
Abstract
Study Design
Systematic review and meta-analysis.
Objective
Although uniportal and biportal endoscopic decompression have emerged as promising minimally invasive options for the management of lumbar spinal stenosis (LSS), their relative advantages remain debated. This systematic review and meta-analysis aims to evaluate the efficacy and safety of both approaches in LSS treatment.
Methods
In adherence to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines, we systematically searched PubMed, Embase, Cochrane Library, and Web of science for randomized controlled trials and observational studies comparing the outcomes of uniportal and biportal endoscopic techniques for LSS treatment. Meta-analysis was performed using a random-effects model.
Results
A total of 11 studies were included, comprising 1199 patients. Biportal endoscopy was associated with a significantly lower operation time (P < .01), Oswestry Disability Index (ODI) at 12 months (P < .01), and higher postoperative dural sac area (P < .01) and dural sac area expansion (P = .02). There were no significant differences between groups in intraoperative blood loss, hospitalization time, back pain, leg pain, or ODI at other timepoints, ipsilateral facetectomy angle, and overall complications, including dural tear, infection, postoperative hematoma, lower limb numbness, and nerve root injury.
Conclusion
In this meta-analysis, biportal endoscopic decompression demonstrated significantly lower operation time, ODI at 12 months, and higher postoperative dural sac area and dural sac area expansion, although both techniques showed similar safety profiles and complication rates. Further high-quality studies are needed to better assess the advantages of both techniques for LSS treatment.
Keywords
Introduction
