
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Mental health disorders like depression and psychoses are increasingly recognized in surgical populations and may adversely affect outcomes. This study aimed to: (1) evaluate the prevalence of these disorders among patients undergoing single-level lumbar fusion, (2) compare perioperative complications, costs, and discharge disposition; and (3) determine whether psychotic disorders confer greater risk than depression.
Methods
A retrospective study of the National Inpatient Sample (2016-2022) identified adults undergoing elective single-level lumbar fusion procedures. Patients were stratified into depression, psychoses, or control cohorts. Multivariable logistic regression was adjusted for demographic, hospital, and clinical covariates and used to assess associations with perioperative complications, non-home discharge, and inpatient mortality. Hospital costs were converted and inflation-adjusted to 2022 United States (U.S.) dollars.
Results
Among 792 065 weighted admissions, 17.7% had depression and 2.6% had psychotic disorders. Depression was independently associated with increased odds of cardiovascular complications (OR 1.26), mechanical complications (OR 1.25), adverse events (OR 1.26), and non-home discharge (OR 1.17, all P < .001). Psychotic disorders had greater risk, with higher odds of cardiovascular (OR 1.41), mechanical (OR 1.45), any adverse event (OR 1.42), and non-home discharge (OR 1.59; all P < .001). Mean costs ($41 097 vs $39 256 vs $38,117; P < .001) and length of stay (3.72 vs 3.51 vs 3.19 days; P < .001) were greatest in psychoses.
Conclusion
Depression and psychotic disorders are common in patients undergoing lumbar fusion, and are independently associated with increases in perioperative morbidity, non-home discharge, and costs. Tailored perioperative planning may help mitigate these risks.
Keywords
Introduction
Mental health disorders represent an important and underappreciated factor in surgical outcomes.1-3 Depression affects nearly one in five adults in the United States, while psychotic disorders have been associated with significant morbidity and overall increased health care utilization.4-6 Patients undergoing spine surgery often present with chronic pain and functional disability, further highlighting the intersection between mental illness and surgical recovery. 7 Psychiatric comorbidities have been shown to influence pain perception, adherence to postoperative regimens, and utilization of rehabilitation services, all of which may potentially affect perioperative morbidity and overall postoperative course.8-11
Prior studies in the orthopedic and neurosurgical literature have suggested that patients with depression experience higher complication rates, greater length of stay, and increased non-home discharge following elective procedures.2,7,8,12-14 However, current analyses have either combined psychiatric diagnoses into broad categories or examined depression in isolation,7,12,15 leaving the impact of severe conditions such as psychotic disorders relatively unexplored. This has contributed to a knowledge gap, as patients with psychotic disorders often have additional comorbidities, socioeconomic challenges, and experience barriers to coordinated perioperative care.14-16
National data related to lumbar fusion outcomes does not currently sub-stratify depression vs other psychotic disorders when classifying mental diagnoses. To this end, the purpose of this study was to: (1) evaluate the prevalence of depression and psychotic disorders among patients undergoing single-level lumbar fusion; (2) compare perioperative complications, costs, and discharge disposition; and (3) determine whether psychotic disorders result in greater perioperative risks and costs relative to depression. We hypothesized that depression and psychotic disorders would be associated with increased perioperative complications, longer length of stay, and overall higher healthcare utilization, with psychotic disorders imparting the greatest risk due to their increased severity.
Methods
Data Source
We conducted a retrospective observational study using the National Inpatient Sample (NIS) from 2016 to 2022, a 20% stratified sample of discharges from U.S. community hospitals that excludes rehabilitation and long-term acute care facilities.
Cohort Identification and Exclusion Criteria
Adults (≥18 years) who underwent single-level lumbar fusion were identified using ICD-10-PCS procedure codes capturing anterior lumbar interbody fusion (ALIF), posterolateral fusion (PLF), posterior/transforaminal lumbar interbody fusion (P/TLIF), and combination procedures (ALIF + PLF, P/TLIF + PLF). We excluded nonelective admissions; records with missing or implausible age, key hospital characteristics, payer, or cost data; procedures not performed on the admission day; and encounters with negative costs or lengths of stay.
