
Abstract
Study design
Retrospective cohort study.
Objectives
To describe temporal trends in opioid use disorder (OUD) among adults undergoing inpatient cervical fusion, identify factors independently associated with OUD, and compare resource use and complications by OUD status.
Methods
Adult elective cervical fusion hospitalizations were identified in the National Inpatient Sample (NIS) from 2016 to 2022. OUD was defined using ICD-10-CM code lists. Survey-weighted procedures estimated annual prevalence and group means. Multivariable logistic regression was used to evaluate risk factors associated with OUD as well as medical complications and discharge disposition. Significance was set at P < 0.05.
Results
Odds of OUD were higher at ages 30-39 (OR 2.38, P < 0.001), 40-49 (OR 2.25, P < 0.001), 50-59 (OR 2.11, P = 0.001), and 60-69 (OR 1.65, P = 0.031) vs <30, and increased with clinical severity (Severity 2 OR 1.29; Severity 3 OR 1.79; Severity 4 OR 1.58; P < 0.001 for all). OUD patients had higher odds of undergoing multilevel fusion (OR 1.12, P < 0.001) and having co-occurring mental illness (OR 1.23, P < 0.001), alcohol abuse (OR 1.41, P < 0.001), and cannabis use (OR 1.59, P < 0.001). OUD was associated with higher odds of cardiovascular (OR 1.31, P < 0.001) and mechanical complications (OR 1.76, P < 0.001). OUD was associated with longer inpatient stays (3.23 vs 2.47 days, P < 0.001) and higher costs ($31,900 vs $27,000, P < 0.001) than those without OUD.
Conclusions
Patients with OUD undergoing cervical fusion are a clinically complex, resource-intensive subgroup with higher risks of cardiovascular and mechanical complications and non-routine discharge. Targeted risk stratification and OUD-tailored perioperative pathways can be used to improve outcomes.
Keywords
Introduction
Opioid use disorder (OUD) has risen sharply and is a major public health concern. In 2022, an estimated 2.1 million Americans aged 12 years or older met criteria for OUD, reflecting a growing healthcare burden. 1 Opioid use also affects surgical care. Nearly 1 in 4 patients present for surgery already using opioids, and the prevalence of diagnosed OUD among surgical inpatients more than doubled from 0.58% in 2010 to 1.41% in 2018.2,3 Spine procedures, particularly cervical fusion operations such as anterior cervical discectomy and fusion (ACDF) and posterior cervical decompression and fusion (PCDF), involve substantial postoperative pain, so opioids remain common in perioperative management. 4 As more opioid-dependent patients enter the cervical fusion pathway, concerns about management and outcomes continue to grow.
Preoperative opioid exposure predicts persistent postoperative use and adverse cervical fusion outcomes. 5 Chronic opioid use is linked to lower fusion success, including a higher risk of pseudoarthrosis and, in some cases, revision after ACDF. 6 Functional outcomes show similar patterns, with chronic users reporting worse pain and lower satisfaction at baseline. 7 OUD also adds financial burden, with longer hospital stays, more intensive care unit (ICU) care, and markedly higher hospitalization costs — on the order of 5 extra days and more than $50,000 per admission. 1 These trends, together with evolving opioid epidemiology and changing cervical fusion volumes in the United States, support the need for updated, nationally representative analyses across single and multilevel ACDF and PCDF.
The aim of this study was to (1) characterize recent trends in OUD among patients undergoing cervical fusion, (2) quantify the association between OUD and perioperative resource use, and (3) evaluate OUD-associated differences in surgical and discharge outcomes. We hypothesized that patients with OUD would demonstrate higher complication rates, greater odds of non-routine discharge, and increased resource use when compared to those without OUD.
Methods
Data Source
We performed a retrospective observational study using the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) from 2016 to 2022, a stratified sample of U.S. community hospital discharges that supports national estimates after applying survey weights. Given that the HCUP-NIS is a de-identified, publicly available database, this study was exempt from institutional review board (IRB) approval, and informed consent was not required. Because the NIS captures information only for individual hospitalizations and does not include longitudinal patient identifiers, outcomes in this study were limited to events occurring during the index hospitalization.
Cohort Identification and Exclusions
We included adults (≥18 years) hospitalized for cervical fusion procedures from 2016 to 2022. Encounters were excluded if the admission was non-elective; if age or essential hospital/payer/cost fields were missing or implausible; if the index fusion was not performed on admission day; or if recorded length of stay or costs were negative. Because indication-level clinical detail is limited in the NIS, revision procedures and specific underlying diagnoses such as pseudarthrosis, OPLL, or neoplasm were not separately excluded if they were captured within otherwise eligible elective cervical fusion hospitalizations.
Opioid Use Disorder
OUD was defined using the HCUP-published ICD-10-CM code list, which includes diagnostic codes for opioid use, abuse, dependence, poisonings/adverse effects, and long-term opioid therapy. 8 Patients were assigned to the OUD cohort if any listed diagnosis during the index hospitalization matched the HCUP-published ICD-10-CM code list. Accordingly, this study examined diagnosis-based OUD identified during the index hospitalization rather than preoperative opioid exposure characterized by prescription duration, chronicity, or morphine milligram equivalent thresholds.
