
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare the outcomes of C2 dome-like laminoplasty (C2-Dom LP) and C2 laminectomy with fusion (C2-LF) in patients with C2-involving ossification of the posterior longitudinal ligament (OPLL) and to identify radiological predictors that guide optimal surgical selection.
Methods
A retrospective analysis of 143 patients (C2-Dom LP, 71; C2-LF, 72) was performed. Radiological evaluations were C2 cross-sectional area (CSA), cervical range of motion (ROM), canal-occupying ratio, and sagittal alignment parameters. Clinical outcomes were assessed using Japanese Orthopedic Association (JOA) scores, neck disability index, and visual analog scale. Subgroup analysis was conducted according to canal compromise severity. A propensity-matched analysis using demographic and perioperative variables was performed to ensure an unbiased comparison.
Results
After propensity-matched analysis, C2-Dom LP preserved cervical ROM and sagittal alignment, whereas C2-LF produced substantially greater canal expansion. Both groups demonstrated clinical improvement, but C2-LF achieved a significantly higher JOA recovery rate following matching, highlighting its superior neurological benefit. In the high-compromise subgroup, defined by a CSA cutoff of 92.24 mm2, C2-LF yielded markedly better neurological recovery than C2-Dom LP. Logistic regression identified smaller CSA, larger sagittal vertical axis, and lower baseline JOA score as independent predictors of poorer outcome.
Conclusions
C2-Dom LP preserved motion and alignment and can be effective for standard-risk patients. C2-LF achieved greater canal expansion and better recovery in high-compromise patients. A CSA-based, risk-stratified approach could improve with adoption of this threshold, potentially enhancing surgical decision-making and the long-term outcomes of patients with C2 involvement OPLL.
Keywords
Introduction
Ossification of the posterior longitudinal ligament (OPLL) involves the formation of heterotopic bone and leads to progressive cervical canal stenosis and myelopathy.1-3 OPLL at the C1-2 level is uncommon, accounting for less than 5% of cases. 4 Because the spinal canal is widest at C1 and narrows toward C3-4, OPLL involving C2 often presents as long, thick ossified segments that extend into the narrower canal, typically at C3-4. As C2-involving OPLL can differ in surgical outcomes and clinical significance from that at other levels, it presents unique diagnostic and therapeutic challenges, and more research is needed to optimize surgical strategies and improve patient outcomes.
Anterior decompression for C2-involving OPLL, such as total corpectomy through a combined transoral and upper cervical approach, followed by posterior occipitocervical fusion is technically demanding and carries significant risks.5,6 Consequently, most patients undergo posterior decompression, including laminoplasty (LP) or laminectomy with fusion (LF). 7 A dome-like or double-dome LP spares the C2 lamina, preserving the insertions of the semispinalis cervicis (SSC), reducing postoperative neck pain and maintaining cervical alignment. 7 However, some researchers have noted that patients with severe stenosis, extensive OPLL extending behind C2, or a long life expectancy require fusion surgeries because C2-sparing LP can lead to inadequate decompression and OPLL progression, which complicate revision surgery.8,9 The decision to perform C2-sparing LP or C2 laminectomy with fusion (C2-LF) remains controversial.
Previous studies on C2-involving OPLL have been limited to small series. 10 For this study, we conducted a comparative analysis of C2 dome-like laminoplasty (C2-Dom LP) and C2-LF to evaluate surgical strategies for optimizing neurological recovery and functional outcomes. To the best of our knowledge, this is the first study to directly compare these 2 procedures specifically in patients with OPLL involving the C2 segment.
This retrospective study compares the clinical and radiological outcomes of C2-Dom LP and C2-LF in patients with cervical myelopathy caused by C2-involving OPLL. Additionally, we evaluate the relationships between cervical radiological parameters and neurological recovery, particularly in high-compromise (HC) patients at risk of poor outcomes.
Materials and Methods
Patient Demographics
This retrospective cohort study included 880 patients who underwent surgery for cervical OPLL at 1 of 2 university-affiliated hospitals between January 2013 and December 2022. Diagnosis was established through cervical spine radiography and computed tomography (CT), and demographic details, including sex and age, were obtained from the hospital medical records.
The inclusion criteria were (1) surgical treatment for cervical OPLL involving C2; (2) posterior decompression with C2-Dom LP or C2-LF; (3) radiographic CT confirmation that OPLL extended beyond the mid-C2 lamina; and (4) ≥24 months of clinical and radiological follow-up. The exclusion criteria were (1) prior cervical surgery; (2) traumatic spinal cord injury; (3) neoplasm; (4) infection; (5) combined anterior and posterior staged surgery; and (6) other neurological disorders. Among the 672 posterior cases, 143 met all the inclusion criteria and completed their follow-up (Figure 1). Our study protocol was approved by our institutional review board (IRB No. 9-2023-0207), which waived the need for patient consent because of the retrospective design. This study adhered to the Declaration of Helsinki. Flowchart of patient selection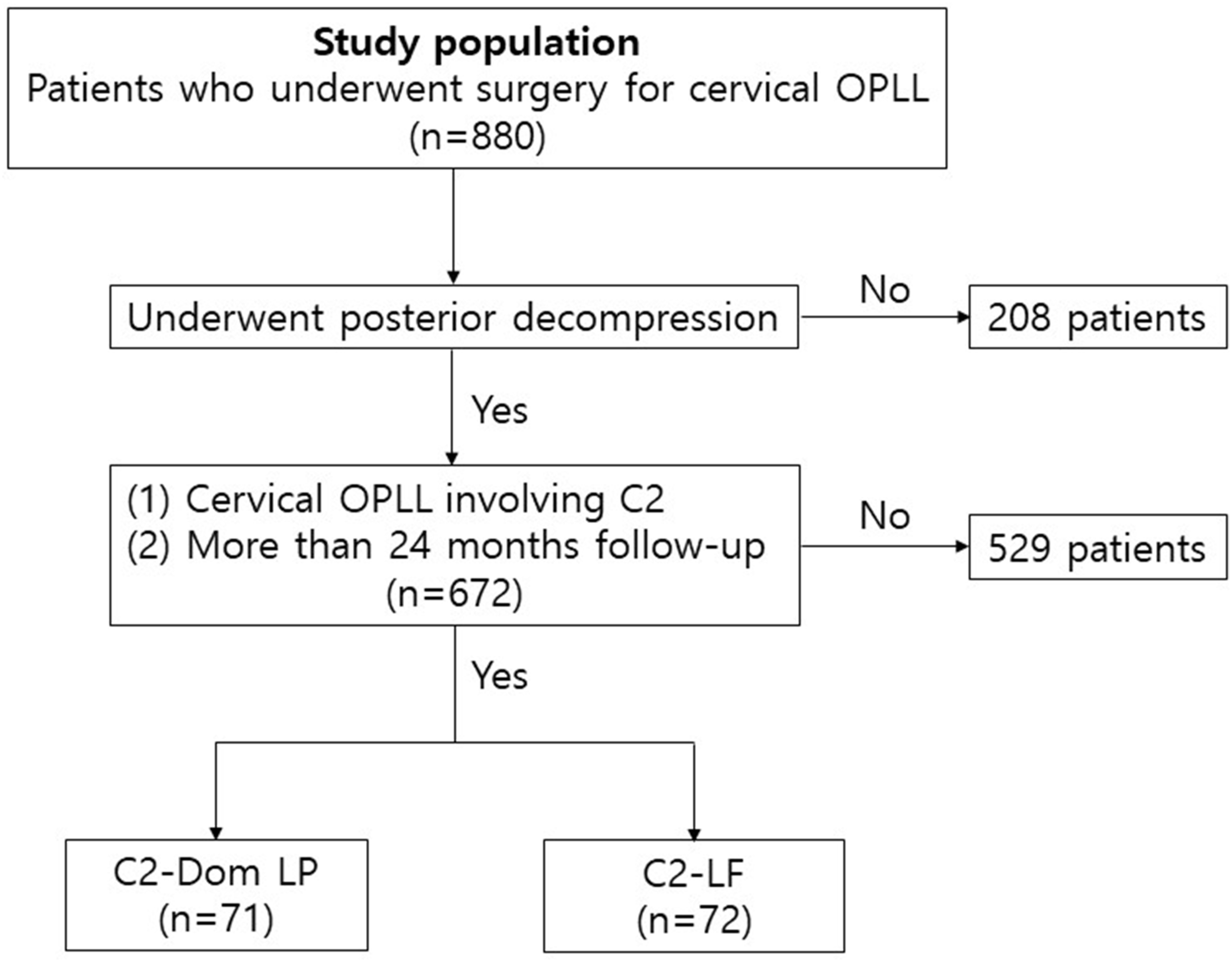
Surgical Procedures
Under intraoperative neurophysiological monitoring, a standard midline posterior skin incision was created from C2 to the affected levels. The paraspinal muscles were dissected laterally to expose the posterior elements.
