
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To identify prevalence of ossification of the posterior longitudinal ligament (OPLL) of the cervical spine in a large sample, to characterize spinal involvement, and to identify associations with patient characteristics.
Methods:
Computed tomography (CT) scans of all patients receiving cervical spine CT imaging in a level-1 emergency department from January 1, 2014 to December 31, 2014 were reviewed. Diagnosis and classification of OPLL was performed, and data for associated patients was obtained (age, sex, race, ethnicity, body mass index, diabetes). US Census data was referenced for the sample population. Statistical analysis included t test and chi-square testing, with significance cutoff P < .05.
Results:
There were no significant differences between the sample and population data. Of 2917 patients reviewed, 74 exhibited OPLL (2.5%). Age distribution between OPLL and non-OPLL cohorts was significantly different (P < .01), with highest prevalence of OPLL between ages 40 to 49 and 50 to 59 years. Comorbid diabetes also differed between groups (27% OPLL, 13% non-OPLL, P < .01). There was no difference in distribution of sex, race, or ethnicity. For OPLL, segmental type is most common (67.6%), involving on average 3.4 levels. OPLL involvement begins at any level, but ends most commonly at C6 (40.5%) or C7 (36.5%). Among OPLL patients, 18 (24.3%) demonstrated concurrent ponticulus posticus.
Conclusions:
This review of 2917 patients reaffirms previous data, with OPLL prevalence of 2.5%. In asymptomatic patients, incidental diagnosis is frequently seen as early as ages 40 to 49 years. OPLL is better characterized with a significant association with diabetes, segmental type being the most common, and the caudal extent typically involving C6-7 (77%).
Introduction
Ossification of the posterior longitudinal ligament (OPLL) is an incompletely understood, hyperostotic spinal condition. While the pathogenesis is not fully known, it involves the ectopic ossification of the posterior longitudinal ligament. 1 Symptoms vary and are often dependent on the degree of spinal stenosis arising from the OPLL. 1,2 The epidemiology of this condition is a matter of ongoing study. 2,3
The posterior longitudinal ligament plays a supportive structural role, primarily to prevent hyperflexion of the spine. 4 Ossification, or thickening and calcification, can occur for a number of reasons. 1,5 Research has suggested a possible relationship with diffuse idiopathic skeletal hyperostosis (DISH) as well as diabetes mellitus. 6 -8 Bone turnover marker abnormalities have been noted in patients with OPLL, especially with osteocalcin (OSC) and Dickkopf-related protein 1 (DKK-1). 9 Previously thought to be associated with certain races or regions (East Asia), more recent studies demonstrate the prevalence of this condition across ethnicities. 1,10,11 Multiple genomic studies have identified possible genetic anomalies and familial inheritance patterns, including variants of COL6A1, BMP4, and BMP9. 12 -14
The classification of OPLL is based on the appearance of the lateral cervical spine x-ray or sagittal computed tomography (CT) scan. Types include localized, segmental, continuous, or mixed (Figure 1a and b). 11 Localized type involves ossification of the PLL bridging the intervertebral disk only, not involving the PLL at the level of the vertebral body. Segmental type involves ossification posterior to the vertebral bodies only. The continuous type is an ossified mass that spans several vertebral bodies and disk spaces. Mixed type is a combination of both continuous and segmental types.