Mental Health Exposure and Comorbidities
Mental health exposures were defined using Elixhauser indicators mapped from ICD-10-CM: depression and psychoses (Appendix 1). Patients were classified into mutually exclusive groups—Psychoses, Depression, or Control (neither condition). To avoid collinearity with the exposures, we calculated an Elixhauser Comorbidity Index (ECI) as the row-wise sum of Elixhauser comorbidities with depression and psychoses removed.
Outcomes
Perioperative complications were captured from ICD-10 diagnosis/procedure codes recorded during the index admission and summarized into grouped categories: cardiovascular, respiratory, neurological, and systemic (Appendix 2). We also assessed mechanical complications, inpatient mortality, and a composite adverse-event indicator flagging the presence of ≥1 complication. Discharge disposition was categorized as routine (home) vs non-routine (transfer to another facility, skilled nursing, intermediate care, or home health). Deaths were analyzed separately and were not excluded based on discharge code.
Cost Conversion and Inflation Adjustment
Total hospital charges were converted to costs using hospital- and year-specific cost-to-charge ratios (CCRs), such that each hospitalization’s total charges were multiplied by the corresponding CCR to approximate actual resource costs. These estimated costs were then adjusted to 2022 U.S. dollars using year-specific Consumer Price Index (CPI) inflation multipliers so that all values reflect constant 2022 purchasing power.
Survey Design and Statistical Analysis
