
Abstract
Study Design/Setting
Scoping review.
Objective
To map the landscape of endoscopic spine surgery research, identify areas of clinical application, and highlight evidence gaps to guide future studies.
Methods
Following PRISMA-ScR guidelines, systematic searches were performed across MEDLINE, EMBASE, CINAHL, and Cochrane Library (January 1, 2010–September 22, 2024). Eligible studies involved adults undergoing uniportal or biportal endoscopic spine surgery. Non-English studies, case reports (<5 patients), and abstracts were excluded. Two reviewers independently screened studies, with conflicts resolved by the senior author.
Results
A total of 1193 studies including 877 285 patients were identified, with publications increasing markedly over the past decade. Most studies were low-level evidence, primarily case series (49.3%) and retrospective cohorts (33.2%). Clinical effectiveness without comparison groups was common (35.3%). Lumbar disc herniation (47.3%) and uniportal endoscopy (83.9%) were the most studied pathology and technique, respectively. The transforaminal approach (50.4%) was more frequently evaluated than the interlaminar approach (30.0%). Outcomes often included pain scores (85.5%) and complication/readmission rates (79.5%). Few studies examined learning curve (0.8%), economic impact (0.7%), or neuromonitoring (0.5%). Research on enabling technologies such as navigation, robotics, and augmented reality accounted for 3% of studies.
Conclusions
The literature on spine endoscopy is expanding but remains dominated by low-level evidence focused on lumbar uniportal transforaminal approaches. High-quality studies are needed to advance the field.
Introduction
Endoscopic spine surgery has emerged as a novel minimally invasive spine surgery technique that allows surgeons to treat various spinal pathologies. 1 Spine endoscopy refers to spine procedures performed through small incisions using a camera, instruments, and constant irrigation. 1
Spine endoscopy has steadily advanced over the past few decades and is now used to treat a spectrum of spinal pathologies, including degenerative, traumatic, oncologic, and infectious conditions of the cervical, thoracic, and lumbar spine.2-4 Reported benefits of spine endoscopy compared to conventional open surgery include less soft tissue trauma, less blood loss, decreased infection rates, earlier rehabilitation, shorter hospital stays, and better functional outcomes.5,6 Disadvantages of spine endoscopy may include a steep learning curve, high costs, and radiation exposure.5,6
Spine endoscopy is performed either through uniportal or biportal access. Uniportal endoscopy uses a single incision through which both the endoscope and instruments are inserted, while biportal endoscopy uses two separate incisions, one for visualization and one more for working instruments.7,8 The smaller working space in uniportal endoscopy results in a steeper learning curve, while biportal endoscopy offers a wider surgical field and greater maneuverability. 7 Despite these differences, long-term clinical outcomes, complication rates, and recovery metrics are generally comparable between the two techniques. 9
With the growing interest in endoscopic spine surgery, there is a rapidly expanding but seemingly fragmented body of literature. This makes it challenging for clinicians and researchers to clearly grasp current evidence, trends, and knowledge gaps. Major themes in endoscopic spine research range from clinical effectiveness studies, 10 comparative studies with conventional surgical methods,11-13 patient recovery trajectories after surgery, 14 surgical technique and approaches, 15 learning curve, 16 to anesthetic considerations.17,18 In this study, we performed a scoping review to systematically map available studies, establish temporal trends in endoscopic spine surgery advancement, and identify under-explored domains for research in endoscopic spine surgery.
Methods
This review was reported according to the PRISMA for Scoping Review (PRISMA-ScR) guidelines. Patients and the public were not involved in the development of the systematic review. 19
Eligibility Criteria
We included endoscopic spine surgery studies that involved adult human subjects (age >18 years). We excluded systematic reviews, meta-analyses, case reports (<5 patients), conference abstracts, study protocols, letters to the editor, and technique guides. We also excluded studies using endoscopy as an adjunct to open or minimally invasive surgery (e.g., microendoscopic techniques), transoral or endonasal approaches for occipitocervical pathologies, non-decompressive indications (e.g., lumbar rhizotomies), and endoscopic-mediated thoracoscopic or laparoscopic techniques.
Identification of Studies
In consultation with a research librarian, a comprehensive search was conducted in MEDLINE, EMBASE, CINAHL, and the Cochrane Library databases to identify studies published from January 1st, 2010, to September 22, 2024. We limited our search from January 2010 onwards to capture the contemporary evidence reflecting current surgical techniques, technological advancements, and clinical practices in endoscopic spine surgeries. We used filters to exclude non-English studies. The search strategy combined MeSH terms “spine” and “endoscopy” with free-text keywords to comprehensively capture relevant literature. Spine-related free-text terms included “spin* surgery” or “spine” or “spinal”. For endoscopy, free-text terms included “ultra-minimally invasive,” or “ultra-MIS,” or “uniportal,” or “biportal,” or “endoscop*” or “microendoscop*”. The search was adapted to the syntax and indexing of each database to maximize both sensitivity and specificity. Boolean operators combined spine-related terms with endoscopy-related terms in each database, and the final results were limited to human studies published in English. The grey literature was not searched. The full search strategy for each database can be found in Appendix A (Online Supplemental Material).
Screening and Data Extraction
Two reviewers (DM, CYK) performed duplicate screening of all titles and abstracts for eligibility using a web-based screening platform for conducting systematic reviews (Covidence, Melbourne, Australia). Approved titles and abstracts were assessed in full-text review, and the accepted full-text studies were analyzed and data was extracted by two reviewers (DM, CYK). All discrepancies were resolved through consensus with the senior author (MY) at each stage. Cohen’s Kappa inter-rater coefficient was calculated for abstract and full-text stages using Covidence. 20
Study information extracted included publication year, journal, country, funding source, main theme, study design, and level of evidence. 21 Reported population characteristics included sample size of each study, sex distribution of study participants and mean patient age. Surgical data extracted included endoscopic technique (uniportal vs biportal), endoscopic method (transforaminal vs interlaminar), use of enabling technology, anatomical location of surgery (cervical, thoracic, or lumbar), mean number of surgical levels treated, pathology of interest, procedure (decompression vs fusion), and case status (elective vs emergent). Additionally, our study documented whether individual studies included the following reported outcomes: radiographic and physical exam findings, laboratory markers, intraoperative variables (i.e., blood loss, duration), length of stay (LOS), complications, reoperations, pain scores, generic and spine-specific patient reported outcome measures (PROMs), satisfaction, learning curve and costs. The timing of the first and last post-operative patient reported outcome evaluation were also collected.
