
Abstract
Study Design
Retrospective cohort study.
Objectives
To explore the correlation between Facet Tropism (FT) and OPLL in cervical spine.
Methods
One-hundred patients with OPLL of cervical spine and one-hundred normal participants without OPLL or cervical disc herniation were included in this study, the patients were matched to the normal participants respectively based on the same sex and similar age (±5). For patients, the cervical levels with and without OPLL were categorized into “OPLL group” and “patient control group,” respectively. Bilateral facet joint angles at C2/3-C6/7 were measured on sagittal, coronal, and axial planes on CT.
Results
On every planes at the level of C2/3-C6/7,the mean difference between left and right facet angles and FT incidence in the most levels of the OPLL group were significantly greater than those in the control groups (P < 0.001). At the most cervical levels, there was no significant difference in mean difference of facet angles and FT incidence between the 2 control groups. On the axial plane, the incidence of FT in segmental type OPLL patients was significantly higher than that in continuous type OPLL patients (P = 0.036). On the coronal plane, the incidence of FT in segmental type OPLL was significantly higher than that in the other OPLL types (P < 0.001), and local type OPLL had a higher incidence of FT compared to mixed type OPLL (P = 0.016). On the sagittal plane, the incidence of FT in segmental type OPLL was higher than that in continuous type OPLL (P = 0.019) and mixed type OPLL (P = 0.036).
Conclusions
There is a significant correlation between OPLL of cervical spine and FT. There are significant differences in the incidence of FT among different cervical OPLL types.
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is characterized by ectopic bone formation in the spinal ligament. Previous studies have shown that this pathological change is associated with various factors, including genetic, endocrine, and mechanical stress.1-3 Facet tropism (FT) is defined as the asymmetry in the angles of the left and right facet joints. Previous research had reported that FT is associated with disc herniation, lumbar spondylolisthesis, Lumbar spondylolysis, and lumbar spinal stenosis.4-8 However, no study explored whether there is a relationship between FT and OPLL in the cervical spine.
Therefore, this study aims to explore the correlation between FT and OPLL in the cervical spine. The study included patients with OPLL between C2-C7, and angles of the facet orientation were measured on axial, coronal, and sagittal planes, respectively.
Materials and Methods
A total of 100 patients with cervical OPLL treated at our hospital from March 2023 to April 2024 were retrospectively analyzed. All patients had given informed consent to allow their information to be used for research purposes. And the study protocol was approved by the Ethics Committee of Shanghai Changzheng Hospital (Project License No.2024SL027). The exclusion criteria included: previous cervical surgery, trauma history, tumor, infection, congenital deformity, spondylolisthesis, spondylolysis, anterior longitudinal ligament ossification, or ankylosing spondylitis. Another 100 participants who had cervical CT scans for thyroid disease examination in our hospital (a mean age of 47.2 yrs [28-75], 50 males and 50 females) were included as the “normal control group”. The “normal” was defined as no cervical disc herniation, OPLL, or other abnormalities. The cervical OPLL patients (a mean age of 49.15 yrs [31-71], 50 males and 50 females) were matched for similar age (±5 yrs) and same-sex to the normal control group. For cervical OPLL patients, cervical levels with and levels without OPLL were categorized into “OPLL group” and “patient control group.”