Patient, Hospital, and Clinical Characteristics
We summarized demographics, socioeconomic indicators, primary payer, and hospital characteristics. Clinical factors included illness severity, fusion level (single vs multi-level), co-occurring mental illness (depression or psychoses), alcohol use disorder, and cannabis use. Comorbidities were derived via HCUP Elixhauser definitions, and a summary Elixhauser Comorbidity Index (ECI) was computed as the count of present conditions.
Outcomes
Primary outcomes were annual prevalence of OUD among cervical fusion hospitalizations and patient and hospital factors associated with OUD (adjusted odds by demographics, payer, comorbidity burden, illness severity, fusion level, and hospital characteristics). Secondary outcomes were resource-use trends by OUD status such as inpatient length of stay (LOS), inflation-adjusted hospital costs, and perioperative complications. Perioperative complications were identified during the index hospitalization using ICD-10-CM/PCS codes and grouped into cardiovascular, respiratory, and neurologic categories. Individual complications such as dysphagia, mechanical complications, and sepsis were also captured. A binary composite indicating 1 or more complications was created and labeled adverse events.
Cost Conversion and Inflation Adjustment
Total hospital charges were converted to costs using hospital and year-specific cost-to-charge ratios and then adjusted to 2022 U.S. dollars using Consumer Price Index multipliers.
Statistical Analysis
All analyses incorporated NIS stratification, clustering, and discharge weights per HCUP guidance. Because this was an exploratory retrospective analysis of a national administrative database, no a priori sample size calculation was performed. Instead, all eligible cervical fusion hospitalizations meeting study criteria during 2016-2022 were included. We estimated annual OUD prevalence and survey-weighted means with 95% CIs and summarized temporal change using compound annual growth rate. To identify factors associated with OUD, we fit a survey-weighted logistic regression including year and all covariates above, reporting odds ratios (ORs) with 95% CIs. To evaluate perioperative outcomes associated with OUD, we fit survey-weighted logistic models for the adverse-event composite, complication categories and selected individual complications, and non-routine discharge, adjusting for the same covariates. Statistical significance was set at P < 0.05. Analyses were conducted in R (version 4.4.0; R Project for Statistical Computing, Vienna, Austria).
Results
Temporal Trends in OUD Prevalence and Utilization
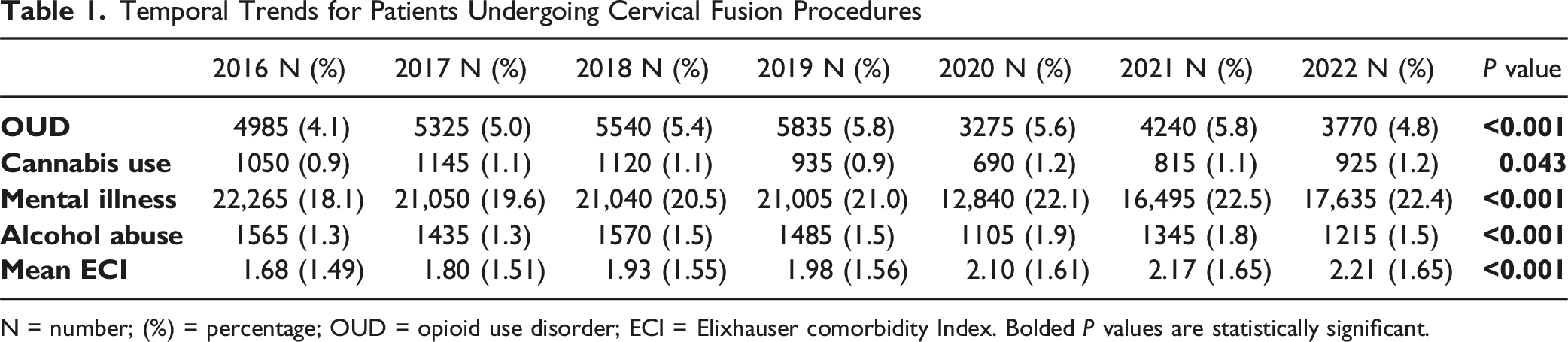
