
Abstract
Study Design:
Retrospective study.
Objective:
To determine whether opioid use disorder (OUD) patients undergoing 1- to 2-level anterior cervical discectomy and fusion (1-2ACDF) have higher rates of: 1) in-hospital lengths of stay (LOS); 2) readmissions; 3) complications; and 4) costs.
Methods:
OUD patients undergoing primary 1-2ACDF were identified within the Medicare database and matched to a control cohort in a 1:5 ratio by age, sex, and medical comorbidities. The query yielded 80,683 patients who underwent 1-2 ACDF with (n = 13,448) and without (n = 67,235) OUD. Outcomes analyzed included in-hospital LOS, 90-day readmission rates, 90-day medical complications, and costs. Multivariate logistic regression analyses were used to calculate odds-ratios (OR) for medical complications and readmissions. Welch’s t-test was used to test for significance for LOS and cost between the cohorts. An alpha value less than 0.002 was considered statistically significant.
Results:
OUD patients were found to have significantly longer in-hospital LOS compared to their counterparts (3.41 vs. 2.23-days, P < .0001), in addition to higher frequency and odds of requiring readmissions (21.62 vs. 11.57%; OR: 1.38, P < .0001). Study group patients were found to have higher frequency and odds of developing medical complications (0.88 vs. 0.19%, OR: 2.80, P < .0001) and incurred higher episode of care costs ($20,399.62 vs. $16,812.14, P < .0001).
Conclusion:
The study can help to push orthopaedic surgeons in better managing OUD patients pre-operatively in terms of safe discontinuation and education of opioid drugs and their effects on complications, leading to more satisfactory outcomes.
Introduction
In the United States, it is estimated that opioid use disorder (OUD) affects over 2.1 million Americans. 1 The Diagnostic and Statistical Manual of Mental Disorders (DSM-V), defines OUD as the following: A problematic pattern of opioid use leading to clinically significant impairment or distress, with at least 2 of the following observations made within a 12-month period, which may include taking opioids in larger amounts or over a longer period than was intended, a desire or unsuccessful effort to cut down or control use, craving, or a strong desire or urge to use opioids, or continued use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of opioids, among other criteria. 2 In addition to its high rate of overdose mortality, it is associated with well-known morbidities such as dependence, respiratory depression, and other adverse events. 3 These morbidities may pervade and complicate an OUD patient’s medical care, particularly when it comes to surgery. The complications associated with chronic opioid use and surgical outcomes have been well-documented in most surgical fields, particularly within the field of orthopedic surgery.4-11
Compared to their non-opioid using counterparts, OUD patients have been reported to have higher rates complications such as thromboembolic and infectious related complications. Vakharia et al, reported that OUD patients undergoing primary total knee arthroplasty resulted in higher rates of coagulation-related complications, leading to longer hospitalizations and increased morbidity. 10 These publications highlight the importance of identifying OUD patients who are at higher post-operative risk, as well as informing both the patient and doctor of the likelihood of specific complications. While literature has demonstrated how OUD effects post-operative outcomes in many orthopedic procedures, none have shown its effects on patients exclusively undergoing 1-to 2-level anterior cervical discectomy and fusion surgery (1-2ACDF). As the annual prevalence of cervical radiculopathy, a common indication for anterior cervical discectomy and fusion (ACDF), has increased in the United States, the number of patients seeking treatment, both operatively and non-operatively, has invariably increased. 12
Studies have reported that the prevalence of OUD to range from 20 to 55% in patients undergoing elective spine surgery, however these studies have focused exclusively in patients undergoing lumbar spine surgery. As such, a well-powered study investigating the association of OUD on outcomes following primary 1-2ACDF for cervical radiculopathy is warranted. Therefore, the aim of this retrospective study was to analyze a large comprehensive nationwide administrative claims database to determine whether OUD patients undergoing primary 1-2ACDF for cervical radiculopathy have higher rates of: 1) in-hospital lengths of stay (LOS); 2) readmission rates; 3) medical complications; and 4) healthcare costs.