C2-Dom LP
In the C2-Dom LP procedure, an arc-shaped resection of the dorsal C2 lamina beneath the lower margin of the spinous process was performed using a high-speed drill under a microscope. The ligamentum flavum was removed until adequate decompression was achieved, with dorsal resection extended to the C2 lamina cranial margin as necessary. Excessive cortical removal was avoided to prevent C2 spinous process fractures (Figure 2). Technique of C2-Dom LP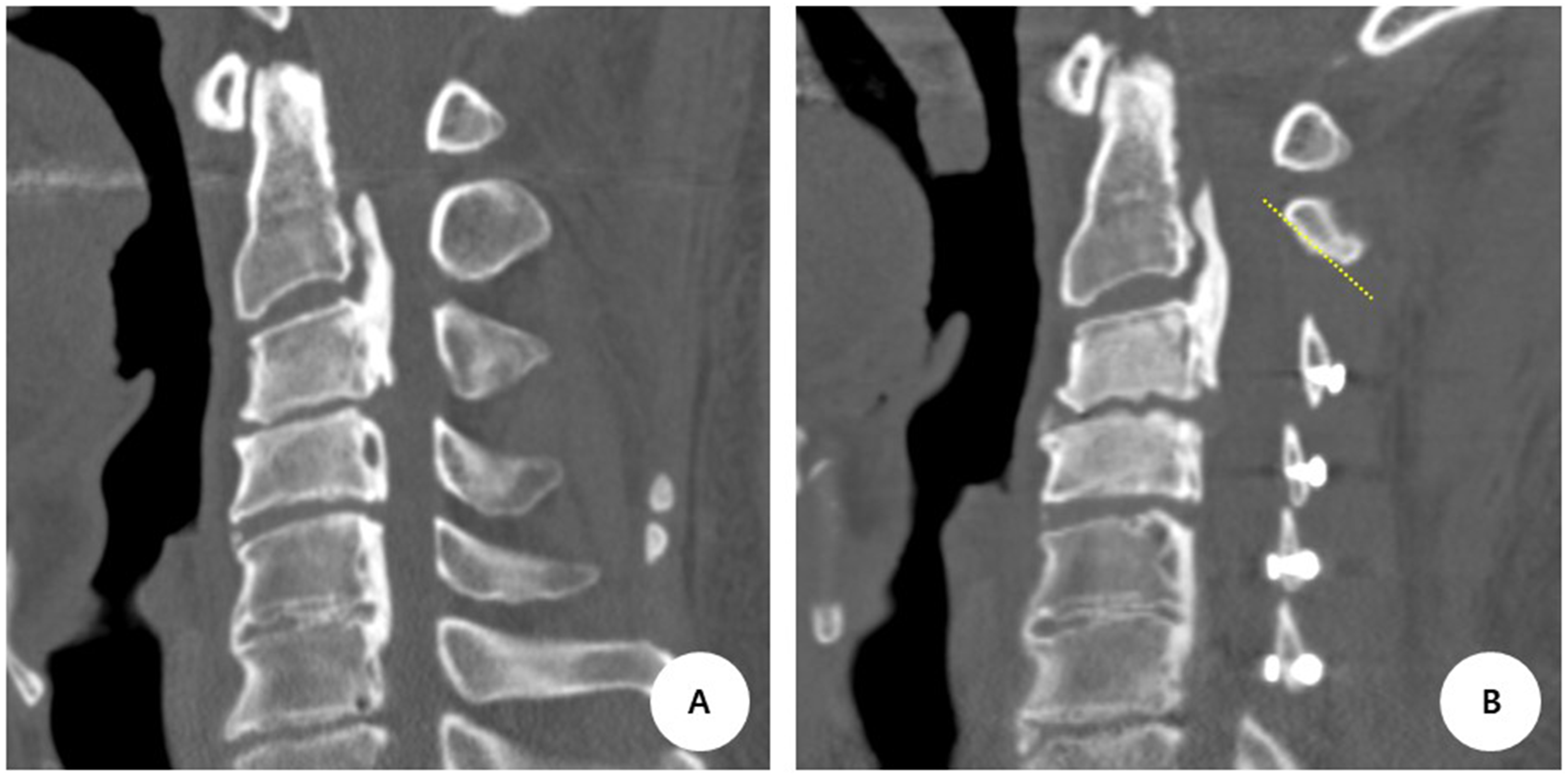
C2-LF
In the C2-LF procedure, bilateral laminectomy extended across the dura, followed by pedicle screw fixation as part of the fusion construct. When OPLL extended to C7 or T1, posterior instrumentation was extended across the cervicothoracic junction. Paravertebral muscles were reapproximated.
Clinical Rationale for Procedure Selection
Surgical procedures were selected based on neurological severity, radiological findings, patient comorbidities, and surgeon clinical judgment. In our policy for surgical treatment of C2-involving OPLL, C2-Dom LP is preferred for patients in whom motion preservation is considered achievable with reliable dorsal decompression, whereas C2-LF is preferred when more extensive decompression and stabilization are required due to congenital stenosis, high canal occupancy, or pre-existing sagittal malalignment.
Radiological Measurements
The cervical sagittal alignment parameters were the C2 slope (C2S), defined as the angle between the lower endplate of C2 and the horizontal plane; C2-7 Cobb angle (CA), measured between the inferior endplates of C2 and C7; sagittal vertical axis (SVA), the horizontal distance from the centroid of C2 to the posterior-superior corner of C7; and T1 slope (T1S), defined as the angle between the upper endplate of T1 and a horizontal line. 11 The K-line was drawn by connecting the midpoints of the spinal canal at C2 and C7 on lateral radiographs to determine whether it intersected with the OPLL (K-line [−]) or not (K-line [+]). 11 The K-line tilt, which is the angle between the K-line and a line perpendicular to the horizon, was measured.
