
Abstract
Study Design
Systematic Review and Meta-analysis.
Objectives
Lumbar degenerative disease (LDD) is prevalent among aging adults. While tubular retraction is a widely used minimally invasive approach, biportal endoscopic spine surgery has emerged as a potential alternative. This systematic review and meta-analysis compares the clinical outcomes of tubular retraction and biportal endoscopy for decompression procedures (discectomy, laminectomy, laminotomy) and transforaminal lumbar interbody fusion (TLIF) in LDD patients.
Methods
A systematic review and meta-analysis of comparative studies was conducted per PRISMA guidelines. A comprehensive search of PubMed, Embase, and Scopus identified relevant studies published before October 7, 2024. Data were analyzed using a random-effects model to assess Oswestry Disability Index (ODI), visual analog scale (VAS) scores for back and leg pain, complication rates, operative time, and length of stay at preoperative, ≤2-weeks postoperative, and ≥1-year postoperative time points.
Results
A total of 772 patients were included (400 tubular, 372 biportal). Biportal endoscopic surgery was associated with a lower complication rate (10.73% vs 15.94%; P < .001) and lower ≤2-week postoperative VAS back pain (2.70 ± 0.27 vs 3.55 ± 0.49; P < .001) relative to tubular spine surgery. Biportal decompression had a lower complication rate (15.13% vs 22.34%; P = .006) but similar patient-reported outcomes. Biportal TLIF had longer operative times (189.93 ± 25.90 vs 145.1 ± 14.90 min; P = .026) but lower complication rates (6.33% vs 9.55%; P = .026) and ≥1-year VAS leg pain (1.88 ± 0.29 vs 2.02 ± 0.26; P < .001).
Conclusions
Biportal endoscopy for LDD had lower complication rates and similar patient-reported outcomes relative to tubular retraction, though longer operative times in TLIF subanalysis. Future studies are necessary to validate findings and guide patient-specific decision-making.
Introduction
As the population ages with increasing activity demands, the incidence of lumbar degenerative disease (LDD) is rising, with over 90% of adults over the age of 60 exhibit radiographic signs of LDD. 1 This condition can manifest clinically as lumbar disc herniation (LDH), lumbar spinal stenosis (LSS), and facet and disc degeneration. When conservative treatments fail to provide relief, decompressive surgical interventions such as discectomy, laminectomy, laminotomy, or fusion are indicated.2,3 Recent surgical management of LDD has shifted towards minimally invasive spine surgery (MISS) techniques, utilizing instruments such as tubular retractors or endoscopy systems to minimize soft tissue damage, preserve the integrity of paraspinal musculature, decrease blood loss, lower postoperative pain and infection rate, and accelerate overall postoperative recovery.4-6 While there has been significant clinical progress in the development, clinical utilization, and success of MISS techniques, the benefits of individual minimally invasive techniques must be contextualized with their potential drawbacks: higher economic burden, increased radiation exposure, lack of tactile feedback, decreased ability to treat certain intraoperative complications, and the additional learning curve that surgeons must undertake to master the technique.7-10
A major milestone in the evolution of MISS began with tubular access to the lumbar disc, which was first reported by Faubert and Caspart in 1991. 11 This paved the way for the development of modern tubular retractor systems and other minimally invasive instruments. 12 More recent lumbar spine literature on MISS techniques has heavily focused on the uniportal and biportal endoscopic approaches.13-15 The uniportal approach utilizes a singular portal and has been associated with fewer complications, quicker recovery times, and reduced postoperative pain.16,17 The biportal approach, on the other hand, uses a separate “working” portal and “viewing” portal, which may be advantageous in improving the maneuverability and widening the visualized surgical field - effectively combining the benefits of the uniportal approach and traditional open surgery. 18
Despite the rapid advances in minimally invasive lumbar spine surgery, there is a lack of consensus on how newer endoscopic approaches, such as biportal endoscopy, compare to older MISS developments. As such, the present systematic review and meta-analysis aims to elucidate differences in biportal endoscopic vs tubular-access approaches to lumbar discectomy, laminectomy and laminotomy, and transforaminal lumbar interbody fusion (TLIF).
Methods
Search Strategy
For the present review, PubMed (MEDLINE), Embase, and Scopus databases were searched according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and Cochrane Review recommendations, aiming to find all related articles published before October 7th, 2024. Keywords, synonyms, and variations of the terms “endoscopic spine surgery,” “lumbar,” “discectomy,” “laminectomy,” “laminotomy,” and “fusion” were queried in various Boolean combinations. To ensure comprehensive coverage, the reference lists of all included articles were reviewed to identify any additional relevant studies. The complete search string is provided in the supplemental materials.
Selection Criteria
This systematic review and meta-analysis included comparative studies evaluating patients diagnosed with LDD who underwent biportal endoscopic spine surgery in comparison to tubular spine surgery. To be eligible, studies needed to be an original study comparing biportal endoscopic spine surgery and tubular spine surgery clinical outcomes for the treatment of LDD. In addition, the study must report at least one of the following outcomes: visual analog scale (VAS) scores for back and leg pain, Oswestry Disability Index (ODI), complication rates, operative duration, or hospital length of stay. Only English-language studies published in peer-reviewed journals qualified for inclusion.
Studies were excluded if they included patients with fractures, tumors, infections, or scoliosis, to maintain a focus on treatment of LDD. Non-comparative studies were excluded to minimize heterogeneity and confounding effects of study designs and patient populations. Additionally, case reports, reviews, conference abstracts, and letters were not considered. Articles missing essential outcome data, such as means and standard deviations, were also excluded.
Study Screening and Data Extraction
Two reviewers independently screened the identified studies based on their titles, abstracts, and full texts, adhering to the inclusion and exclusion criteria. Any disagreements were resolved by a third reviewer, and reasons for study exclusion were documented. Final confirmation of the included studies was provided by the senior author.
Data extraction was carried out independently by the reviewers using standardized forms. Extracted information included study characteristics (e.g., authorship, publication year, study design, sample size, age distribution, and sex ratio) as well as reported outcomes (VAS scores for back and leg pain, ODI, operative time, hospital stay duration, and complication rates).