From 2016 to 2022, the prevalence of documented OUD among cervical fusion hospitalizations increased from 4.1% in 2016 to 5.8% in 2019, remained relatively stable through 2021 (5.6%–5.8%), and then declined to 4.8% in 2022 (P < 0.001). Cannabis use, mental illness, alcohol abuse, and the mean ECI also rose over time (Figure 1; Table 1). Annual prevalence of opioid use disorder (OUD) among cervical fusion hospitalizations from 2016 to 2022 Temporal Trends for Patients Undergoing Cervical Fusion Procedures N = number; (%) = percentage; OUD = opioid use disorder; ECI = Elixhauser comorbidity Index. Bolded P values are statistically significant.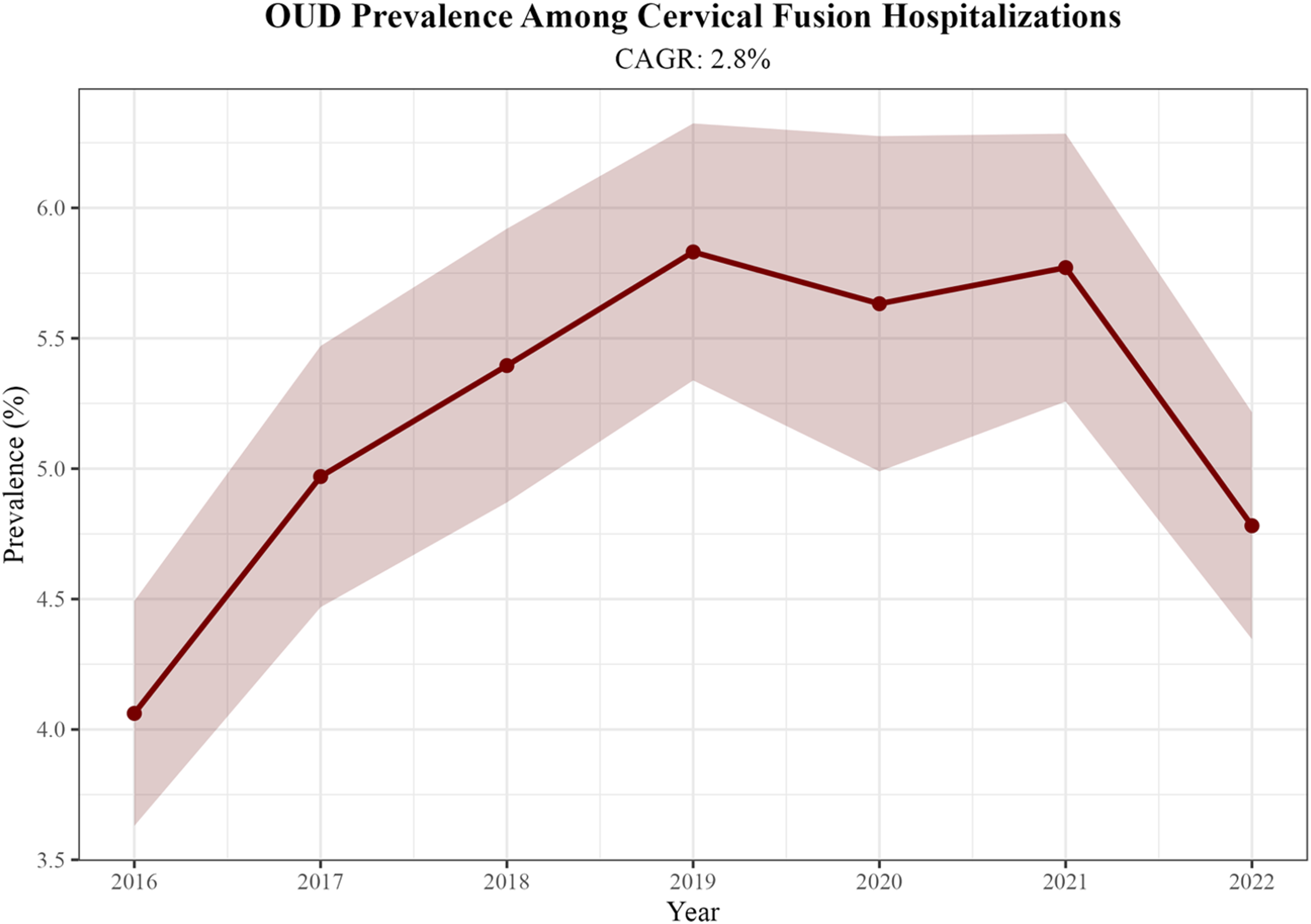
Patient Characteristics by OUD Status
Temporal Trends in Opioid Use Disorder and Comorbidities Among Patients Undergoing Cervical Fusion From 2016 to 2022
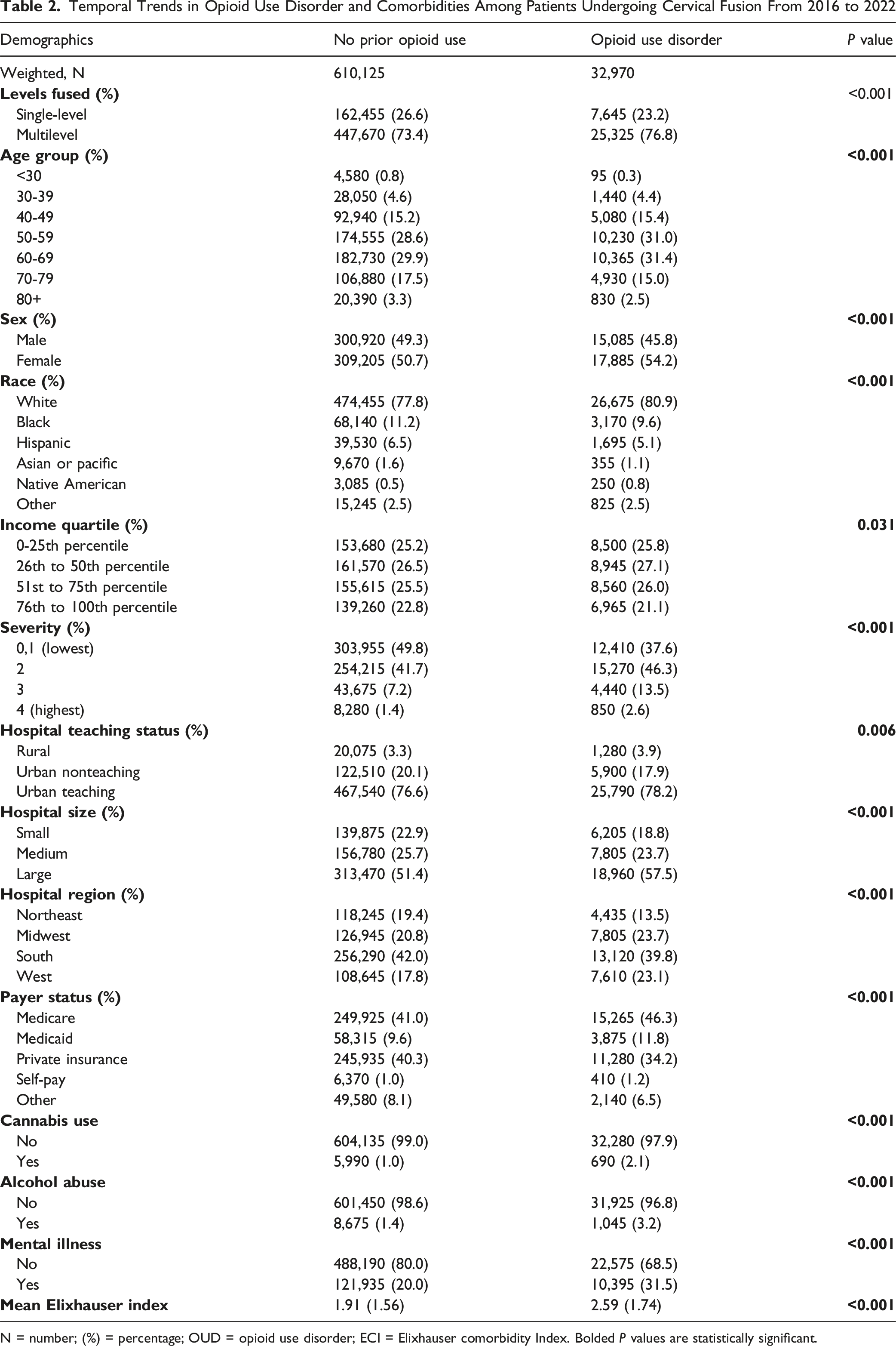
N = number; (%) = percentage; OUD = opioid use disorder; ECI = Elixhauser comorbidity Index. Bolded P values are statistically significant.
Factors Independently Associated With OUD
Multivariable Analysis of Factors Associated With Opioid Use Disorder in Cervical Fusion Patients
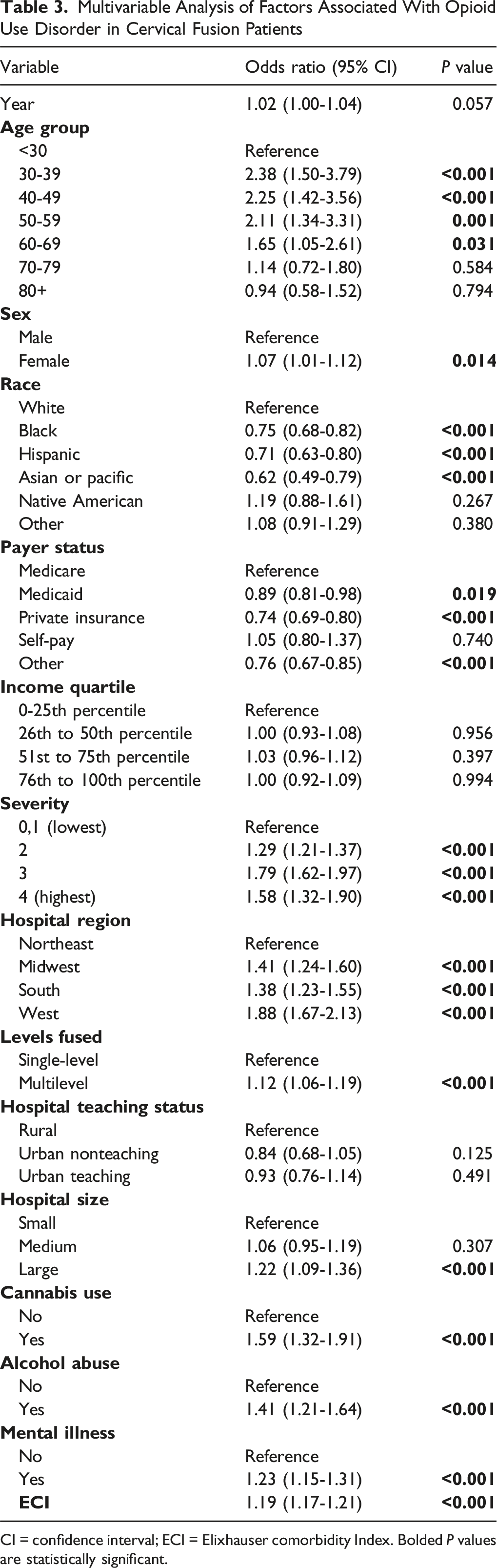
CI = confidence interval; ECI = Elixhauser comorbidity Index. Bolded P values are statistically significant.