The canal-occupying ratio (COR) was calculated as the maximum thickness of the OPLL divided by the anteroposterior diameter of the spinal canal at the most affected level. OPLL was classified preoperatively on CT as segmental, continuous, mixed, or localized type. The cross-sectional area (CSA) of the spinal canal was measured at the midline level of C2 on axial CT images. The CSA of the OPLL mass at the same C2 level was measured separately to quantify the lesion size for potential progression (Figure 3). All radiological measurements were performed using PACS software (ZeTTA PACS, TaeYoung Soft Co., Ltd., Gwacheon, Korea). Radiological measurements were obtained from the database and independently reviewed by 2 surgeons (SJY and SJP). Discrepancies were resolved through consensus discussion. Measurement of canal CSA and OPLL mass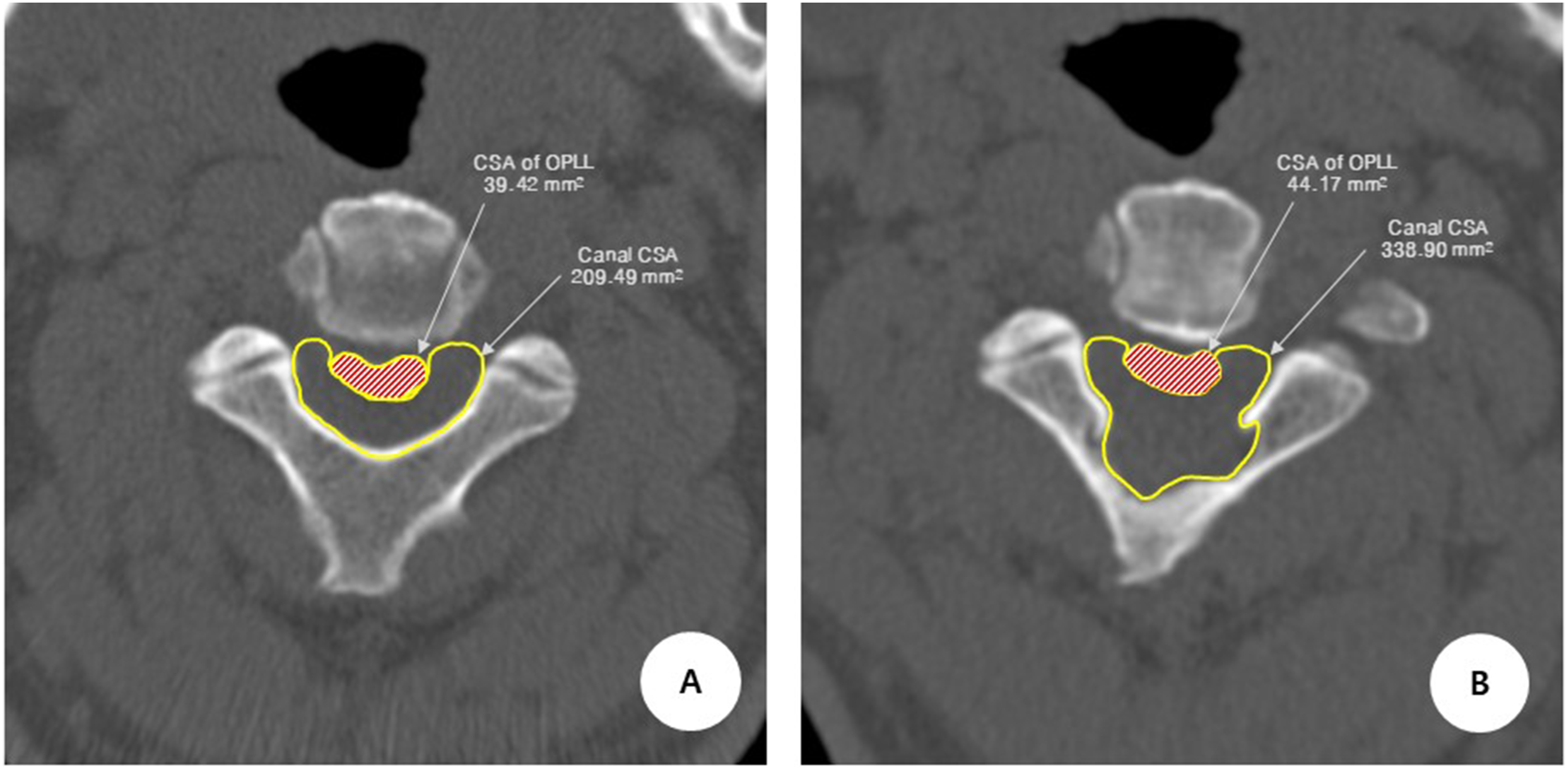
Clinical Assessments
Clinical evaluations were performed preoperatively and at the final follow-up (≥24 months postoperatively) to assess neck and arm visual analog scale (VAS) scores, the Japanese Orthopedic Association (JOA) score, JOA recovery rate, and neck disability index (NDI). The JOA recovery rate was calculated as follows 11 : (Postoperative JOA score – Preoperative JOA score)/(17 – Preoperative JOA score) × 100%.
A JOA recovery rate greater than 50% is considered a good outcome, and a rate less than 50% is defined as a poor outcome. 12 Perioperative complications, including C5 nerve palsy, surgical site infection, neurological deterioration, and revision surgery, were reviewed.
Statistical Analysis
Values were reported as mean ± standard deviation or percentage, as appropriate. Normally distributed continuous variables were compared using Student’s t-test, while non-normally distributed data were analyzed using the Mann–Whitney U test. Categorical variables were evaluated using chi-square or Fisher’s exact test. Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal CSA cutoff for distinguishing high-from low-compromise patients, with thresholds selected using the maximum Youden index. To minimize baseline imbalance between the C2-Dom LP and C2-LF groups, propensity-matched analysis was performed using a logistic regression model that included demographic and perioperative variables (age, sex, BMI, symptom duration, smoking status, hypertension, diabetes, and operative levels). A 1:1 nearest-neighbor algorithm was applied without replacement, and the matched cohorts were used for all subsequent comparative analyses. For radiological measurements, interobserver reliability was assessed using Cohen’s κ coefficient for categorical variables and intraclass correlation coefficients (ICCs) for continuous parameters, calculated using a two-way mixed-effects model with consistency agreement and 95% confidence intervals. Agreement levels were categorized as follows: poor (0.00-0.20), fair (0.21-0.40), moderate (0.41-0.60), good (0.61-0.80), and very good (0.81-1.00). 13 All statistical analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY, USA), with statistical significance set at P < 0.05.
Results
Patient Demographics
Clinical and radiographic data were collected from 143 patients (113 males and 30 females) who underwent C2-Dom LP (n = 71) or C2-LF (n = 72), with a minimum follow-up of 24 months. The mean age at surgery was 57.5 ± 9.4 years (range, 41-79), and the average follow-up duration was 57.2 ± 29.9 months.
Patient Demographics and Baseline Characteristics Between Groups
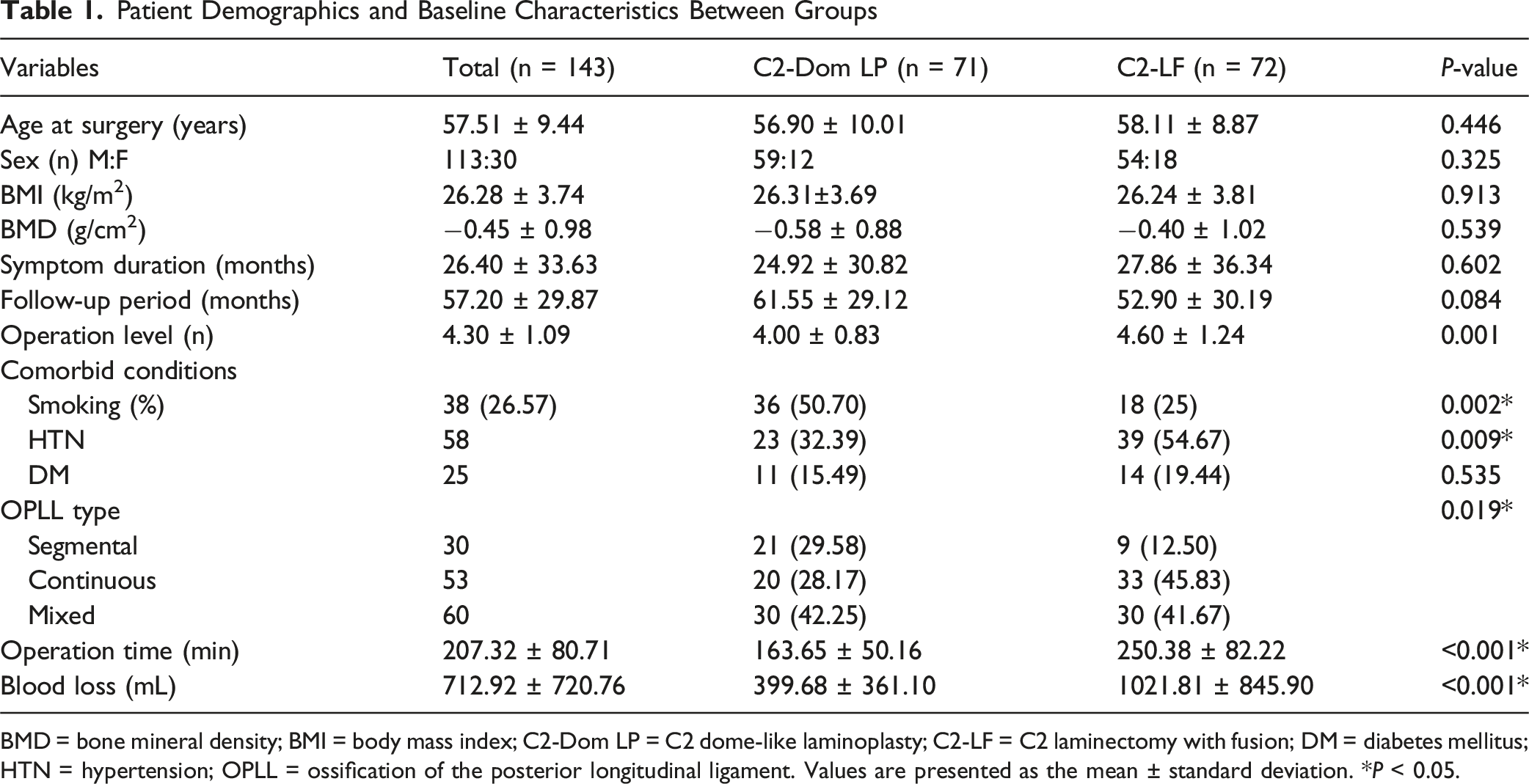
BMD = bone mineral density; BMI = body mass index; C2-Dom LP = C2 dome-like laminoplasty; C2-LF = C2 laminectomy with fusion; DM = diabetes mellitus; HTN = hypertension; OPLL = ossification of the posterior longitudinal ligament. Values are presented as the mean ± standard deviation. *P < 0.05.