Methods
Database
A study was performed looking at the Part A and Part B 100% Medicare Standard Analytical Files from January 1st, 2005 to March 31st, 2014 using the PearlDiver (PearlDiver Technologies, Fort Wayne, Indiana) supercomputer. PearlDiver is a commercially available database, which is compliant with the Health Information Portability and Affordability Act (HIPAA) and contains the records of over 100 million patients. The database provides information such as diagnoses, complications, procedures, LOS, charges, reimbursements, in addition to other metrics. Patients and complications were queried using International Classification of Disease, ninth revision (ICD-9) codes. Due to its comprehensive availability in research metrics, the database has been used extensively in spine-related research and other orthopedic subspecialties.13-16 Since the database provides deidentified information, the study was exempt from our institution’s Institutional Review Board (IRB) approvals.
Cohorts
The database was initially queried for all patients who underwent ACDF using ICD-9 procedural code 81.62. To ensure that these patients underwent 1-2ACDF, patients from this cohort were filtered using ICD-9 procedural code 81.62. OUD patients were identified using ICD-9 diagnostic codes 304.01, 304.02, 305.51, and 305.52. Patients who have cervical degenerative pathology were queried using ICD-9 diagnostic codes: 721.1, 722.71, 723.4, 721.0 722.0, 722.4, 722.91, and 723.0. These codes were utilized as they have been utilized in a previously published study. 17 The inclusion criteria for the study cohort consisted of patients undergoing primary 1-2ACDF for the treatment of cervical degenerative pathology with a concomitant diagnosis of OUD, whereas, patients without OUD served as the comparison cohort. Exclusions from the study included those patients with malignancy, paralysis, and trauma (Figure 1). To minimize any potential confounding, study group were randomly matched to cohorts in a 1:5 ratio by age, sex, and the following medical comorbidities—chronic obstructive pulmonary disease (COPD), diabetes mellitus, hyperlipidemia, hypertension, obesity—defined as a body mass index (BMI) greater than 30kg/m2, and tobacco use (Table 1). These comorbid conditions were chosen as they have been implicated as the most commonly encountered comorbidities by orthopaedists.18,19
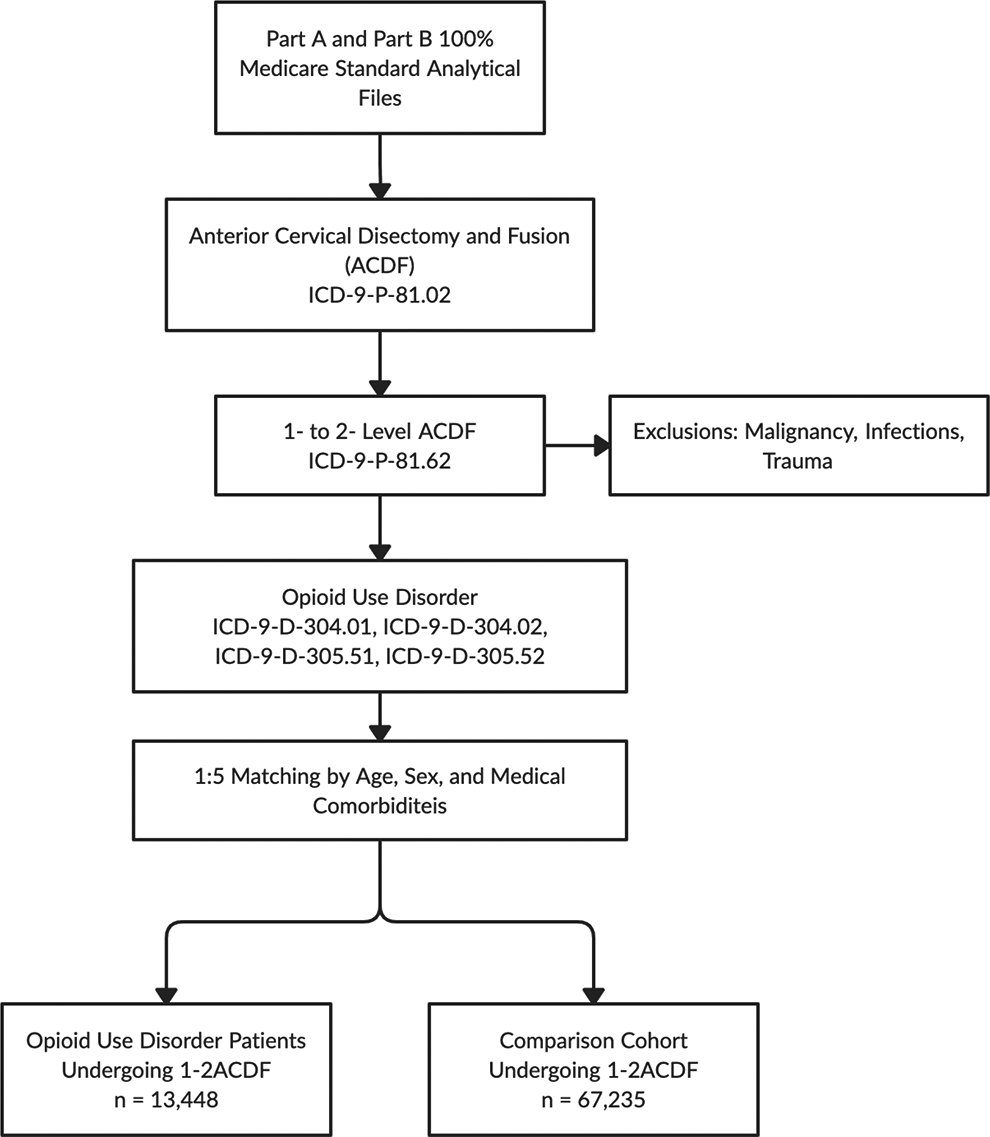
Flow diagram of cohorts.