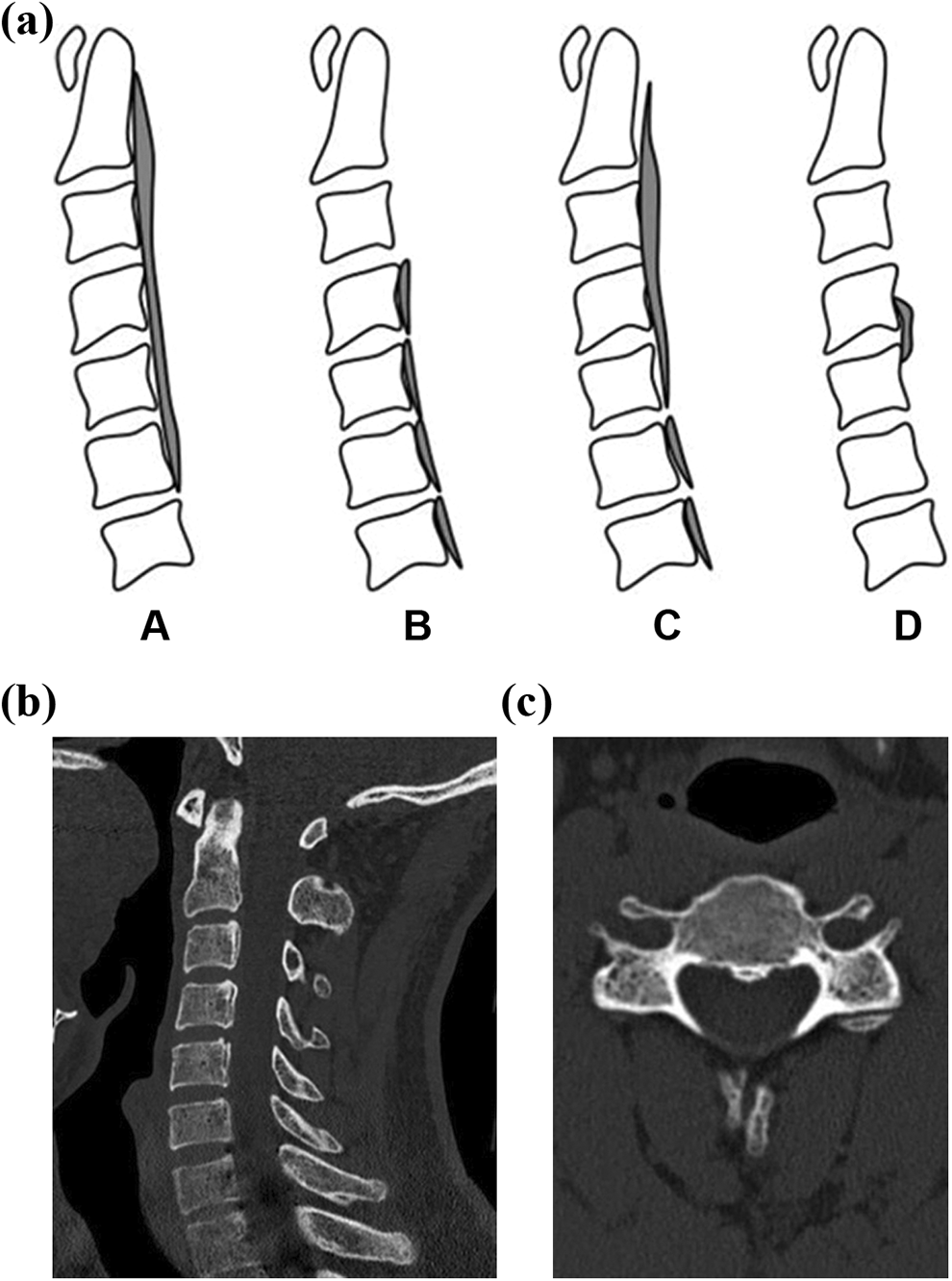
(a) Classification of ossification of the posterior longitudinal ligament (OPLL): (A) is continuous, (B) is segmental, (C) is mixed, (D) is localized. (b) Sample computed tomography (CT) sagittal reconstruction of patient with OPLL, segmental type C3-C5. (c) Sample CT axial reconstruction of patient with OPLL, segmental type C3-C5.
OPLL is most common in the cervical spine. In patients with cervical OPLL, involvement of other regions such as the thoracic spine, is common and can be seen in 50% to 60% of patients. 2 Dural defects can be identified via close CT scan review, using the double-layer sign. 15 Magnetic resonance imaging (MRI) is useful in determining the extent of spinal cord compression.
The epidemiology of this condition is a subject of ongoing study. Previous work suggests prevalence as low as 0.6% in western Europe and North America, ranging up to 2.2%, although in Far Eastern communities this is much higher. 1,16 In Japanese communities, prevalence can reach 2% to 4%. 16 Among patients with myelopathy, a large global study found OPLL in 10% of patients. 17 Our objective was to evaluate the prevalence of cervical OPLL in a local geographic sample representative of the generalized US population and assess its association with other cervical spinal conditions and demographic factors.