Radiological Outcomes
Cervical ROM was significantly better preserved in the C2-Dom LP group than in the C2-LF group (22.35° vs 7.96°, P < 0.001). The reduction in ROM was also significantly greater in the C2-LF group (22.54°, corresponding to a 73.1% decrease from baseline) than in the C2-Dom LP group (10.15°, 14.9% decrease) (P < 0.001). C2-7 SVA and C2S were notably smaller in the C2-Dom LP group before and after surgery. T1S and the K-line tilt were also reduced in the C2-DOM LP group at final follow-up, indicating improved preservation of sagittal alignment with C2-Dom LP.
Comparison of Radiological Parameters Between C2-Dom LP and C2-LF
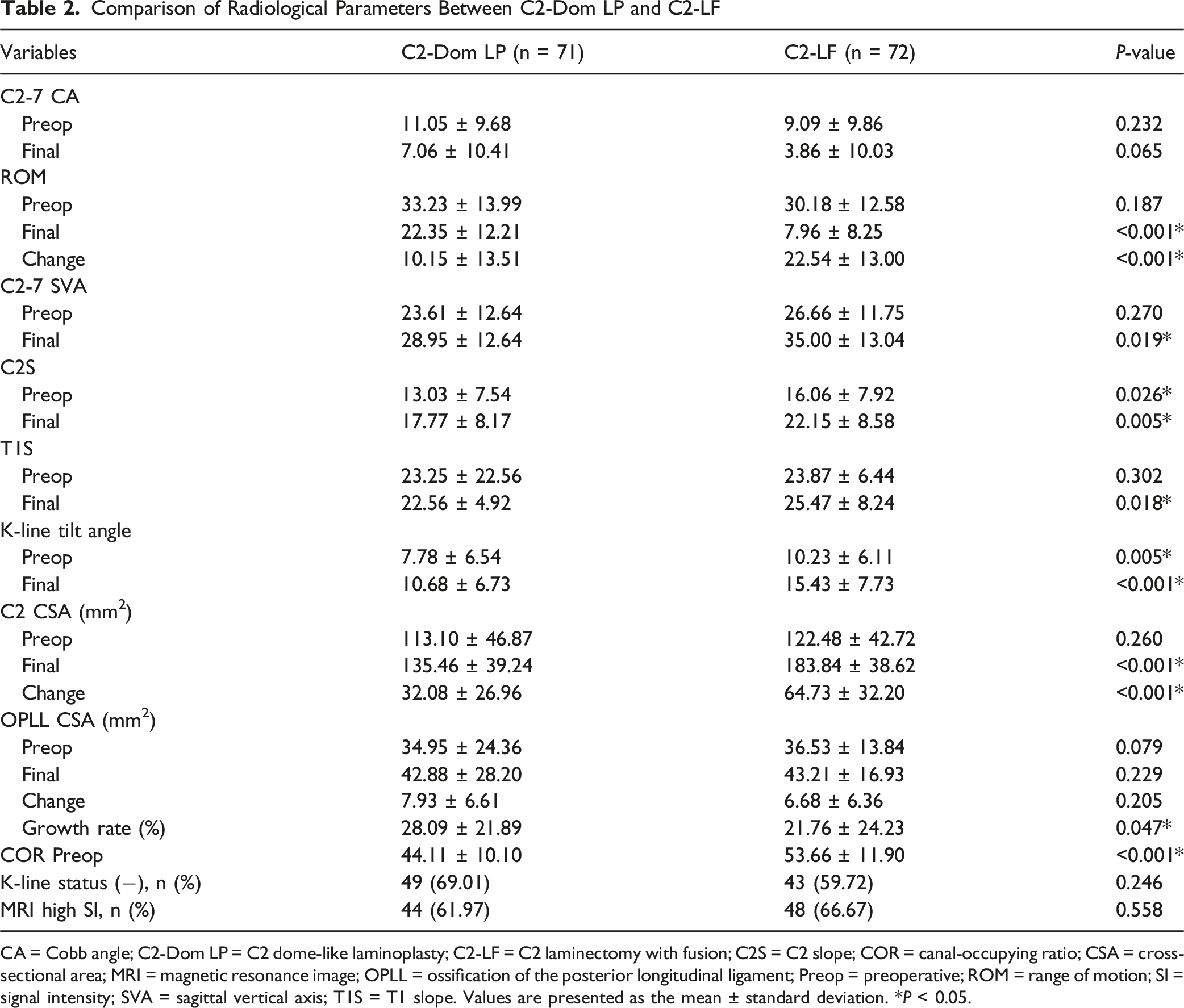
CA = Cobb angle; C2-Dom LP = C2 dome-like laminoplasty; C2-LF = C2 laminectomy with fusion; C2S = C2 slope; COR = canal-occupying ratio; CSA = cross-sectional area; MRI = magnetic resonance image; OPLL = ossification of the posterior longitudinal ligament; Preop = preoperative; ROM = range of motion; SI = signal intensity; SVA = sagittal vertical axis; T1S = T1 slope. Values are presented as the mean ± standard deviation. *P < 0.05.
Clinical and Functional Outcomes
Postoperative improvement was observed in JOA scores in all patients, but the C2-LF group showed significantly greater improvement than the C2-Dom LP group (2.68 ± 2.35 vs 1.82 ± 2.05, P = 0.021). Although the final JOA scores and recovery rates did not differ significantly between the groups, the recovery rate tended to be higher in the C2-LF group (55.38 ± 31.13%) than in the C2-Dom LP group (42.94 ± 43.53%) (P = 0.052). Neck and arm VAS scores improved in both groups without significant between-group differences.