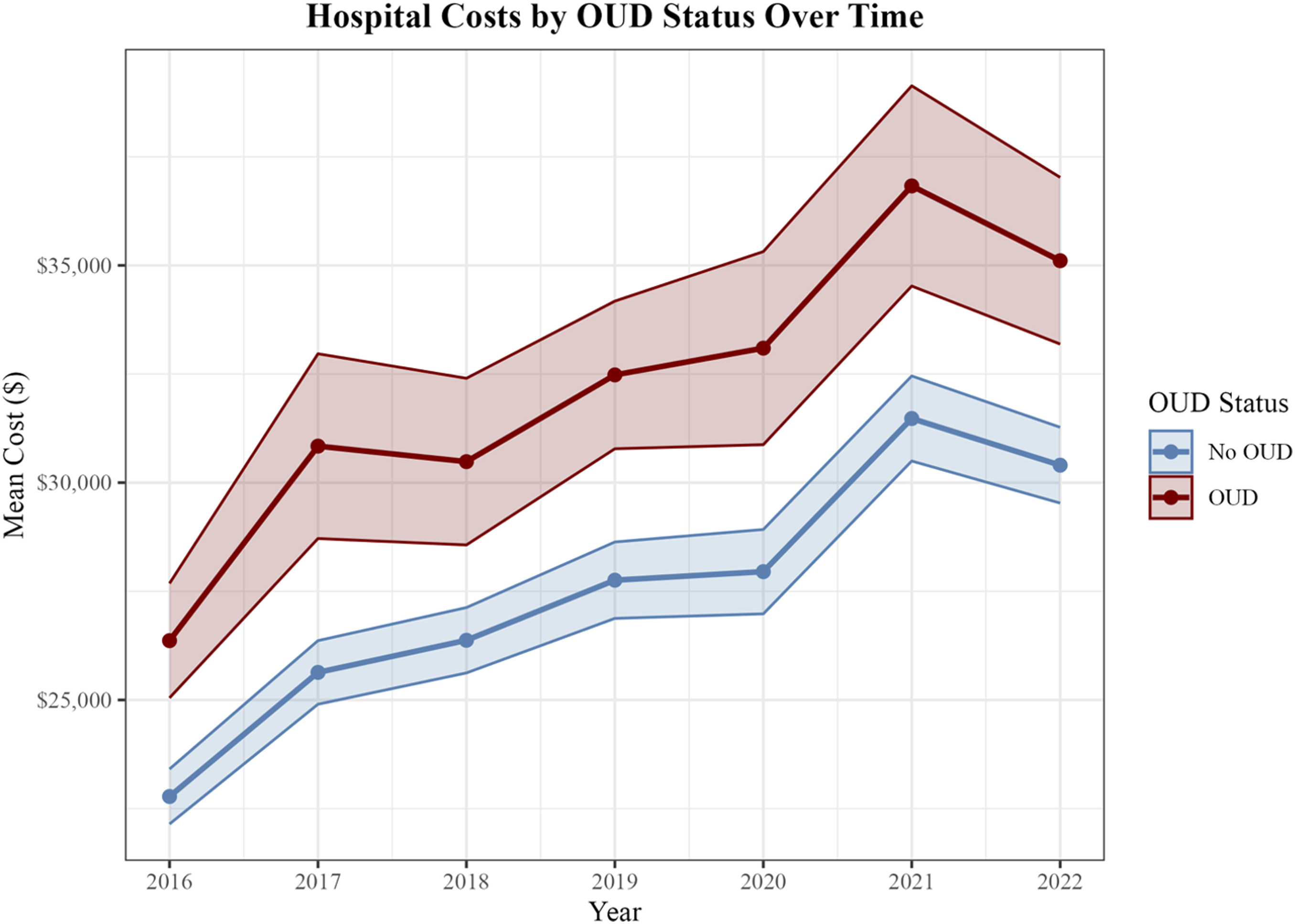
Length of Stay and Hospital Costs by OUD Status
OUD was associated with longer inpatient stays (3.23 vs 2.47 days, P < 0.001) and higher costs ($31,900 vs $27,000, P < 0.001) than those without OUD. Both groups showed temporal shifts consistent with broader utilization patterns (Figures 2 and 3). Length of stay (LOS) by opioid use disorder (OUD) status among cervical fusion hospitalizations from 2016 to 2022 Hospital costs by opioid use disorder (OUD) status among cervical fusion hospitalizations from 2016 to 2022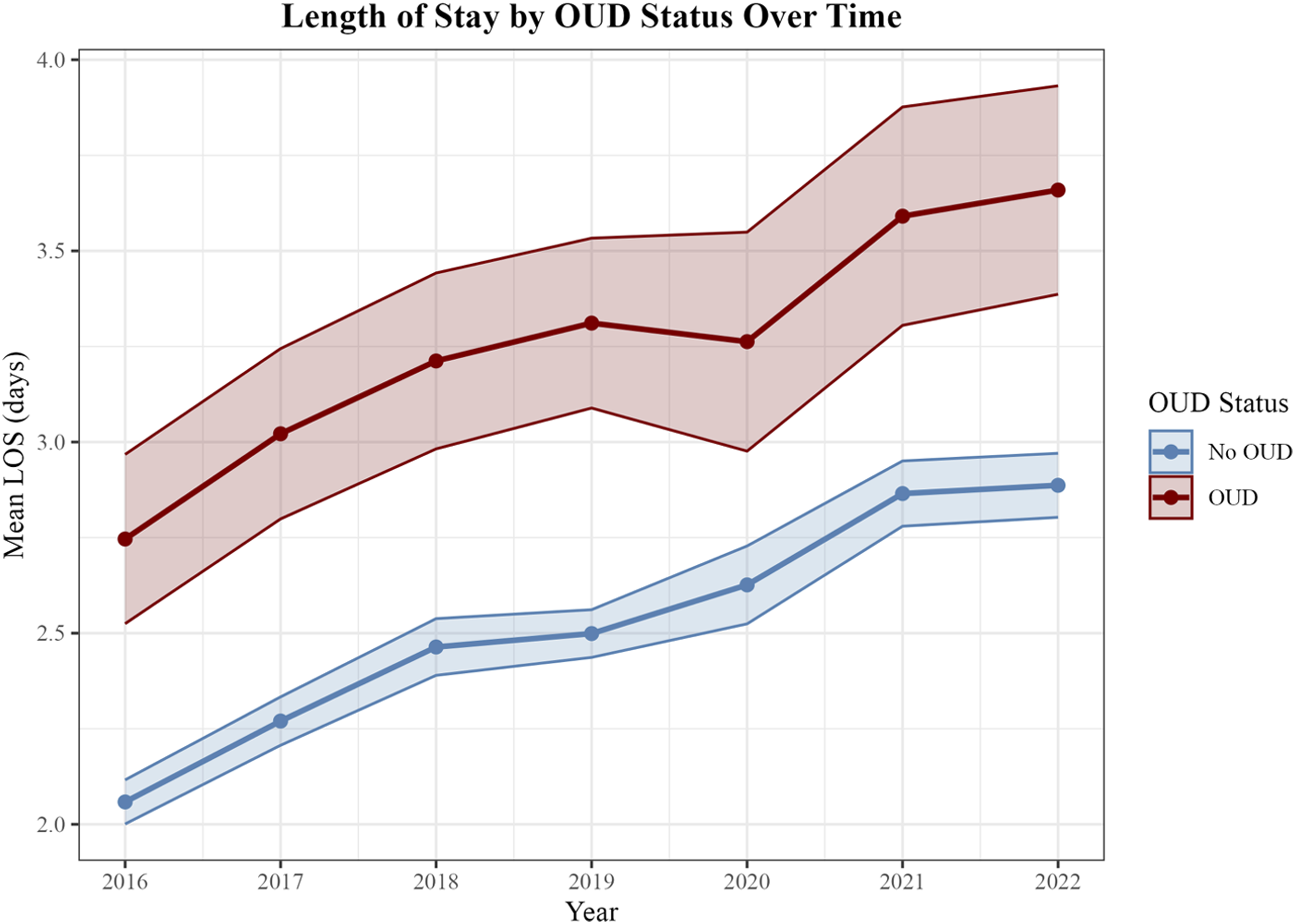
Perioperative Complications Associated With OUD
Adjusted Odds Ratios for Perioperative Complications Associated With OUD
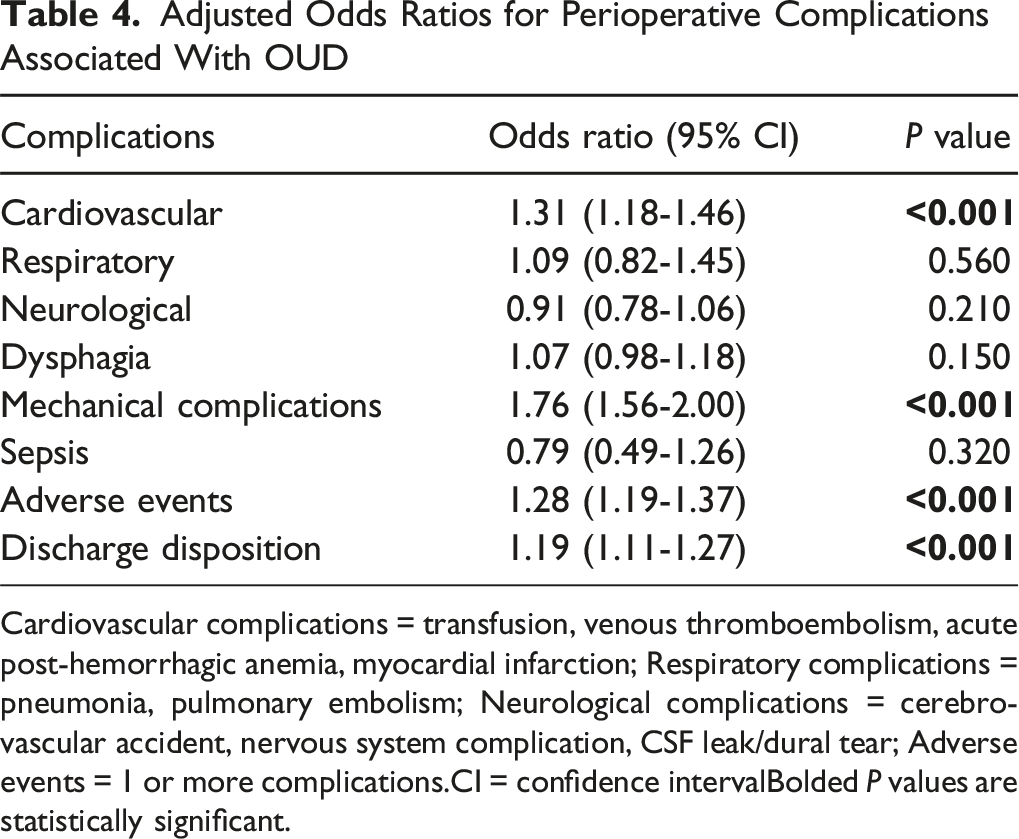
Cardiovascular complications = transfusion, venous thromboembolism, acute post-hemorrhagic anemia, myocardial infarction; Respiratory complications = pneumonia, pulmonary embolism; Neurological complications = cerebrovascular accident, nervous system complication, CSF leak/dural tear; Adverse events = 1 or more complications.CI = confidence intervalBolded P values are statistically significant.
Discussion
OUD remains a prevalent and consequential risk factor in modern cervical spine surgery. In this nationally representative cohort of inpatient cervical fusion hospitalizations from 2016 to 2022, OUD was common and clustered with higher clinical severity and multimorbidity. Patients