Study Designs and Levels of Evidence
Two reviewers (DM, CYK) independently determined the study design. Randomized controlled trials were further reviewed by two reviewers (DM, CV) to assess the level of evidence, and discrepancies were resolved by the senior author (MY). While formal risk of bias assessment was outside the scope of this review, we determined the level of evidence according to the Oxford Centre for Evidence-Based Medicine guidelines.20,21 High-quality randomized control trials (RCTs) were considered Level I, lesser quality RCTs and high-quality prospective cohort studies were classified as Level II, lesser quality prospective cohort studies, retrospective cohort studies, and case-controlled studies were classified as Level III, while uncontrolled studies and those without comparator groups were classified as Level IV.
Literature Themes
The two reviewers (DM, CYK) generated a list of primary study themes after completing title and abstract screening. A sample of 50 included studies were used to pilot these themes for face validity and content validity. These themes were applied in the data-extraction stage for each study.
Statistical Analysis
Data analyses were performed using R. 22 Descriptive statistics were used to summarize categorical variables, reported as counts (percent), with denominators based on the total number of included articles or the number of articles reporting data on the variable of interest. The mean number of participants was weighted according to the sample size of each study, and standard deviations were pooled accordingly. Surgical technique variables were stratified by year of publication to assess potential trends and changes in practice over time.
Results
Literature Search and Study Characteristics
Our search yielded 8504 titles, from which duplicates were removed, resulting in 5374 unique titles and abstracts for screening. Following abstract screening, 1563 studies were included in full-text review, and 1193 were included in final data extraction (Figure 1). Cohen’s Kappa coefficient for inter-observer reliability for title and abstract, and full-text review was 0.84 and 0.75, respectively. PRISMA flowchart