CT Measurement
Bilateral facet angles of C2/3 to C6/7 were measured on axial, coronal, and sagittal planes of CT images. The midpoint of the anterior and posterior ends of the superior and inferior articular process was defined as the facet line. For the axial plane (Figure 1A), the scan had a similar size to the superior and inferior articular processes selected, and a line was drawn perpendicular to the posterior wall of the vertebral body. The angle between this line and the facet line was defined as the facet angle (α). For the sagittal plane (Figure 1(B), (C)), the midsagittal scan was selected, and the line drawn along the inferior margin of the superior vertebral body was defined as the endplate line. The scan with a similar scale of the superior and inferior articular processes was selected to draw the facet line, and the angle between these 2 lines was defined as the facet angle (β). For the coronal plane (Figure 1(D), (E)), the plane with the largest scale of the vertebral body was selected, and a midsagittal line was drawn perpendicular to the inferior margin of the superior vertebral body. The plane with the largest overall area and similar sizes of the superior and inferior articular process was selected to draw the facet line, and the angle between these 2 lines was defined as the facet angle (γ).
4
OPLL was assessed on CT scans (Figure 2) to determine whether there was ectopic bone formation in the posterior longitudinal ligament between and inferior half of the superior vertebral body and the superior half of the inferior vertebral body. If the ossification was present in this segment, it was classified into the “OPLL group”; if there was no ossification, it was classified into the “patient control group.” According to the type of OPLL, patients were classified as continuous type, segmental type, local type, or mixed type. Measurements of the facet angles at each cervical level were performed by 2 independent observers and their averages were used for further analysis. Diagram of the measurements of facet angles on axial, sagittal, and coronal CT images. Diagram of the method to determine whether there was ectopic bone formation in the posterior longitudinal ligament between and inferior and the superior vertebral bodies.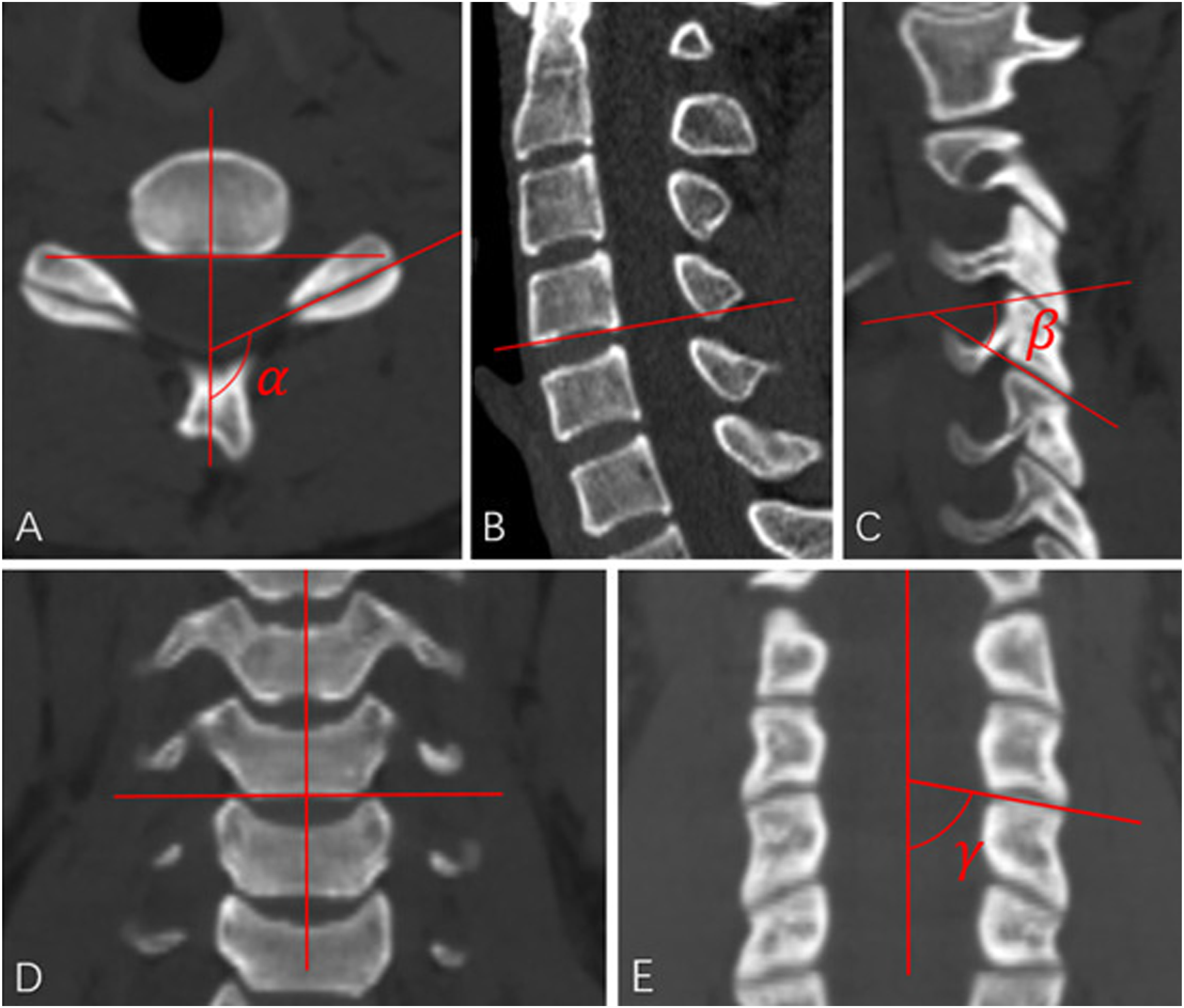

Statistical Analysis
The intraclass correlation coefficient was calculated to assess intraobserver and interobserver reliability. The mean and standard deviation (SD) of the difference between left and right facet angles on the axial, sagittal, and coronal planes were calculated on each cervical segment. FT was defined as the difference between left and right facet angles exceeding the mean ± SD. Depending on the distribution of the data, either Independent-Samples t-tests or Mann–Whitney U test was used to analyze differences in facet angles between different groups. The chi-square test or Fisher exact test was used to assess the correlation between FT and OPLL, as well as the difference in the incidence of FT among different types of OPLL. A P-value <0.05 was considered as statistically significance. All statistical analyses were performed using SPSS 25.0 (IBM Corp, Armonk, NY, USA).
Results
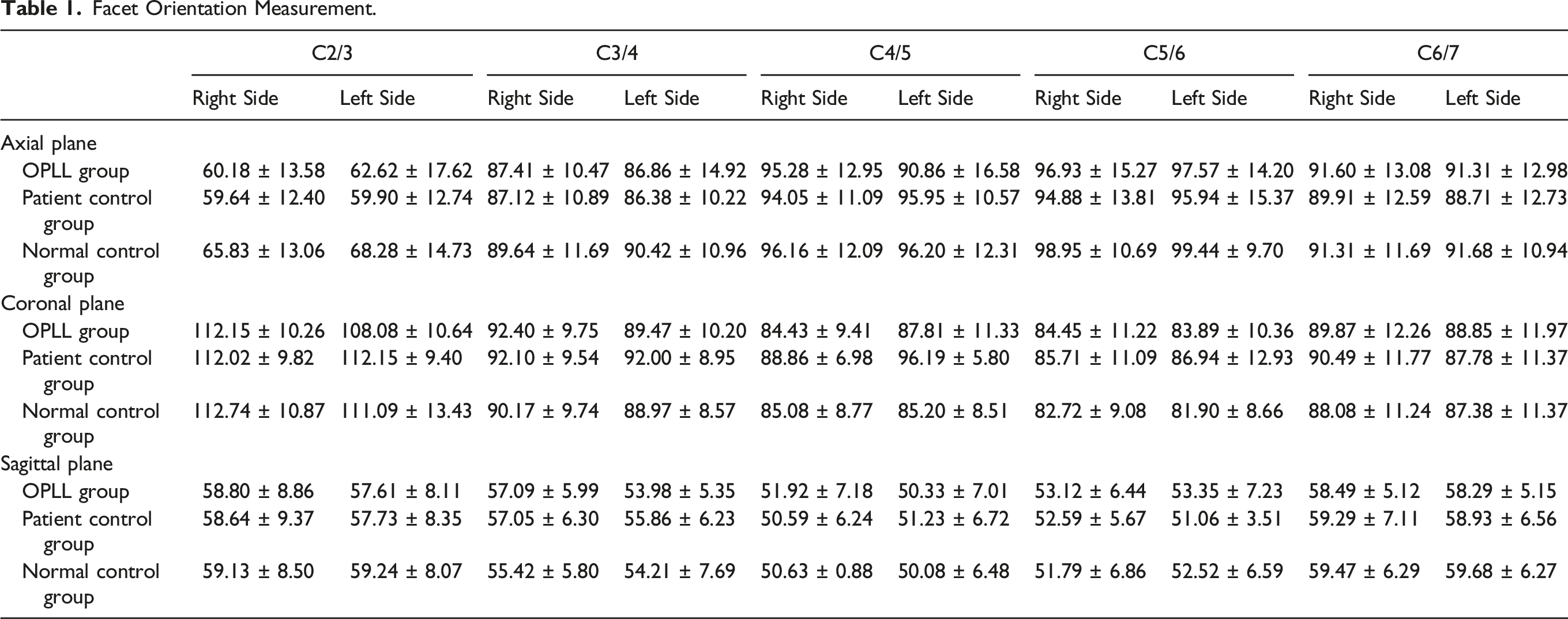
Facet Orientation Measurement.