All analyses incorporated the complex survey design of the NIS (stratification, clustering, discharge weights) to generate national estimates. Discharge weights were applied to each record, and survey procedures accounted for stratified sampling and hospital-level clustering when estimating standard errors and confidence intervals. We compared demographic, hospital, and clinical characteristics across mental-health groups using survey-weighted chi-square tests for categorical variables and survey-weighted linear models for continuous variables. Primary analyses used survey-weighted logistic regression to estimate associations for depression vs control and psychoses vs control with grouped complications (cardiovascular, respiratory, neurological, systemic), mechanical complications, any adverse event, non-routine discharge, and inpatient mortality. Models adjusted for age, sex, race, income quartile, primary payer, hospital region, hospital size, teaching status, procedure category (ALIF, PLF, P/TLIF, ALIF + PLF, P/TLIF + PLF), and ECI. As an exploratory analysis, we also compared psychoses vs depression for the same outcomes. Costs and length of stay were compared across groups using survey-weighted linear regression models with mental health group as the primary factor, providing global tests of between-group differences. Statistical significance was set at P < .05. Given eight prespecified outcome endpoints, multivariable models for complications, adverse events, discharge disposition, and inpatient mortality were additionally adjusted for multiple comparisons using a Bonferroni-corrected threshold of P < .006. Analyses were conducted in R (version 4.4.0; R Project for Statistical Computing, Vienna, Austria) using the survey package.
Results
Patient Demographics
Demographic Information for Patients Undergoing Single-Level Lumbar Fusion
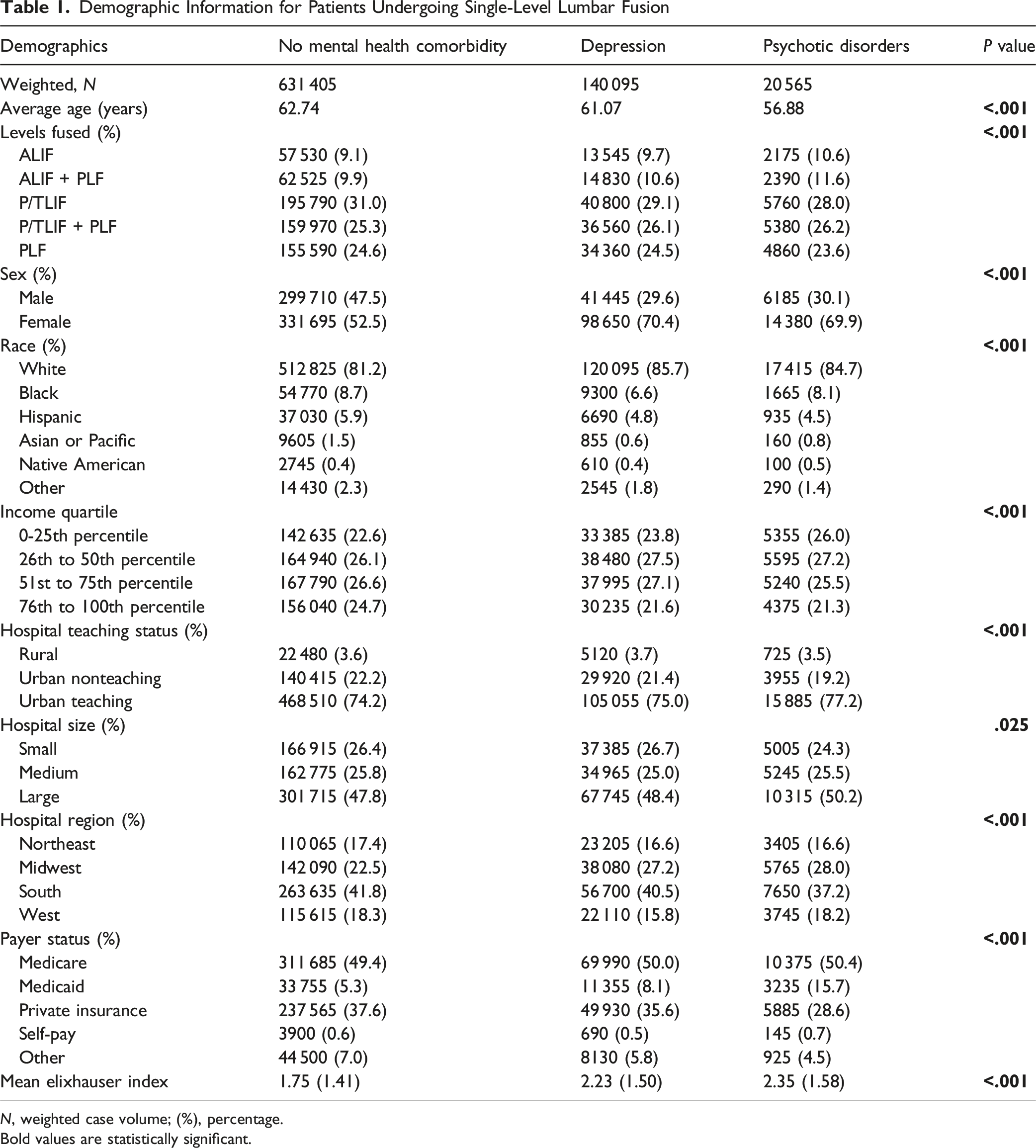
N, weighted case volume; (%), percentage.
Bold values are statistically significant.
Comorbidities
Prevalence of Comorbidities
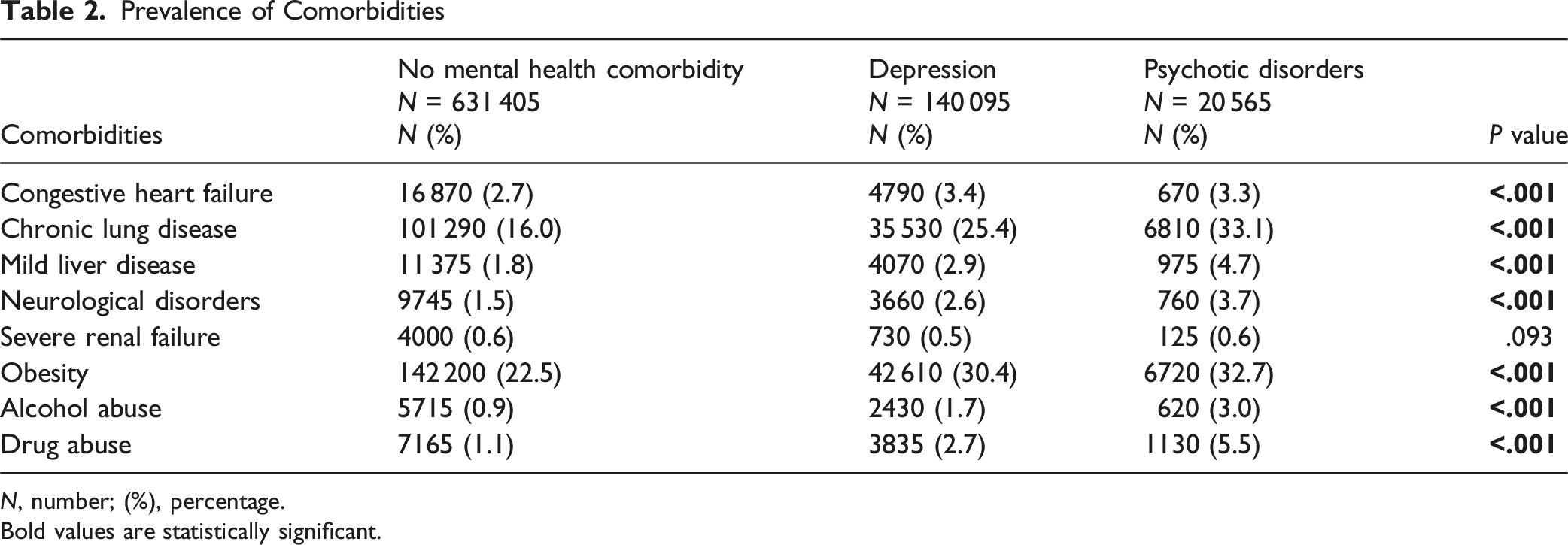
N, number; (%), percentage.