Of the 1193 studies, sample size data was available for 1190 (99.7%). These studies represented 877 285 patients with publication dates ranging from 2010 to 2024. There was a marked increase in publications from 2016, peaking in 2023 (Figure 2). The mean and median sample size were 737 (standard deviation (SD): 16 148.0) and 60 (inter-quartile range (IQR): 29-106), respectively. These sample size results were heavily skewed by one study with a sample size of 549 531 patients.
23
Sex was reported in 1137 studies (95.3%) and females comprised 371 837 patients (42.4%). Mean age and SD were extractable from 309 studies (25.9%), covering a sample size of 681 888 (77.7%). The weighted mean age was 50.9 years (SD 15.6 years). Trends in reports of uniportal, biportal or both techniques reported in the spine literature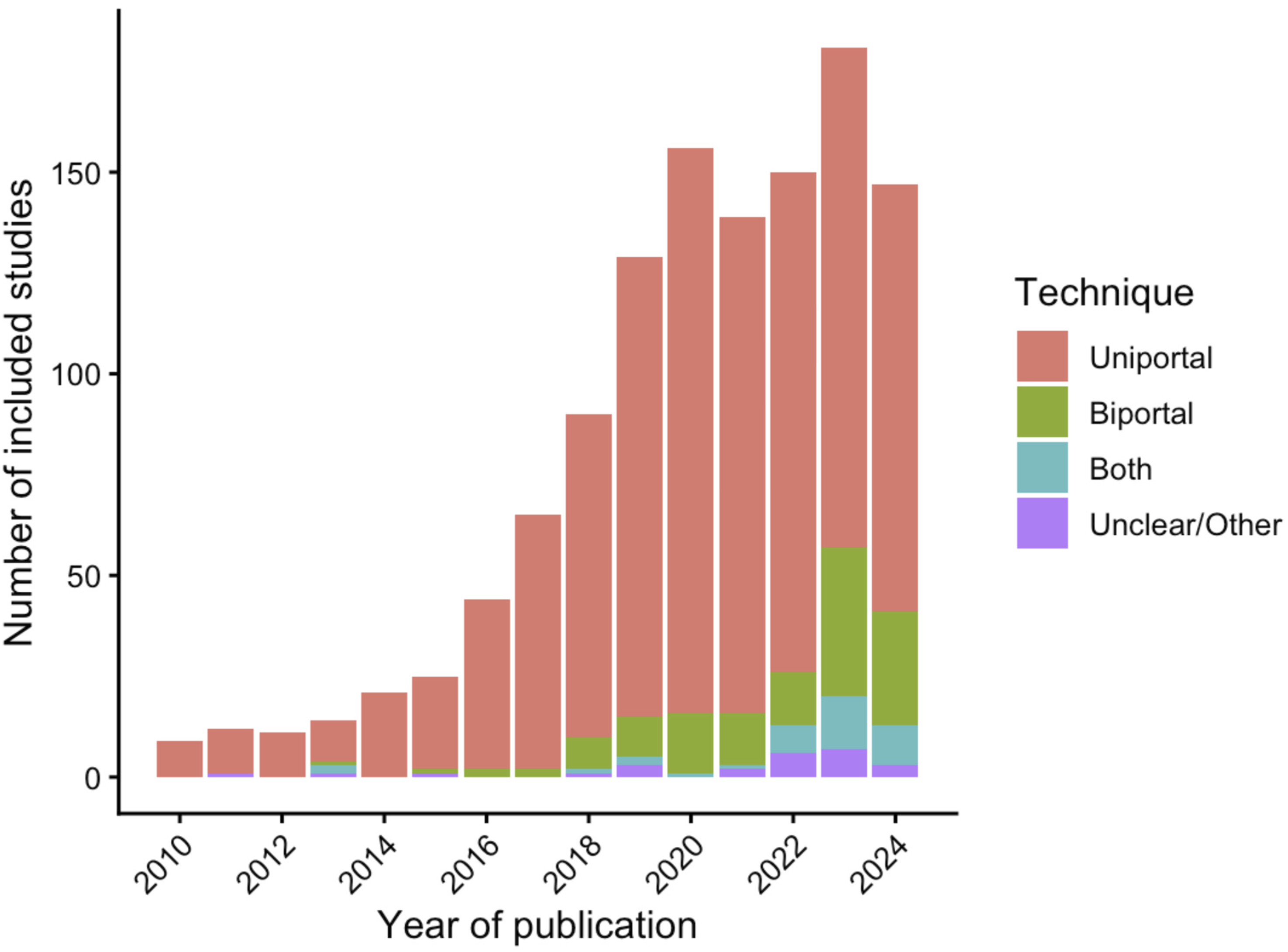
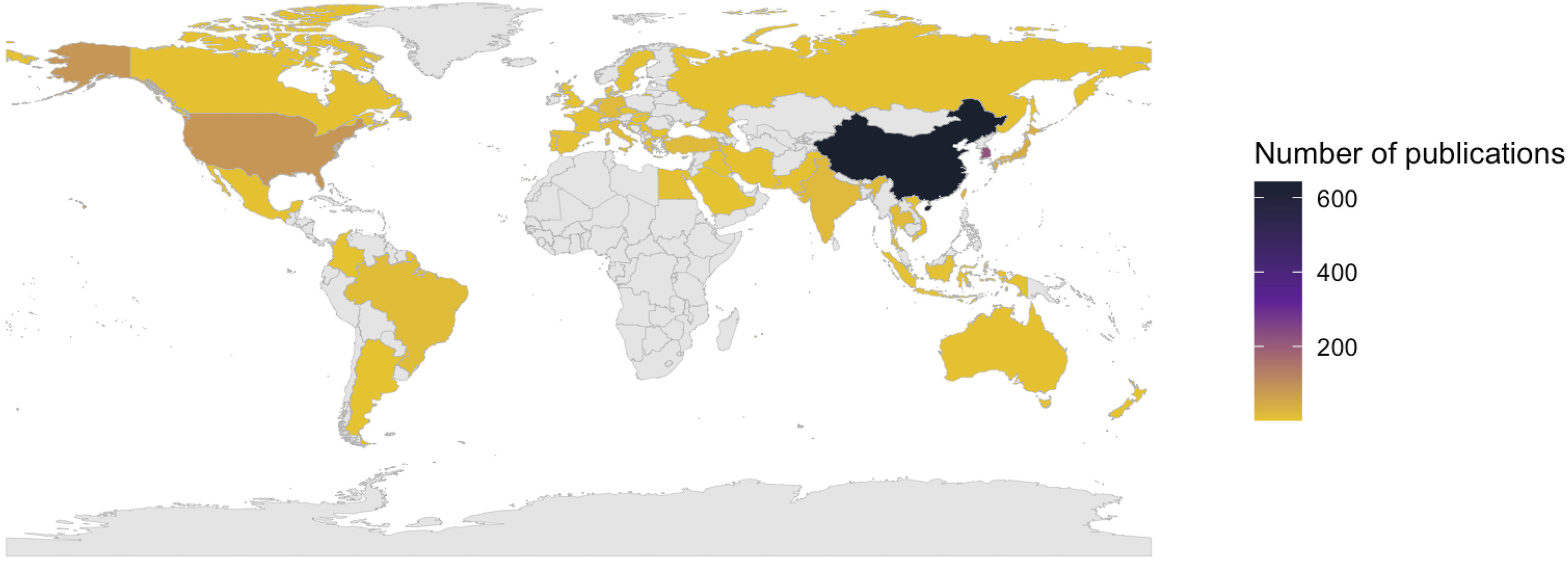
The top journals for endoscopic spine surgery publications were World Neurosurgery (n = 170, 14.2%), Pain Physician (n = 78, 6.5%), Orthopaedic Surgery (n = 57, 4.8%), European Spine Journal (n = 51, 4.3%), BMC Musculoskeletal Disorders (n = 51, 4.3%), and Journal of Orthopaedic Surgery and Research (n = 45, 3.8%) (full list in online Supplemental Material etable 1). The ten most popular journals for publication are illustrated in Figure 3. Authors contributing to these publications originated from forty different countries, with most originating from China (n = 641, 53.6%), South Korea (n = 218, 18.2%), followed by the United States (n = 87, 7.3%), Japan (n = 42, 3.5%) and Taiwan (n = 31, 2.6%) (Figure 4). Few studies were industry sponsored (n = 13, 1.1% of all included studies). Most popular journals for publication Global map demonstrating the amount of endoscopic research by country. Darker colors indicate larger publication volumes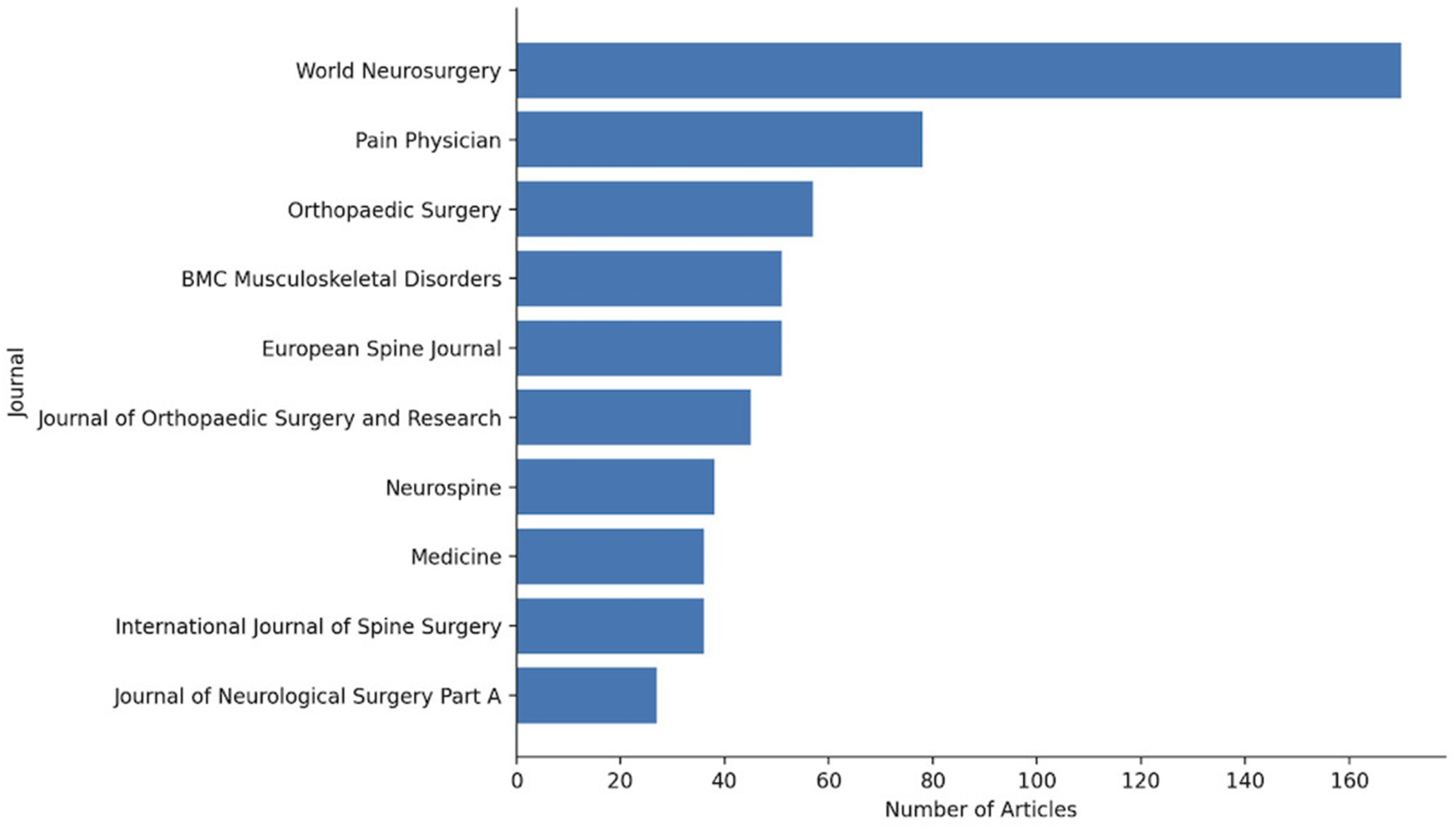
Study Design and Literature Themes
Summary of Level I Studies in Endoscopic Spine Surgery