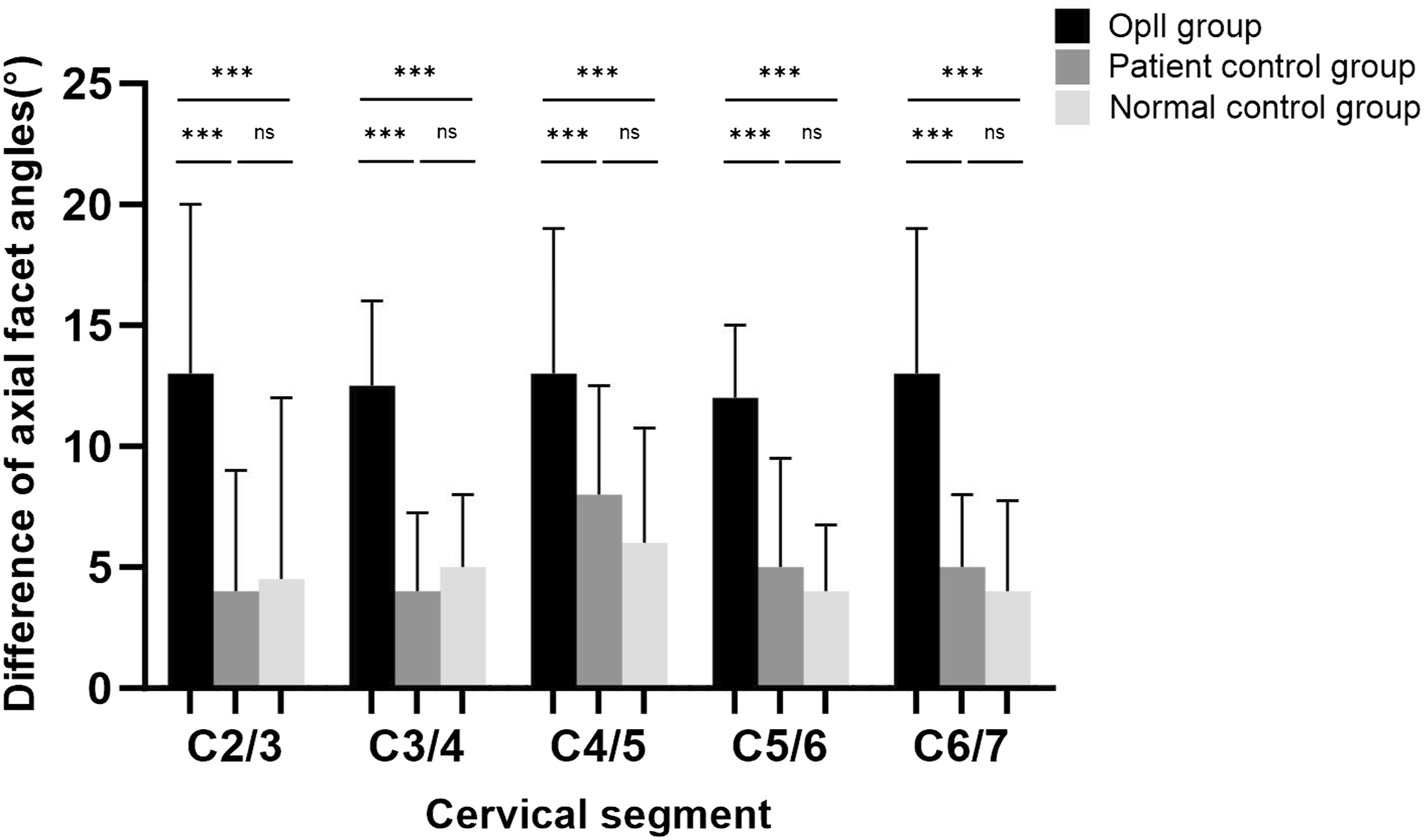
The mean difference between bilateral facet angles on the axial plane among the 3 groups, ‘‘*’ indicates P < 0.05, “**” indicates P < 0.01, “***” P < 0.001.