Risk of Bias Assessment
The methodological quality of non-randomized studies was evaluated using the Newcastle-Ottawa Scale (NOS), which assesses 3 domains: selection, comparability, and outcomes. 19 Each study could achieve a maximum score of 9. Studies scoring between 5 and 9 were classified as having a lower risk of bias, while those scoring below 5 were deemed to have a higher risk. Any discrepancies between reviewers were resolved by a third reviewer.
Statistical Analysis
Clinical outcomes such as operative time, length of hospital stay (LOS), VAS scores, and ODI were compared between tubular and biportal surgery groups. Subgroup analyses were conducted for decompression (discectomy, laminectomy, laminotomy) and fusion procedures. Mean values for subgroups and overall totals were calculated by pooling means and standard deviations from individual studies, following Cochrane’s Handbook for Systematic Reviews of Interventions.
P-values for differences between the tubular and biportal cohorts were calculated using Cohen’s d effect size within a random-effects model. This model accounted for variability in patient populations and surgical techniques, enhancing the generalizability of findings. The control group included patients who underwent tubular spine surgery, while the biportal group served as the treatment cohort.
Clinical outcomes were categorized into 0-2 weeks postoperative and ≥1-year postoperative periods, ensuring consistency with prior research and minimizing temporal variability. For instances in which a study reported outcomes at multiple time periods within the ≤2-week or ≥1-year postoperative windows, only outcomes at the latest follow-up time point within the respective window were included to maximize consistency in outcome categorization. Effect sizes were calculated as differences in standard deviations between biportal and tubular approaches. Cochran’s Q-test and I2 statistics were used to determine heterogeneity. Statistical significance was set at a P-value <.05. Data analysis was performed using IBM SPSS Statistics version 29.0.
Results
Search Results
The initial database searches yielded 757 studies after removing duplicates. Following the title and abstract screening, 456 studies were excluded. The remaining 301 full-text reports were assessed, with 9 studies deemed suitable for