Bold values are statistically significant.
Inpatient Complications and Disposition
Complications in Patients Undergoing Single-Level Lumbar Fusion
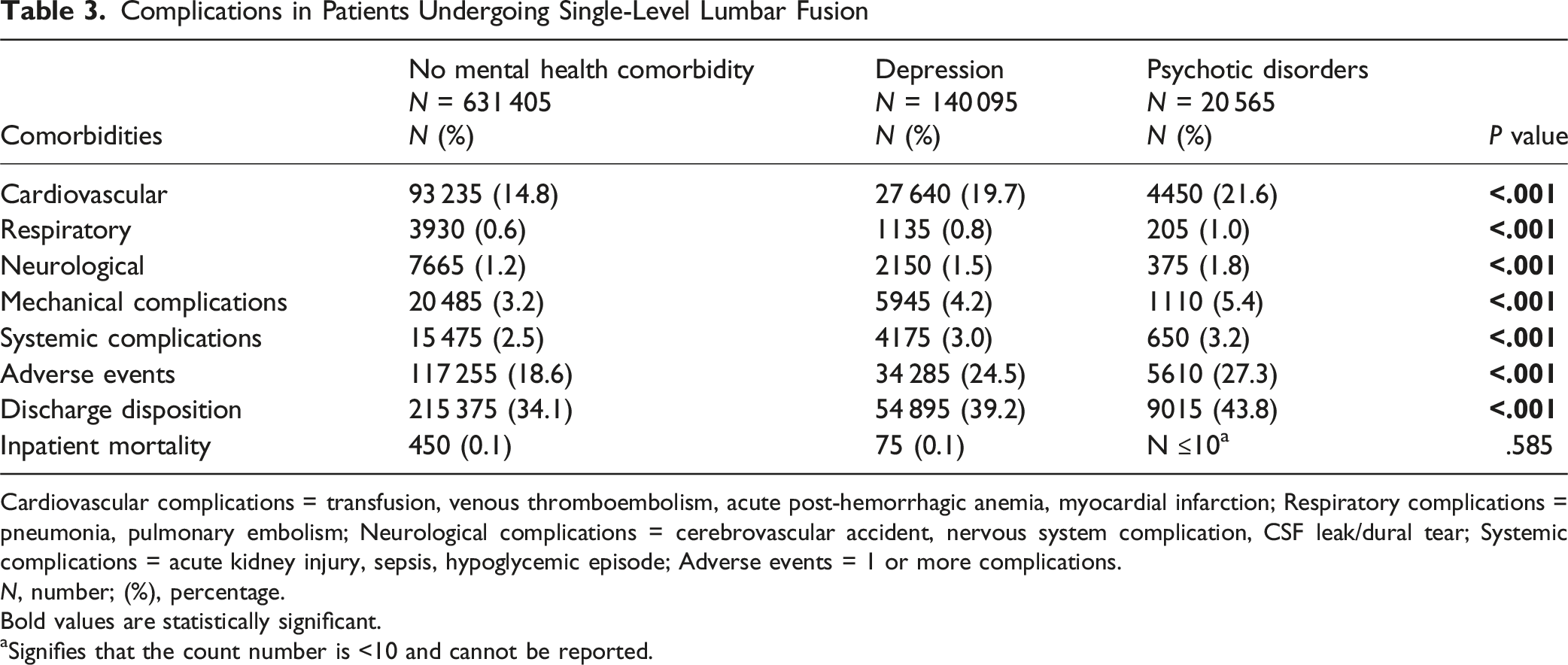
Cardiovascular complications = transfusion, venous thromboembolism, acute post-hemorrhagic anemia, myocardial infarction; Respiratory complications = pneumonia, pulmonary embolism; Neurological complications = cerebrovascular accident, nervous system complication, CSF leak/dural tear; Systemic complications = acute kidney injury, sepsis, hypoglycemic episode; Adverse events = 1 or more complications.