Clinical and Functional Outcomes Between C2-Dom LP and C2-LF
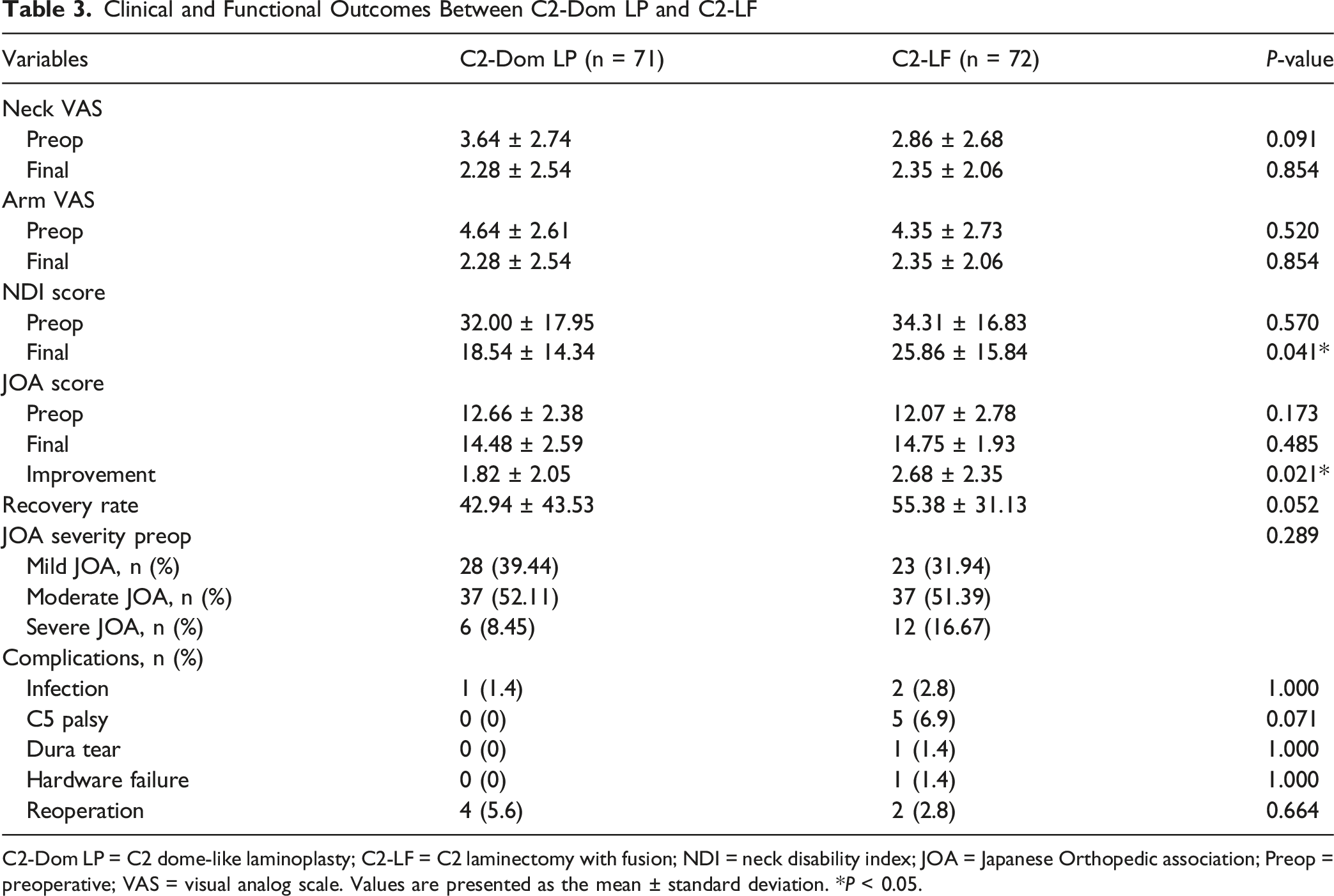
C2-Dom LP = C2 dome-like laminoplasty; C2-LF = C2 laminectomy with fusion; NDI = neck disability index; JOA = Japanese Orthopedic association; Preop = preoperative; VAS = visual analog scale. Values are presented as the mean ± standard deviation. *P < 0.05.
Subgroup Analysis Based on HC Status
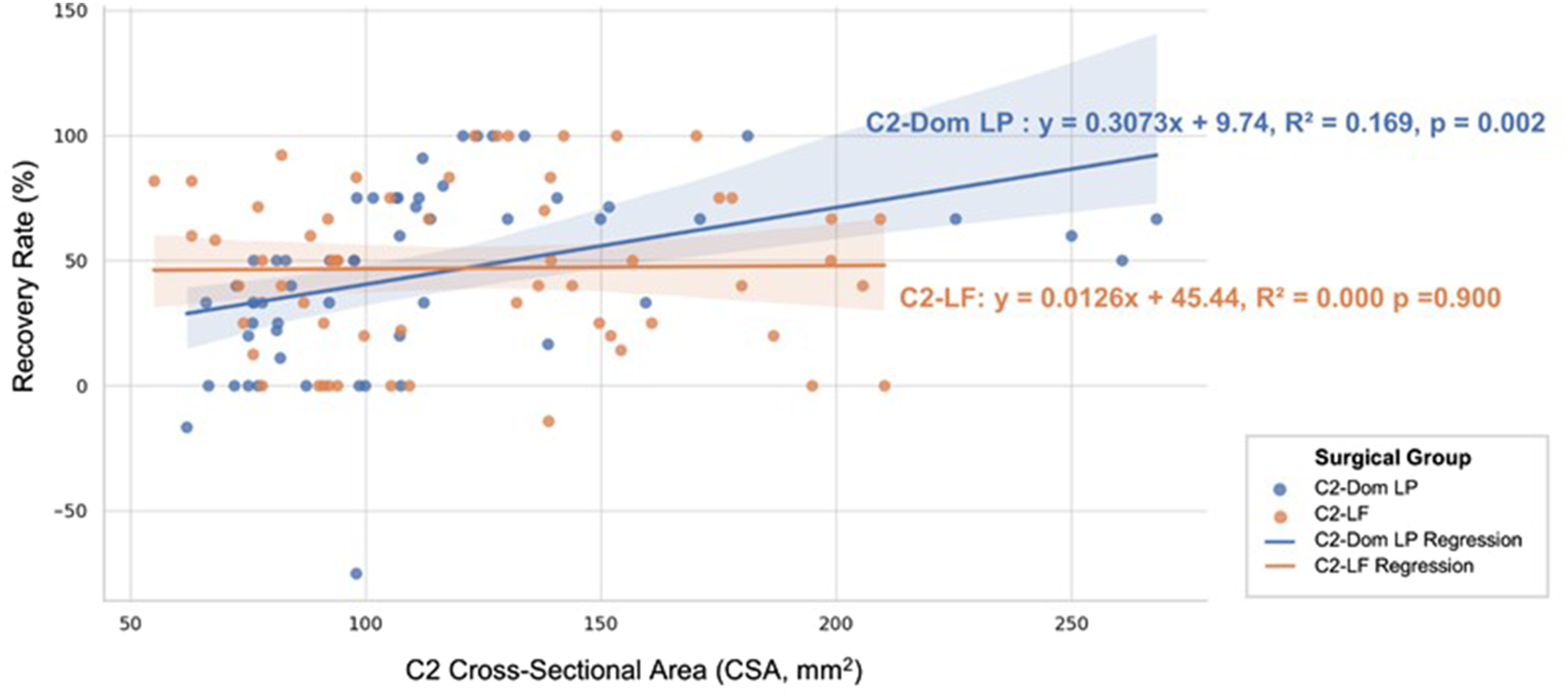
To further evaluate the effect of spinal cord compression severity on surgical outcomes, patients were stratified according to HC status, defined as a C2 CSA <92.24 mm2, which was determined in an ROC curve analysis (Figure 4). In the non-HC group, recovery rates did not differ significantly between the C2-Dom LP and C2-LF groups (57.74 ± 36.02% vs 49.28 ± 33.44%, P = 0.289). In contrast, in the HC group, the C2-LF group demonstrated significantly higher recovery rates than the C2-Dom LP group (42.01 ± 30.50% vs 23.02 ± 19.59%, P = 0.027) (Table 4). This finding was supported by a scatterplot showing that lower CSA values, indicative of HC status, correlated with worse outcomes in C2-Dom LP, whereas C2-LF enabled better recovery (Figure 5). These results suggest that C2-LF might be the preferred surgical strategy, particularly in patients with severe C2 spinal cord compromise (CSA <92.24 mm2). ROC curve for identifying the optimal C2 CSA cutoff to predict poor neurological recovery Comparison of Recovery Rates By Surgical Group and Compromise Status C2-Dom LP = C2 dome-like laminoplasty; C2-LF = C2 laminectomy with fusion; HC = high-compromise. Values are presented as the mean ± standard deviation. *P < 0.05. Scatterplot of the recovery rate and C2 CSA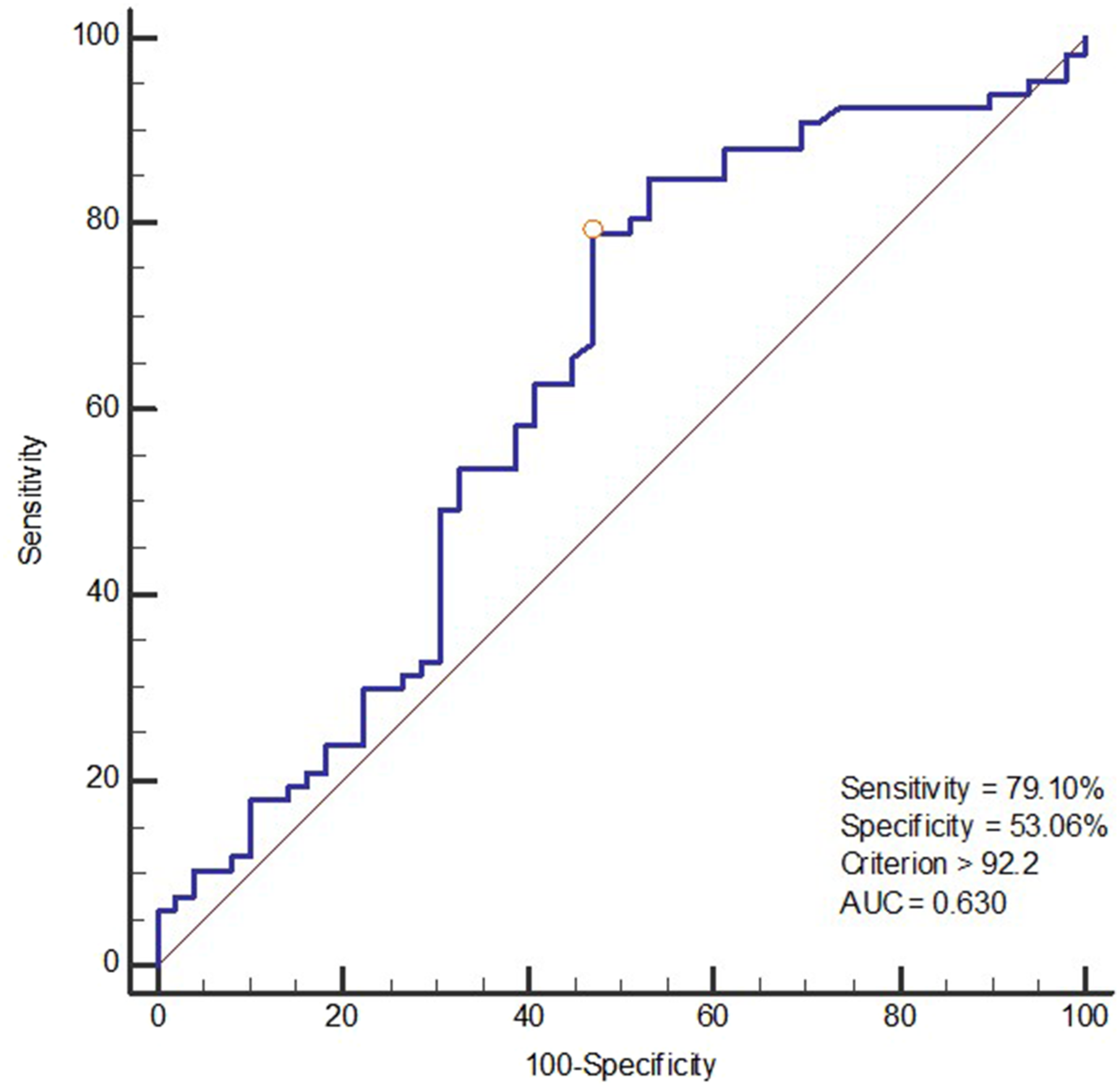

Predictors of Neurological Recovery
Multiple Logistic Regression Analysis of Neurological Outcomes and Cervical Parameters
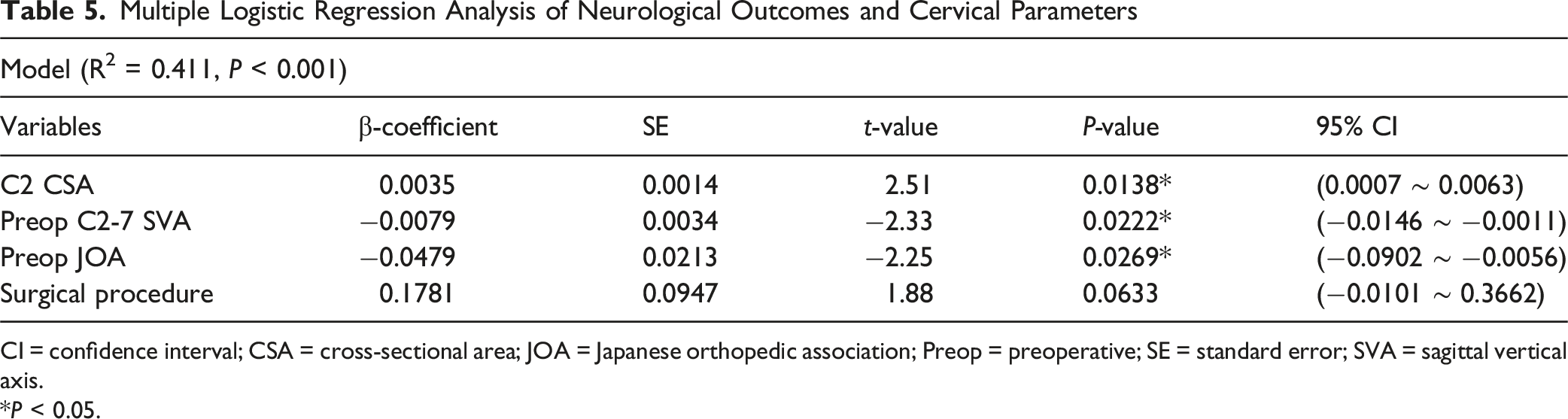
CI = confidence interval; CSA = cross-sectional area; JOA = Japanese orthopedic association; Preop = preoperative; SE = standard error; SVA = sagittal vertical axis.
*P < 0.05.
Comparison of Baseline Characteristics and Outcomes after Propensity Score Matching
After propensity-matched analysis, 28 vs 28 patients were included in the demographic comparison, 49 vs 49 in the radiological analysis, and 70 vs 70 in the clinical evaluation. Propensity score matching effectively reduced the baseline imbalance between the C2-Dom LP and C2-LF groups. All demographic and perioperative variables, including age, sex distribution, BMI, symptom duration, smoking status, hypertension, diabetes, operative levels, and other comorbidities, were balanced between the 2 groups (Supplemental Table 1).