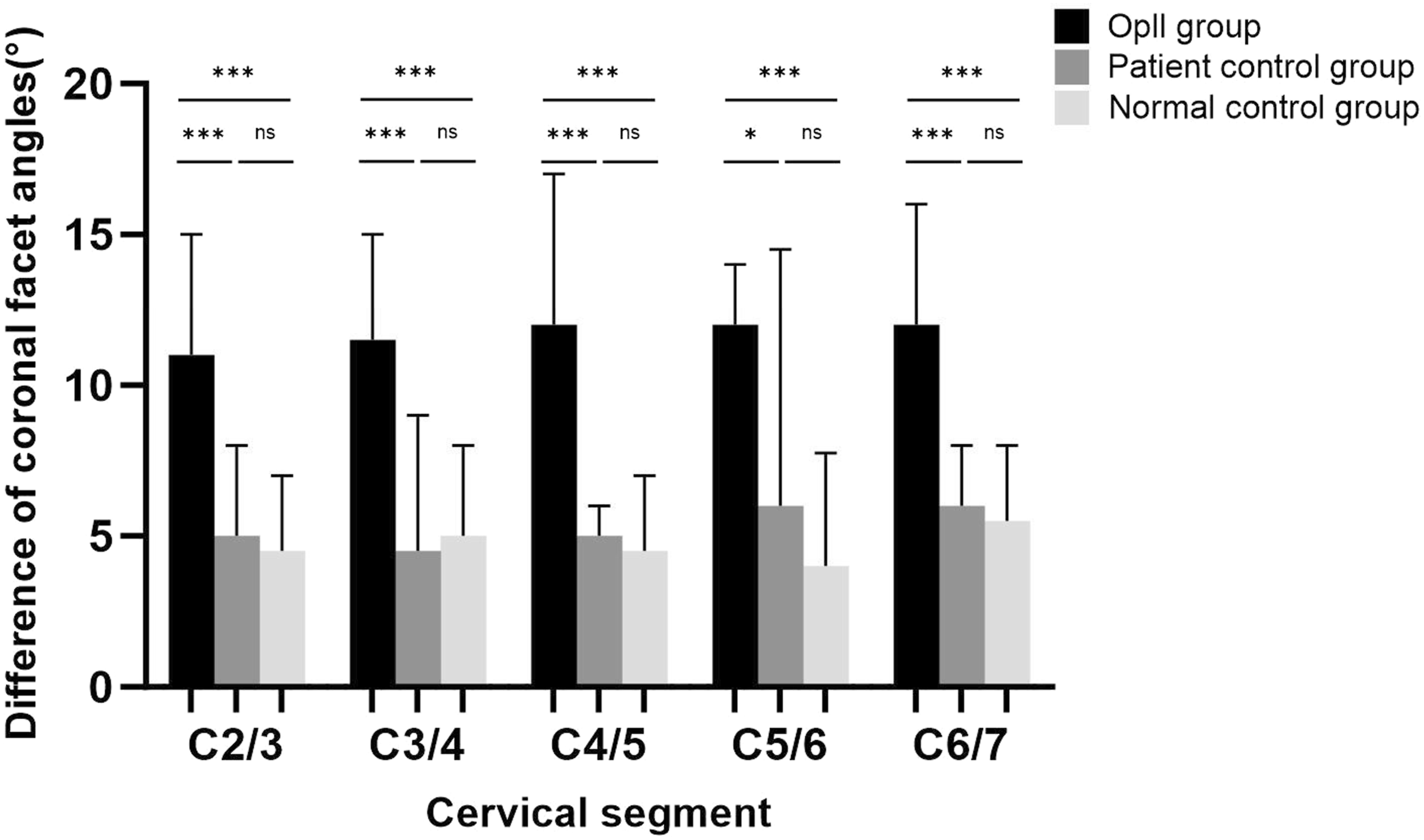
The mean difference between bilateral facet angles on the coronal plane among the 3 groups, ‘‘*’ indicates P < 0.05, “**” indicates P < 0.01, “***” P < 0.001.
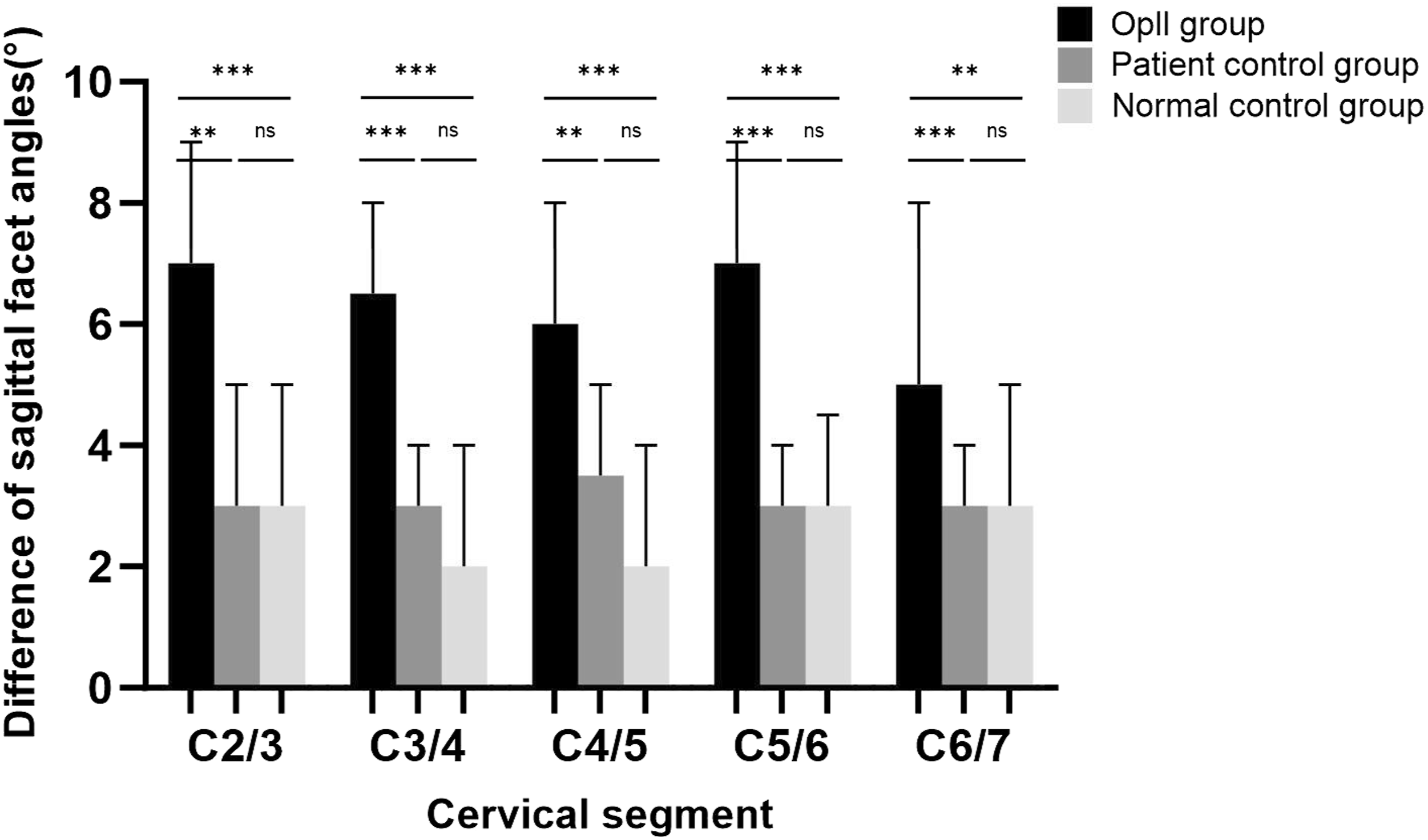
The mean difference between bilateral facet angles on the sagittal plane among the 3 groups, ‘‘*’ indicates P < 0.05, “**” indicates P < 0.01, “***” P < 0.001.