Study Endpoints
Outcomes analyzed and compared included in-hospital LOS, 90-day readmission rates, 90-day medical complications, in addition to day of surgery and total global 90-day costs of care between the cohorts. Ninety-days was chosen to be compliant with the bundled payment care initiative (BPCI) set in place by the Centers for Medicare and Medicaid Services (CMS). 20
Medical complications assessed included: acute kidney injuries, cerebrovascular accidents, deep vein thromboses, ileus episodes, myocardial infarctions, pneumoniae, pulmonary emboli, respiratory failures, surgical site infections, urinary tract infections, transfusion of blood products, and venous thromboemboli. Costs of care were compared using reimbursement data, as it is a more accurate representation of what providers are paid from the insurance companies. Costs is aggregated from the PearlDiver platform to include all events following the time from the surgical procedure to the end point of the investigators interest and may include medication refills, office visits, additional diagnostic tests, as described in a previously published study. 21
Data Analysis
Descriptive and statistical analyses were performed with the programming language R (R Foundation for Computational Statistics, Vienna, Austria). Pearson’s chi-square analyses were used to compare patient demographics. It should be of note that while age is a continuous variable, the PearlDiver platform provides age as a categorical variable with 5-year age increments and was thus analyzed using the aforementioned method. For categorical variables with a sample size less than 11 patients, Fischer’s exact test was utilized. To determine the association of OUD on readmission rates and medical complications, a multivariate logistic regression analyses was utilized to calculate the odds-ratios (OR) and their respective 95% confidence intervals, adjusting for age, sex, geographic region, and Elixhauser-Comorbidity Index (ECI). Due to the number of medical complications being assessed, Bonferroni-adjusted corrections were performed to reduce the probability of a type I errors. 22 As a result, an alpha value less than 0.002 was considered statistically significant. This was attained by dividing 0.05 by the number of medical complications assessed (n = 19). Figures were produced using the “ggplot2” package of the R statistical software.
Results
In-Hospital LOS and Readmission Rates
OUD patients undergoing primary 1-2 ACDF were found to have significantly longer in-hospital LOS (3.41 vs. 2.23-days, P < .0001) compared to their counterparts. The data demonstrated in-hospital LOS for OUD users increased from 3.28-days to 3.69-days during the study interval. When comparing LOS between sex, male OUD patients were found to have longer in-hospital LOS compared to female OUD patients (3.68-days vs. 3.09-days). Additionally, OUD patients were found to have significantly higher frequency and odds of readmissions within the episode of care period following 1-2 ACDF (21.62 vs. 11.57%; OR: 1.38, 95%CI: 1.31 to 1.45, P < .0001) compared to the matched-control cohort.