inclusion in the final analysis. A PRISMA flow chart detailing the screening process and literature search outcomes is displayed in Figure 1. PRISMA Flow Chart of the Study Selection Process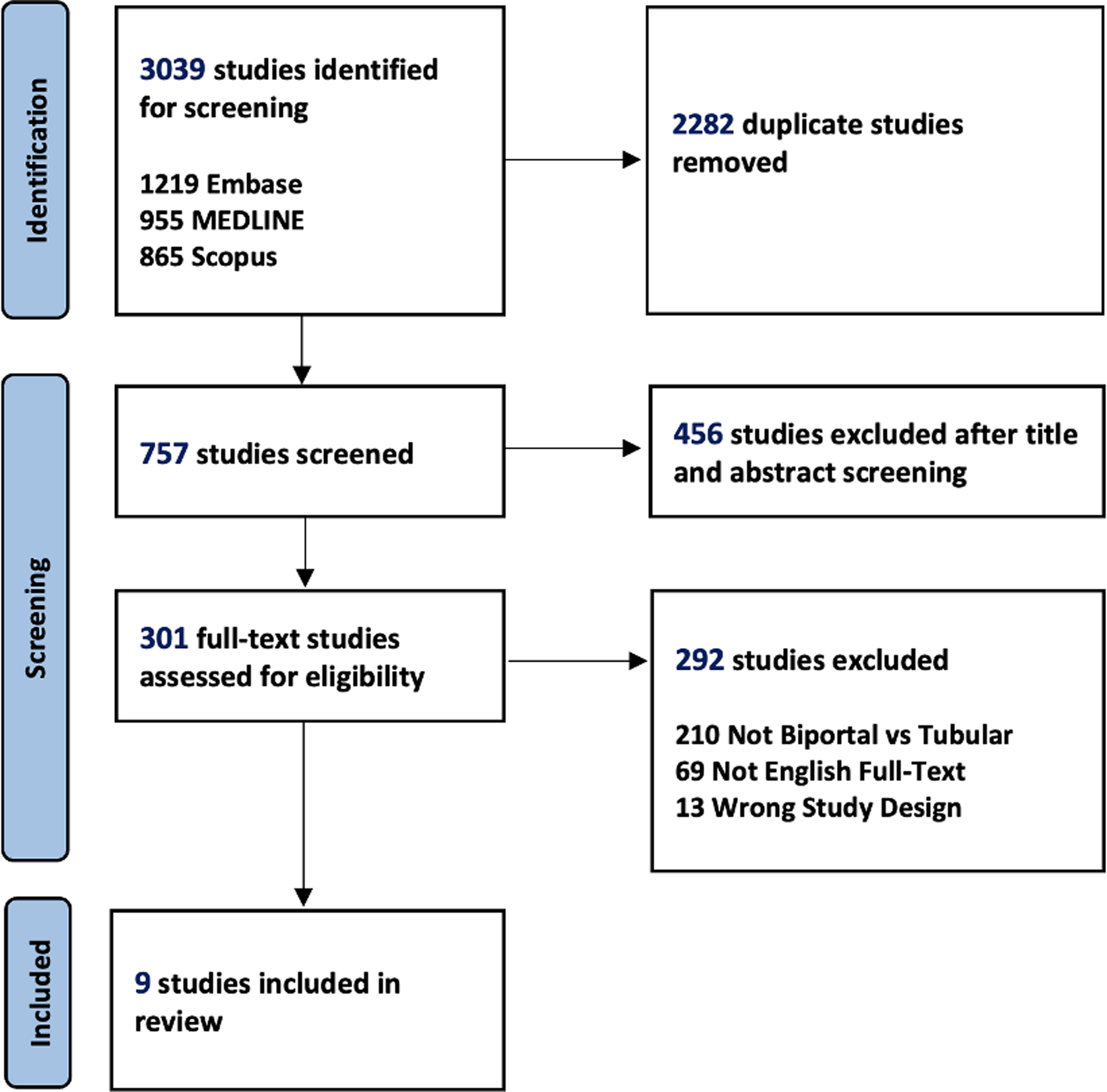
Characteristics of Comparative Studies on Tubular Retracted vs Biportal Endoscopic Lumbar Spine Surgery
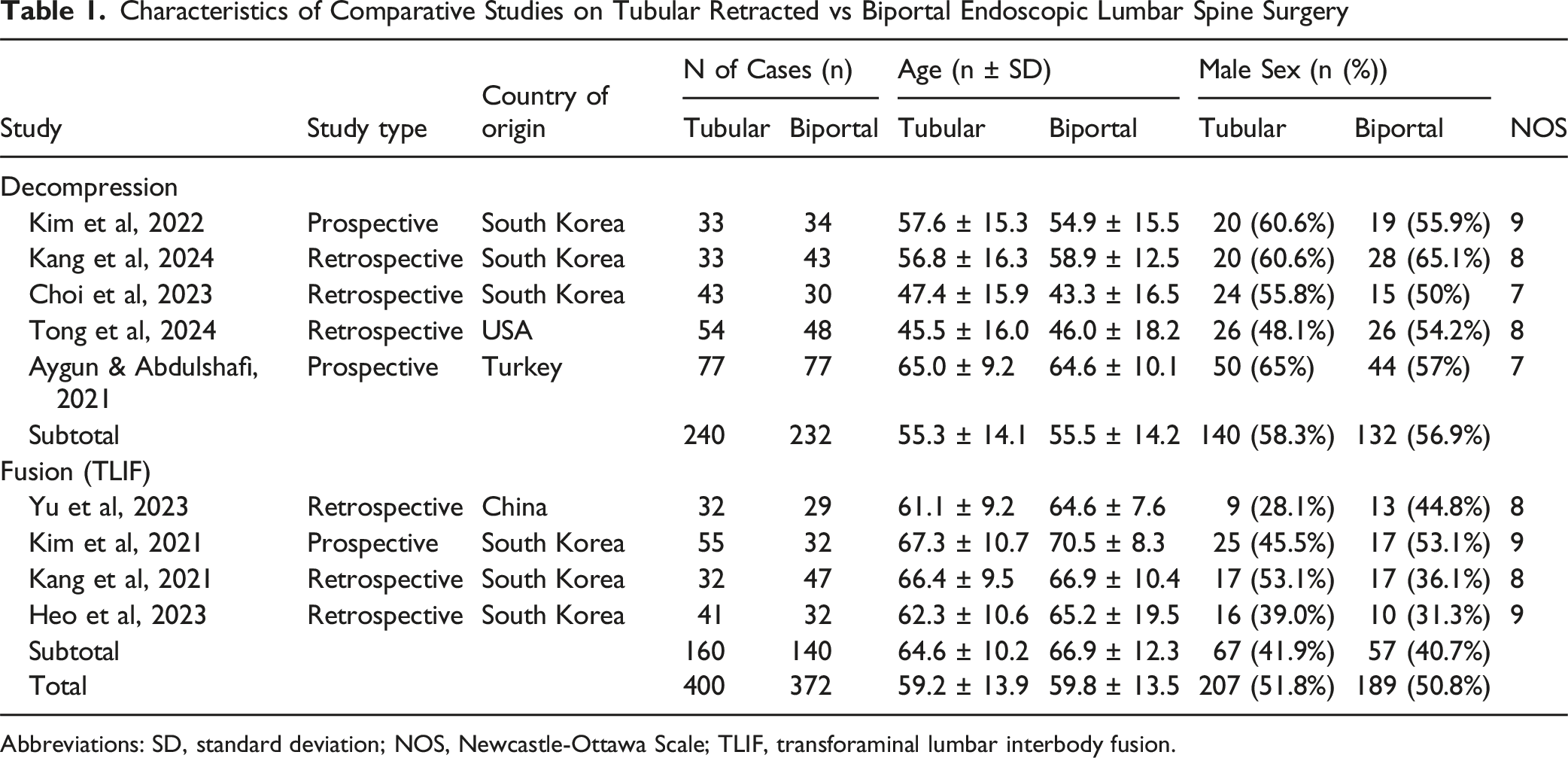
Abbreviations: SD, standard deviation; NOS, Newcastle-Ottawa Scale; TLIF, transforaminal lumbar interbody fusion.
Overall Outcomes
Clinical Outcomes of Patients Undergoing Tubular Retracted vs Biportal Endoscopic Lumbar Spine Surgery
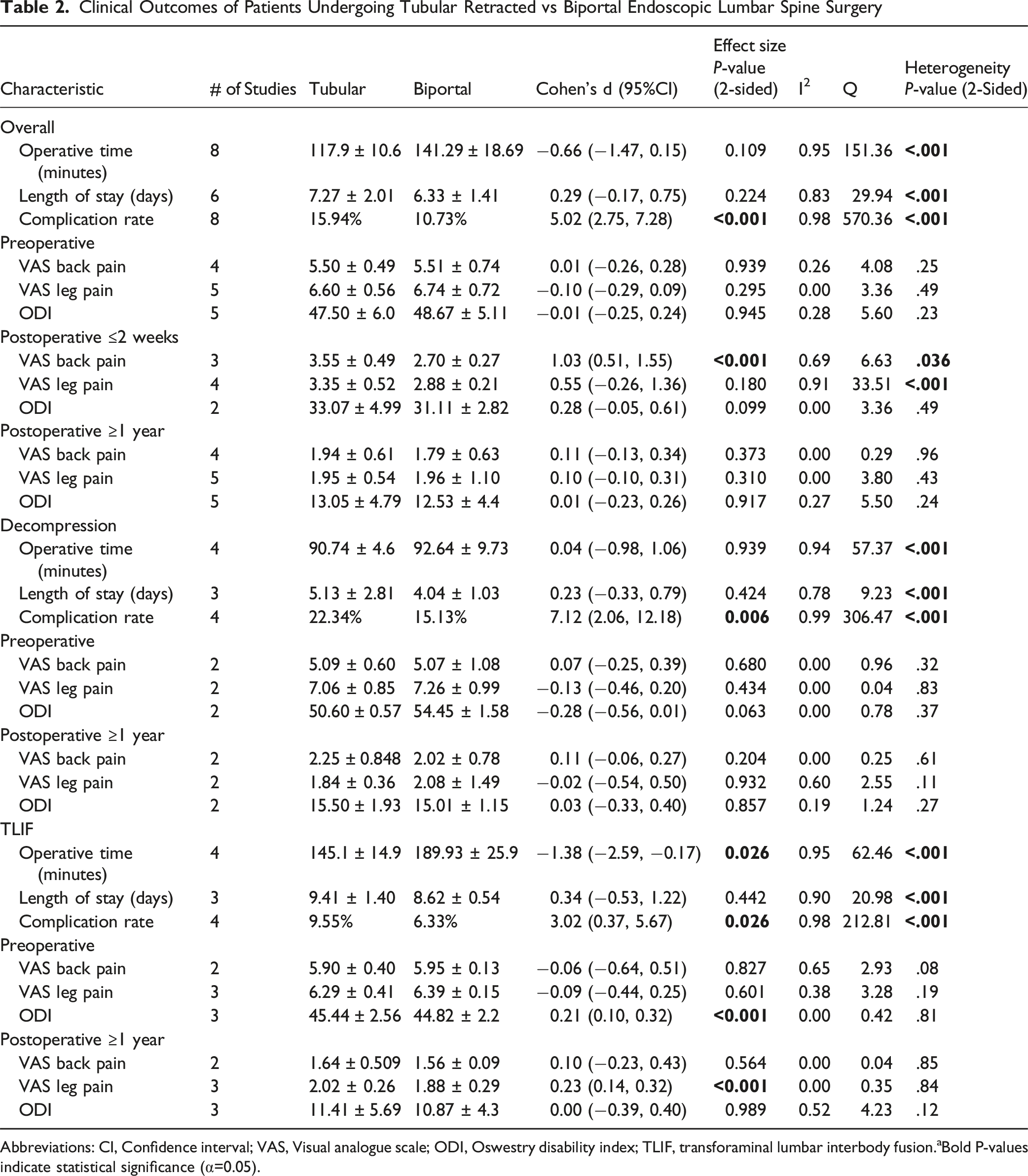
Abbreviations: CI, Confidence interval; VAS, Visual analogue scale; ODI, Oswestry disability index; TLIF, transforaminal lumbar interbody fusion.aBold P-values indicate statistical significance (α=0.05).
Breakdown of Complications Between Tubular Retracted vs Biportal Endoscopic Spine Surgery
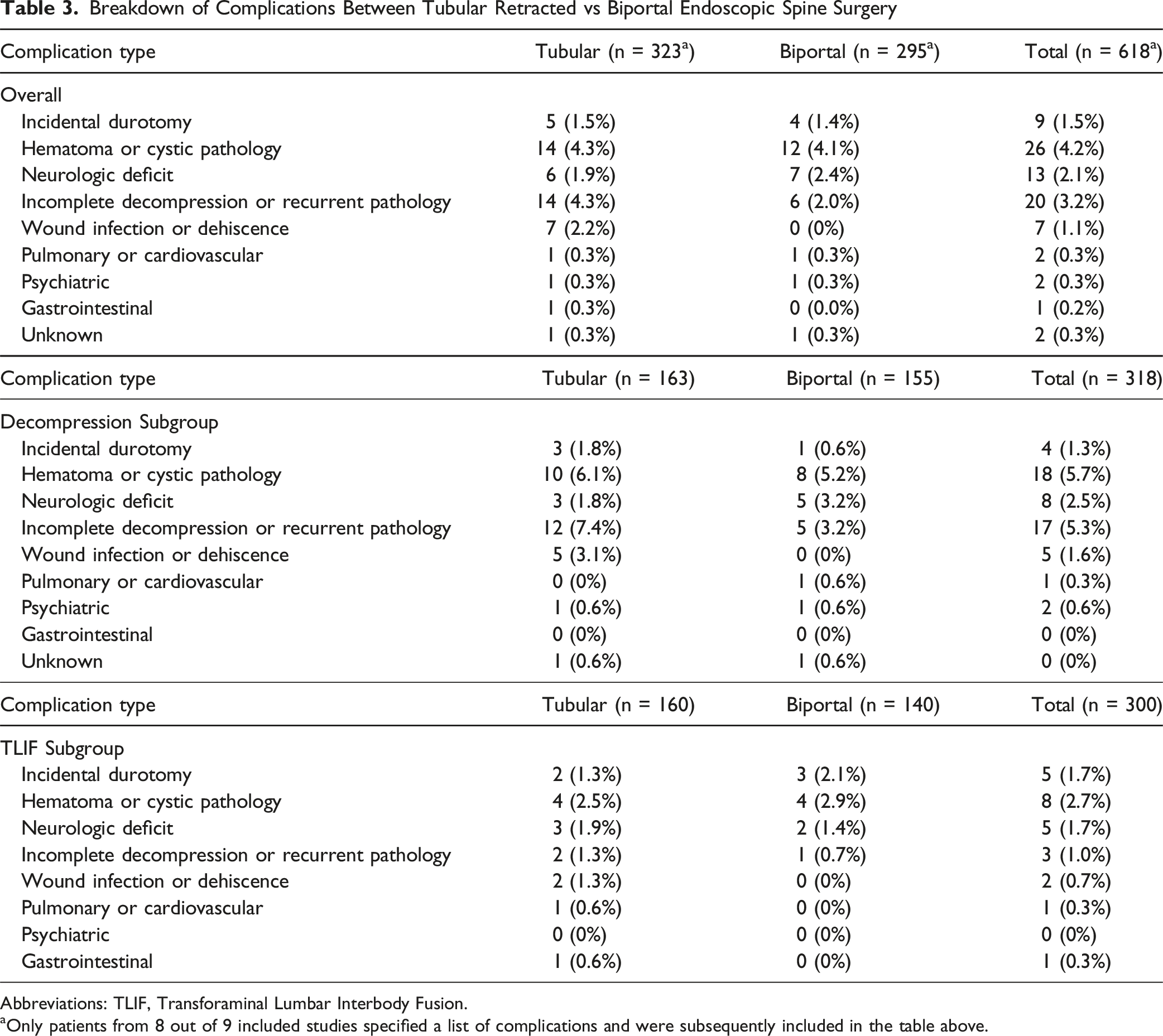
Abbreviations: TLIF, Transforaminal Lumbar Interbody Fusion.
aOnly patients from 8 out of 9 included studies specified a list of complications and were subsequently included in the table above.