The most commonly explored primary themes in the endoscopic spine surgery literature were clinical effectiveness studies without a comparator arm (n = 422, 35.3%), technical note of the surgical technique and approaches used (n = 291, 24.4%), and comparative studies assessing the clinical effectiveness of endoscopic spine technique against another surgical method (n = 222, 18.6%). There were relatively few studies evaluating anesthesia considerations (n = 85, 7.1%), learning curve (n = 10, 0.8%), health economics (n = 8, 0.7%), and neuromonitoring requirements (n = 6, 0.5%) for endoscopic spine surgery. These themes are summarized in Figure 5. Primary themes explored in the endoscopic spine literature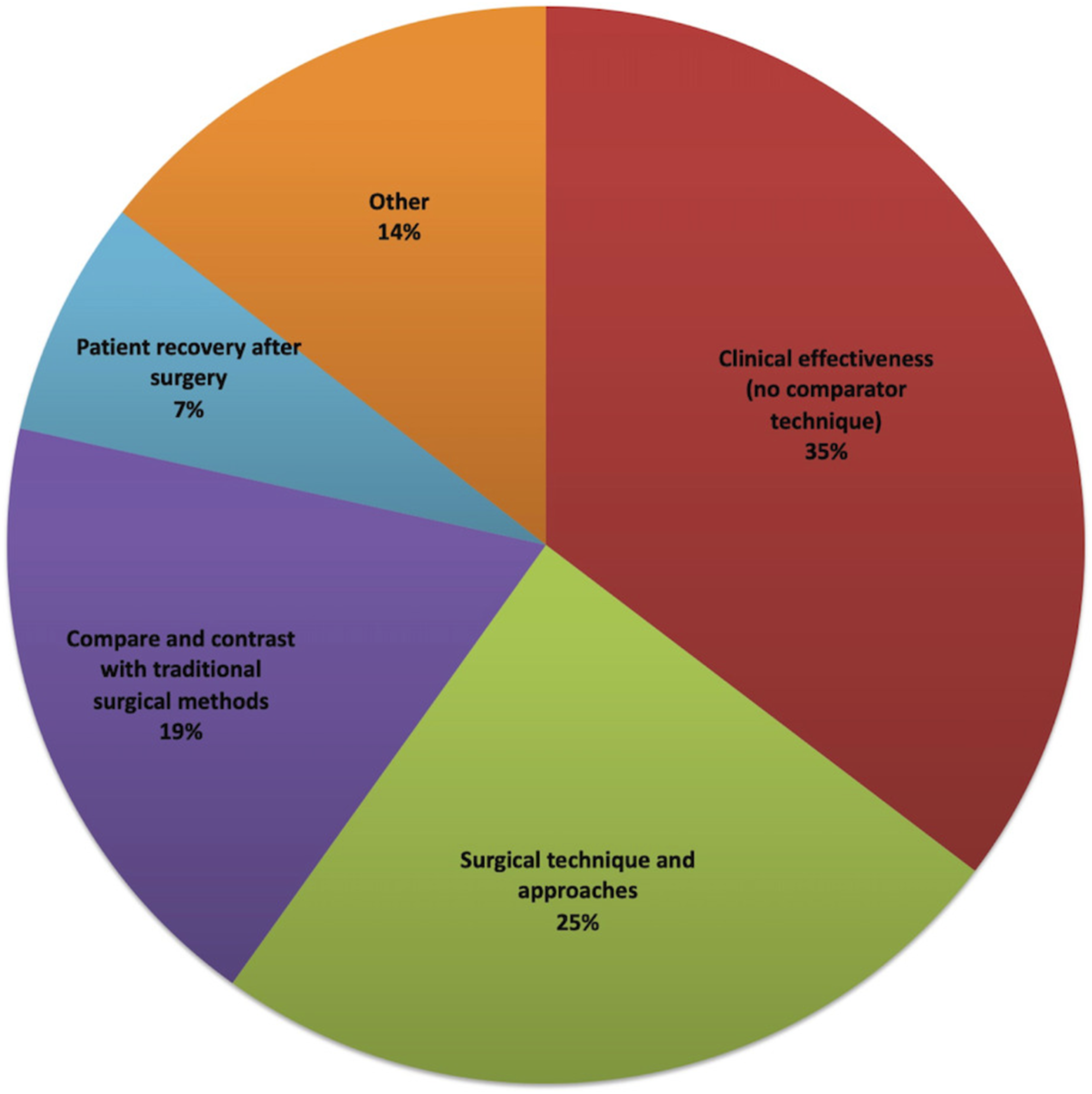
Technique Characteristics
Uniportal and biportal endoscopy represented 83.9% (n = 1001) and 10.9% (n = 130) of included studies, respectively. Biportal endoscopy studies began to appear in the literature in 2013 and rose substantially starting in 2018 (Figure 2). Studies that described both uni- and biportal endoscopy began to appear more substantially in 2022. The transforaminal approach was the most frequently described (n = 601, 50.4%), followed by the interlaminar (n = 358, 30.0%) approach. A smaller number of studies reported using both approaches
The use of enabling technologies was described in 36 studies (3.0%). The most commonly reported enabling technologies were 2D navigation (n = 16, 44.4%), 3D navigation (n = 11, 30.6%), both 2D and 3D navigation (n = 1, 2.8%), robotic assistance (n = 6, 16.7%), and augmented reality (n = 2, 5.6%). The use of enabling technologies has been increasingly described in the literature since 2019, with 2D navigation first being reported in 2012 (Figure 6). Trends in the use of reported enabling technologies in the endoscopic spine literature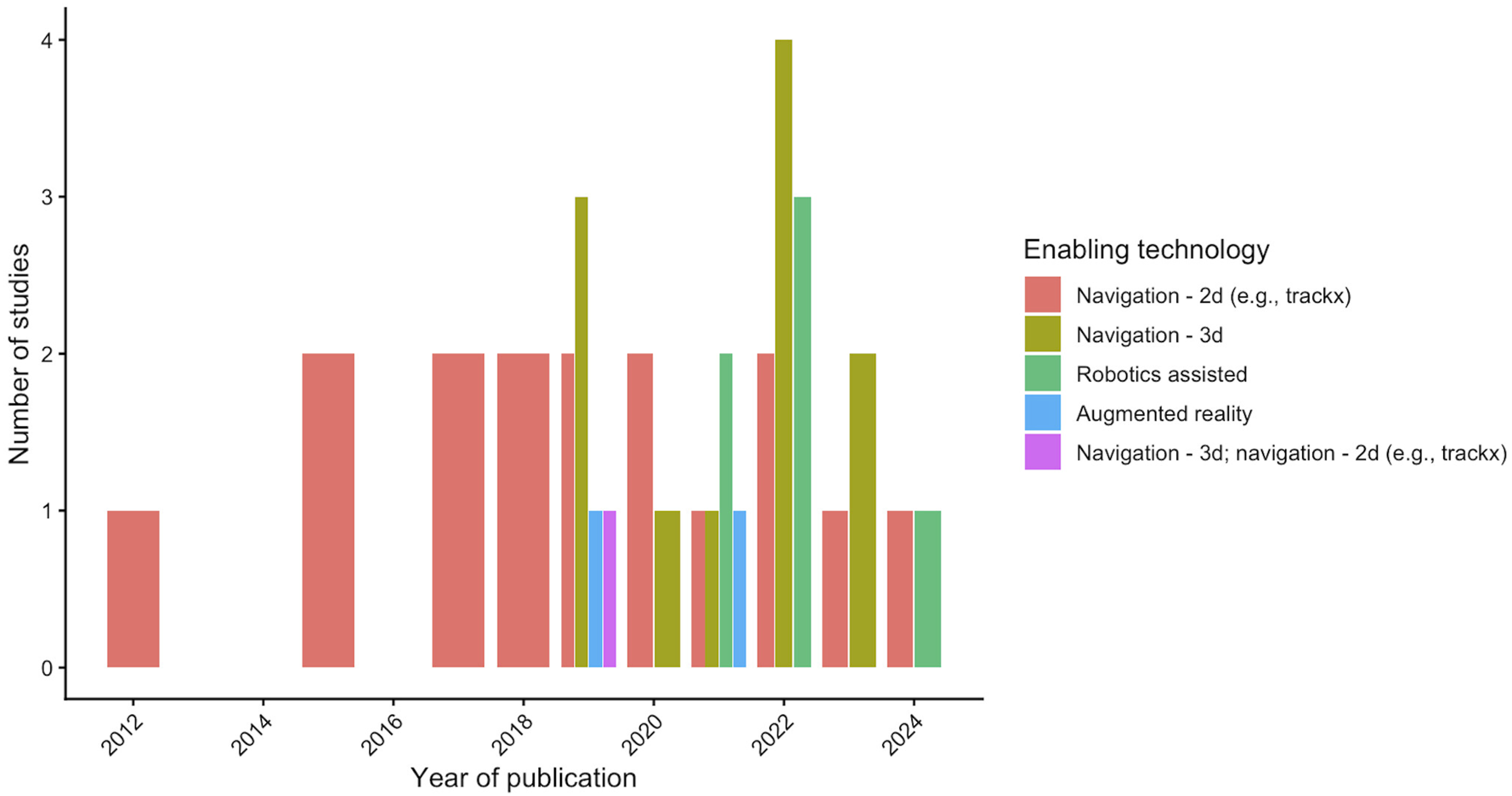
Surgery was most commonly performed in the lumbar spine (n = 1,047, 87.8%) followed by cervical (n = 88, 7.4%) and thoracic spine (n = 32, 2.7%). The location of surgery was multiple or mixed in 21 studies (1.8%) and unspecified in 5 (0.4%). Of the cases reporting endoscopic spine surgery on the thoracic spine, 14 were performed to address thoracic disc pathology (43.8%). A posterior or posterolateral approach was used in the majority of cases (n = 1,160, 97.2%), with few utilizing anterior (n = 18, 1.5%), lateral (n = 3, 0.3%) or mixed approaches Most commonly reported pathologies of interest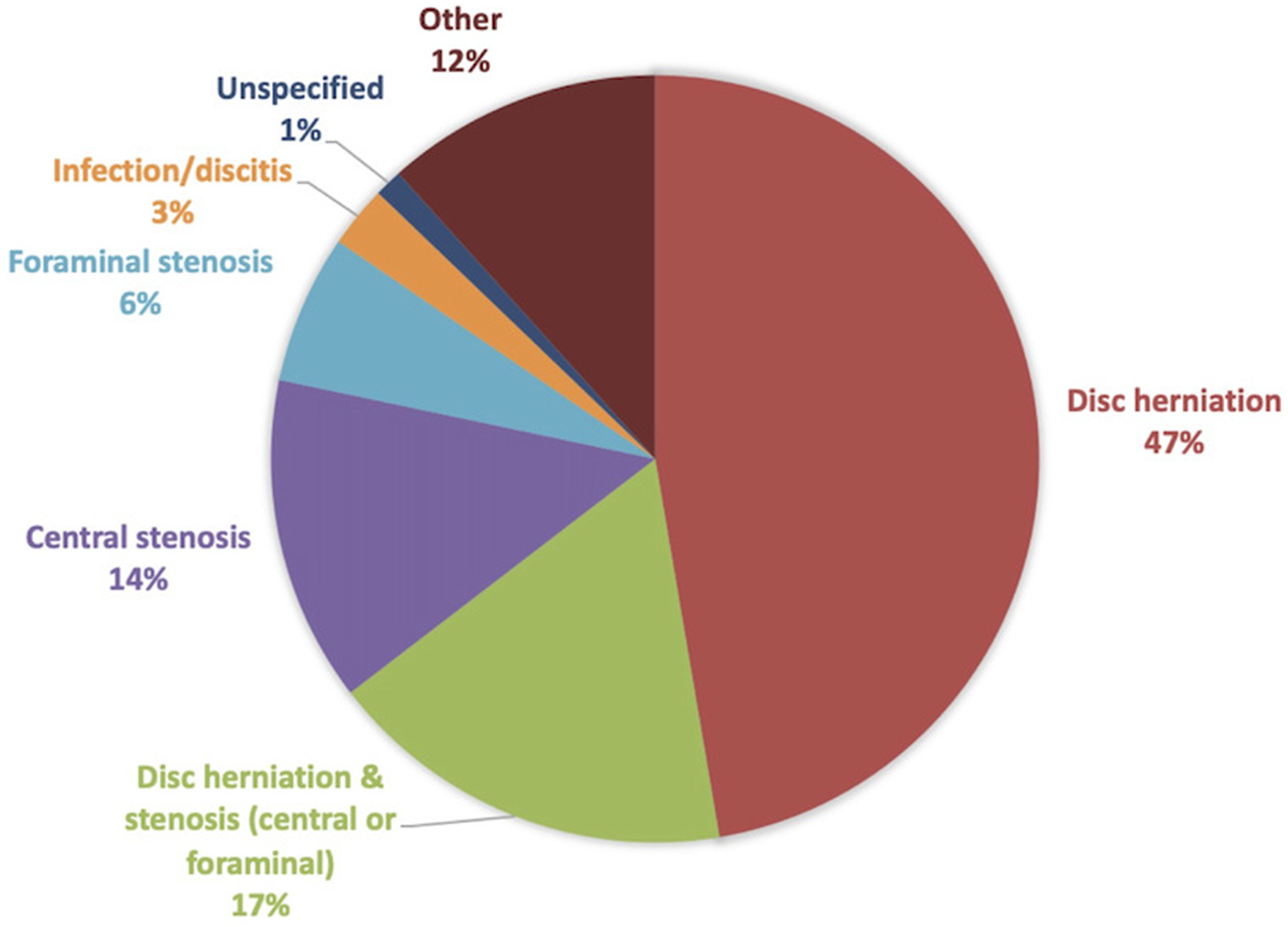