Ninety-Day Medical Complications and Costs of Care
OUD patients were found to have greater incidences and ORs of total medical complications 90 days after 1-2ACDF compared to their comparison cohort (31.16% vs 8.47, OR: 2.25, 95%CI: 2.13 to 2.38, P < .0001) (Table 2). In addition to higher rates of ileus (0.88 vs. 0.19%; OR: 2.80, 95%CI: 2.15 to 3.65, P < .0001) which would be expected from the study cohort, OUD patients were found to have higher rates of thromboembolic complications, including pulmonary emboli (0.57% vs 0.20, OR: 1.80, 95%CI: 1.33 to 2.42, P < .0001), venous thromboemboli (1.23% vs 0.47, OR: 1.78, 95%CI: 1.46 to 2.18, P < .0001), and cerebrovascular accidents (2.22% vs 0.87, OR: 1.74, 95%CI: 1.49 to 2.01, P < .0001)(Table 2). In addition to thromboembolic complications, OUD patients were also found to have higher rates of myocardial infarctions (0.81% vs 0.29, OR: 1.68, 95%CI: 1.29 to 2.11, P < .0001) and infectious-related complications such as urinary tract infections (9.10% vs 2.88, OR: 2.17, 95%CI: 2.01 to 2.36, P < .0001), pneumoniae (5.30% vs 0.18, OR: 2.07, 95%CI: 1.86 to 2.29, P < .0001) and surgical site infections (1.96% vs 0.76, OR: 2.02, 95%CI: 1.72 to 2.36, P < .0001) when compared to the comparison cohort (Table 2).
Baseline Demographics of the Matched Study and Control Cohorts Undergoing 1- to 2-Level Anterior Cervical Discectomy and Fusion Within the Medicare Claims Database.
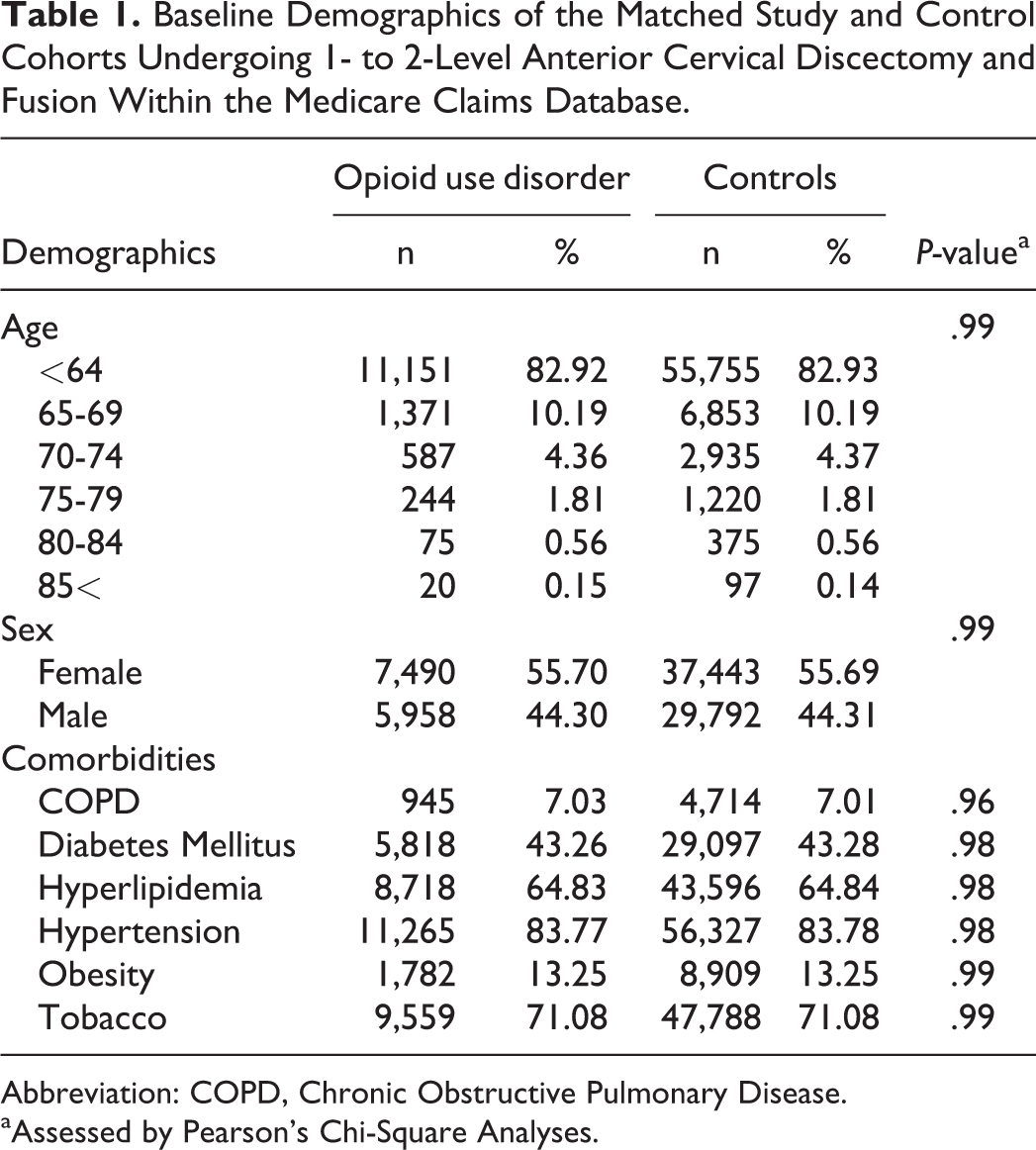
Abbreviation: COPD, Chronic Obstructive Pulmonary Disease.
