The patient had respiratory distress and was therefore hospitalized and monitored with daily chest X-rays. The patient’s pleural effusion did not decline during follow-ups, and respiratory distress began. Therefore, a thoracic drainage catheter was inserted based on a recommendation from the thoracic surgery department (Figure 1). Respiratory distress began on the second day after the removal of chest tubes in patients, and atelectasis was observed on chest X-rays (Figure 2). A computed tomography (CT) scan of the chest was performed on patients based on the recommendation of the thoracic surgery consultant. Bronchoscopy was recommended for the patients, and a mucus plug in the bronchi was observed during bronchoscopy. Two patients who underwent bronchoscopy were monitored in intensive care for a day. After the mucus plugs were removed, the patients’ complaints started to decrease, and radiological images started to improve. Posteroanterior chest X-ray taken due to respiratory distress in a patient with pleural effusion (A). X-ray image on the second day after insertion of the drainage catheter (B). X-ray image on the fourth day after removal of the drainage catheter (C) Posteroanterior chest X-ray of a patient following removal of the chest tube from the left lung after double major curve AVBT surgery (A). Chest CT images of the patient (B and C). Follow-up X-ray taken on the second day after bronchoscopy (D)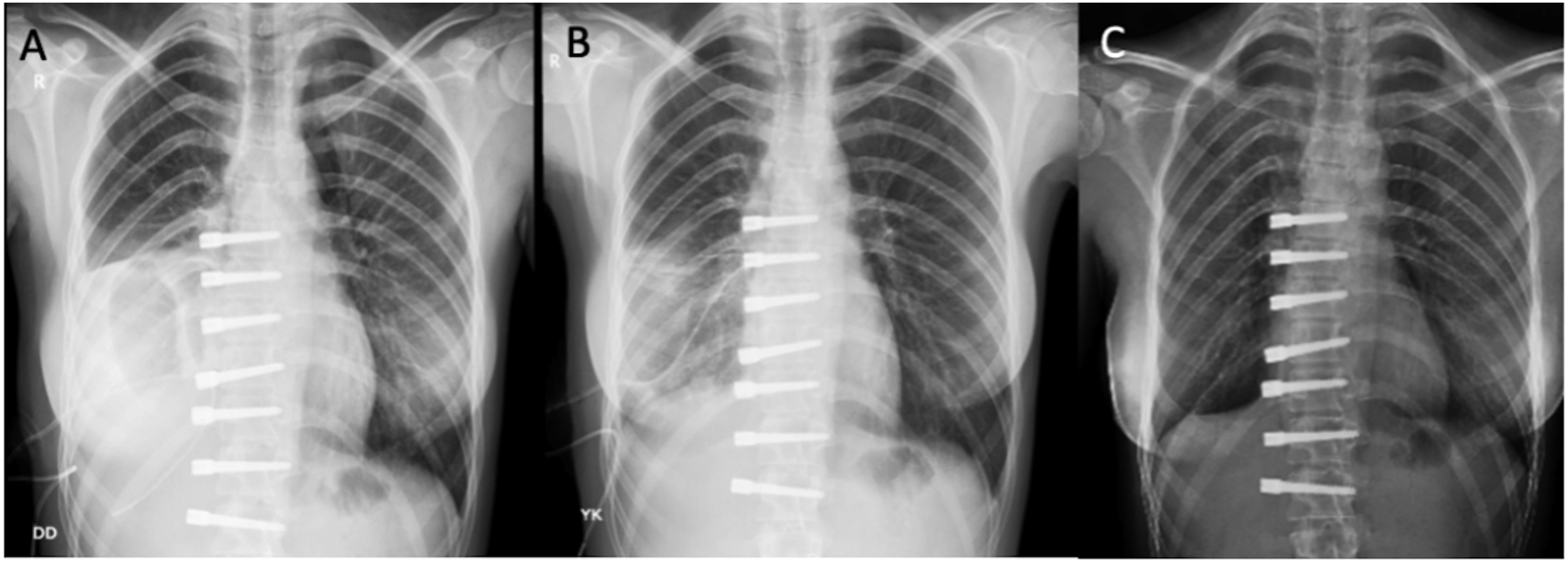

In the group that underwent PPR, five patients (3.47%) developed pleural effusion. Two of them were in the thoracolumbar group, and three were in the double major curve group. Among the patients with pleural effusion, two presented with symptoms of respiratory distress, which were mild in severity. Pleural effusion was detected in four patients during their follow-up in the ward, and they were monitored with daily chest X-rays. Improvements were seen in the radiological images without any additional interventions. At the sixth-week follow-up, one patient reported experiencing mild dyspnea. A chest radiograph obtained during scoliosis imaging revealed pleural effusion. The patient was therefore hospitalized and managed conservatively.