1187 studies (99.5%) reported the number of spinal levels treated. The weighted mean number of levels was 1.03 (SD 0.12, range 1-4). The number of multilevel procedures reported over time increased noticeably starting in 2016 (Figure 8). The urgency of the case was reported in 1186 studies (99.4%). The vast majority were elective procedures (n = 1,163, 97.5%), with only a small number classified as urgent or emergent (n = 23, 1.9%). The number of multilevel procedures reported over time (n = 177)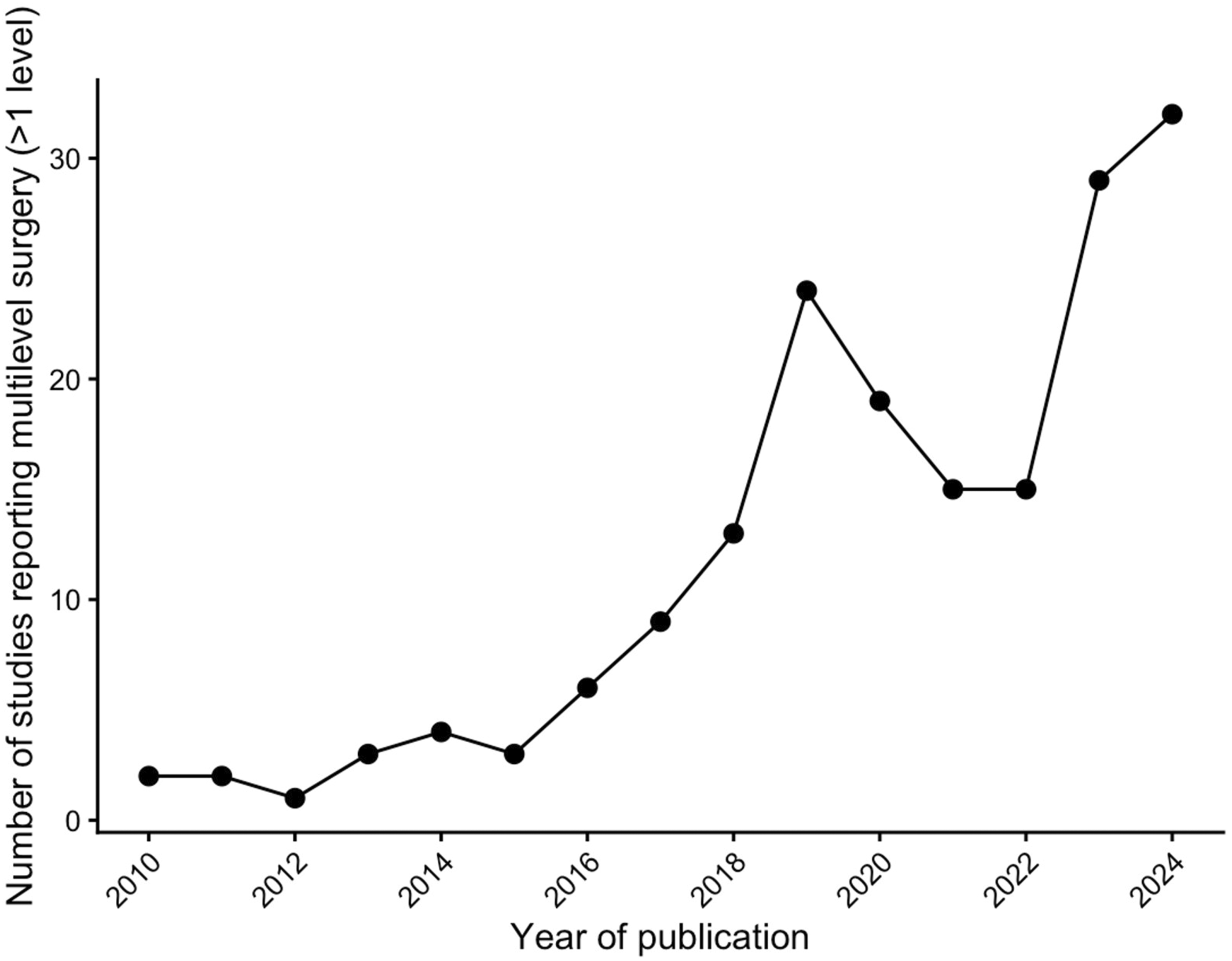
Reported Outcomes
The most frequently reported outcomes in the literature included pain scores (n = 1020, 85.5%), complication rates and readmissions (n = 948, 79.5%), spine-specific patient-reported outcome measures (PROMs) such as Oswestry Disability Index (n = 871, 73%) and intraoperative variables such as operating room time (n = 818, 68.6%). The least commonly reported outcomes were education and learning curve related outcomes (n = 52, 4.4%), and costs related to endoscopic spine surgery (n = 43, 3.6%). Most studies reported preoperative baseline PROMs (n = 1077, 90.3%). The most common first and last postoperative PROM data collection was <2 weeks (n = 465, 38.9%) and 12 weeks to 1 year (n = 490, 41.1%). PROMs that were collected >1 years after surgery represented 31.0% of studies (n = 370).
Discussion
Evidence Gaps and Future Research Directions in Endoscopic Spine Surgery

CUSUM, cumulative sum analysis; LOS, length of stay; RCT, randomized controlled trials,ODI, Oswestry Disability Index; PROM, patient-reported outcome measure; QALY, quality-adjusted life-year; RTW, return to work.
The current literature is disproportionately concentrated in Asia, particularly in China and South Korea, which together accounted for 72% of all studies. This reflects earlier adoption of endoscopic spine surgery in Asian countries compared to Western countries. In China, one reason for early adoption was its cost-effectiveness, as endoscopic instrument sets were cheaper than microscopes required for minimally invasive spine surgery. 