In Figure 6, the incidences of FT were compared. On the axial plane, the FT incidence in the OPLL group was significantly higher than those in the normal control group at C2/3 (P = 0.001), C3/4 (P < 0.001), C4/5 (P < 0.001), C5/6 (P < 0.001), and C6/7 (P < 0.001). The OPLL group also showed a significantly higher incidence of FT compared to the patient control group at C2/3 (P = 0.001), C3/4 (P < 0.001), C5/6 (P < 0.001), and C6/7 (P < 0.001), while no significant difference was observed at C4/5. There was no significant difference was observed between the patient control group and the normal control group on the axial plane. On the coronal plane, the OPLL group exhibited a significantly higher incidence of FT compared to the normal control group concerning all cervical levels (P < 0.001). The OPLL group had a significantly higher incidence of FT compared to the patient control group at C2/3 (P < 0.001), C3/4 (P = 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001), but no statistical significance was observed at C5/6. The incidence of FT between the patient control group and the normal control group had a significant difference only at C5/6 (P = 0.015). On the sagittal plane, the OPLL group exhibited a significantly higher incidence of FT compared to the normal control group at all cervical levels (P < 0.001). Also, the OPLL group had a significantly higher incidence of FT compared to the patient control group at C2/3 (P < 0.001), C3/4 (P = 0.003), C4/5 (P = 0.006), C5/6 (P = 0.009) and C6/7 (P < 0.001). The incidence of FT between the patient control group and the normal control group had a significant difference only at C6/7 (P = 0.001). The incidence of facet tropism between groups on the axial, coronal, and sagittal planes was compared between each group at each cervical level, ‘‘*’’ indicates P < 0.05, ‘‘**’’ indicates P < 0.01, ‘‘***’’ indicates P < 0.001.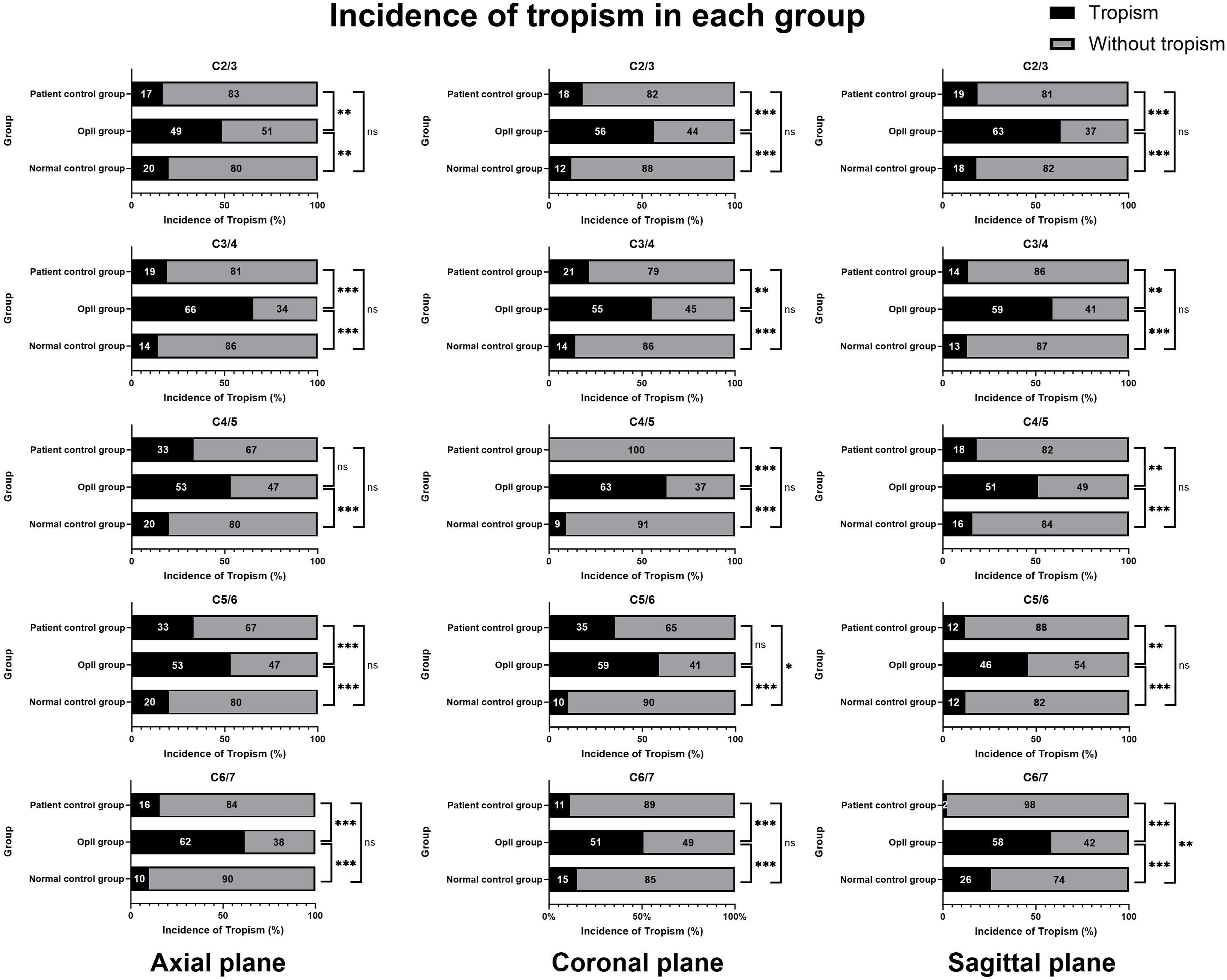