Materials and Methods
After institutional review board approval, all patients who received a cervical spine CT performed in the emergency department of a level-1 trauma center at a single institution between January 1, 2014 and December 31, 2014 were identified. All cervical spine CT scans performed were included in the study, regardless of the indication. Indications ranged from neck pain to mechanism of trauma. For patients who received more than 1 cervical spine CT, only the first CT scan was included/reviewed. All images were reviewed using the institution’s Picture Archiving and Communication System (PACS) server. Only patients who had a complete CT cervical spine series, including axial, coronal, and sagittal reconstructions were included in this study. Images were reviewed for quality and those with complete but unreadable quality images were excluded.
The images were reviewed by board-certified orthopedic spine surgeons, an orthopedic spine surgery fellow, orthopedic surgery resident, or a fourth-year medical student who were all trained to identify and classify OPLL via CT scan, in addition to other conditions, including DISH, Klippel-Feil syndrome (KFS), ponticulus posticus (PP), and ossification of the yellow ligament (OYL). For each patient, the diagnosis of OPLL also included classification as described earlier, as either localized, segmental, continuous, or mixed type. CT scans were also noted for the presence of either DISH, KFS, or PP. For all patients, demographic data was recorded, including age, sex, race, body mass index, and relevant medical history, including diabetes mellitus. US Census data was obtained for the local geographic county from the US Census database. 18 History of other relevant associated spinal conditions was also reviewed, including presence of OYL or DISH affecting other parts of the spine. Power analysis was conducted, necessitating 1620 patients for a power of 80% to identify differences in demographic data from the general population.
Statistical analysis included student’s t test for mean comparison between groups. Mann-Whitney U testing was also performed to account for any variables with a nonparametric distribution. Distribution of age and race between groups was compared using chi-square analysis. Statistical significance was established at a cutoff value of P < .05.
Results
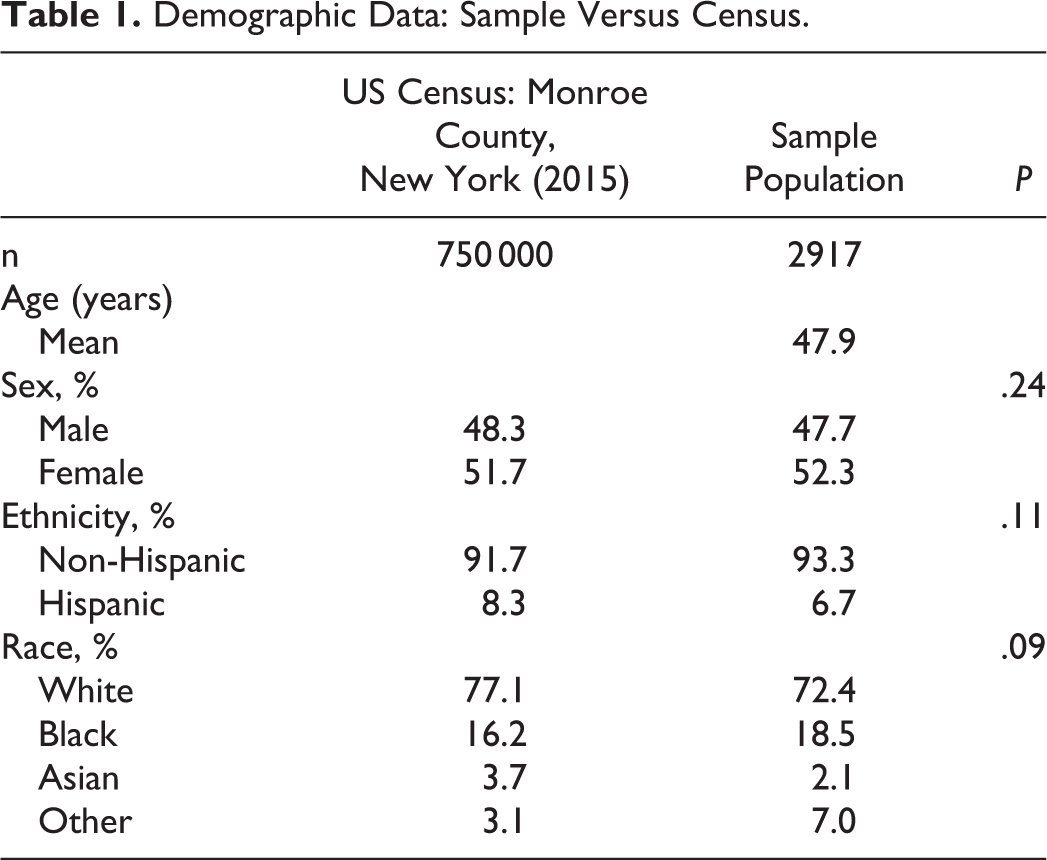
A total of 2917 patients qualified for the study, satisfying criteria and with appropriate imaging. US Census data for the local county is included (Table 1). Demographic data demonstrates no significant difference between the sample population and US data with respect to distribution of gender (P = .24), ethnicity (P = .11), and race (P = .09) (Table 1). Mean age of the sample population is 47.9 years.