Lumbar spinal stenosis (LSS) is a prevalent degenerative condition defined by narrowing of the lumbar spinal canal, which often results in nerve compression and associated symptoms such as pain, weakness, or numbness. Treatment options for LSS are divided into conservative and surgical approaches. 1 Conservative management includes pain medications, epidural steroid injections, and physical therapy. However, surgical treatment aimed at decompressing neural structures becomes essential when symptoms persist or worsen.2,3
Decompression is typically performed through open laminectomy, a well-known procedure that effectively alleviates neural compression. Nevertheless, open techniques are associated with significant drawbacks, such as extensive soft tissue dissection, postoperative pain, muscle atrophy, and prolonged recovery periods.4,5 To overcome these issues, minimally invasive surgical approaches, like endoscopic spinal surgery, have gained popularity, offering significant advantages like reduced soft tissue damage, precise decompression, and quicker recovery compared to traditional surgery.6,7
Among these techniques, biportal endoscopic unilateral laminotomy for bilateral decompression (BE-ULBD) has emerged as a popular option. This method involves 2 small incisions for the insertion of an observation portal and a working portal, facilitating clear visualization and precise decompression.8,9 An alternative is the uniportal endoscopic unilateral laminotomy for bilateral decompression (UE-ULBD), which employs a single incision for a combined portal (endoscopic and instrumental), potentially decreasing tissue disruption and postoperative morbidity.10,11
Although both techniques are increasingly adopted, their relative advantages remain debated. Some studies suggest that biportal techniques offer better visualization and technical versatility, whereas others emphasize the advantages of uniportal approaches in minimizing tissue trauma.6-11 This systematic review and meta-analysis aims to evaluate the efficacy and safety of UE-ULBD and BE-ULBD for LSS by comparing their clinical, radiological, and surgical outcomes.