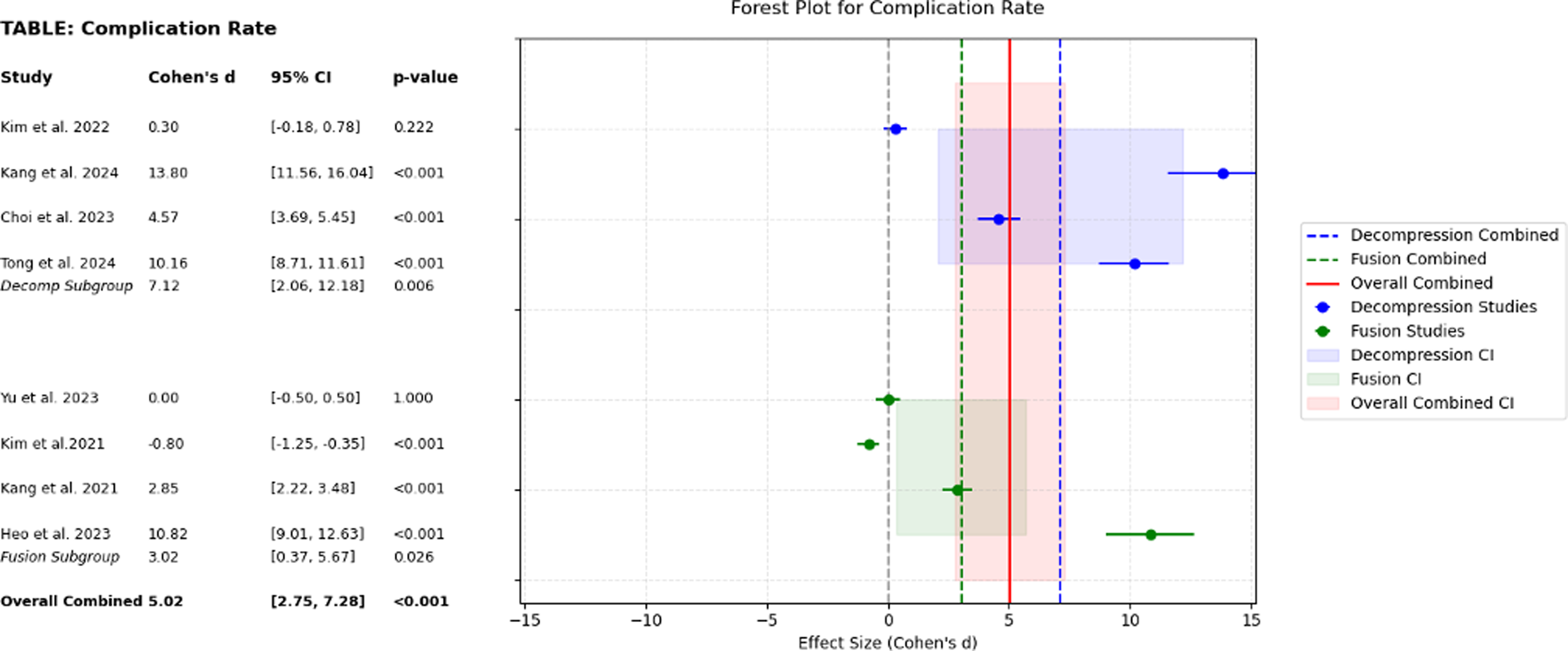
Forest Plot on the Effect of Tubular Retracted vs Biportal Endoscopic Spine Surgery on Complication Rate
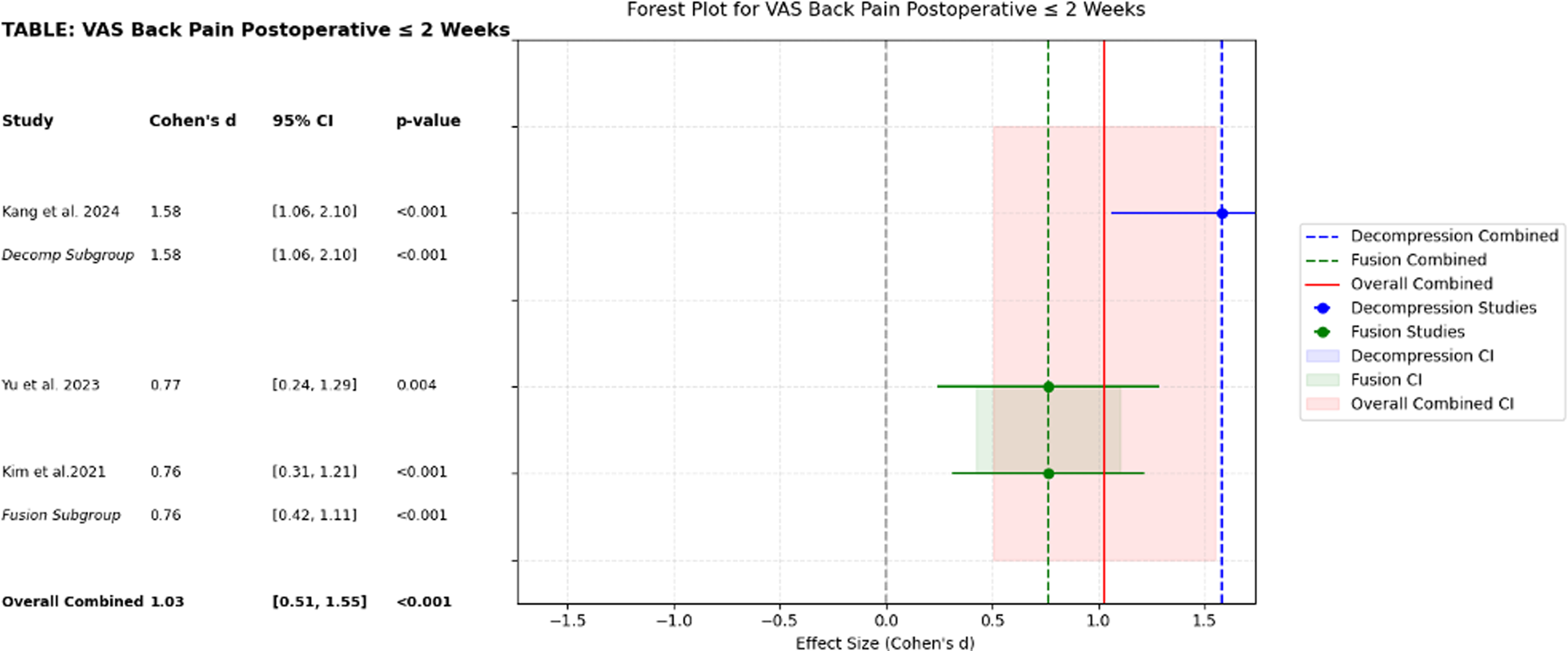
Forest Plot on the Effect of Tubular Retracted vs Biportal Endoscopic Spine Surgery on ≤2-Week Visual Analogue Scale Back Pain
Tubular v. Biportal Decompression
A subgroup analysis was performed on the 5 studies specific to decompression, with a total of 240 tubular and 232 biportal patients. The tubular cohort had a mean age of 55.3 ± 14.1 years and consisted of 140 (58.3%) males. The biportal cohort had a mean age of 55.5 ± 14.2 years and consisted of 132 (56.9%) males (Table 1). Cohen’s d effect size measure demonstrated there was a significantly greater complication rate of 22.34% in the tubular cohort compared to 15.13% in the biportal cohort (d = 7.12 [2.06, 12.18], P = .006) (Table 2). There were no significant