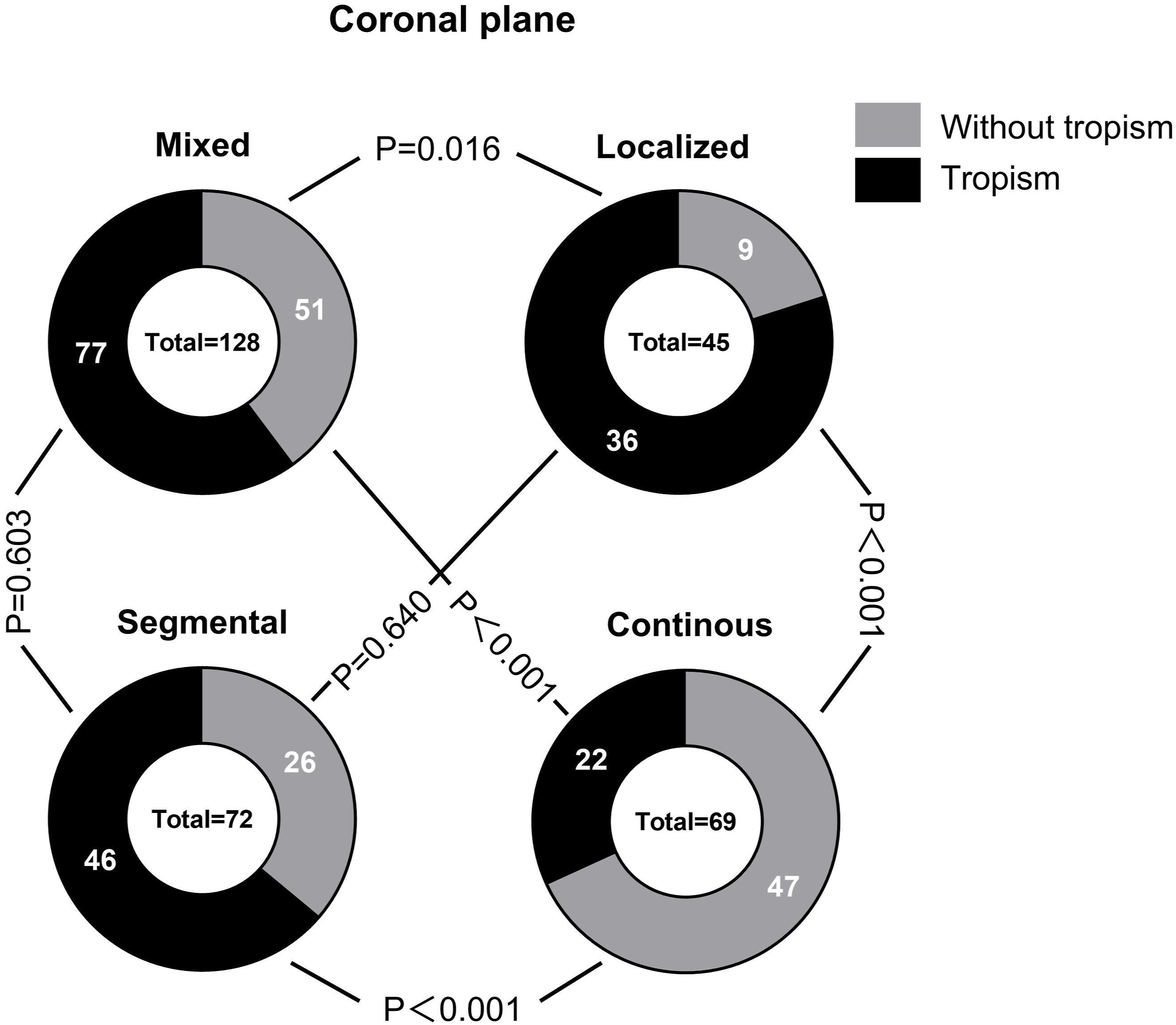
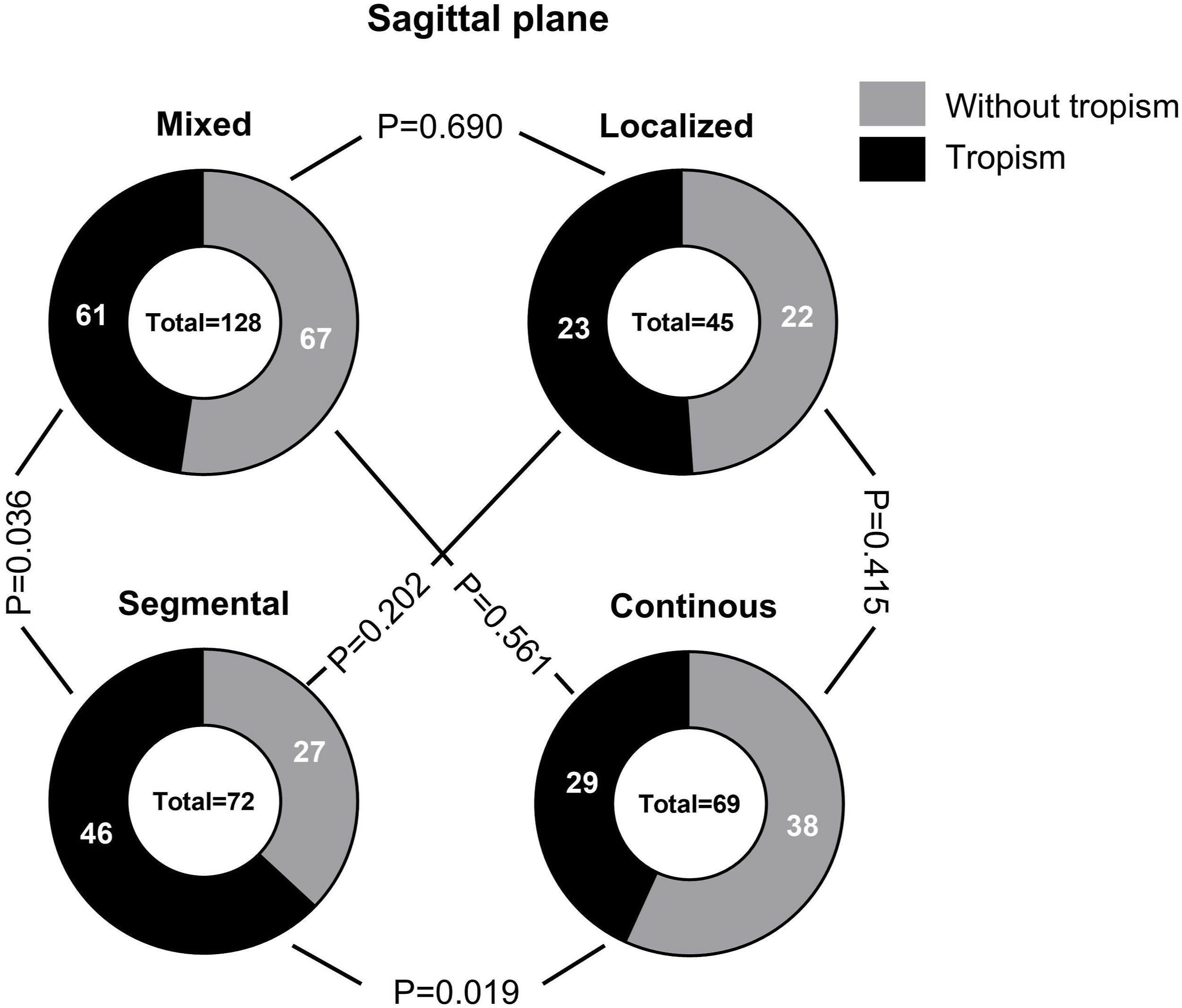
The comparison of the incidence of FT between different types of OPLL is shown in Figures 7–9. On the axial plane (Figure 7), the incidence of the FT in the mixed type OPLL was 58.6%, the local type OPLL was 60.9%, the segmental type OPLL was 69.4% and the continuous type OPLL was 52.2%. The occurrence rate of FT in segmental-type OPLL was significantly higher than that in continuous-type OPLL (P = 0.036). On the coronal plane (Figure 8), the incidence of the FT in the mixed type OPLL was 60.2%, the local type OPLL was 80%, the segmental type OPLL was 63.9% and the continuous-type OPLL was 31.9%. The occurrence rate of FT in continuous-type OPLL segments was significantly lower than that in local type, mixed type, and segmental type OPLL (P < 0.001). Additionally, the occurrence rate of FT in local-type OPLL was significantly higher than that in mixed-type OPLL (P = 0.016). On the sagittal plane (Figure 9), the incidence of the FT in the mixed type OPLL was 47.7%, the local type was 51.1%, the segmental type was 63.9% and the continuous type was 42.0%. The occurrence rate of FT in segmental type OPLL was higher than that in continuous type OPLL (P = 0.019) and mixed type OPLL (P = 0.036). The incidence of facet tropism between different types of OPLL on the axial plane was compared. The incidence of facet tropism between different types of OPLL on the coronal plane was compared. The incidence of facet tropism between different types of OPLL on the sagittal plane was compared.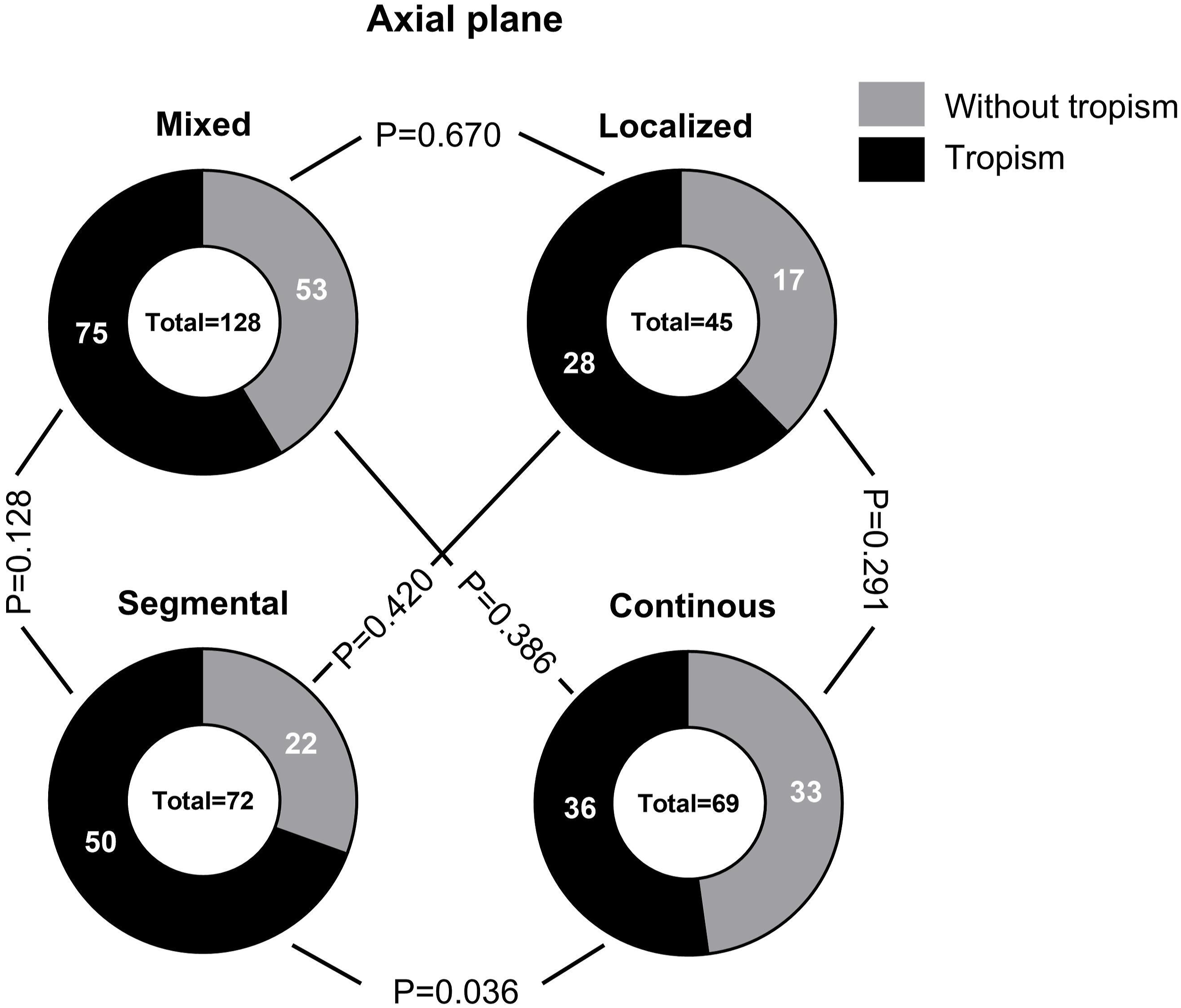