Following propensity-matched analysis, preoperative cervical parameters, including C2-7 CA, ROM, C2-7 SVA, C2S, and T1S, did not differ significantly between groups. However, at final follow-up, the C2-LF group demonstrated significantly reduced cervical ROM and greater C2-7 SVA than the C2-Dom LP group. Postoperative C2 CSA was also significantly larger in the C2-LF group (146.04 mm2 vs 132.15 mm2, P = 0.047), indicating more effective canal decompression (Supplemental Table 2).
Clinical and functional outcomes after propensity-matched analysis showed significant improvements in neck and arm pain in both groups, with no intergroup difference in final VAS scores. Preoperative NDI was significantly higher in the C2-LF cohort (P = 0.009), and this difference persisted at final follow-up (P = 0.023). Importantly, JOA recovery rates were significantly higher in the C2-LF group (55.25 ± 31.57% vs 41.06 ± 45.08%, P = 0.033) (Supplemental Table 3).
Interobserver Reliability
Interobserver reliability for the CSA measurements showed very good agreement, with ICC values ranging from 0.89 to 0.97 for C2 canal CSA, OPLL CSA, and COR (Supplemental Table 4). Similarly, the cervical alignment parameters of C2-7 CA, ROM, C2-7 SVA, C2S, and T1S demonstrated very good agreement, with ICC values ranging from 0.85 to 0.94.
Discussion
This study demonstrated that C2-Dom LP effectively preserved cervical mobility and sagittal alignment in patients with cervical OPLL involving the C2 level, while C2-LF achieved greater canal expansion and better neurological recovery, especially in patients with HC status. These results, reinforced by propensity score matching to address baseline differences, clearly highlighted the distinct advantages of C2-Dom LP and C2-LF. These findings emphasize the importance of a risk-stratified surgical strategy based on the severity of canal compromise.
The posterior longitudinal ligament terminates at C2 and continues cranially as the tectorial membrane. 14 This transition, together with the tapering canal diameter from C1 to C4, complicates OPLL involving the C2 segment. 15 Unlike subaxial OPLL, which is frequently segmental or localized, the C2-involving OPLL in this study was predominantly the continuous or mixed type, consistent with prior reports.4,16 These anatomical distinctions present unique challenges for surgical planning in the upper cervical spine and could explain the differential outcomes between the motion-preserving and fusion procedures.