29 Geographic concentration may also be driven by more formalized training pathways, high-volume centers, and influential opinion leaders who have helped disseminate endoscopic techniques across Asia.29-32 In Korea, patient acceptance has also been cited as a contributing factor, given the minimally invasive profile of endoscopic surgery and its feasibility under less invasive anesthesia approaches than general anesthesia. 30 Overall, economic factors likely interact with professional dissemination networks and health-system context. Taken together, this geographic skew highlights both the maturity of the evidence base in early-adopting regions and an important opportunity to broaden global research collaboration to support generalizability across diverse healthcare systems and patient populations.
The predominance of low-level evidence in the current endoscopic spine surgery literature, specifically the high proportion of case series (n = 588, 49.3%) and retrospective cohort studies (n = 396, 33.2%) has important implications for clinical practice and future research. This imbalance limits the ability to draw definitive conclusions regarding the efficacy, safety, and long-term outcomes of endoscopic techniques across various spinal pathologies. Further, without high-quality comparative studies with non-endoscopic spine approaches, that includes varied pathologies (e.g., central vs foraminal stenosis, and different zones of disc migration), this hinders the development of personalized treatment approaches. Many studies lack methodological rigor, with inadequate control groups, short follow-up, and limited reporting of patient-centered outcomes. This presents a substantial opportunity to create prospective multicenter studies, high-quality randomized controlled trials, and well-designed clinical registries to fill these gaps. The recently established Endoscopic Spine Research Group (ESRG) represents a promising initiative to improve the quality and generalizability of data in endoscopic spine surgery. 33 The ESRG fosters collaboration across US institutions and enables the design and implementation of multicenter studies that can overcome the limitation of small, single-center case series that currently dominate the literature. 33 Similarly, the Canadian Spine Outcomes and Research Network (CSORN) has developed a Canadian multicenter registry in endoscopic spine surgery, including a comparative control arm for patients undergoing traditional open or minimally invasive surgery.34,35