aAssessed by Pearson’s Chi-Square Analyses.
Comparison of Frequency of 90-Day Medical Complications Among Opioid Use Disorder Patients and Controls Following Primary 1- to 2-Level Anterior Cervical Discectomy and Fusion.
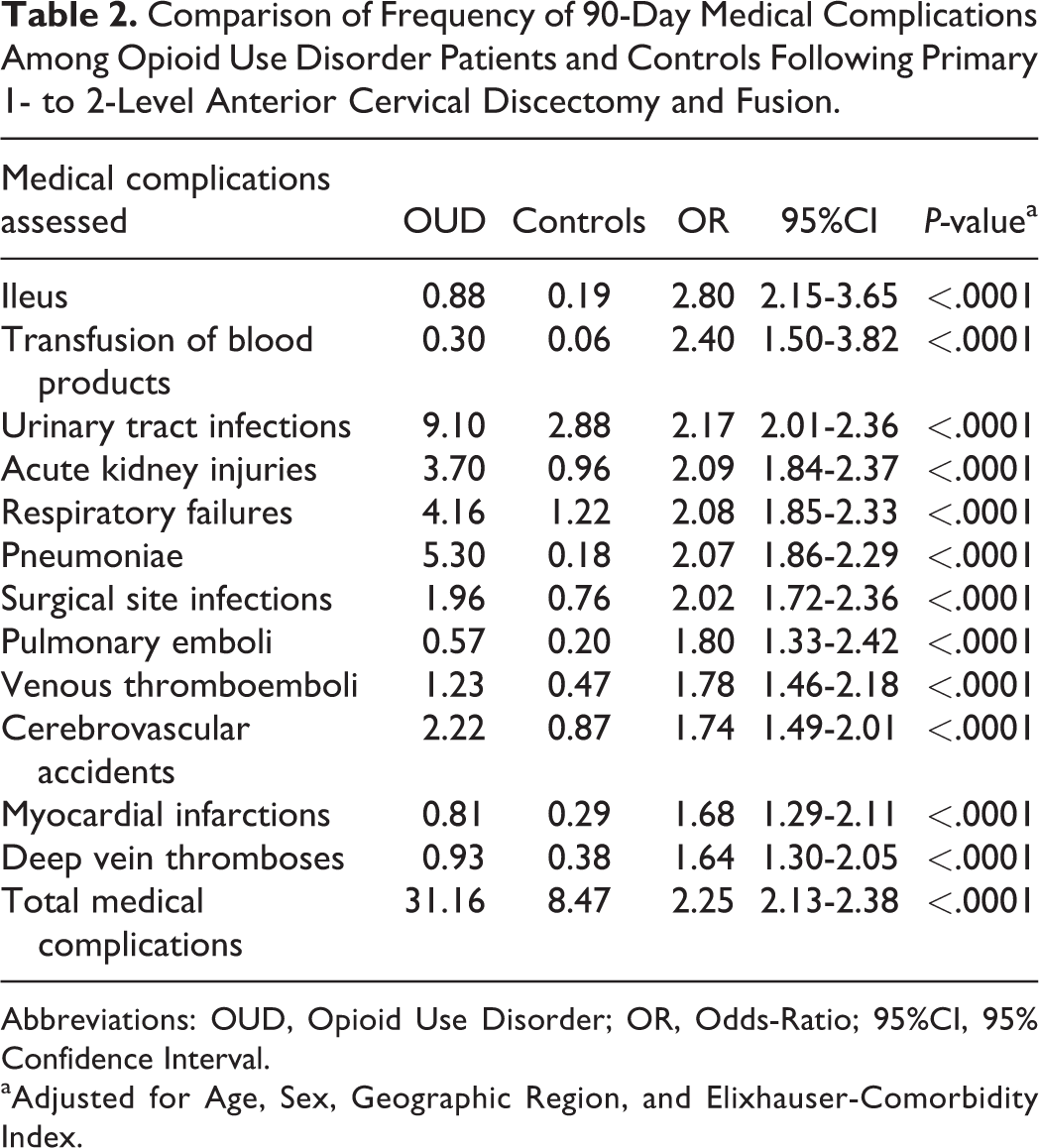
Abbreviations: OUD, Opioid Use Disorder; OR, Odds-Ratio; 95%CI, 95% Confidence Interval.