differences in operative time or LOS, or in VAS back pain, VAS leg pain, or ODI preoperatively or at ≥1-year postoperatively. Clinical outcomes for the decompression subgroup analysis are summarized in Table 2. Heterogeneity analysis found significant variation between studies for operative time (I2 = 0.94, Q = 57.37, P < .001), length of stay (I2 = 0.78, Q = 9.23, P < .001), and complication rate (I2 = 0.99,Q = 306.47, P < 0.001).
Tubular v. Biportal TLIF
Summary of Advantages and Disadvantages of Tubular Spine Surgery Versus Biportal Endoscopic Spine Surgery for Lumbar Degenerative Disease.
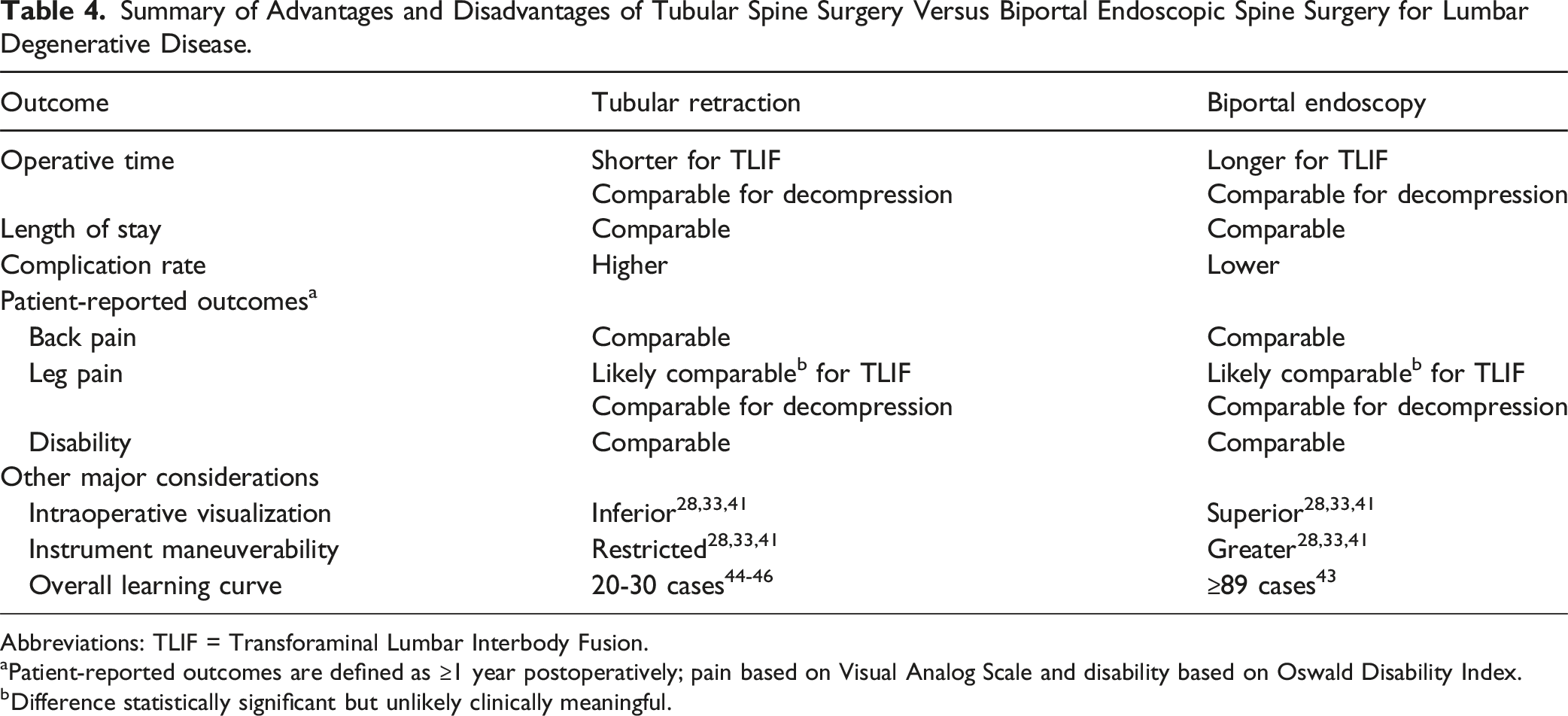
Abbreviations: TLIF = Transforaminal Lumbar Interbody Fusion.
aPatient-reported outcomes are defined as ≥1 year postoperatively; pain based on Visual Analog Scale and disability based on Oswald Disability Index.
bDifference statistically significant but unlikely clinically meaningful.