In laminectomy alone or traditional LP, complete detachment of the SSC from the C2 spinous process disrupts the posterior cervical tension band and increases the risk of instability, axial neck pain, or postoperative kyphosis.17-24 In contrast, C2-LF has been used to maintain lordosis and prevent kyphotic deformity, though it is associated with reduced neck mobility and long operative times.11,25 To address those drawbacks, C2-sparing techniques have been introduced, including C2-Dom LP, 17 double dome LP, 7 and C2 recapping LP. 24 These techniques preserve the C2 spinous process and SSC insertion, minimizing damage to the posterior tension band. However, when ossification extends beyond the mid-C2 lamina toward C1-2 or when severe canal compromise is present, C2-sparing techniques can be technically demanding, risk worsening cord compression during the procedure, and leave residual cranial ossification that predisposes the patient to restenosis. Consequently, controversy persists regarding whether C2-sparing LP or C2-LF provides the optimal balance of motion preservation and decompression in patients with OPLL involving the C2 segment.
C2-Dom LP, as a C2-sparing technique, minimizes damage to the SSC and preserves cervical motion and alignment, resulting in better maintenance of ROM and fewer axial symptoms. 8 In contrast, Jentzsch et al emphasized the role of fusion in preventing post-laminectomy kyphosis and progressive instability in cases with severe canal narrowing. 26 A prospective randomized trial reported that cervical ROM decreased by 75% after LF but by only 20% after LP. 27 Consistent with those findings, our results show that, for C2-involving OPLL, cervical ROM was more significantly preserved in the C2-Dom LP group than the C2-LF group (14.9% vs 73.1% reduction). Furthermore, sagittal parameters of C2 slope, C2-7 SVA, and K-line tilt were more favorable in the C2-Dom LP group, indicating better preservation of sagittal alignment.
LF has been shown to provide greater canal decompression and neurological improvement than LP in extensive multilevel OPLL, despite a higher risk of complications such as instrumentation failure, reoperation, C5 nerve palsy, and dural injury.11,28 Additionally, previous studies suggested that motion-preserving laminoplasty better maintains cervical ROM and alignment than fusion. However, these observations have been derived largely from subaxial OPLL rather than C2-involving OPLL.8,29 Yu et al compared C2-Dom LP and expansive open-door LP but did not evaluate fusion or provide criteria for fusion. 8 To our knowledge, no prior study has established a quantitative, radiologically defined C2 CSA threshold to guide surgical decisions between C2-Dom LP and C2-LF, especially in C2-involving OPLL. This study introduces a CSA-based, image-derived cutoff of 92.24 mm2 to determine when C2-Dom LP is adequate and when C2-LF might be necessary to achieve reliable neurological recovery. Given the limited comparative data and the complex anatomy of C2-involvement OPLL, this threshold provides a novel, clinically useful algorithm for risk-stratified surgical planning.
In this study, postoperative C2 CSA was significantly improved in the C2-LF group, including patients with severe preoperative canal compromise. Our findings confirm that C2-LF achieves greater canal expansion in cases of advanced compression, emphasizing a trade-off between structural decompression and motion preservation.
The incidence of postoperative C5 nerve palsy is lower after LP than after LF, with rates of 4-6% for LP and 9-13% for LF. 30 In patients with severe canal-compromised OPLL, this risk increases further, particularly following extensive decompression.30,31 Consistent with previous reports, 30 our study observed a higher rate of C5 palsy in the C2-LF group (6.9%) than in the C2-Dom LP group (0%), although that difference was not significant.
Several studies have reported favorable outcomes with C2-sparing LP, reducing neck pain while maintaining postoperative lordotic alignment, with a mean JOA recovery rate of approximately 58%.7,8,24 In contrast, meta-analyses comparing LP and LF have suggested that LF can result in improved postoperative cervical lordosis and potentially lower neck pain. 25 Propensity-matched analyses further indicated that LF was associated with significantly greater improvement in VAS scores than LP, although the JOA outcomes were comparable. 32 Other comparative studies similarly demonstrated that both LF and LP yield significant improvements in neck pain, but neither consistently outperforms the other in VAS outcomes. 33
In this study, the JOA recovery rates were similar between C2-Dom LP and C2-LF, although C2-LF achieved greater absolute JOA score improvements. The C2-LF group tended to have higher recovery rates, but that difference was not statistically significant. Conversely, NDI scores were significantly lower in the C2-Dom LP group, indicating superior functional outcomes related to neck disability. Taken together, these findings suggest that motion-preserving techniques such as C2-Dom LP can provide better functional outcomes and pain relief, whereas C2-LF can confer superior neurological improvements. However, the interpretation of these unmatched results was limited by baseline imbalances between the 2 groups, particularly in patient characteristics such as smoking status and preoperative disability.
A propensity-matched analysis was performed to address baseline imbalances and enhance the validity of the comparative analysis. Before matching, the recovery rate demonstrated a nonsignificant trend favoring the C2-LF group, limiting the clinical interpretability of the findings. After adjusting for baseline differences, including important demographic factors such as smoking and preoperative disability, the C2-LF group showed a clearly superior recovery rate. Postoperative C2 CSA was greater in the C2-LF group, indicating more effective canal expansion. These findings suggest that the benefits of C2-LF regarding canal decompression and neurological recovery were partly obscured in the unmatched analysis, and that a propensity-matched analysis provided a more precise and unbiased comparison between the 2 surgical approaches.
When we stratified the patients by canal compromise severity, the recovery rates did not differ significantly between procedures in those without severe compromise. However, in patients with severe canal compromise (C2 CSA <92.24 mm2), recovery rates were significantly higher in the C2-LF group than the C2-Dom LP group. This finding emphasizes that fusion-based approaches, such as C2-LF, offer more reliable neurological recovery in cases of severe compression than C2-sparing LP.
CT scans before and after surgery were used to assess OPLL mass progression. Bone union and remodeling of non-ossified OPLL segments after posterior fusion have been associated with decreased OPLL thickness, 34 and diminished dural pulsation following stabilization might also contribute to this effect. 35 Posterior fixation reduces mechanical stress on the cervical spine, suppressing further ossification. In three-dimensional OPLL volume studies, posterior fusion reduced the OPLL growth rate compared with motion-preserving LP. 28 In the present study, C2-LF suppressed the growth rate of OPLL more effectively than C2-Dom LP. The significantly lower OPLL growth rate in the C2-LF group provides evidence that segmental immobilization can mitigate mechanical stress and suppress further ossification. These findings align with recent volumetric studies 28 suggesting that fixation can reduce future disease burden and the likelihood of revision, emphasizing the long-term suppression of OPLL progression as an important surgical goal to optimize neurological recovery.
Several studies have investigated the prognostic factors associated with neurological recovery after surgery for multilevel cervical OPLL.12,36 However, only a few studies, including Hua et al, 37 have specifically examined C2 involvement as a prognostic factor in cervical OPLL when assessing neurological recovery. Strong evidence supports the COR as a critical determinant of surgical decision-making and outcomes, with a value greater than 60% associated with significantly poorer postoperative recovery than a lower COR.14,38,39 Consistent with previous studies,38,39 our multivariate regression analysis identified a small C2 CSA as an independent predictor of low JOA recovery rates in C2-involving OPLL.
In addition, we found that preoperative sagittal imbalance, particularly an increased C2-7 SVA, correlated negatively with surgical outcomes. Similarly, Sakai et al reported that preoperative C2-7 SVA was an independent predictor of poor functional recovery after posterior decompression. 38
The baseline neurological status, represented by the preoperative JOA score, is another well-established prognostic factor. Chen et al demonstrated that low preoperative JOA scores were associated with reduced recovery in cervical OPLL, regardless of the surgical approach.40,41 We found that low baseline JOA scores were significantly associated with poor neurological recovery, confirming previous findings.40,41
In summary, although the increase in CSA was greater in the C2-LF group, C2-Dom LP still achieved meaningful decompression. However, this less invasive technique might be insufficient in patients with severe canal compromise from C2-involving OPLL. Based on our findings, we propose a CSA-based surgical algorithm (Figure 6). For patients with C2 CSA ≥92.24 mm2 and preserved cervical alignment, C2-Dom LP might be favored to maximize motion preservation and reduce the perioperative burden. For patients with CSA <92.24 mm2, particularly those with preoperative sagittal imbalance or severe myelopathy, C2-LF is recommended to achieve adequate decompression and neurological recovery. CSA provides a direct anatomical measure of canal reserve at the point of maximal compression, and our results demonstrate that a smaller CSA strongly correlates with poorer JOA recovery. Our findings support the use of a C2 CSA threshold of 92.24 mm2 as a quantitative, image-based criterion for selecting between motion-preserving and fusion procedures in C2-involving OPLL. This threshold also underscores the utility of axial CT–based CSA measurement over lateral radiographs in guiding surgical decision-making.