aAdjusted for Age, Sex, Geographic Region, and Elixhauser-Comorbidity Index.
Additionally, OUD patients had greater incidences and ORs of transfusion of blood products (0.30% vs 0.06, OR: 2.40, 95%CI 1.50 to 3.82, P < .0001), acute kidney injuries (3.70% vs 0.96, OR: 2.09, 95%CI: 1.84 to 2.37, P < .0001), and respiratory failures (4.16% vs 1.22, OR: 2.08, 95%CI: 1.85 to 2.33, P < .0001). Furthermore, OUD patients incurred significantly higher day of surgery ($15,634.05 vs. $13,858.47, P < .0001) and total global 90-day episode of care costs ($20,399.62 vs. $16,812.14, P < .0001)
Discussion
Opioids have historically been a go-to drug of orthopedics to manage their patients’ pain. 23 Despite its effectiveness at treating acute pain, the use of opioids has been questioned and greatly diminished on account of their addictive and harmful side-effects. 24 As a result, it is important to understand how OUD can create barriers to improvement on surgical outcomes in patients undergoing ACDF. Well-powered studies investigating the association of OUD on patients undergoing primary 1-2ACDF for cervical degenerative pathology with advanced statistical analyses are limited. The purpose of this study was to use a nationwide administrative claims database to determine whether OUD patients undergoing primary 1-2ACDF have higher rates of in-hospital LOS, readmission rates, complications, and overall healthcare expenditures. Adjusting for baseline covariates, this study demonstrates that OUD is associated with higher rates of LOS, readmissions, complications and costs of care following 1-2ACDF.
The results of this study coincide with the results of the other investigations. This study demonstrated that patients with OUD undergoing 1-2ACDF had significantly longer in-hospital LOS and 90-day readmission rates, which is consistent with results seen in published literature. Gupta et al, demonstrated that patients who had opioid abuse had increased LOS (10 vs 5 days; P < .0001) and greater 30-day readmission rates when compared to non-opioid abusing patients (OR: 1.72, P < .0001). 25 Utilizing the Truven Health MarketScan database, Weick et al used found patients undergoing primary TKA with a history of opioid abuse were found to have greater odds of 30-day readmissions compared to controls. 26 Jain et al, demonstrated chronic preoperative opioid use in posterior lumbar fusion patients was associated with greater rates of readmissions (OR 1.15, P = .02) compared to non-opioid users. 9 Unfortunately, limitations to the aforementioned studies included either assessing the association of OUD on other orthopedic subspecialties, limiting the follow-up period to only 30-days, nor investigating OUD within the setting of patients undergoing primary 1-2ACDF for cervical pathology. As such, the current investigation helps to enhance the current orthopedic spine literature. In addition to longer in-hospital LOS and readmission rates, the study found OUD to be associated with higher frequency and odds of developing medical complications.