Demographic Data: Sample Versus Census.
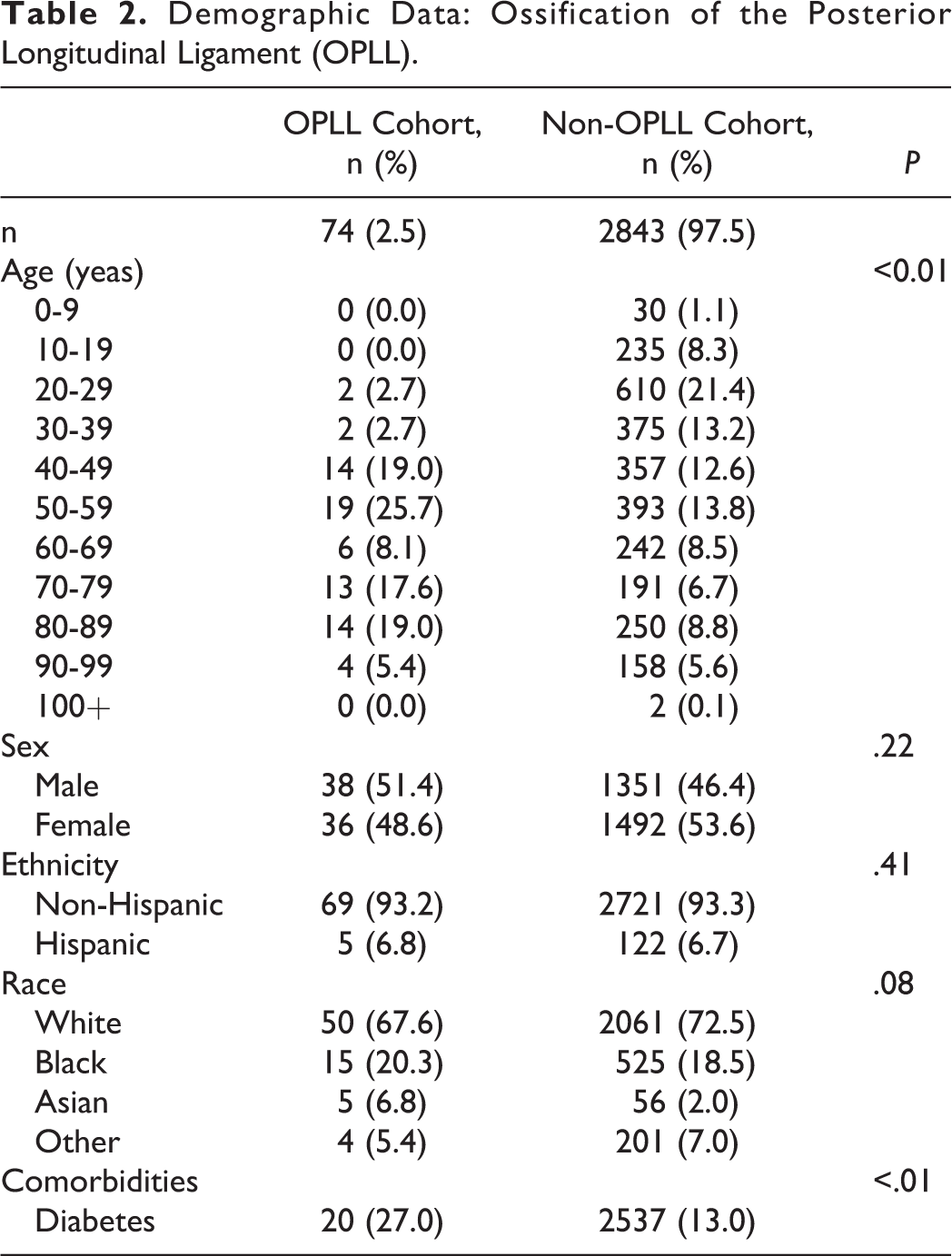
Seventy-four patients were diagnosed with OPLL via CT scan, for a prevalence of 2.5% (Table 2). Chi-square analysis of age distribution shows a significant difference between the OPLL and non-OPLL cohorts (P < .01). Among patients with OPLL, the greatest distribution was across ages 40 to 49 years (19.0%) and 50 to 59 years (25.7%). There was no difference between cohorts in distribution of sex (P = 0.22), ethnicity (P = 0.41), and race (P = 0.08). Race distribution was most different between groups with regard to the Asian designation (6.8% OPLL, 2.0% non-OPLL). The prevalence of diabetes was significantly different between the cohorts, 27.0% among OPLL patients and 13.0% among non-OPLL (P < 0.01).
Demographic Data: Ossification of the Posterior Longitudinal Ligament (OPLL).
Classification of the 74 patients in the OPLL cohort reveals 11 (14.9%) localized type, 50 (67.6%) segmental type, 4 (5.4%) continuous type, and 9 (12.1%) mixed type (Table 3). Mean number of levels involved include 2 levels for localized type, 3.4 levels for segmental type, 2.7 levels for continuous type, and 5 levels for mixed type. Distribution of levels involved are summarized, with most cases of OPLL starting at the C3 level (28.4%) and most cases ending at the C6 level (40.5%). 77% of cases involve levels below C5.
Ossification of the Posterior Longitudinal Ligament (OPLL) Cohort.