N, number; (%), percentage.
Bold values are statistically significant.
aSignifies that the count number is <10 and cannot be reported.
Multivariable Regression Analysis
Regression Modeling Predicting Influence of Mental Illness on Inpatient Complications
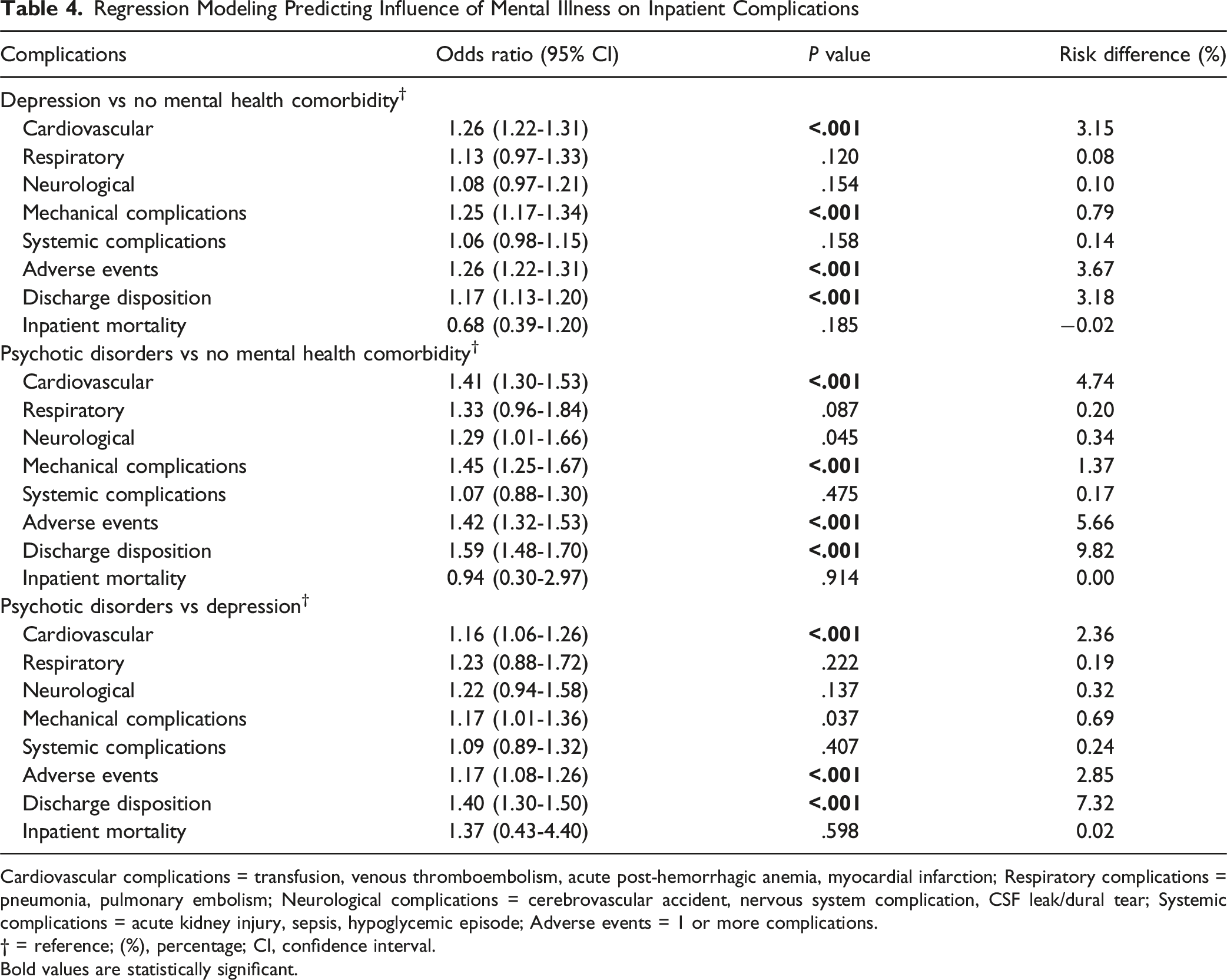
Cardiovascular complications = transfusion, venous thromboembolism, acute post-hemorrhagic anemia, myocardial infarction; Respiratory complications = pneumonia, pulmonary embolism; Neurological complications = cerebrovascular accident, nervous system complication, CSF leak/dural tear; Systemic complications = acute kidney injury, sepsis, hypoglycemic episode; Adverse events = 1 or more complications.