Methods
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines, 12 and was registered in the PROSPERO database (CRD42024615712).
Search Strategy
PubMed, Embase, Cochrane Library, and Web of Science databases were independently searched by 2 authors (K.L., C.S.) from inception to November 2024 using the following search strategy: (uniportal OR monoportal OR single-port OR single-portal OR single-channel OR full-endoscopic OR percutaneous OR UESS) AND (biportal OR dual-port OR dual-portal OR dual-channel OR UBE OR BESS) AND (“spinal stenosis” OR “lumbar stenosis” OR LSS OR “canal stenosis” OR “neurogenic claudication”).
Eligibility Criteria
Inclusion criteria were as follows: (1) randomized controlled trials (RCTs) or observational studies; (2) comparing the outcomes of uniportal and biportal endoscopic decompression; and (3) in patients diagnosed with LSS. Exclusion criteria were as follows: (1) studies in which unilateral laminotomy for bilateral decompression (ULBD) technique was not applied; and (2) conference abstracts.
Data Extraction and Outcomes
Two researchers (K.L., Y.S.) independently performed data extraction, with disagreements resolved after discussion with a third author (R.O.). The outcomes assessed included operation time; intraoperative blood loss; length of hospitalization; Visual Analog Scale (VAS) scores for leg and back pain; Oswestry Disability Index (ODI); MacNab criteria excellent or good rate; radiological outcomes at the last follow-up, including postoperative dural sac area, dural sac area expansion, and ipsilateral facetectomy angle; and incidence of complications, such as dural tear, infection, lower limb numbness, nerve root injury, and postoperative hematoma.
Quality Assessment