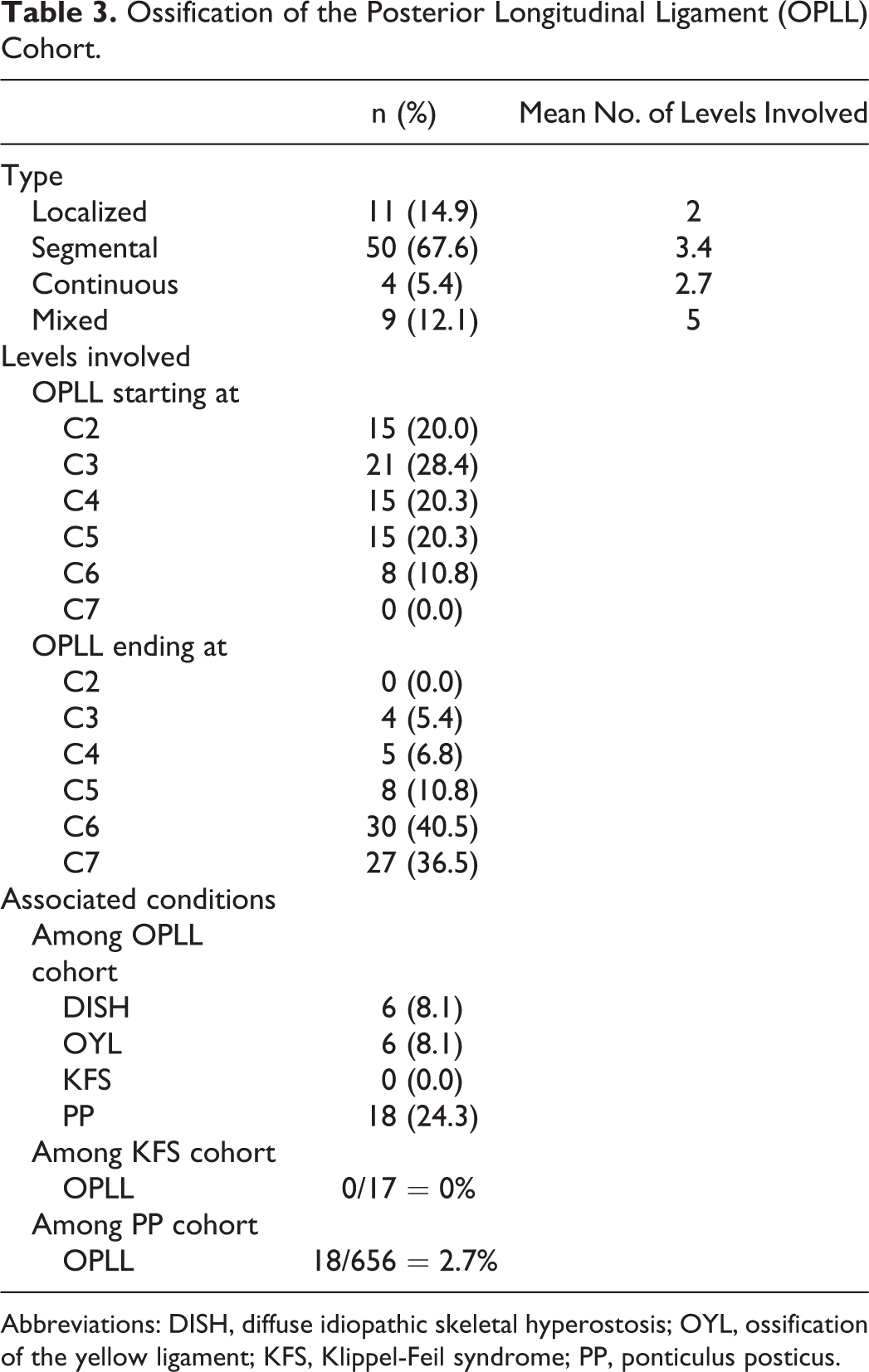
Abbreviations: DISH, diffuse idiopathic skeletal hyperostosis; OYL, ossification of the yellow ligament; KFS, Klippel-Feil syndrome; PP, ponticulus posticus.
Associated conditions among the OPLL cohort include DISH, seen in 6 (8.1%) patients, and OYL, seen in 6 (8.1%) patients as well (Table 3). There were no cases of KFS diagnosed on CT scan amongst the OPLL cohort, while there were 18 (24.3%) patients with OPLL that were diagnosed with concurrent PP.
Discussion
OPLL is not a common diagnosis, with most of the available literature addressing clinical presentation and symptomology. Onset of OPLL is most common in men, in the fifth or sixth decade of life. 19,20 Symptoms are variable, although most significantly, OPLL can cause myelopathy, especially in the cervical spine. 21,22 The exact cause of symptoms is a combination of both static and dynamic factors, as the ossified ligament results in direct compression on the spinal cord in addition to restricting range of motion of the spine. Greater space occupancy of the lesion increases likelihood of developing myelopathic symptoms. 1,23 Myelopathic progression often occurs and can lead to severe disability. Patients at risk for progressive symptoms include those with preexisting cervical stenosis or earlier age of onset. 1,24 Radiculopathy can also occur at levels specifically affected by the presence of OPLL.
When associated with trauma, the presence of OPLL requires a heightened level of concern, similar to the management of cervical DISH. As a space-occupying lesion, areas of ossification are associated with cervical stenosis. Spinal cord injury can therefore occur even without fracture. With OPLL, patients are predisposed to spinal cord injury (SCI) after minor trauma, such as a fall. 25,26 In continuous OPLL, SCI is often at the caudal end of spinal involvement due to the stiff segment and long lever arm. In segmental OPLL, SCI usually involved the intervening disk level. 26 This is due to the concentration of stress between 2 stiff segments when a force, such as trauma, is applied.
Management of this condition is variable, and often a function of symptomology. If asymptomatic, or presenting with radiculopathy, nonoperative management is pursued with physical therapy, oral analgesia, and monitoring. 27 Surgical intervention, through a variety of approaches, is reserved for severe or progressive myelopathy, or failure of nonoperative management. 28
Among existing OPLL literature, there are few studies that focus on North American patients. Fewer still evaluate the relationship of cervical OPLL with other spinal comorbidities, or the distribution of spinal involvement, in as many patients (2917). Thus, there are a multitude of valid conclusions that can be drawn from this cross-sectional study.