† = reference; (%), percentage; CI, confidence interval.
Bold values are statistically significant.
Costs and Length of Stay
Costs and Length of Stay for Patients Undergoing Single-Level Lumbar Fusion

N, Number; LOS, length of stay. Bolded signifies any value that reaches statistical significance.
Discussion
Our national database analysis of patients undergoing single-level lumbar fusion reveals that psychiatric comorbidities are prevalent with clinically significant effects in this surgical population. Overall, nearly one in five patients carried an underlying diagnosis of depression, while ∼3% had a psychotic disorder. Both conditions were independently associated with higher complication rates, longer hospitalization, greater costs, and increased likelihood of non-home discharge. Importantly, psychotic disorders conferred a substantially greater burden than depression across nearly all outcome measures.
The prevalence of depression in this study aligns with those of prior studies reporting that up to 15-30% of patients undergoing spine surgery meet diagnostic criteria for depression.2,4 One systematic review of 24 articles quantified overall prevalence of depression as 30.8% in patients undergoing operative management for degenerative spine disease. 4 To this end, our findings reinforce that psychiatric illness is not incidental, but rather represents an important feature of the lumbar fusion population. While psychotic disorders were less common in our cohort, they also presented as a sizeable subgroup. Of note, current literature rarely isolates psychosis in surgical cohorts, 17 often excluding such patients or collapsing them into broader psychiatric categories, which obscures their unique risk profile.2,7,8 By quantifying overall prevalence from a national database, our study highlights a growing need for identifying mental illness for patients in routine perioperative risk assessment and considering such patients for further perioperative optimization. In practical terms, this may include systematically screening for depression and psychotic disorders during preoperative evaluation, involving psychiatry or behavioral health teams when appropriate, anticipating higher rates of medical and mechanical complications in perioperative planning, and engaging case management early to coordinate post-acute care and discharge disposition.
As expected, depression and psychosis were both associated with higher rates of perioperative complications, adverse events, and non-routine discharge. To this end, our findings are consistent with prior reports linking depression to greater perioperative morbidity, worse functional recovery, and increased resource use.4,18-21 One study of the National Hospital Discharge Survey Database found that presence of a preoperative psychiatric disorder (depression, anxiety, schizophrenia, dementia) was associated with higher rates of nonroutine discharge and adverse events. 2 Another retrospective review of 8967 patients with schizophrenia undergoing surgery found they have significantly higher rates of postoperative complications (acute renal failure, pneumonia, bleeding, septicemia, stroke and 30-day mortality) relative to controls. 22 Another retrospective review of 435 patents undergoing cervical or lumbar surgery found that patients with preoperative mood disorders had worse Neck Disability Index (NDI) scores and received more opioid prescriptions as well. 23 Our study extends this evidence by demonstrating similar and, in the case of psychotic disorders, more pronounced effects. The observed stepwise increase in costs and length of stay across the three groups also has important implications for health systems, suggesting that psychiatric illness is associated with not only additional clinical, but also financial burden. Although the per-admission adjusted cost differences were modest (on the order of ∼$2000–$3000), they may be operationally meaningful when scaled across institutional and national lumbar fusion volumes. From a budgeting perspective, these incremental costs likely reflect higher resource utilization (such as longer length of stay, complication-related care, and greater post-acute discharge needs) and underscore the value of targeted perioperative planning and early discharge coordination in patients with psychiatric comorbidity. However, because costs and length of stay were compared using unadjusted survey-weighted tests, these differences may partially reflect variation in procedure mix and baseline clinical complexity across cohorts.