We identified 21 studies with Level I evidence. Ten of these RCTs compared and contrasted endoscopic vs traditional surgical approaches: (1) percutaneous transforaminal endoscopic discectomy vs open microdiscectomy,36-38 (2) percutaneous transforaminal endoscopic discectomy vs microendoscopic discectomy,11-13 (3) unilateral biportal endoscopic decompression vs anterior cervical decompression and fusion for unilateral cervical radiculopathy, 39 and (4) biportal endoscopic vs microscopic lumbar decompression for spinal stenosis.40-42 High-quality Level I evidence remains to be lacking in many domains of spinal endoscopy, such as comparing uniportal and biportal endoscopic techniques, comparative efficacy of endoscopic vs traditional techniques in multilevel lumbar spinal stenosis, far lateral or foraminal disc herniation, highly migrated disc herniations, and thoracic disc herniations.
Our review found that uniportal techniques dominated the current literature, comprising 83.9% of all included studies. This likely reflects both the earlier development and broader global dissemination of uniportal techniques, which have traditionally been considered the foundational platform for endoscopic spine surgery. In contrast, biportal endoscopy, which first appeared in the literature in 2013, has seen a marked increase in publications since 2018, signaling growing interest and adoption. The emergence of biportal endoscopy introduces a different surgical philosophy, offering enhanced instrument maneuverability, a wider field of view, and arguably a more familiar workflow for surgeons trained in open or tubular surgery. 43 The increased adoption of biportal endoscopy may stimulate comparative studies that examine clinical outcomes, learning curves, complication profiles, and cost-effectiveness between uniportal and biportal systems. The co-existence of both techniques raises important questions regarding optimal indications, patient selection, surgeon training pathways and the need to establish evidence-based practice standards.