Discussion
To the best of our knowledge, this is the first study to analyze the correlation between cervical OPLL and FT. FT refers to an indicator of asymmetry in the cervical facet angle. Previous studies had explored the correlation of FT with a range of degenerative spinal conditions, especially on cervical spondylosis, research shows cervical disc herniation is associated with the presence of FT, yet the greater facet angle at the left or right side does not affect the side of herniation, and the severity of cervical disc degeneration is also unrelated to FT. 4 Wu et al also discovered that patients with degenerative cervical spondylolisthesis was generally associated with more horizontal facet angle on the sagittal plane and more FT compared to individuals with general cervical degeneration. 9 In the axial plane, a more sagittal facet angle and FT are significantly associated with degenerative lumbar spinal stenosis. 10 FT is also correlated with the occurrence of symptoms, Yang et al found that FT is an independent risk factor for chronic low back pain. 11 Results of the finite element study showed that the facet tropism caused imbalanced stress distribution at both the intervertebral disc and facet joints. 12 Therefore, it is reasonable to speculate that the facet tropism might be an anatomical risk factor for the development of cervical disc degeneration. However, it is unknown whether this asymmetry characterized by FT affects the posterior longitudinal ligament of the cervical spine, or whether cervical FT is correlated with ossification of the posterior longitudinal ligament of the cervical spine.