with OUD were more frequently middle-aged, underwent more multilevel cervical fusion, and were treated disproportionately in regions outside the Northeast. They also experienced longer LOS, higher inflation-adjusted costs, and higher rates of select medical and mechanical complications and non-routine discharge.
We observed an early rise and sustained prevalence of OUD among cervical fusion inpatients across the study period, a pattern consistent with prior studies showing increasing opioid-related diagnoses among hospitalized patients with spinal conditions. 9 Regional concentration of OUD outside the Northeast aligns with geographic variation in perioperative opioid exposure and prolonged postoperative use, with elevated risk in the South and West. 10 Together, these trend and distributional signals suggest that prescribing culture, access to treatment, and regional practice patterns likely shape the OUD burden within cervical fusion inpatients, reinforcing the importance of routine psychosocial and substance-use screening and region-aware care planning.11,12
OUD was more likely among middle-aged patients, those with greater clinical severity, multilevel constructs, and co-occurring mental illness or substance use. This pattern aligns with a meta-analysis by Mohan et al, which found that preoperative opioid exposure, depression/anxiety, substance dependence, and female sex are among the strongest predictors of prolonged postoperative use after spine surgery. 13 One possible explanation is the presence of opioid tolerance or opioid-induced hyperalgesia among patients with greater opioid exposure, which may increase postoperative analgesic requirements without proportionally altering perceived functional improvement or PROM trajectories. In patients undergoing ACDF, opioid tolerance and longer preoperative exposure have been associated with higher risk of persistent use.14,15 Moreover, a substantial subset either remains or becomes newly opioid-dependent after surgery, with dependence associated with higher healthcare payments and increased readmissions.14,15 A prospective study by Uhrbrand et al aimed to identify why patients continue opioids after elective spine surgery, reporting that withdrawal symptoms were common and that non-surgical reasons often sustained use despite taper plans. 16 A multicenter registry analysis by Kim et al sought to determine predictors of long-term opioid use after elective cervical and lumbar procedures, reporting that preoperative opioid use and use at 90 days were the strongest predictors of 1-2-year dependence, and failure to achieve meaningful functional improvement further increased risk. These findings support front-end optimization, early addiction-medicine and behavioral-health involvement, clear expectation setting, and structured tapering, for patients who screen positive for psychosocial or substance-use risk.