Methodologic quality and risk of bias were assessed independently by 2 authors (K.L., N.R.) using the Cochrane Collaboration Risk of Bias (ROB-2) tool for RCTs. 13 For observational studies, the Cochrane Collaboration ROBINS-I tool (Risk Of Bias In Non-randomized Studies - of Interventions) was used. 14 In case of discordant results, a third reviewer (C.S.) made a final decision after discussion with the team.
Statistical Analysis
Meta-analysis of extracted data was performed utilizing R software. Odds ratio (OR) and mean differences (MDs) were calculated as summary measures for dichotomous and continuous outcome variables, respectively, using DerSimonian and Laird random-effects model and a 95% confidence interval (CI). Effect sizes with P-values inferior to .05 were considered statistically significant. Heterogeneity was assessed with the Cochran Q test and I2 statistics. The P values inferior to .10 and I2 ≥ 50% were considered significant for heterogeneity. Sensitivity analysis was used to investigate the sources of heterogeneity. The possibility of publication bias in outcomes with at least 10 studies was determined through funnel plots and Egger test. In cases of missing standard deviation of values, a correlation coefficient of 0.5 was applied, as recommended by the Oxford Centre for Evidence-Based Medicine. 15
Results
Search Results and Study Characteristics
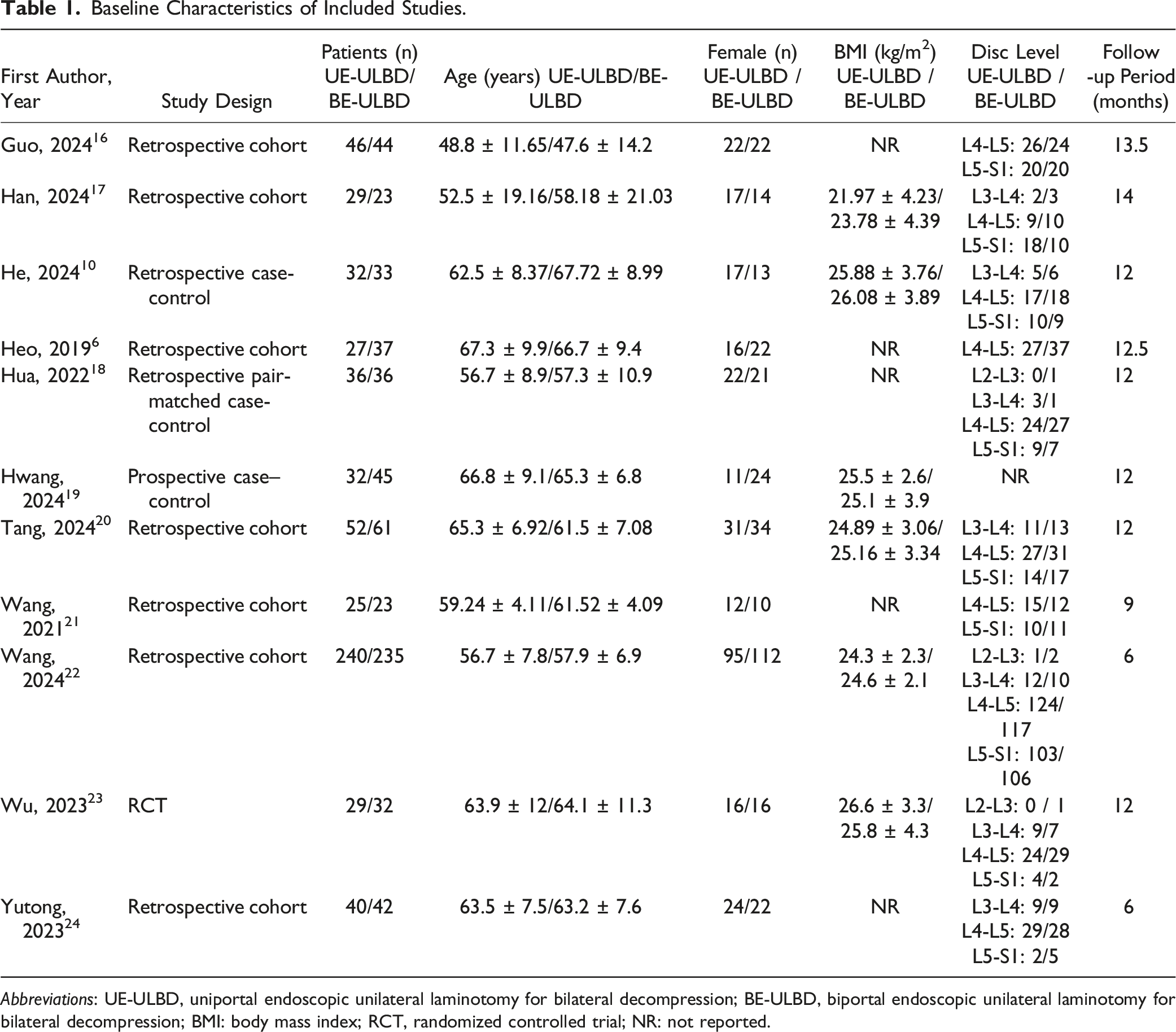
The search yielded 176 results. After the removal of duplicate records and ineligible studies, 16 articles remained and were fully reviewed based on inclusion criteria. Of these, a total of 11 studies (1 RCT and 10 observational studies) were eligible for inclusion (Figure 1).6,10,16-24 These studies comprised 1199 participants, of whom 588 (49%) underwent UE-ULBD and 611 (51%) underwent BE-ULBD. Table 1 outlines both the study and participant characteristics of each included study. Study selection flow diagram. Baseline Characteristics of Included Studies. Abbreviations: UE-ULBD, uniportal endoscopic unilateral laminotomy for bilateral decompression; BE-ULBD, biportal endoscopic unilateral laminotomy for bilateral decompression; BMI: body mass index; RCT, randomized controlled trial; NR: not reported.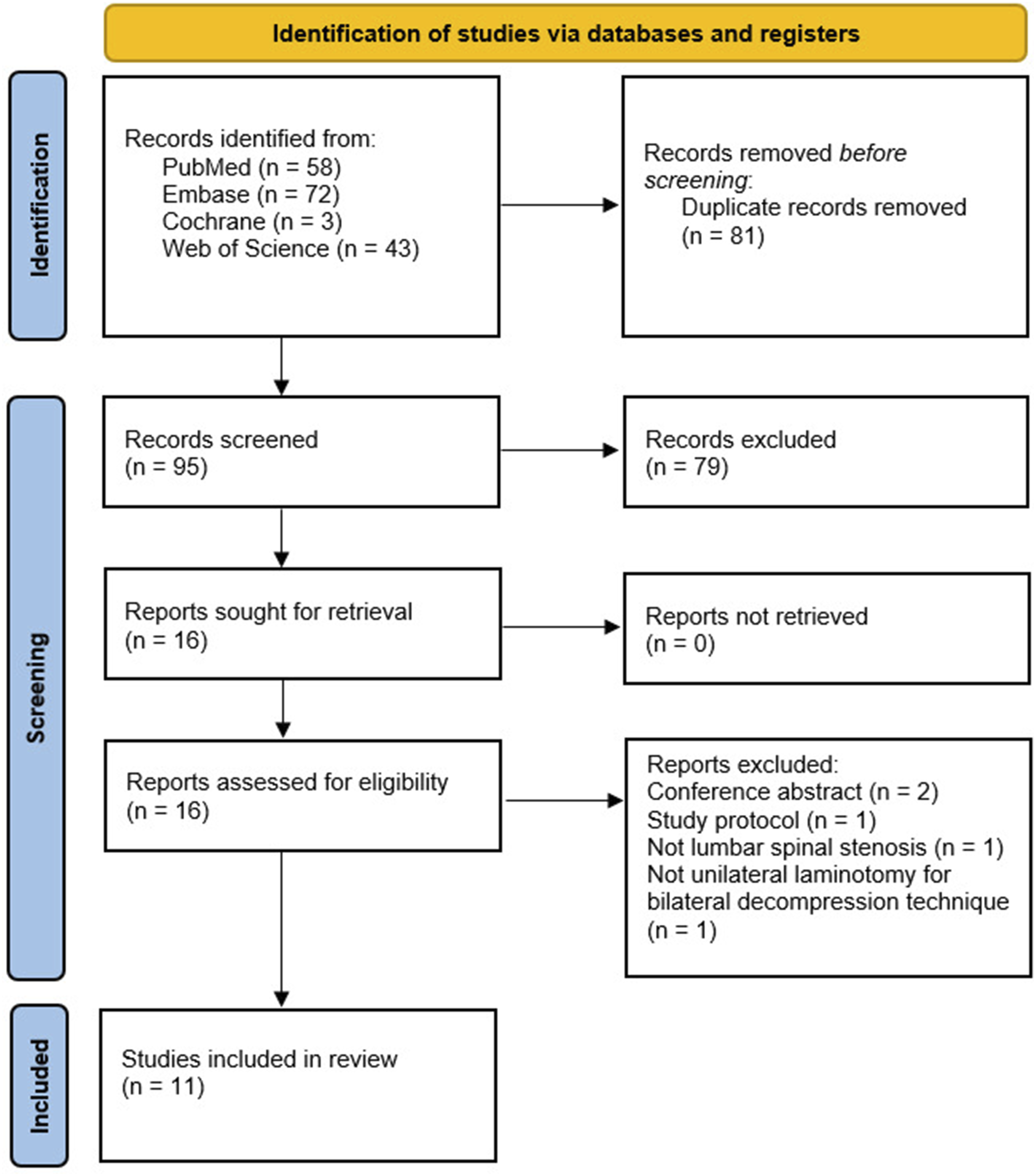