Direct comparison revealed that major psychotic disorders were associated with significantly greater odds of cardiovascular complications, as well as higher rates of adverse events and non-home discharge. These results support our hypothesis and reflect the distinctive challenges of managing patients with severe psychiatric illness. Potential mechanisms for these increased risks of perioperative complications include higher baseline medical comorbidity, reduced engagement with outpatient care, and difficulties with treatment adherence. Another NIS study of 647 951 patients undergoing lumbar fusion from 2016-2020 revealed that patients with depression, bipolar, or anxiety had higher rates of respiratory, urinary, fusion disorders, lengths of stay, and overall costs (P < .001 for all), although they grouped patients with depression and psychosis under one cohort. 11 Taken together, our findings suggest that it may be inappropriate to treat psychiatric diagnoses as a homogeneous risk group and highlight the importance of differentiating between specific mental illness disorders.
There are several potential limitations to this study. First, the use of administrative data introduces the potential for coding errors, and as with other studies does not allow assessment of severity of psychiatric disease, perioperative medication use, or longitudinal outcomes. Accordingly, we could not distinguish active vs historical diagnoses, evaluate symptom acuity or treatment status, or stratify outcomes by psychiatric severity; perioperative risk may therefore differ substantially in patients with more severe or untreated illness. In addition, our identification of depression and psychoses relied on ICD-10-CM diagnosis codes, which may misclassify historical, rule-out, or subclinical conditions as active psychiatric illness despite the use of validated Elixhauser definitions. It is important to note patients with active psychoses or non-optimized medical conditions are not surgical candidates and likely not represented in the study. In addition, even after multivariate analysis, it is possible that residual confounding related to patient socioeconomic status and psychosocial support still exist. Further, the NIS database captures only inpatient encounters, limiting analysis to short-term perioperative outcomes and excluding procedures performed in ambulatory settings. The absence of patient-reported outcome measures represents an important gap, as psychiatric illness may influence pain, function, and satisfaction in ways not captured by administrative codes. As a result, we could not evaluate longer-term, patient-centered recovery trajectories (such as disability improvement, return to baseline function, or sustained opioid use) that may differ by psychiatric comorbidity despite similar in-hospital outcomes. Nevertheless, our study’s use of a national dataset strengthens overall generalizability and highlights that early recognition and management of psychiatric illness may improve clinical outcomes in this vulnerable patient population.
Conclusion
Our study demonstrates that depression and psychotic disorders are common among patients undergoing single-level lumbar fusion. In addition, our results indicate that both depression and psychotic disorders are independently associated with increased postoperative morbidity, hospitalization, costs, and an overall greater likelihood of non-home discharge. As expected, psychotic disorders carried a greater burden of risk than depression, underscoring the importance of differentiating/stratifying between mental health disorder types. Overall, our findings further underscore a growing need for incorporation of mental health assessment into surgical planning and perioperative risk stratification.