In this study, we compared the differences in facet angle and FT incidence between OPLL patients and normal control participants. To eliminate the potential influence factors like age and gender in assessing facet angles, we conducted pairwise matching between OPLL patients and normal participants. 13
As shown in Figure 3, Figures 4 and 5, on the axial, sagittal, and coronal planes, across most cervical levels, the incidence of FT and the average difference of the bilateral facet angles in the OPLL group was significantly higher than those in the control groups. This suggests that the changes in facet joint morphology are more frequent at the cervical level with OPLL compared to those without OPLL, and there was no significant difference observed between the normal control group and the OPLL control group. These findings implied that the change of facet joint morphology may represent a specific feature of OPLL cervical level rather than a generalized characteristic of OPLL patients.
Furthermore, based on previous research, the formation of OPLL is associated with abnormalities in endocrine function, mechanical stress, and gene expression.1-3 Our study further reveals a significant correlation between the presence of cervical OPLL and FT. We hypothesize that the FT, represented by the difference in bilateral facet angles, will change the normal trajectory of cervical movement, leading to asymmetrical motion that induces abnormal tension in the posterior longitudinal ligament, thereby promoting its ossification.
Additionally, our study found variations in the occurrence rates of FT among different types of OPLL which are classified as segmental, local, continuous, and mixed types. Segmental and local types OPLL showed higher occurrence rates of FT, whereas continuous and mixed types OPLL showed lower rates. Previous studies have found the OPLL types classified by the plain radiographs presented different genetic and clinical symptoms, leading some researchers to categorize them into OPLL continuous (including mixed type OPLL) group and OPLL segmental (including local type OPLL) group. OPLL continuous group exhibits overexpression of osteogenic-specific genes, whereas OPLL segmental group shows moderate to high levels of expression of these genes. 14
Kudo et al 15 investigated the genetic differences in the osteogenic differentiation potential among different types of OPLL, indicators such as Bone morphogenetic protein-2 (BMP-2), alkaline phosphatase (ALP), and Osterix which suggested the OPLL continuous group has a higher osteogenic differentiation potential than the OPLL segmental group. Compared with the OPLL segmental group, spinal ligament cells from the OPLL continuous group tend to mineralize more easily, with ALP activities of 2.56 ± 0.05 for the OPLL continuous group, 1.21 ± 0.11 for the OPLL segmental group and 1.00 ± 0.05 for non-OPLL. 16
The posterior longitudinal ligament is composed of deep and superficial layers; the deep layer is located behind the vertebral body and connects 2 adjacent vertebral bodies, which is why we choose the inferior half of the superior vertebral body and the superior half of the inferior vertebral body’s OPLL to match the same level facet joints; the superficial layer of the ligament spans 3 to 4 vertebral body. Based on our previous hypothesis that the orientation of the articular process will produce abnormal tension on the ligament of the same cervical level, we speculate that this tension could also affect the distribution of normal tension in the superficial ligament of the adjacent cervical level, thereby promoting the formation of ossification on the tension-sensitive posterior longitudinal ligament, such as the continuous type OPLL, and thus explaining the lower incidence of FT in the continuous type OPLL. Although surgery is an effective way to treat the disease, the growth of OPLL after decompression surgery has been considered the main reason for reoperation within the first 2 years after surgery. 17 Particularly in patients with greater cervical mobility after laminoplasty (LP), increased tension on the posterior longitudinal ligament leads to faster growth of the ossified volume. 18 Our study suggests a significant correlation between FT and OPLL. FT may exert abnormal tension on the posterior longitudinal ligament and serves as a risk factor for the onset and progression of OPLL. Therefore, for patients with FT, especially those with greater cervical mobility, surgeons should prioritize fusion surgery over laminoplasty to prevent the progression of ossification. Additionally, patients should be advised to extend the duration of wearing a cervical collar after surgery to reduce excessive cervical movements.
Understanding FT as a risk factor aids surgeons in making surgical decisions and predicting the progression of ossified volume in OPLL. This enables the provision of personalized health guidance for patients. To the best of our knowledge, this is the first study to attempt establishing a correlation between OPLL and cervical anatomy. The study found a significant correlation between FT and OPLL, which may be attributed to the abnormal tension exerted by FT on the posterior longitudinal ligament.
Conclusion
FT is associated with OPLL across cervical levels from C2/3 to C6/7 on axial, sagittal, and coronal planes. Among the various OPLL types, the segmental OPLL group showed a higher correlation with FT, whereas the continuous OPLL group showed a lower correlation. Our study supported the classification of OPLL into continuous and segmental groups. However, it only established a correlation between FT and OPLL and didn’t explain the exact mechanisms involved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Shanghai Health Science Youth Talent Ability Promotion Project (JKKPYC-2022-11), Shanghai Municipal Health Commission Advanced and Appropriate Technology Promotion Project (2019SY008), and Shanghai Educational Science Research Project (C2024121).