Meta-Analysis Results
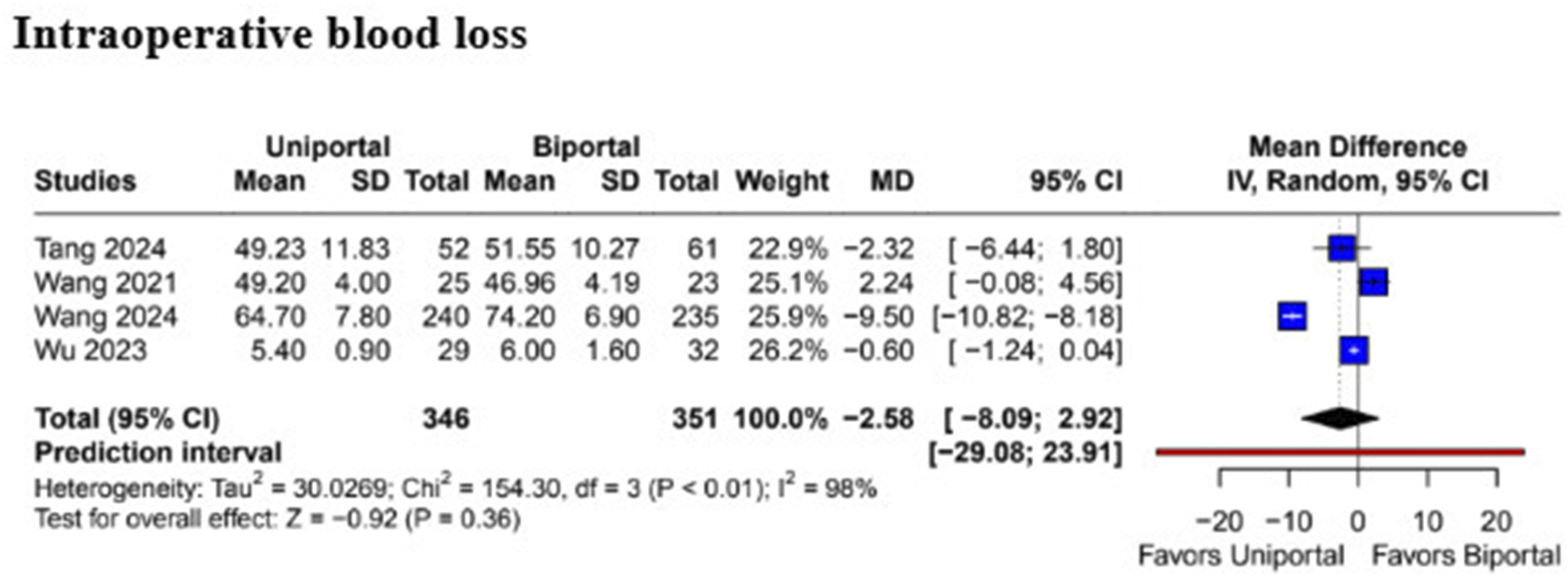
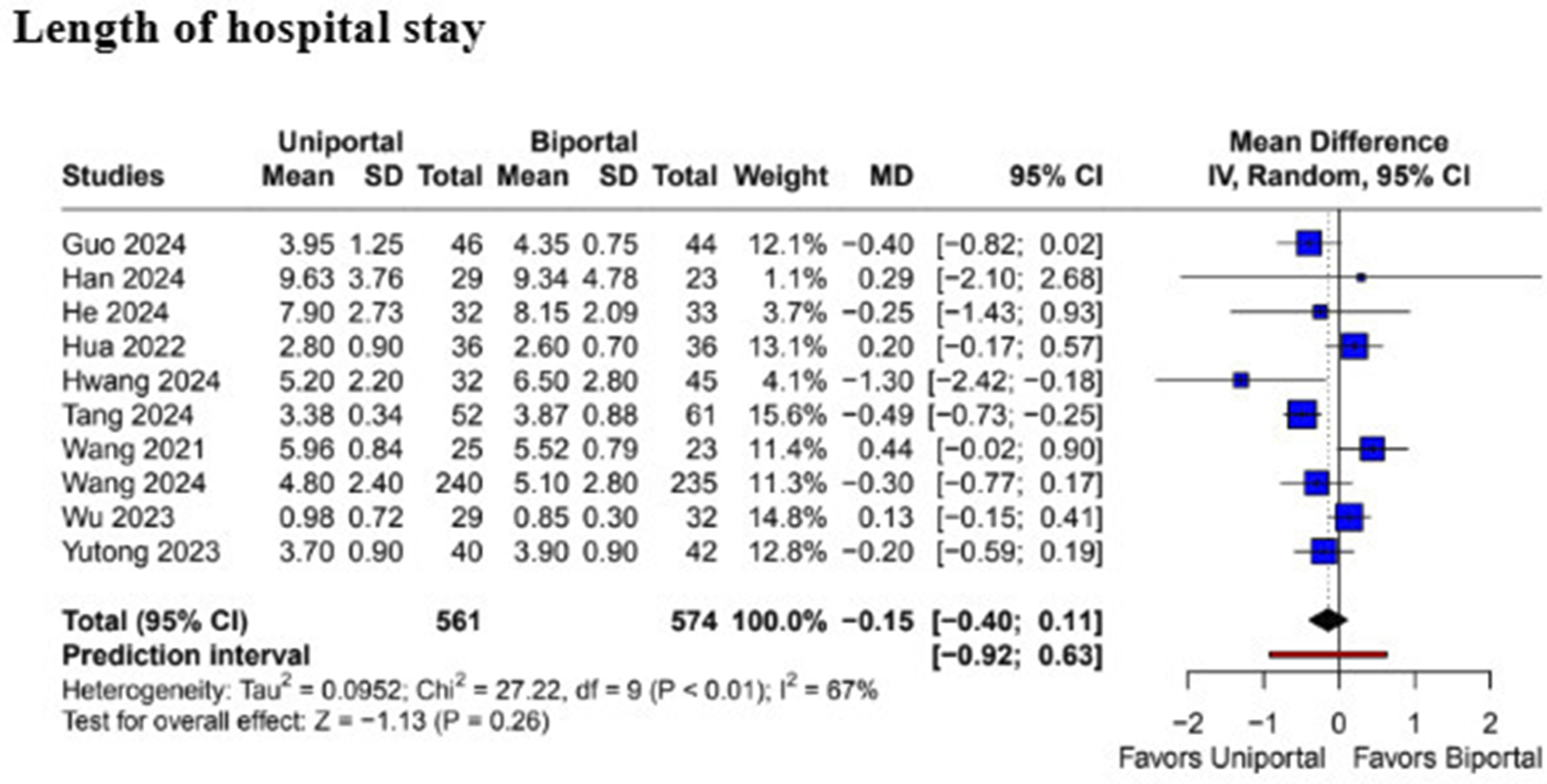
The pooled analysis revealed that patients undergoing BE-ULBD had a significantly shorter operation time compared to UE-UBLD (MD 15.85; 95% CI [4.27, 27.44]; P < .01; I2 = 99%) (Figure 2). However, there was no statistically significant difference in intraoperative blood loss (MD −2.58; 95% CI [−8.09, 2.92]; P = .36; I2 = 98%) (Figure 3) and length of hospital stay (MD −0.15; 95% CI [−0.40, 0.11]; P = .26; I2 = 67%) (Figure 4) between the 2 surgical techniques. Forest plots comparing uniportal and biportal decompression in terms of operation time. Forest plots comparing uniportal and biportal decompression in terms of intraoperative blood loss. Forest plots comparing uniportal and biportal decompression in terms of length of hospital stay.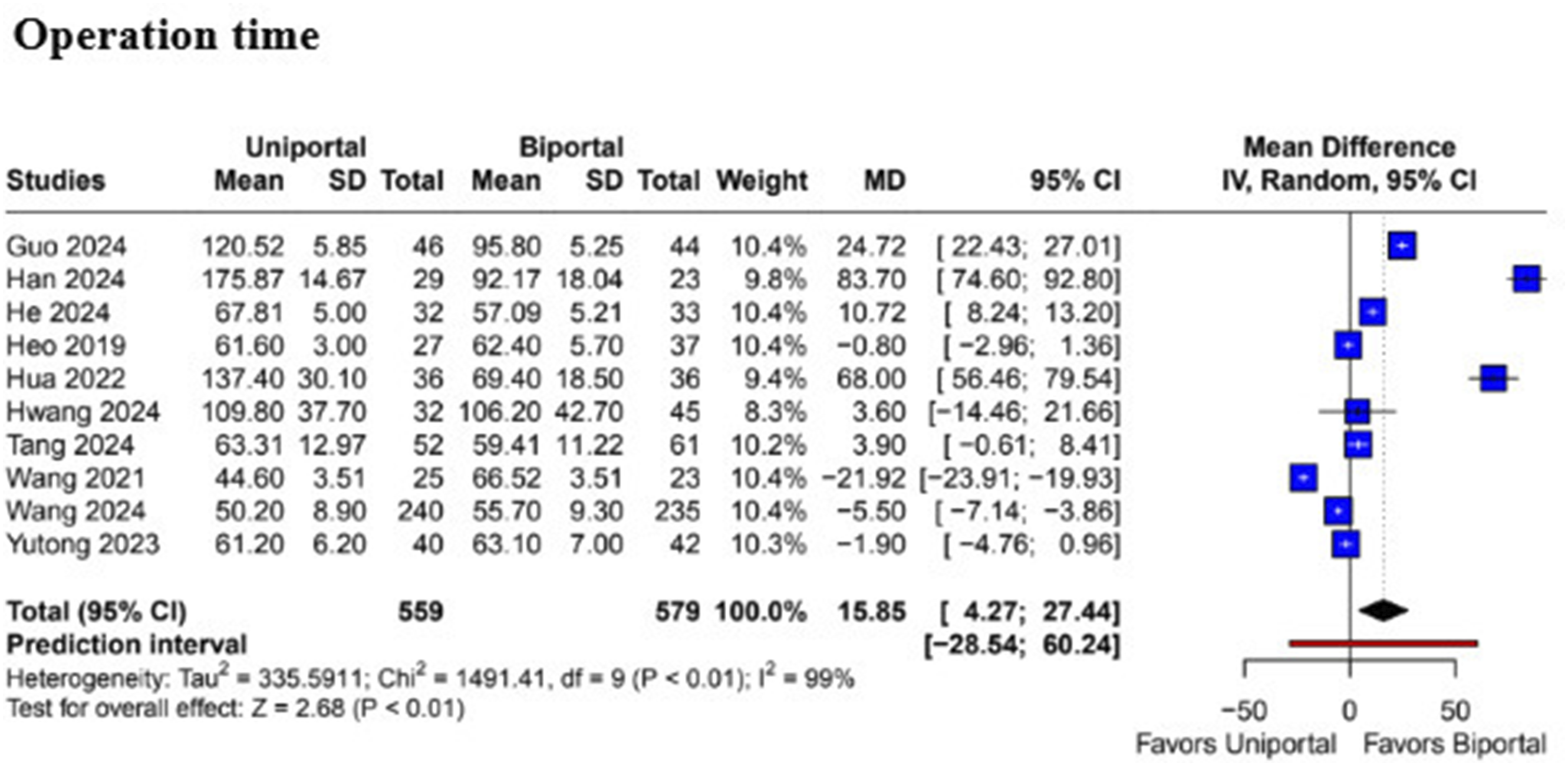
In terms of pain outcomes, there were no significant differences in lower back pain between patients undergoing UE-ULBD or BE-ULBD at 3 days (MD 0.13; 95% CI [−0.31, 0.57]; P = .55; I2 = 66.4%), 3 months (MD −0.02; 95% CI [−0.15; 0.10]; P = .75; I2 = 27.9%), 6 months (MD 0.12; 95% CI [−0.12, 0.36]; P = .32; I2 = 64.5%), and 12 months (MD 0.10; 95% CI [−0.03, 0.23]; P = .11; I2 = 31.9%) (Figure 5). Forest plots comparing uniportal and biportal decompression in terms of Visual Analog Scale (VAS) for back pain at 3 days, 3 months, 6 months, and 12 months postoperatively.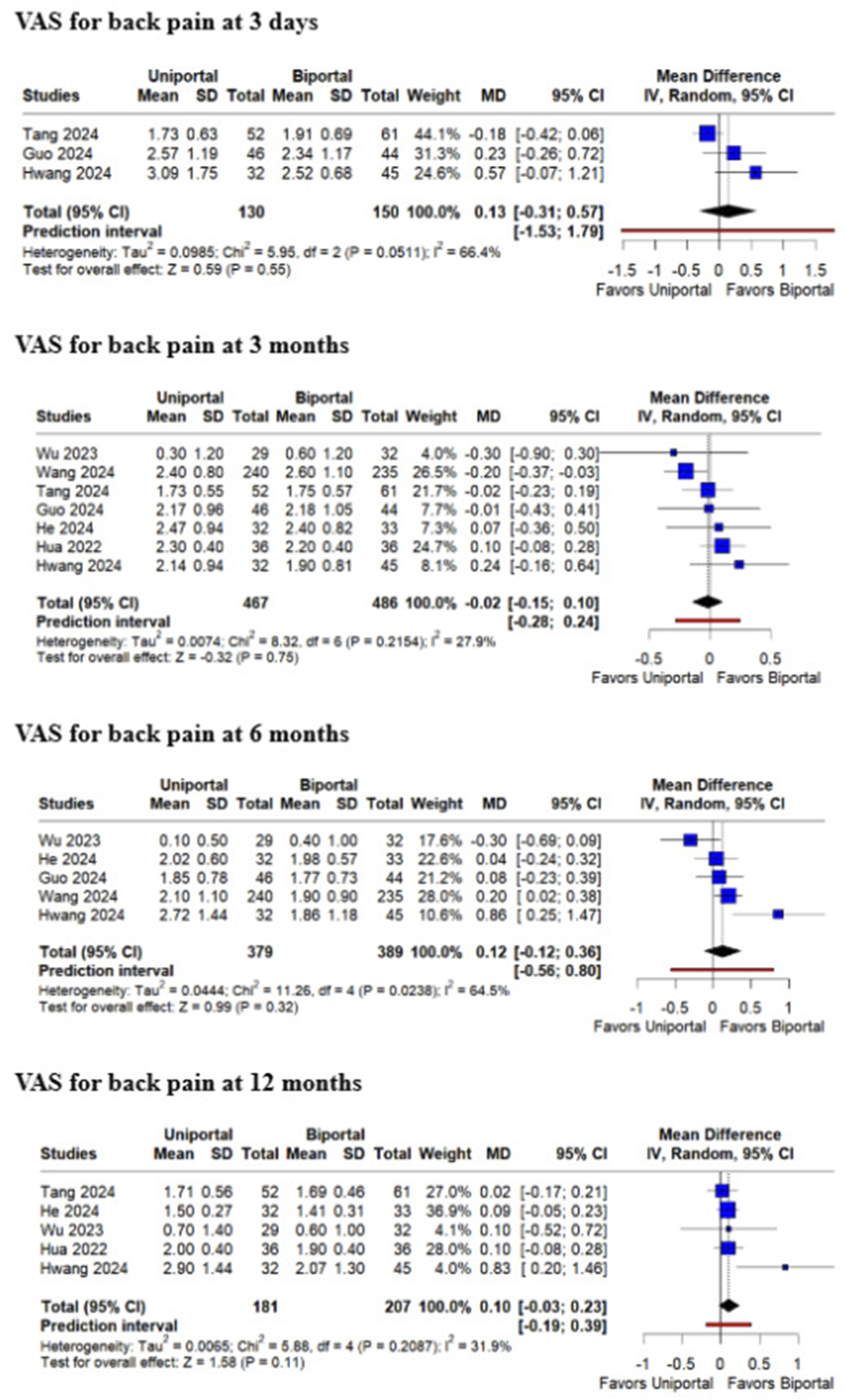