In another retrospective study of a private claims database, Jain et al assessed the impact of chronic opioid use among 29,101 patients undergoing cervical fusion and demonstrated significantly higher rates of post-operative complications compared to their control cohort. 11 When looking at other orthopedic subspecialties, Sodhi et al showed OUD patients were found to have significantly higher rates of SSIs following primary total joint arthroplasty within their investigation. 27 The findings in this study also coincide with those by Vakharia et al who found OUD patients were found to have significantly higher rates of thromboembolic complications following primary TKAs. 10 Even in non-surgical settings, opioid use has been associated with a hypercoagulable state, resulting in various presentations of DVTs and PEs.28,29 However, a limitation to the aforementioned studies included either coalescing all cervical fusion procedures into a single study cohort, making it difficult to delineate the association of OUD in patients exclusively undergoing primary 1-2ACDF, utilizing only univariate analyses, or the results of the study were not generalizable to patients undergoing cervical spine surgeries. In Azdaki et al, opioid-addicted patients had higher blood levels of acute phase reactants (APRs) fibrinogen and CRP. 30 Since these APRs play various role in the coagulation cascade, it can serve as an explanation for the increased number of thromboembolic complications seen in OUD patients. Other studies have also demonstrated that long term use of opioids can hinder immune regulations increasing the susceptibility to develop infections—which could potentially explain the higher rates of infections seen within this investigation.3,31-33 Proper education about avoidable complications associated with opioid use can be employed to achieve more favorable post-operative outcomes.
In the context of ACDFs, adequately controlling pain remains one of a surgeon’s priorities. While no study has demonstrated how opioid use disorder may lead to post-operative complications following 1-to-2 level ACDFs, it is important to understand the risks associated with the procedure. As demonstrated by the current study, OUD patients were at greater odds of developing a variety of post-operative complications, notably ileus, thromboembolisms, and infections. These complications highlight the need for a multi-modality approach to addressing pre-and post-operative pain associated with orthopedic procedures, especially ACDFs. For example, using a combination of drugs that target nociceptive and neuropathic sources of pain simultaneously, such as acetaminophen, gabapentin, NSAIDs, steroids, and lidocaine in addition to opioids have shown to significantly decrease the need for post-operative opioids. In a review study by Li et al, it was demonstrated that a multimodal approach to pain that included COX-2 inhibitors and pregabalin pre-operatively, as well as nerve blocks and opioids peri and post-operatively, was just as effective, if not more effective than opioid use alone. 34 Proper preoperative management can also be effective in mitigating the need for opioids, thus decreasing the associated complications described in this paper. In Nguyen et al, by decreasing patient’s use of opioids before surgery, they were able to achieve markedly improved outcomes that were comparable to patients who had not used opioids at all. 35
Limitations
While a large sample size was used in this study’s analysis, there were limitations that should be considered. Principally, the study is a retrospective observational study, which means that it should be interpreted with the inherent limitations that come with these studies. In addition, the current investigation relies on accurate diagnostic and procedural coding in order to correctly categorize patients. However, it is estimated that the overall coding error rate within the Medicare claims database is around 1.3%. 36 Additionally, it is possible patients who had OUD were consuming other illicit drugs, which was not controlled for within this investigation and could potentially have skewed the results of the study. This study only analyzed a single insurance claims database, and the results of this study may not be a true accurate representation on the association of OUD and the dependent variables measured within this study. Furthermore, the current investigation was unable to stratify study group patients by the severity of opioids consumed by using morphine milligram equivalents, as patients who have more profound pain could potentially be consuming greater quantities of opioids compared to those with minimal pain and this could potentially skew the results of this investigation. Additionally, due to limitations of the PearlDiver database, we were unable to stratify the mode of opioid abuse, its duration, and whether certain pharmacological formulations of opioids to be associated with worse outcomes following 1-2ACDF; however, this can serve as the basis for future prospective studies. Despite these limitations, the study is the first, to the best of the author’s knowledge to determine the impact of OUD in a large sample of patients on various dependent variables in patients undergoing 1-2ACDF for cervical degenerative pathology.
Conclusion
It is the purpose of the study to demonstrate that patients with OUD are at increased risk for a wide range of complications after undergoing ACDF, such as gastrointestinal, thromboembolic, or infectious etiology. It can start with patient education, using a multimodal approach to addressing patients’ pain, and continued vigilance against opioid monotherapy, which may predispose a patient to OUD. However, understanding that OUD is associated with various postoperative complications only serves to increase the need to decrease the prevalence of opioid use to achieve better outcomes. As the complications described in this study all represent increased financial costs carried by both the patient and the hospital, it would also be in both parties’ interests to encourage decreased opioid use. Future studies can examine the potential cost-savings associated with mitigating pre-operative opioid use.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.