The majority of studies reported on clinical effectiveness (without a comparison group) (n = 422, 35.3%), surgical techniques (n = 291, 24.4%) and comparison with traditional surgical methods (n = 222, 18.6%) as their primary themes. Endoscopic spine surgery is technically challenging and reported to be associated with a steep learning curve, yet only 10 of the 1193 studies (0.8%) reported learning curve as their primary theme.44-46 This is an opportunity for more high-quality studies evaluating the learning curve for endoscopic spine surgery and their impact on patient outcomes and complications. 47 The high initial capital investment and ongoing disposable costs of endoscopic spine surgery is often quoted as a barrier to adopting this technology. Despite this, only 8 out of 1193 studies (0.7%) identified health economics or cost as their primary outcome. 48 In publicly funded health care systems or resource-constrained environments, such as in Canada, rigorous cost-effectiveness and cost utility analyses are essential to justify investment and guide resource allocation. While endoscopic spine surgery has been associated with potential cost savings due to shorter length of hospital stays, earlier return to work, and lower infection rates, these advantages need to be evaluated through formal economic analysis. 49 Without this data, healthcare administrators may be reluctant to support or scale endoscopic spine surgery programs, even in the face of promising clinical outcomes. Furthermore, comparative economic studies between endoscopic spine surgery and conventional surgical techniques are necessary to understand the broader value proposition. Capturing both direct costs (e.g., equipment, hospital stay, readmission), and indirect costs (e.g., loss of work productivity, and absenteeism) will be key to informing evidence-based policies and clinical guidelines.
The integration of enabling technology, such as 2D or 3D navigation, robotics, and augmented reality into endoscopic spine surgery represents an exciting frontier with the potential to enhance surgical precision, reduce complications, and improve ergonomics for surgeons. Despite these advantages, our review found only 3% of studies reported the use of enabling technology, indicating their adoption within the field remains in its infancy.16,50,51 Future research should focus on evaluating the clinical impact and cost-effectiveness of these technologies. Studies comparing standard vs technology assisted endoscopic spine surgery are needed to assess whether these tools improve patient outcomes, reduce operative time, improve surgeon safety through less radiation exposure, or lower complication rates.
Limitations
Our scoping review has several methodological limitations inherent to its design. First, while our search strategy was comprehensive and guided by PRISMA-ScR methodology, we excluded non-English language studies, which may have introduced language bias and limited the global representation of the literature. This is especially important when most included studies were from Asian countries.
In addition, our thematic classification of each study was limited to a single primary theme, potentially underestimating the breadth of secondary outcomes (e.g., cost, neuromonitoring, or learning curve) that were not the focus of the study but may still be clinically relevant. The review also focused on the presence or absence of reported data points rather than performing a critical appraisal of study quality or risk of bias, which limited our ability to comment on the overall methodological rigor of the included studies. This could increase the risk of misclassification error for the level of evidence. We restricted our inclusion window to studies published from January 2010 to September 2024 to capture contemporary trends, but this may have excluded relevant foundational literature prior to 2010 that helped shape the evolution of endoscopic techniques. Similarly, selecting September 22, 2024 as the search cutoff date resulted in the omission of certain high-quality studies that were published in 2025, including a biportal endoscopy-related RCT. 52 This search cutoff date also excludes studies expected to be published in 2026-2027, including the ENDO-F trial (studying endoscopy for lumbar spinal stenosis and lumbar disc herniations), NCT05480267 (UBE vs MIS-TLIF), and NCT07151651 (recently registered). 53
Our study was aimed for surgeons and researchers, with the goal of mapping current available evidence in the field of spine endoscopy and to help guide future research directions. The goal was not to provide clinical recommendations for endoscopic spine surgery. This study was also not intended to inform insurance companies or industry stakeholders, and therefore we did not extract data relevant to these two groups.
Finally, although the title and abstract screening and full-text review was duplicated by two reviewers, the data extraction was divided between the two reviewers and were not duplicated. Consensus meetings were held to ensure definitions were agreed upon to maintain consistency in data collection.
Conclusions
Although the number of publications on spine endoscopy has increased significantly from 2010 to 2024, current literature primarily consists of low-quality studies with limited high-quality comparative studies or randomized controlled trials. This scoping review highlights critical knowledge gaps and emphasizes the need for more robust, high-quality studies to guide clinical decision-making and advance the field of endoscopic spine surgery.
Supplemental Material
Supplemental Material - Endoscopic Spine Surgery: A Scoping Review of the Literature
Supplemental Material for Endoscopic Spine Surgery: A Scoping Review of the Literature by Drew Mulhall, MD, Chien Yew Kow, MD, Catherine Veilleux, MD, Anand Oliveira Masson, MD, PhD, Steven Casha, MD, PhD, Stephan du Plessis, MD, Ken Thomas, MD, MHSc, Michael M. H. Yang, MD MSc M.Biotech in Global Spine Journal.
Footnotes
Acknowledgements
The above authors would like to acknowledge the Calgary Health Foundation for funding the research project.
Author Contributions
Drew Mulhall, MD – Conceptualization, data curation, formal analysis, investigation, methodology, visualization, writing – original draft and review/editing
Chien Yew Kow, MD – Conceptualization, data curation, formal analysis, investigation, methodology, writing –review/editing
Catherine Veilleux, MD – Data curation, formal analysis, methodology, software, visualization, writing – original draft and review/editing
Anand Oliveira Masson, PhD – Conceptualization, data curation, investigation, methodology, project administration, resources, writing – original draft and review/editing
Steven Casha, PhD – Conceptualization, formal analysis, supervision, writing –review/editing
Stephan du Plessis, PhD – Conceptualization, formal analysis, supervision, writing –review/editing
Ken Thomas, MD, MHSc – Conceptualization, formal analysis, investigation, investigation, methodology, supervision, validation, writing –review/editing
Michael M.H. Yang, MD, MSc, M.Biotech – Conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, writing –review/editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The above authors would like to acknowledge the Calgary Health Foundation for funding the research project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.