Regarding leg pain, there were no significant differences between groups at 3 days (MD 0.05; 95% CI [−0.20, 0.29]; P = .71; I2 = 0%), 3 months (MD 0.10; 95% CI [−0.05, 0.25]; P = .17; I2 = 41.7%), 6 months (MD 0.10; 95% CI [−0.05, 0.24]; P = .20; I2 = 20.6%), and 12 months (MD 0.08; 95% CI [−0.08, 0.25]; P = .31; I2 = 45.4%) (Figure 6). Forest plots comparing uniportal and biportal decompression in terms of Visual Analog Scale (VAS) for leg pain at 3 days, 3 months, 6 months, and 12 months postoperatively.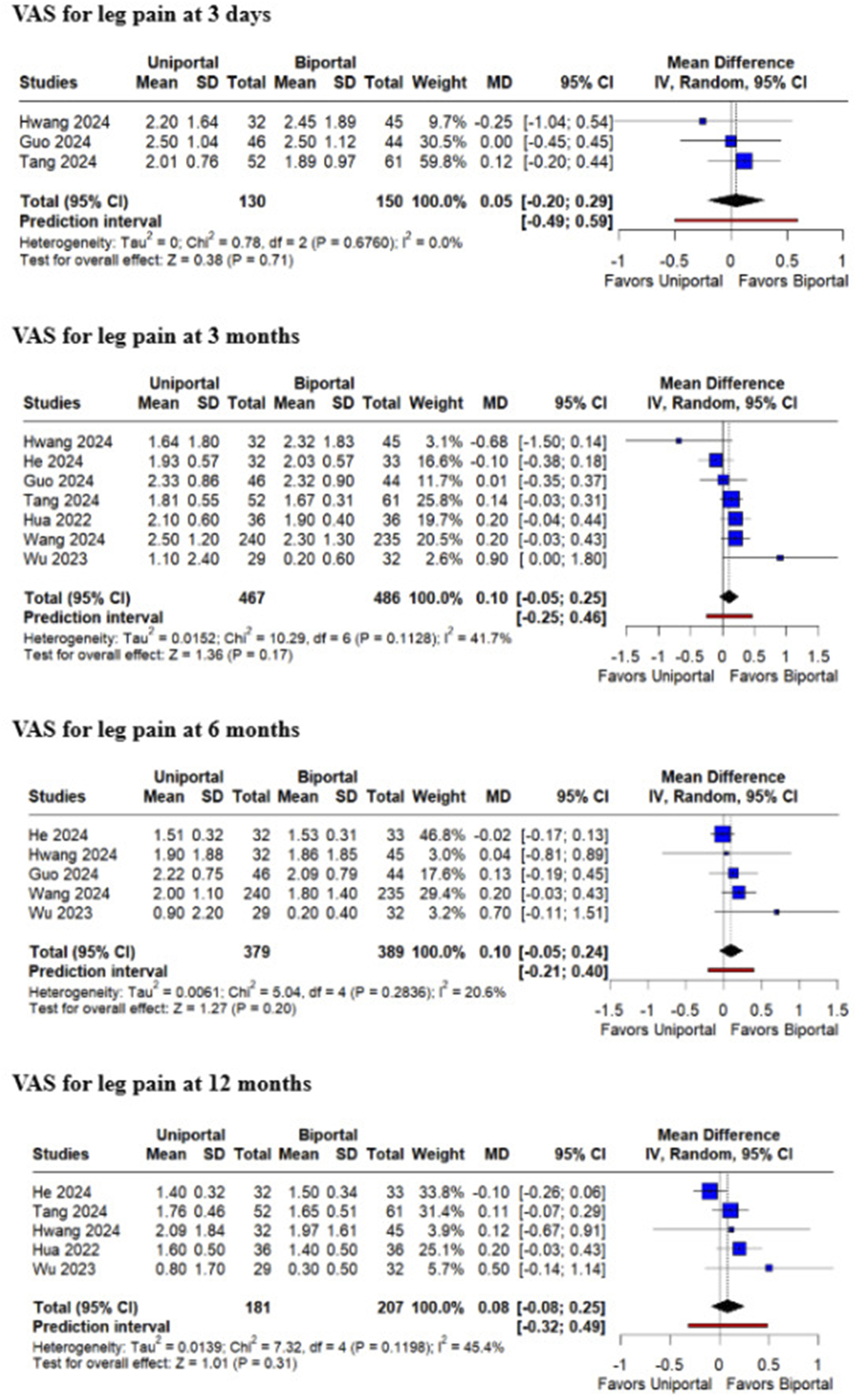
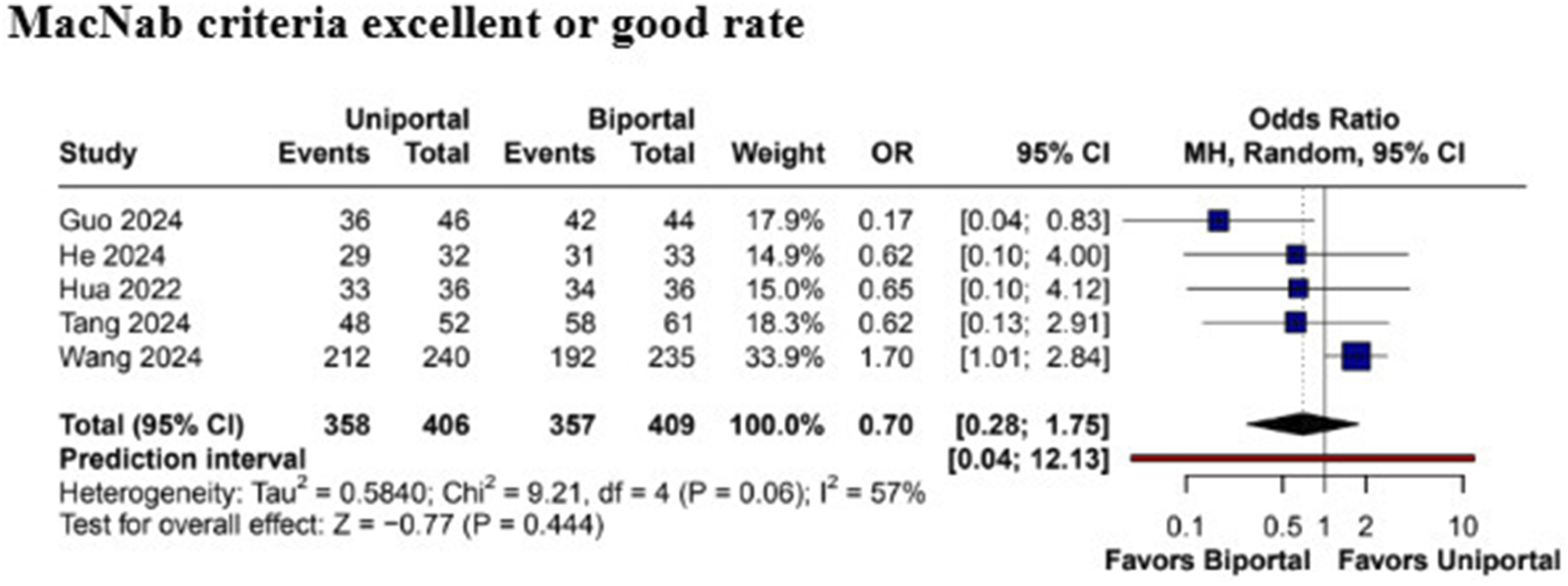
The ODI scores did not differ significantly between the 2 procedures at 3 months (MD 3.32; 95% CI [−1.55, 8.20]; P = .18; I2 = 98.6%) or at 6 months (MD 6.25; 95% CI [−1.91, 14.41]; P = .13; I2 = 99.5%). However, at 12 months, patients who underwent UE-UBLD demonstrated a statistically significant improvement in ODI scores compared to BE-ULBD (MD 0.88; 95% CI [0.37, 1.39]; P < .01; I2 = 0%) (Figure 7). The excellent or good rate of the MacNab criteria did not differ significantly between the groups (OR 0.70; 95% CI [0.28, 1.75]; P = .44; I2 = 57%) (Figure 8). Forest plots comparing uniportal and biportal decompression in terms of Oswestry Disability Index (ODI) at 3 months, 6 months, and 12 months postoperatively. Forest plots comparing uniportal and biportal decompression in terms of MacNab criteria excellent or good rate.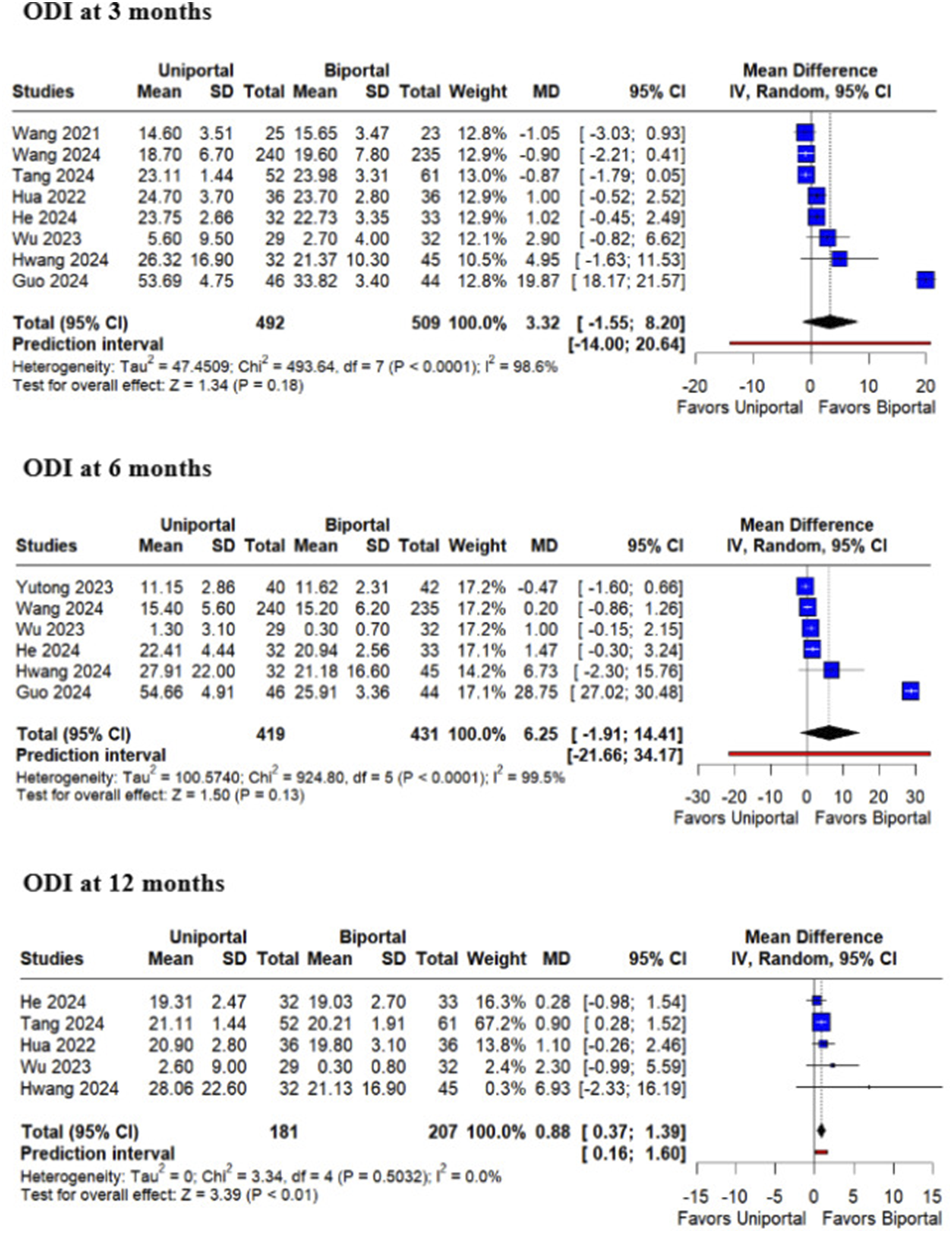
Regarding radiological outcomes, the postoperative dural sac area was significantly higher in patients undergoing BE-ULBD compared to those receiving UE-UBLD (MD −11.01; 95% CI [−15.79, −6.24]; P < .01; I2 = 71.5%), as well as the dural sac area expansion from baseline (MD −14.64; 95% CI [−26.76, −2.51]; P = .02; I2 = 89.3%). Both surgical techniques showed similar results for ipsilateral facetectomy angle (MD 11.33; 95% CI [−0.44, 23.10]; P = .06; I2 = 99%) (Figure 9). Forest plots comparing uniportal and biportal decompression in terms of postoperative dural sac area, dural sac area expansion, and ipsilateral facetectomy angle.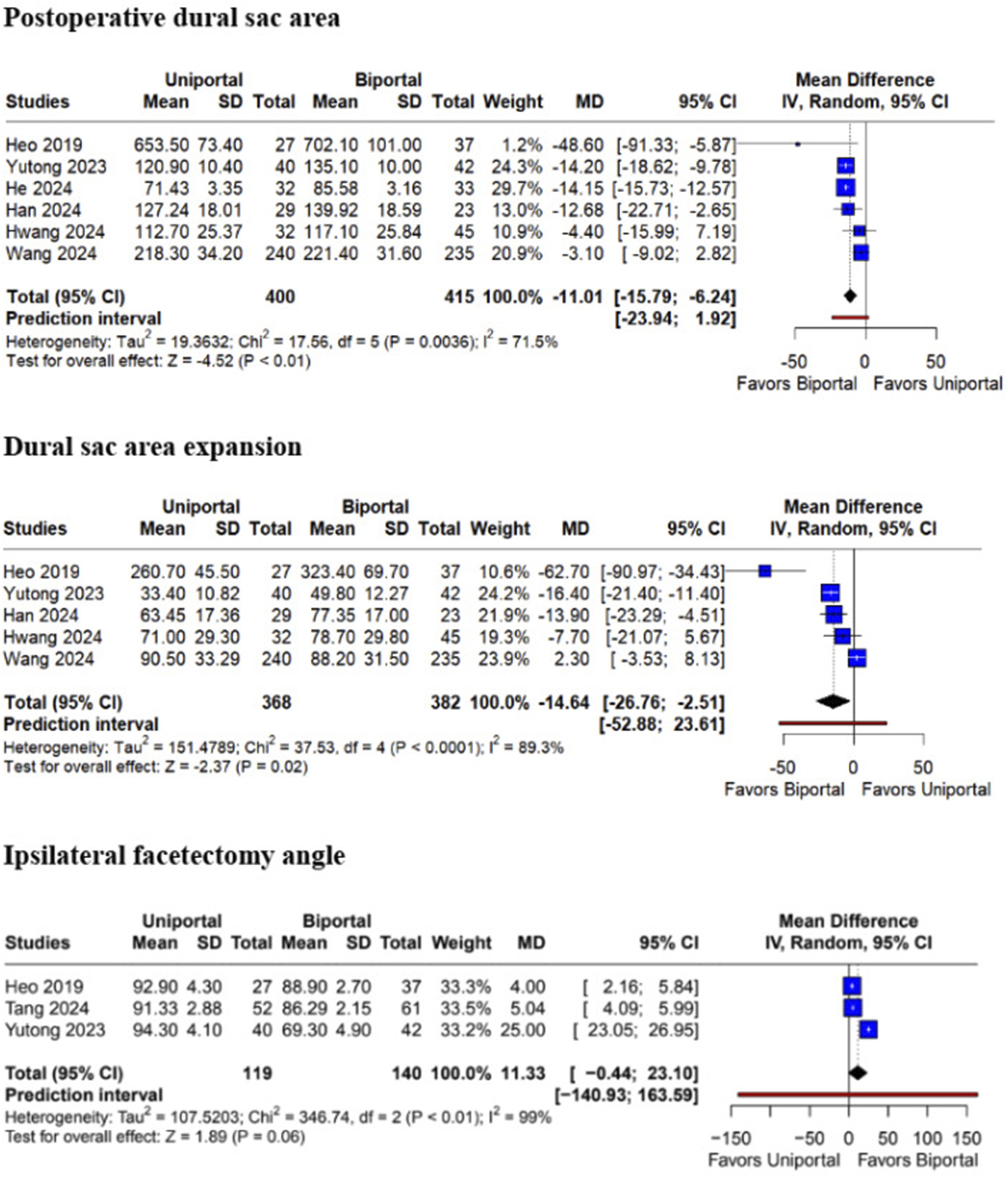
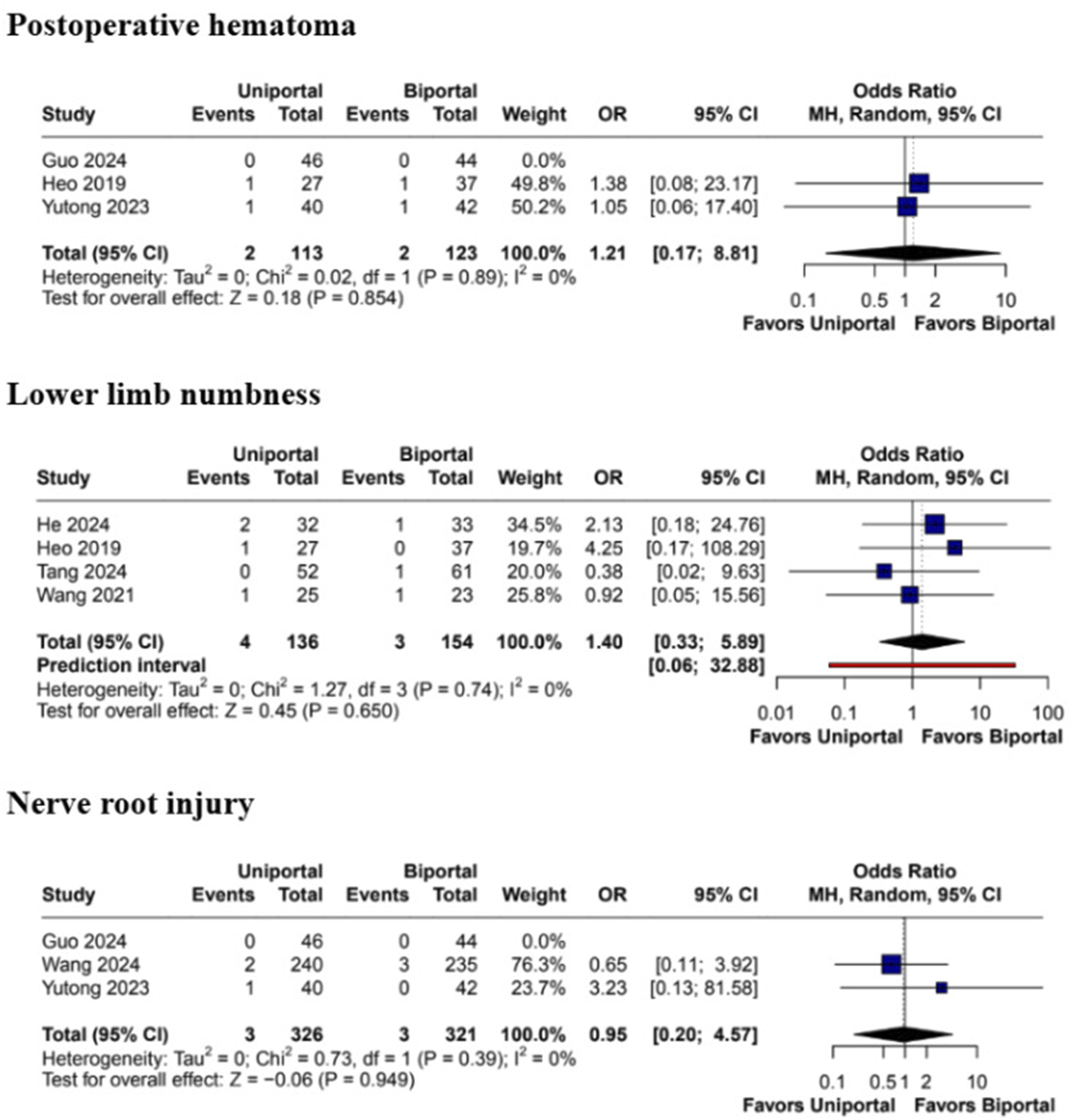