Discussion
This study is the first in the literature to evaluate preoperative pulmonary rehabilitation in preventing pulmonary complications seen after AVBT surgery. Minimal, asymptomatic pleural effusions are frequently observed after thoracic surgery and usually resolve spontaneously without clinical recognition or intervention. Minimal pleural effusions can occur after thoracic surgery and often resolve on observation alone; however, in this study, we recorded pulmonary complications confirmed radiographically (chest X-ray and/or CT) within the first 6 weeks postoperatively. To emphasize clinical significance, we further classified complications as clinically significant when they were associated with respiratory symptoms (eg, dyspnea, hypoxemia, persistent cough) and/or increased care (eg, intensive care unit monitoring, bronchoscopy, pleural drainage). This approach allowed us to distinguish clinically significant events from incidental imaging findings. In the present study, it was determined that pulmonary complications in the early postoperative period were statistically significantly decreased in patients who underwent PPR compared to those who did not. These findings suggest that incorporating a standardized PPR protocol into preoperative care may help reduce early pulmonary complications after AVBT.
In a study by Baroncini et al. evaluating the learning curve of AVBT, 90 patients were analyzed, and a significant reduction in operative time and intraoperative blood loss was observed after the first 20 cases. 19 The authors concluded that the learning curve for AVBT is relatively short. In a study by Trobisch et al., cases from the early phase of the learning curve were excluded, and a total of 140 patients were included; the rate of pulmonary complications was reported as 10%. 9 In a study by Alanay et al. including 31 patients, pulmonary complications were observed in 4 patients (12%). 8 Similarly, studies evaluating pulmonary complications following AVBT have reported rates ranging from 3% to 25%.19,20,21,22 In our study, consistent with the literature, pulmonary complications were observed in 11 out of 181 patients (5.9%). Notably, the rate of symptomatic pulmonary complications was 13.4% in the first 41 patients, compared to 3.5% in the group in which PPR was applied. We believe that PPR may have contributed to the reduction in complication rates; however, the effect of the learning curve was not specifically evaluated and therefore cannot be excluded.
In the literature, there are studies in which it has been reported that preoperative pulmonary rehabilitation, especially in thoracic surgery, can reduce postoperative complications. In a prospective randomized study conducted by Sweity et al. including 80 patients, participants were divided into two groups. Incentive spirometry was applied to 40 patients prior to coronary artery bypass surgery. The incidence of atelectasis was 20% in the intervention group compared to 42.5% in the control group. Additionally, a significant difference was observed in postoperative mechanical ventilation duration. 18 In another study, patients who underwent lung resection for small cell lung cancer were evaluated. Among 26 patients, 14 received preoperative respiratory muscle endurance training for 3 weeks. This group demonstrated a significantly lower rate of postoperative pulmonary complications. 23 Similarly, in a study by Benzo et al., patients undergoing lung resection for lung cancer were assessed, and those who received preoperative pulmonary rehabilitation achieved better clinical outcomes. 24 Overall, the effectiveness of preoperative physiotherapy in reducing postoperative complications has been demonstrated in thoracic surgery, cardiac surgery, and lung cancer surgery. 25 PPR was not applied in the first 41 patients in our case series, and pulmonary complications were observed in six (14.6%) patients in the early period. Four of these pulmonary complications were pleural effusion, and two were atelectasis. Three patients who developed pleural effusion applied with respiratory complaints after discharge. Chylothorax developed in one patient during follow-up. To reduce these rates, we developed a preoperative pulmonary rehabilitation protocol based on the literature and strictly adhered to this protocol for all subsequent patients. Pulmonary complications were observed in five (3.5%) of the 144 patients who received PPR. No atelectasis developed in the group that underwent PPR, and all complications were pleural effusion. No pulmonary complication was observed in any of the patients included in the study after the sixth postoperative week.