Supplemental Material
Supplemental Material - Differential Impact of Depression and Psychotic Disorders on Complications, Costs, and Discharge After Single-Level Lumbar Fusion
Supplemental Material for Differential Impact of Depression and Psychotic Disorders on Complications, Costs, and Discharge After Single-Level Lumbar Fusion by Mitchell K. Ng, Leonidas E. Mastrokostas, Paul G. Mastrokostas, Gregorio Baek, Jonathan Dalton, Adam Fano, Alec Giakas, Rajendra Singh, Afshin E. Razi, Arya Varthi, Mark F. Kurd, Zachary Wilt, Daniel R. Fassett, Alan S. Hilibrand, Alexander R. Vaccaro, Gregory D. Schroeder, Christopher K. Kepler, and Andrew P. Alvarez in Global Spine Journal
Supplemental Material
Supplemental Material - Differential Impact of Depression and Psychotic Disorders on Complications, Costs, and Discharge After Single-Level Lumbar Fusion
Supplemental Material for Differential Impact of Depression and Psychotic Disorders on Complications, Costs, and Discharge After Single-Level Lumbar Fusion by Mitchell K. Ng, Leonidas E. Mastrokostas, Paul G. Mastrokostas, Gregorio Baek, Jonathan Dalton, Adam Fano, Alec Giakas, Rajendra Singh, Afshin E. Razi, Arya Varthi, Mark F. Kurd, Zachary Wilt, Daniel R. Fassett, Alan S. Hilibrand, Alexander R. Vaccaro, Gregory D. Schroeder, Christopher K. Kepler, and Andrew P. Alvarez in Global Spine Journal
Footnotes
ORCID iDs
Ethical Considerations
This is an IRB-approved retrospective study (approval #19D.508). All patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted without any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All data utilized in this study were sourced from institutional records.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mitchell K. Ng has the following disclosures: Stryker. Inc, Johnson & Johnson Ethicon Inc (paid consultant), CurvaFix Inc (paid consultant), Pacira BioSciences Inc (paid consultant), Sage Products Inc (paid consultant), Alafair Biosciences Inc (paid consultant), Next Science LLC (paid consultant), Bonutti Technologies Inc (paid consultant), Hippocrates Opportunities Fund LLC (paid consultant), and Ferghana Partners Inc (paid consultant). Arya Varthi has the following disclosures: DePuy Synthes Spine (Professional Activities). Alan S. Hilibrand has the following disclosures: CTL Amedica (IP royalties), North American Spine Society (board or committee member), Paradigm Spine (stock or stock options), and ZimVie (IP royalties). Alexander R. Vaccaro has the following disclosures: Accelus (other financial or material support; stock or stock options), Advanced Spinal Intellectual Properties (stock or stock options), AO Spine (other financial or material support), Atlas Spine (stock or stock options), Avaz Surgical (stock or stock options), AVKN Patient Driven Care (stock or stock options), Cytonics (stock or stock options), Deep Health (stock or stock options), Dimension Orthotics LLC (stock or stock options), Electrocore (stock or stock options), Elsevier (publishing royalties, financial or material support), Flagship Surgical (stock or stock options), FlowPharma (stock or stock options), Globus Medical (stock or stock options), Harvard Medtech (stock or stock options), Innovative Surgical Design (stock or stock options), Jaypee (publishing royalties, financial or material support), Jushi (Haywood) (stock or stock options), National Spine Health Foundation (board or committee member), Nuvasive (stock or stock options), Orthobullets (stock or stock options), Parvizi Surgical Innovation (stock or stock options), Progressive Spinal Technologies (stock or stock options), Rothman Institute and Related Properties (stock or stock options), Sentryx (other financial or material support; stock or stock options), Stout Medical (stock or stock options), Taylor Francis/Hodder and Stoughton (publishing royalties, financial or material support), Thieme (publishing royalties, financial or material support), and ViewFi Health (stock or stock options). Gregory D. Schroeder has the following disclosures: Advance Medical (paid consultant), Bioventus (paid consultant), Surgalign (paid consultant), AOSpine (board or committee member; other financial or material support), Cervical Spine Research Society (board or committee member), Cerapedics (research support), DePuy, A Johnson & Johnson Company (research support), Medtronic Sofamor Danek (research support), and Wolters Kluwer Health – Lippincott Williams & Wilkins (editorial or governing board). Christopher K. Kepler has the following disclosures: Clinical Spine Surgery (editorial or governing board), Curetiva (IP royalties), and Regeneration Technologies, Inc (IP royalties). All other authors have no other relevant financial disclosures. The author(s) declare that there is no conflict of interest and received no financial support for the research, authorship, and/or publication of this article. No IRB approval was required for performance of this review.
Data Availability Statement
All relevant data are included in the manuscript draft, tables, and figures. The raw data are available upon reasonable request from the corresponding author.
Drug Statement
The drug(s) mentioned in this study is FDA-approved or approved by corresponding national agency for this indication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.