No statistically significant differences were observed in overall complication rates (OR 1.38; 95% CI [0.71, 2.71]; P = .34; I2 = 0%). Similarly, there were no significant differences in the rates of dural tears during surgery (MD 1.56; 95% CI [0.63, 3.88]; P = .34; I2 = 0%) and postoperative infection (OR 0.33; 95% CI [0.01, 8.02]; P = .49) (Figure 10). There were also no significant differences in the rates of postoperative hematoma (OR 0.21; 95% CI [0.17, 8.81]; P = .85; I2 = 0%), nerve root injury (OR 0.95; 95% CI [0.20, 4.57]; P = .95; I2 = 0%), or in reports of lower limb numbness (OR 1.40; 95% CI [0.33, 5.89]; P = .65; I2 = 0%) (Figure 11). Forest plots comparing uniportal and biportal decompression in terms of total complications, dural tear, and infection. Forest plots comparing uniportal and biportal decompression in terms of postoperative hematoma, lower limb numbness, and nerve root injury.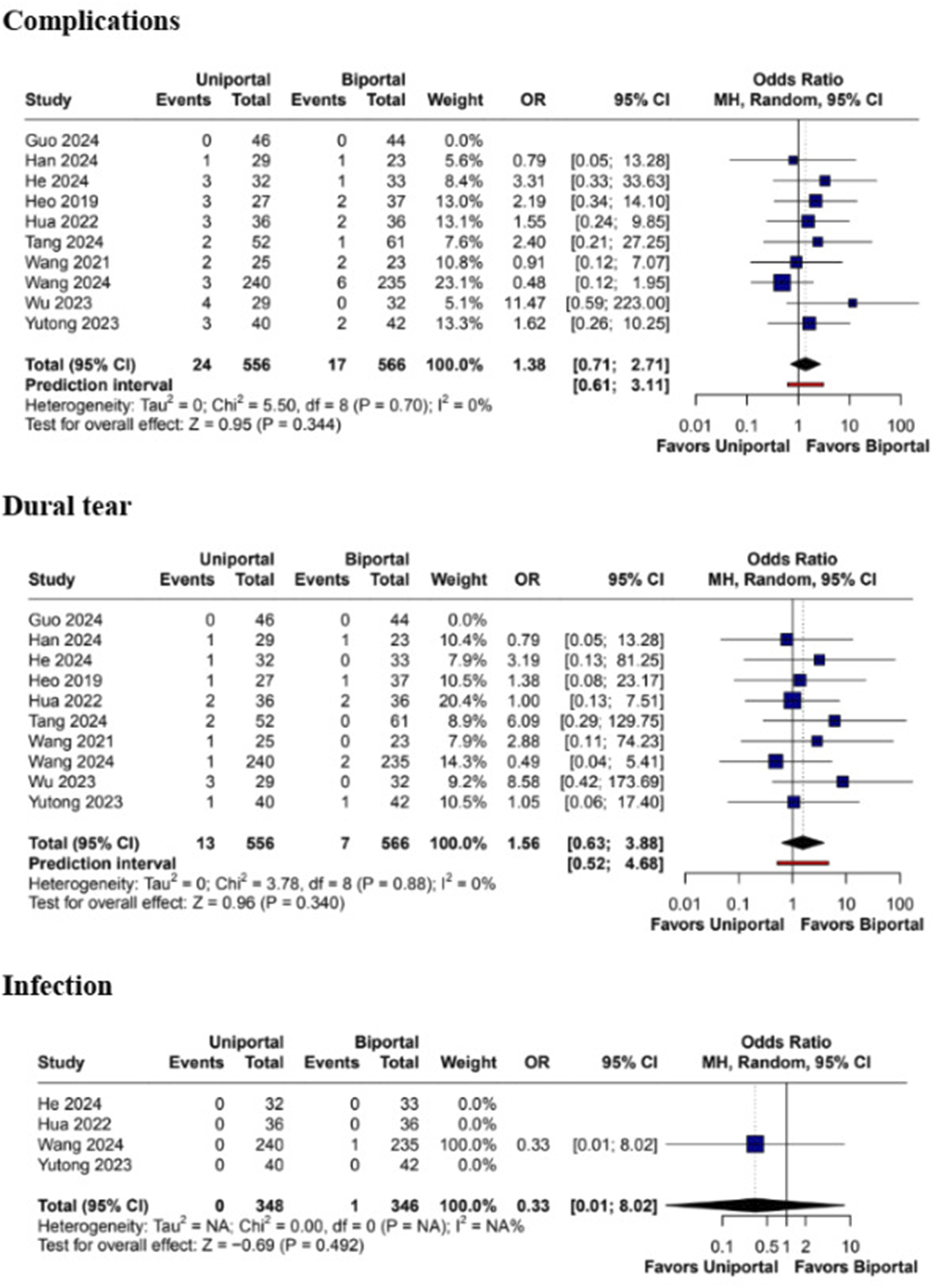
Sensitivity Analysis
Leave-one-out sensitivity analysis did not demonstrate a significant effect in the pooled results except for leg pain VAS at 6 and 12 months, and ipsilateral facetectomy angle, in which the overall results significantly favored BE-ULBD (Supplemental Figures S1 to S3). Additionally, ODI at 12 months, dural sac area expansion, and operation time became statistically insignificant after leave-one-out approach (Supplemental Figures S4 to S6).
Regarding heterogeneity, sensitivity analyses were performed for dural sac area expansion, operation time, intraoperative blood loss, length of hospital stay, and ODI at 3 months; however, the results continued to show high heterogeneity (Supplemental Figures S5 to S9). In contrast, leave-one-out sensitivity analysis significantly reduced heterogeneity in ipsilateral facetectomy angle, VAS for back pain at 3 days and 6 months, ODI at 6 months, postoperative dural sac area, and MacNab criteria endpoints (Supplemental Figures S3, and S10 to S14).