In the present study, patients were categorized into three main groups based on the levels of vertebral instrumentation. Although no statistically significant differences were observed among instrumentation subgroups, the clinical implications of curve location and the corresponding surgical approach warrant further consideration. Thoracic procedures are typically performed using a thoracoscopic approach with single-lung ventilation, whereas correction of thoracolumbar curves generally requires diaphragmatic incision. In the double major curve group, bilateral chest drainage tubes were used. These technical differences may influence pulmonary mechanics, postoperative pain, and secretion clearance, potentially affecting both the incidence and type of pulmonary complications. In our cohort, the majority of pulmonary complications occurred in patients who underwent thoracolumbar and double major curve instrumentation. This finding may be associated with diaphragmatic manipulation and increased surgical invasiveness. Although this trend did not reach statistical significance, it may still be clinically relevant. A more detailed evaluation of how variations in surgical approach influence pulmonary outcomes could provide valuable guidance for surgical planning and the selection of instrumented levels.
In the literature, various rates of pulmonary complications have been reported in studies that have reported AVBT results. Although pulmonary complications are seen at a high rate, treatment is generally conservative. 9 In the present study, conservative treatment was applied to eight patients. Among patients with pleural effusion, eight of nine presented with respiratory symptoms, whereas one of nine was detected incidentally on imaging and was managed conservatively. One patient was diagnosed with chylothorax based on changes in the content of drainage from the chest tube.
Considering the treatment of post-AVBT pulmonary complications, conservative treatments were mostly preferred in patients with pleural effusion. A drainage catheter was used in one patient due to persistent effusion. Oral intake was discontinued in the patient who developed chylothorax, and carbohydrate-free, protein-rich IV nutrition was initiated. All complications developed within the first 6 weeks.
Atelectasis was identified on chest radiographs in two patients who presented with respiratory distress and persistent cough. Bronchoscopy was performed in two patients who developed atelectasis, and mucus plugs were observed in the bronchi. After removal of the mucus plugs, lung aeration completely recovered on the third and fourth days. All pulmonary complications recovered without leaving any sequelae in patients. Although atelectasis was observed in two patients in the group that did not undergo PPR, atelectasis did not develop in the group that underwent PPR. Of the two patients with atelectasis, one belonged to the thoracolumbar group and the other to the double major curve group, suggesting that procedures involving diaphragmatic passage may represent a risk factor for atelectasis. No atelectasis developed in the group that received PPR. This observation may reflect improved secretion clearance, breathing mechanics, and early recognition of respiratory symptoms after structured preoperative breathing training.
In a study conducted by Trobish et al. to evaluate pulmonary complications observed after AVBT, it was demonstrated that incision of the diaphragm to allow passage of the sutures was a risk factor for pulmonary complications. In the study, it was reported that 71% of all pulmonary complications developed in cases where the diaphragm was incised. 9 In our study, we observed that 10 (90.9%) pulmonary complications were in the thoracolumbar or double major curve group. In this study, although complications were observed more frequently in the thoracolumbar and double major curve groups, this result was not statistically significant.
This study has several limitations. First, pulmonary function tests were not routinely performed in patients with AIS in our clinical practice. Therefore, preoperative pulmonary capacity could not be objectively assessed. Second, there was a numerical imbalance between the groups, with more patients in the PPR group. This was due to the time-based design, as the PPR protocol was introduced after the initial AVBT cases. Consequently, patients in the PPR group were treated later, and improvements in surgical technique and perioperative care over time may have affected the results. Thus, the observed reduction in pulmonary complications should be interpreted as an association rather than a causal effect. Third, adherence to the pulmonary rehabilitation protocol at home could not be objectively monitored. Although patients received standardized instructions and initial supervision, variations in compliance may have influenced the outcomes. Additionally, the small number of pulmonary complications limited the ability to perform multivariable analyses and may have led to wide confidence intervals. Overall, these limitations indicate the need for larger, prospective, multicenter studies to better clarify the independent effect of preoperative pulmonary rehabilitation on postoperative pulmonary complications after AVBT.
Conclusions
AVBT is a thoracic surgical procedure associated with a risk of pulmonary complications. To date, no studies have specifically evaluated the role of preoperative pulmonary rehabilitation (PPR) in this setting. In the present study, PPR was associated with a lower rate of early postoperative pulmonary complications following AVBT. However, given the retrospective and time-based design, these findings should be interpreted with caution and do not establish causality. Further prospective, multicenter studies with larger sample sizes are needed to better define the independent effect of preoperative pulmonary rehabilitation in this patient population.
Footnotes
Ethical Considerations
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of Memorial Şişli Hospital, Istanbul, Türkiye (Approval No: 002, Date: 23 June 2025).
Consent to Participate
Written informed consent to participate was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.