Across years, OUD admissions stayed about 1 extra hospital day and incurred $4900 higher inflation-adjusted costs per admission, paralleling cervical-specific evidence that OUD in 1-2 level ACDF is associated with longer in-hospital stays, higher 90-day readmissions and complications, and greater episode-of-care costs. 17 Procedure intensity and complications appear to amplify downstream opioid exposure. This is also consistent with lumbar spine literature suggesting that fusion procedures, relative to lower-intensity decompression operations, are associated with greater postoperative opioid exposure, highlighting the likely contribution of procedural intensity to opioid-related risk across spine surgery. A prospective study by Rhon et al demonstrated that higher-intensity procedures like spinal fusion showed greater postoperative opioid fills, and after adjusting for complications, the odds of chronic use were significantly higher in the high-intensity group. 18 Discharge prescribing is a modifiable factor, whereby greater discharge morphine milligram equivalents (MMEs) are independently associated with preoperative opioid use, procedure type, and prescribing provider in patients undergoing ACDF and cervical disc arthroplasty (CDA), supporting protocolized targets. 19 Cervical-specific Enhanced Recovery After Surgery (ERAS) pathways that combine multimodal, opioid-sparing analgesia with standardized discharge prescribing and proactive follow-up are supported by contemporary reviews and clinical algorithms in spine surgery. 12 Other potentially modifiable perioperative factors, including body mass index and operative duration, may also influence postoperative analgesic requirements and represent important targets for future study in datasets with greater clinical granularity.
This study has several limitations. Diagnostic codes cannot distinguish active OUD from remission or delineate medication-assisted treatment, such as buprenorphine/methadone status, limiting exposure granularity. We lacked information on preoperative opioid dose/duration, implant choices, and surgeon or center experience, which may confound utilization and complications. Accordingly, we could not distinguish chronic preoperative opioid use by dosage or duration, including thresholds such as daily morphine milligram equivalents or opioid use extending beyond 3 months before surgery, and our findings should therefore be interpreted as pertaining to diagnosis-based OUD rather than prescription-defined opioid sensitization. In addition, the NIS does not provide granular perioperative variables such as body mass index or operative time, which may confound postoperative opioid-related outcomes but could not be accounted for in the present analysis. Because the NIS is hospitalization-based, we could not assess readmissions, long-term opioid persistence, or outpatient/short-stay pathways. Future work linking inpatient records to longitudinal pharmacy and outcomes data, and embedding perioperative OUD-tailored ERAS pathways, can clarify causality and identify the most effective, scalable interventions.
Conclusion
OUD remains prevalent among cervical fusion inpatients and predominantly affects those with higher clinical severity, greater multimorbidity, and patients undergoing multilevel fusion. From 2016 through 2022, OUD status was consistently linked to longer hospital stays, higher costs, and elevated odds of select medical and mechanical complications and non-routine discharge, underscoring measurable resource and safety impacts. These findings support targeted preoperative risk stratification and perioperative pathways tailored to OUD, whereby the integration of addiction medicine, behavioral health, and protocolized, opioid-sparing analgesia can be used to improve value and outcomes. Potential preoperative interventions include structured opioid tapering protocols when clinically appropriate, early involvement of multidisciplinary pain management teams, and individualized multimodal analgesia planning before surgery. Future work that links inpatient episodes to longitudinal pharmacy and outcomes data, and evaluates OUD-tailored ERAS pathways in trials, can clarify causality and identify scalable, high-value interventions.
Supplemental Material
Supplemental material - Opioid Use Disorder Among Cervical Fusion Inpatients: Trends, Complications, and Resource Use in a Retrospective National Inpatient Sample Analysis, 2016-2022
Supplemental material for Opioid Use Disorder Among Cervical Fusion Inpatients: Trends, Complications, and Resource Use in a Retrospective National Inpatient Sample Analysis, 2016-2022 by Mitchell K. Ng, MD, Leonidas E. Mastrokostas, BA, Paul G. Mastrokostas, BA, BBA, Anton J. Cristofoli, BS, Sean Inzerillo, BS, Gregorio Baek, BS, Khaled Elmenawi, MD, Ameen Barghi, MD, Abigail Razi, BS, Afshin E. Razi, MD, Daniel R. Fassett, MD, MBA, Nicholas U. Ahn, MD, Thomas D. Cha, MD, Jose A. Canseco, MD, Alan S. Hilibrand, MD, Alexander R. Vaccaro, MD, PhD, MBA, Christopher K. Kepler, MD, Gregory D. Schroeder, MD, Andrew P. Alvarez, MD in Global Spine Journal
Footnotes
ORCID iDs
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.