Compared with census data, there were no significant differences between the sample population and the population in the Fingerlakes, New York geographic region. This is a prerequisite for a sound epidemiological survey, as it supports the generalizability of findings from this study. Prevalence of OPLL was found to be 2.5% across the sample. This is in line with previous studies demonstrating a prevalence of 0.6% to 2%. 1,16
Distribution of age among patients with OPLL shows a significant difference from the sample, as is expected, with previous literature establishing diagnosis of OPLL at an average age of 50 years or greater. 19,20 This study does not determine onset of OPLL, or incidence, but rather prevalence. Interestingly, the OPLL cohort demonstrated a significant number of patients, 14 (19.0%), with OPLL of age 40 to 49 years. While this does not suggest age of onset, it demonstrates that this condition does have significant prevalence in this age cohort, and therefore should be taken into consideration in preoperative planning. Prevalence was also high from ages 50 to 89 years, which supports previous literature.
The difference in distribution among genders was not statistically significant in the OPLL cohort; however, there was a slightly higher prevalence in men, in agreement with previous studies. The distribution of race between the groups was not significantly different. However, due to the limited size of the OPLL cohort, any minor differences would not easily reach statistical significance. While the subset of Asian patients suggested a higher rate of prevalence (6.8% vs 2.0%), the effect on distribution across race overall was inconsequential. The burden of comorbid diabetes mellitus was higher among OPLL patients (27.0% vs 13.0%) (P < .01), which supports the previously established correlative relationship between these conditions. 8
With analysis of a cohort this size, OPLL can be better characterized than in previous studies. Table 3 demonstrates that segmental type is the most common type (67.6%), followed by localized, mixed, and continuous. Continuous type is the least common (5.4%). Mean number of levels involved includes 2 for localized type, 3.4 for segmental, 2.7 for continuous, and 5 for mixed. Level involvement of the cervical spine in OPLL is described as well; the starting level of OPLL is variable and distributed fairly evenly from C2 to C5. The endpoint of cervical involvement is most commonly at C6 (40.5%) or C7 (36.5%), which informs surgical planning. Because of the prevalence of involvement so caudal in the cervical spine, these levels should be carefully evaluated when determining the extent of OPLL in a preoperative surgical evaluation.
Review of associated conditions reveals low prevalence of concurrent DISH (8.1%) or OYL (8.1%). While thought to be a hyperostotic condition, OPLL does not share a direct relationship with either of these conditions. However, this study suggests there may be some degree of correlation. Among the 74 OPLL patients, 18 (24.3%) had concurrent PP. As PP is a congenital condition, there is no expected correlation. Additionally, the prevalence in the general population approximates 20%, so 24.3% in the OPLL cohort does not reliably suggest a relationship. 29
This study has limitations. Although the sample size is robust with 2917 CT surveys, it is limiting because of the low prevalence of OPLL. Additionally, indications for CT surveys were not restricted to exclude known myelopathy. This may introduce mild bias in patient selection. However, with a sample size of 2917 this is largely mitigated. Also, it must be noted that epidemiologic conclusions drawn from this study group may not be representative of the symptomatic population that present for medical evaluation, as these CT findings were largely incidental. Further analysis of degree of cord compression would be helpful, although it would likely require MRI. Other avenues for future study include increasing the sample size to better illustrate differences, due to the low prevalence of this condition. Additionally, correlating imaging findings with symptomology would provide insight. There were no attempts made to characterize if the patients developed symptoms associated with the OPLL. A study of incidence in addition to prevalence may yield additional information. The above findings of associated conditions identify a role for continued genetic study to further characterize any potential relationships with DISH, OYL, or PP.
Conclusion
Ossification of the posterior longitudinal ligament is uncommon in North America, and therefore poorly understood and characterized. This study provides a high-volume exploration of patients with incidental OPLL, better characterizing asymptomatic prevalence of pathology and indicating a significant relationship with diabetes. Segmental OPLL is the most common type. The caudal extent of OPLL typically involves levels C6 or C7. While there are multiple avenues for further study, this study provides a better epidemiological understanding of this uncommon condition.
Footnotes
Authors’ Note
This study was approved by the University of Rochester Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.