Publication Bias and Quality Assessment
The Egger’s test was conducted and showed no indication of publication bias for operation time (intercept = 12.437; 95% CI [−2.39; 27.26]; P = .139) and length of hospital stay (intercept = −0.018; 95% CI [−2.5; 2.46]; P = .989). Additionally, there was no evidence of funnel plot asymmetry (Supplemental Figures S15 and S16).
The included RCT 23 raised some concerns about risk of bias, mainly due to issues related to domain 5 (selection of the reported result) (Supplemental Table S1). In the ROBINS-I assessment, 9 studies6,10,16-18,20-22,24 had a moderate risk of bias, and 1 study 19 showed a serious risk of bias (Supplemental Table S2).
Discussion
In this meta-analysis comprising 1199 patients from 11 studies, we compared the treatment outcomes of uniportal and biportal endoscopic ULBD, a technique often referred to as “over-the-top” decompression, for the treatment of LSS. BE-ULBD demonstrated significantly decreased operation time, ODI at 12 months, and increased postoperative dural sac area compared with UE-ULBD, as well as a higher dural sac area expansion from baseline. No significant differences were observed between the 2 techniques regarding intraoperative blood loss, length of hospital stay, VAS for back pain, leg pain, or ODI at other time points, MacNab criteria, ipsilateral facetectomy angle, and incidence of complications, such as dural tear, infection, postoperative hematoma, lower limb numbness, and nerve root injury.
LSS is a prevalent condition that significantly impacts the global population, particularly among the elderly. 25 With the increasing average age of the population, the incidence of LSS is expected to rise, necessitating effective treatment modalities. Decompression surgery has long been considered the gold standard for alleviating neurogenic claudication symptoms. However, evolving surgical techniques aim to achieve similar or better long-term outcomes while minimizing invasiveness and improving short-term results.26-28 Thus, there is growing interest in minimally invasive techniques for lumbar decompression, but there is limited research into the patient-reported functional outcomes and success evaluation between minimally invasive techniques.29-32
Both BE-ULBD and UE-ULBD were found to be effective in addressing the primary symptoms of LSS. Patient satisfaction, assessed using the MacNab criteria, was high and equivalent between the 2 techniques, reaffirming their clinical utility in minimally invasive spine surgery.10,18,20 Both approaches demonstrated significant improvements in ODI by achieving bilateral decompression. However, BE-ULBD showed superior results in ODI scores at 12 months, alongside a greater increase in postoperative dural sac area and dural sac area expansion. Notably, VAS scores for back and leg pain at the same time point demonstrated a slight but non-significant reduction. This discrepancy may reflect the multifactorial nature of functional recovery in LSS patients, since ODI encompasses broader aspects of postoperative improvement, including mobility and daily activity levels, whereas VAS strictly measures pain intensity. These findings suggest a possible relationship between the enhanced decompression achieved through BE-ULBD and the long-term improvement in functional outcomes. UE-ULBD may present technical challenges, as it requires a steep learning curve and is hindered by instrument limitations. Reasons for the lower canal decompression in UE-ULBD in comparison to that obtained with BE-ULBD may be attributed to the restricted instrument maneuverability and the inherent difficulty in removing bone, as the movement of surgical instruments is largely restricted to linear directions. 6
Interestingly, our pooled analyses demonstrated that the use of BE-ULBD over UE-ULBD was associated with a significantly lower operation time, likely due to technical factors such as the ability to use high-speed drills with greater flexibility and a broader range of surgical instruments. Additionally, the learning curve for BE-ULBD may be less steep, as it closely resembles traditional open surgery, which could help to explain the noted differences in efficiency.10,18 However, the larger size of instruments used in BE-ULBD, especially the high-speed burr, may also result in higher soft tissue disruption, as it does not have to fit through a working channel as with UE-ULBD. This increased disruption, combined with the biportal approach itself, may result in greater muscle detachment and manipulation, which could potentially limit the manipulation ability in smaller spaces such as the neuroforamen. 22 These factors align with previous findings, such as those reported by Choi et al, 33 which demonstrated that unilateral biportal endoscopy (UBE) was associated with significantly higher C-reactive protein (CRP) and creatine phosphokinase (CPK) levels compared to percutaneous endoscopic lumbar discectomy and percutaneous endoscopic interlaminar discectomy. Factors such as the use of high-speed drills, plasma radioablation for hemostasis, and the more extensive preparation of the interlaminar window, which includes some degree of muscle detachment and manipulation, may lead to these elevated inflammatory markers and muscle enzyme levels. However, these physiological changes do not necessarily correlate with increased patient-reported pain. This may explain why no significant differences in postoperative pain scores were detected between the groups, despite the higher CRP and CPK values in UBE.
The incidence of complications is a crucial aspect of minimally invasive spinal surgery. 10 Both BE-ULBD and UE-ULBD demonstrated equivalent safety profiles, with comparable rates of complications such as dural tears, infections, postoperative hematomas, lower limb numbness, and nerve root injuries. This equivalence underscores the safety of both techniques when performed under optimal conditions. However, the incidence of surgical complications may be higher during the learning-curve periods of endoscopic spinal approaches. It is strongly recommended that these procedures be conducted under supervision during the initial learning phases to minimize risks and enhance patient safety. 6
Both BE-ULBD and UE-ULBD represent safe and effective options for the management of LSS. They provide equivalent primary outcomes to open laminectomy while offering the secondary benefits of minimally invasive surgery, such as reduced tissue disruption and faster recovery. The choice between these techniques should be guided by surgeon expertise, available resources, and individual patient characteristics. Training programs involving cadaveric models and the presence of experienced mentors during initial procedures are recommended to enhance proficiency and optimize outcomes for both techniques.
Limitations
Despite these positive findings, this study has some limitations that should be acknowledged. Most of the included studies were retrospective analyses, which are naturally subject to confounding and selection biases. Moreover, the follow-up duration of up to 14 months may be insufficient to capture the long-term efficacy and durability of the 2 techniques. High heterogeneity was noted in some outcomes, which persisted despite sensitivity analyses. Additionally, potential surgeon bias and variability in skill levels could have influenced operative times and patient outcomes. Given that UBE has been described as having a shorter learning curve, the possibility of quicker skill development may have influenced some results. Nonetheless, our study does not account for individual surgeon experience, which is a crucial element in surgical results. Expanding the pool of surgeons and cases could mitigate these biases in future studies. Furthermore, since UBE is a relatively newer technique, the current body of literature is still evolving, and there is a need for more high-quality studies with standardized methodologies to strengthen the available evidence.
Conclusion
In this meta-analysis, BE-ULBD demonstrated significantly decreased operation time, ODI at 12 months, and increased postoperative dural sac area compared with UE-ULBD, as well as a higher dural sac area expansion from baseline. No significant differences were observed between the 2 techniques regarding intraoperative blood loss, length of hospital stay, back pain, leg pain or ODI at other time points, MacNab criteria, ipsilateral angle of facetectomy, and incidence of complications, such as dural tear, infection, postoperative hematoma, lower limb numbness, and nerve root injury. Further large-scale randomized trials with extended follow-up are warranted to confirm these findings and refine the understanding of when each technique may be most appropriately applied.
Supplemental Material
Supplemental Material - Uniportal Versus Biportal Endoscopic Decompression for the Treatment of Lumbar Spinal Stenosis: A Systematic Review and Updated Meta-Analysis
Supplemental Material for Uniportal Versus Biportal Endoscopic Decompression for the Treatment of Lumbar Spinal Stenosis: A Systematic Review and Updated Meta-Analysis by Kaike Lobo, Paweł Łajczak, Numa Rajab, Cláudia Santos, Rafael Reis de Oliveira, Yasmin P. Silva, Eshita Sharma, Yan Gabriel M. D. Silva, Ramon Guerra Barbosa in Party Politics
Footnotes
Author Contributions
All authors contributed to the study conception and design. Study selection was performed by K.L. and C.S. Data collection and analysis were performed by K.L., P.L., R.O., and Y.P.S. The first draft of the manuscript was written by K.L, N.R., E.S., R.B, and Y.S., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.