42
Taken together, these results highlight the importance of tailoring the surgical approach to disease severity rather than applying a uniform strategy to all C2-involving OPLL cases. CSA-based surgical algorithm for C2-involving OPLL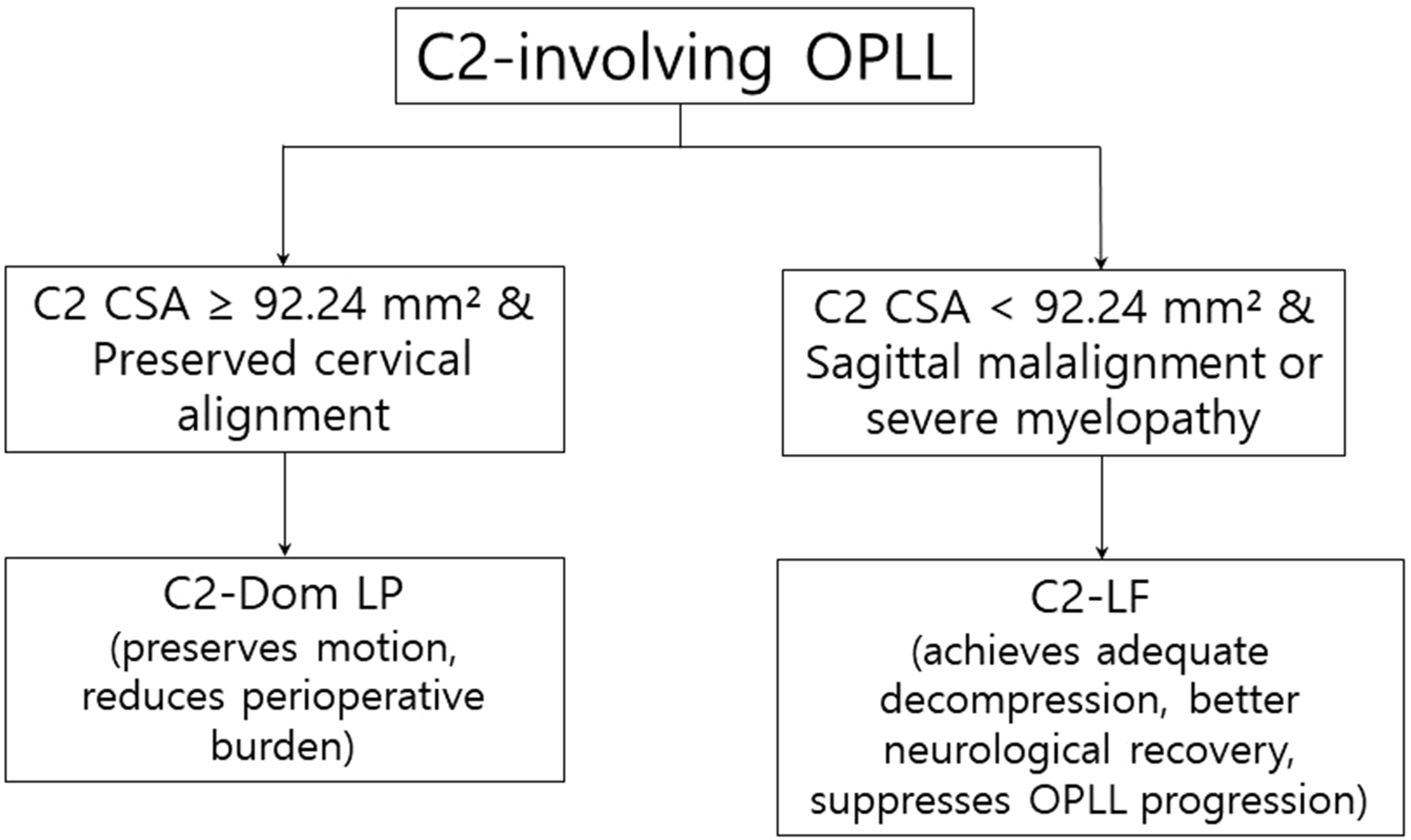
This study has several limitations. First, its retrospective design introduces potential selection and information bias because the surgeons might have favored fusion in patients with more severe stenosis, higher occupying ratios, or preexisting kyphosis. Second, the follow-up duration did not permit evaluation of very long–term OPLL progression, which remains clinically important for assessing the durability of decompression. Third, imaging and clinical assessments were conducted according to routine practice rather than a standardized protocol. On the other hand, this study strengths include a relatively large sample size for this rare condition, longer follow-up than in previous series, and comprehensive clinical and radiological assessments. Importantly, propensity-matched analysis helped reduce baseline imbalances and enhanced the validity of the comparison analysis. Quantitative CSA measurements before and after surgery provide objective insight into decompression efficacy. Future large-scale, prospective, multicenter studies with standardized protocols and extended follow-up are warranted to validate the CSA threshold and refine our proposed risk-stratified algorithm.
Conclusions
C2-Dom LP preserves cervical motion and sagittal alignment while reducing the operative burden, making it a valuable option for standard-risk patients with C2-involving OPLL. In contrast, C2-LF provides greater canal expansion and superior neurological recovery in patients with severe canal compromise. A small C2 CSA, large preoperative C2-7 SVA, and low baseline JOA score were identified as independent predictors of poor recovery. With baseline imbalances mitigated through propensity-matched analysis, these findings provide robust evidence supporting a CSA-based, risk-stratified surgical strategy: motion-preserving C2-Dom LP might be preferred when adequate canal reserve is present, whereas C2-LF is recommended for patients with small CSA or preoperative sagittal malalignment to achieve reliable decompression and neurological improvement. Adoption of this quantitative threshold could optimize surgical decision-making and long-term outcomes in patients with C2-involving OPLL.
Supplemental Material
Supplemental Material - C2-Involving Cervical Ossification of the Posterior Longitudinal Ligament (OPLL): Dome-like Laminoplasty Versus Laminectomy With Fusion
Supplemental Material for C2-Involving Cervical Ossification of the Posterior Longitudinal Ligament (OPLL): Dome-like Laminoplasty Versus Laminectomy With Fusion by Jun Jae Shin, Sun Joon Yoo, Se Jun Park, Dong Kyu Kim, Hyun Jun Jang, Bong Ju Moon, Kyung Hyun Kim, Jeong Yoon Park, Sung Uk Kuh, Dong Kyu Chin, Keun Su Kim, Joongkyum Shin and Yoon Hain Global Spine Journal
Footnotes
Acknowledgments
The authors would like to thank Joongkyum Shin for their contributions in drafting and revising the manuscript for important intellectual content. The authors also wish to thank all of the subjects who participated in the study, as well as the support staff and research coordinator.
Author Contributions
Conception and design: Jun Jae Shin, Sun Joon Yoo, Se Jun Park, Dong Kyu Kim, Hyun Jun Jang, Bong Ju Moon, Kyung Hyun Kim, Jeong Yoon Park, Sung Uk Kuh, Dong Kyu Chin, Keun Su Kim, Yong Eun Cho, Joongkyum Shin, Yoon Ha. Analysis and interpretation of data: Jun Jae Shin, Sun Joon Yoo, Yoon Ha. Drafting the article: Jun Jae Shin, Sun Joon Yoo, Yoon Ha. Reviewed submitted version of manuscript: all authors. Approval of the final version of the manuscript on behalf of all authors: Jun Jae Shin, Sun Joon Yoo, and Yoon Ha. Statistical analysis: Jun Jae Shin, Sun Joon Yoo, Yoon Ha. Study supervision: Jun Jae Shin, Sun Joon Yoo, and Yoon Ha.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.