Discussion
Over the past several decades, MISS has rapidly expanded to include tubular and endoscopic techniques designed to preserve paraspinal muscle integrity, minimize soft tissue damage and blood loss, and enhance postoperative recovery and outcomes in the surgical treatment of LDD.4,29,30 The more recent development in endoscopic technique is the biportal approach, which utilizes a separate viewing and working portal in an effort to improve maneuverability and widen the visual field to facilitate an improved learning curve and minimize complications.13,31 However, there is a lack of consensus in the MISS literature on how the biportal technique compares to more conventional tubular retraction for the treatment of lumbar spine degenerative pathologies. As such, the aim of this systematic review and meta-analysis was to investigate overall perioperative characteristics and postoperative outcomes of tubular retraction vs biportal endoscopy in lumbar decompression and fusion procedures for the treatment of LDD. An overall comparison of tubular vs biportal endoscopy demonstrated significant differences in complication rate and ≤2-week postoperative VAS back. Tubular vs biportal decompression subanalysis similarly demonstrated a significant difference in complication rate. Tubular vs biportal TLIF subanalysis demonstrated significant differences in operative time, complication rate, preoperative ODI, and ≥1-year postoperative VAS leg pain.
The overall analysis demonstrated significantly lower values in VAS back pain 2 weeks postoperatively in the biportal approach compared to the tubular approach. This finding aligns with those of Heo et al, who reported biportal and uniportal endoscopic approaches were associated with superior 1 day postoperative VAS back pain scores relative to the tubular approach. 32 Biportal endoscopy showed significant improvement at the same time points in VAS back pain and ODI scores, but both approaches showed similar ODI and VAS scores at the 12 month follow-up time point. 33 Additionally, tubular retraction was associated with a significantly higher complication rate relative to the biportal endoscopic approach. Previous studies have proposed several reasons for this increased rate.34-36 For example, He et al suggested tubular retractors are associated with increased direct ischemic injury due to the high tissue pressures imposed by a small diameter retractor system. In contrast, the contralateral muscle group is preserved bilaterally in the biportal endoscopic approach, preventing ischemic muscle injury and thus decreasing the overall complication rate.37,38
In the current study, tubular vs biportal endoscopic decompression subanalysis demonstrated biportal decompression was associated with a significantly lower complication rate. Ito et al. similarly demonstrated fewer postoperative complications with biportal laminectomy vs tubular-assisted microscopic laminectomy. 39 Specifically, the microscopic technique resulted in complications such as hematoma, paralysis, dura injury, and reoperation. In addition, the biportal approach to laminectomy demonstrated a decreased bone resection area and was associated with a superior facet preservation rate relative to the tubular approach. As such, by requiring less bone resection and thus minimizing both surgical trauma and intraoperative bleeding, the biportal approach may facilitate a smoother perioperative surgical experience and postoperative patient recovery.
Interestingly, regarding the tubular vs biportal endoscopic TLIF subanalysis, we found biportal TLIF was associated with higher operative time than tubular TLIF. Prior literature has postulated that this increased operative time may be due to certain requirements in the biportal endoscopic technique, such as the setup and careful maintenance of constant irrigation outflow, precise implementation of 2 separate portals, and progressive manipulation of the musculature required to access the surgical site with the endoscope and surgical instruments.36,38 Biportal TLIF was also found to result in lower ≥1-year VAS leg pain scores and lower preoperative ODI compared to tubular TLIF. This contrasts a prior meta-analysis from Alostaz et al, which demonstrated biportal and minimally invasive techniques had no significant differences in 3-month and final postoperative ODI. 37 Although we found that biportal TLIF was associated with statistically lower preoperative ODI and ≥1-year postoperative VAS leg pain compared to tubular TLIF, the absolute differences were small (<1 point) and unlikely to reflect a meaningful change in patient symptoms. This highlights the importance of distinguishing statistical from clinical significance, particularly when evaluating patient-reported outcomes. Future randomized trials are needed to determine whether these modest numerical differences correspond to tangible benefits in real-world settings. Nevertheless, as with the overall analysis and decompression subanalysis, the biportal TLIF complication rate was significantly lower than in tubular TLIF, which may be the result of less soft tissue and muscle trauma, in addition to lower blood loss and thus improved visual visualization relative to tubular TLIF. 26
Differences in the learning curves of the 2 approaches must also be considered. Overcoming the steep learning curve in minimally invasive spine surgery is essential, as it contributes to shorter operative times, reduced length of stay (LOS), and fewer complications, thereby lowering costs and promoting better patient recovery outcomes. 40 Although the biportal endoscopic approach provides clearer visualization and improved postoperative outcomes than the tubular approach,28,33,41 it also requires coordination of both depth and direction of the endoscope and surgical instruments by spine surgeons. 42 The requirement of 2 surgical channels intrinsic to the biportal approach, along with continuous saline irrigation and pressure maintenance, presents a considerable learning curve for surgeons and the need for careful intraoperative maneuvering, especially in the early stages of mastering this procedure. 31 A prior study demonstrated that surgeons require experience with at least 89 cases involving the biportal endoscopic approach before passing the ‘learning stage’ and achieving a reproducible success rate. 43 In contrast, studies report surgeons typically surpass the learning stage for the tubular retraction technique after performing around 20-30 cases.44-46 Despite the potentially steeper learning curve associated with biportal endoscopic spine surgery, Kim et al. reported surgical failure using the biportal endoscopic approach is dramatically reduced from 10.29% to 5.60% after surgeons bypass the learning stage of skill. 47 Overall, while we demonstrated the biportal approach is associated with increased operative time in TLIF, along with a potentially steeper learning curve, 48 our findings also suggest spine surgeons who master the biportal endoscopic technique may be able to minimize postoperative complications across both decompression and fusion procedures relative to the tubular approach.
A major finding in this meta-analysis is LOS on the order of several days. It should be noted longer LOS times across both tubular and biportal approaches is most likely attributed to the fact that many of the included studies in this analysis originate from Asia, where healthcare systems often adopt practices that emphasize longer inpatient care compared to the United States.49,50 Increased length of stay in these regions may be influenced by cultural norms, healthcare policies, and differences in postoperative management strategies. 51 While these practices provide valuable insights into extended recovery and monitoring, they may not fully correspond with the increasing emphasis on ambulatory surgery and same-day discharge efforts in the United States. 52 As ambulatory surgery and rapid postoperative discharge become more prevalent in the United States, largely due to advancements in surgical techniques, anesthesia, and postoperative care, it is essential to evaluate outcomes specific to this trend. As such, future studies should focus on outcomes specific to ambulatory surgery for tubular and biportal approaches to inform clinical decision-making and guide perioperative care protocols tailored to the shifting American healthcare paradigm. 53
Strengths and Limitations
There are noteworthy strengths to this meta-analysis. For example, despite the lack of RCTs in the literature on this subject, the results were generally consistent across included studies and were supported by high NOS scores, which indicates high quality of the included non-randomized studies. In addition, given the observed heterogeneity, a random-effects model was used for all pooled analyses. This approach was chosen because it accounts for both within-study error and between-study differences, offering more conservative and generalizable estimates across diverse clinical settings. Furthermore, the authors minimized potential biases through an extensive literature search utilizing 3 robust databases with independent review and rigorous full-text screening with respect to inclusion and exclusion criteria. Finally, this meta-analysis is novel in quantifying and presenting the first comprehensive summary of comparative lumbar spine surgery literature detailing tubular retraction vs biportal endoscopy in both decompression and fusion procedures.
However, this study is not without limitations. First, no randomized controlled trials comparing biportal and tubular techniques were identified, which limits our ability to infer causality and introduces potential for residual confounding despite use of comparative study designs. Second, selection bias at the meta-analysis level may have occurred, as our inclusion criteria favored published full-text, English-language, comparative studies. This may have excluded studies with less favorable or non-significant results, potentially skewing the pooled estimates. Third, surgical protocols were inconsistently described, with limited reporting of intraoperative details such as portal placement, facet resection technique, irrigation use, and imaging guidance, restricting procedural comparability. Fourth, surgeon experience and case volume were not reported in most studies. Given the known learning curve differences between techniques, this unmeasured variable could contribute to heterogeneity in operative time and complication rates. Fifth, although a comprehensive database search was performed, publication bias remains possible. Studies with non-significant results may be underrepresented, and the exclusion of non-English articles may have further narrowed the scope of the included literature.
Finally, although all studies included in this analysis were comparative in nature to biportal and tubular approaches within their own patient populations and thus minimize potential bias within each study, some degree of heterogeneity was expected and confirmed across the included studies. Cochran’s Q-test and I2 statistics showed substantial variability for several outcomes, particularly operative time and complication rate (I2 > 90%). The observed heterogeneity across outcomes likely stems from several interacting factors. These include technical variability in the application of biportal and tubular techniques (e.g., retractor size, portal positioning, irrigation strategy), differences in surgeon experience and case volume, and variability in patient pathology (e.g., disc herniation, spondylolisthesis, osteoporosis). In addition, institutional variation in perioperative management and discharge protocols across international healthcare systems may contribute to differences in outcomes such as length of stay. The lack of standardized surgical protocols and the retrospective nature of the included studies further confound interpretation. Although we performed subgroup analyses for decompression and TLIF to explore potential sources of variability, further sensitivity analyses such as leave-one-out analysis or influence diagnostics were considered but ultimately not performed provided the limited number of included studies (n = 9), and thus the risk of overfitting the data. Therefore, we acknowledge this as a methodological limitation and emphasize the need for future meta-analyses with larger study pools to enable more robust exploration of heterogeneity. Collectively, these factors limit the generalizability of our pooled estimates and underscore the need for future randomized, standardized, and multicenter trials.
Future Directions
Future research should prioritize prospective, multicenter randomized controlled trials (RCTs) to validate the findings of this study and clarify the comparative effectiveness of biportal vs tubular approaches. Standardization of surgical techniques, perioperative care protocols, and follow-up duration will be essential to reduce heterogeneity. In addition, future studies should include cost-effectiveness analyses, outpatient and ambulatory outcomes, and stratification by patient demographics and comorbidities (e.g., obesity, osteoporosis) to better inform clinical decision-making.
Conclusions
This meta-analysis compares biportal endoscopy and tubular retraction techniques in the management of lumbar degenerative disease. Biportal endoscopy was associated with lower complication rates, but also longer operative times for TLIF, and may involve a steeper learning curve. Both approaches yielded similar patient-reported outcomes. As patient-specific factors such as obesity or osteoporosis may influence the optimal surgical approach, further randomized trials are warranted to validate these findings and guide patient-specific decision-making.
Supplemental Material
Supplemental Material - Comparison of the Biportal Endoscopic Versus Tubular Approach for the Treatment of Lumbar Degenerative Disease: A Systematic Review and Meta-Analysis
Supplemental Material for Comparison of the Biportal Endoscopic Versus Tubular Approach for the Treatment of Lumbar Degenerative Disease: A Systematic Review and Meta-Analysis by Mark Kurapatti, Alexander Yu, Hamza Ahmed, Charu Jain, Ryan Hoang, Gray W. Ricca, Junho Song, Daniel Berman, Joshua Lee, and Samuel K. Cho in Global Spine Journal
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Samuel K. Cho, MD, FAAOS, AAOS: Board or committee member, American Orthopaedic Association: Board or committee member, AOSpine North America: Board or committee member, Cervical Spine Research Society: Board or committee member, Globus Medical: IP royalties and Fellowship support, North American Spine Society: Board or committee member, Scoliosis Research Society: Board or committee member, Stryker: Paid consultant, The remaining authors have no conflicts of interest or sources of support that require acknowledgment.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.