
Abstract
Study Design
Retrospective comparative study.
Objective
To investigate the relationship between pedicle Hounsfield Unit (HU) values and transpedicular screw malposition in scoliosis surgery and to determine a predictive HU threshold for malposition risk.
Methods
Patients who underwent free transpedicular screw fixation for idiopathic or degenerative scoliosis between 2011 and 2024 and had both preoperative and early postoperative spinal computed tomography (CT) scans available were retrospectively reviewed. Screw malposition was identified on postoperative CT, and pedicle HU values and the widths of malpositioned screws were measured on the corresponding preoperative CT images and compared with contralateral and control pedicles. Receiver operating characteristic (ROC) analysis was used to determine a predictive HU threshold for screw malposition.
Results
The study included 121 patients. Mean HU values were significantly higher in malpositioned pedicles compared to controls in both the idiopathic (692 vs 299.5; P < 0.001) and degenerative scoliosis (343.5 vs 250; P < 0.001) groups. ROC analysis determined the HU cut-off value to be 479 and above to predict screw malposition (AUC = 0.796; 95% CI: 0.717-0.876; sensitivity 73.6%, specificity 79.6%). The location of screw malposition according to the convex and concave sides, and the location above and below the apex did not show any significant differences.
Conclusion
Higher pedicle HU values are significantly associated with screw malposition in scoliosis surgery. A HU threshold of 479 may help identify pedicles at increased risk of malposition during free screw placement in both idiopathic and degenerative scoliosis. Preoperative pedicle HU assessment may contribute to surgical planning and risk reduction strategies.
Keywords
Introduction
Transpedicular screw fixation has been widely used for spinal stabilization and deformity correction since its introduction by Boucher in 1959.1-6 Despite advances in technique, screw malposition remains a significant concern in deformity surgery, with reported rates ranging from 8% to 22%.7-9 In complex spinal deformities, this rate can range from 5% to 41%.10-13 Although navigation systems can consistently improve screw placement accuracy compared with freehand techniques,10-13 they are not universally available and can increase cost and operative time.10,14,15 Also, access to navigation systems is limited in many parts of the world. Therefore, freehand techniques are widely used in many settings. Identifying pedicles at increased risk of malposition during freehand screw placement before surgery can allow for the implementation of predictive strategies (e.g., altered entry points, careful trajectory adjustment, or selective use of aids) and potentially reduce neurovascular complications.8-14
Hounsfield Units (HU), derived from routine CT scans, provide a simple and reproducible surrogate for local bone mineral density and trabecular quality.15-24 HU has been associated with clinically relevant endpoints such as osteoporosis screening, vertebral degeneration, and implant-related complications. The relationship with implants has been particularly important in the literature through studies predicting implant subsidence or loosening.16-31 Previous studies have primarily evaluated HU as a predictor of postoperative stability (e.g., screw loosening) rather than initial technical accuracy at the time of screw placement.16-31 Asymmetric loading in scoliosis may lead to regional differences in trabecular structure,17,24,25 but it remains unclear whether these differences increase the risk of malposition during drilling/tapping.
Scoliosis surgery involves correcting the deformity by placing pedicle screws.24,27 Screw malposition remains a significant challenge in scoliosis surgery, as in all procedures involving transpedicular screw placement.8,9,25,30,31 The causes of malposition have been extensively studied. Previous reports have suggested that screw location relative to the apex of the scoliosis21,23 and higher Cobb angles21-23 may increase malposition risk. In our clinical practice, we have observed that pedicle bone density—reflected as pedicle stiffness perceived by the surgeon—is highly influential in screw malposition, particularly in free-hand scoliosis surgeries. This observation prompted us to design the present study. The relationship between bone density and HU values has been well documented in prior studies,28-35 which further motivated us to evaluate pedicle HU values alongside other variables.
From a technical perspective, very dense (sclerotic) pedicles may resist smooth advancement of the pedicle probe along the ideal cancellous path, increasing the risk of slight stripping or reorientation during freehand insertion, even if the intended starting point and gross trajectory are correct. In this context, HU, reflecting local pedicle bone density, can serve as a practical preoperative marker to identify “difficult” pedicles where maintaining the ideal trajectory is more difficult. Therefore, the primary objective of this study was to investigate the relationship between pedicle HU values and transpedicular screw malposition in scoliosis surgery and to determine a predictive HU threshold for malposition risk using the Youden index and ROC analysis. Secondary objectives were to investigate whether this relationship varied according to scoliosis etiology (idiopathic or degenerative), curve anatomy (convex/concave; supra-apex/infra-apex/at-apex), medial or lateral fracture pattern, and pedicle thickness. We hypothesized that higher pedicle HU values might be associated with an increased risk of screw malposition during freehand insertion, and that a predictive risk value could be derived to guide preoperative planning.
Design and Methods
The study was approved by the Ethics Committee of the Faculty of Medicine of xxx University (Selcuk University, Konya, Turkey, 2024/543). Informed consent was not obtained due to the retrospective nature of the study. This retrospective study included patients with degenerative and idiopathic scoliosis who underwent surgery at our clinic between 2011 and 2024. Patients were eligible if they had both preoperative and postoperative spinal CT scans and if screw malposition was detected on early postoperative follow-up CT scans.
Patient and Data Selection
Screw malposition was defined as a ≥2 mm cortical tear in the medial or lateral direction on postoperative CT images or any screw trajectory impinging on adjacent neural or vascular structures. All scans were independently evaluated by 2 spine surgeons, and discrepancies were resolved by consensus. Patients diagnosed with idiopathic or degenerative scoliosis who underwent thoracic, thoracolumbar, or lumbar transpedicular screw placement were included in the study. All surgeries were performed by a single, experienced surgeon using a freehand technique. The study cohort consisted of pediatric patients with idiopathic scoliosis and elderly patients with degenerative scoliosis. For each case, the thickness and HU values of the pedicles with screw malposition were compared with the contralateral pedicle of the same vertebra without malposition and with all control pedicles in the study. Pedicles with screw malposition were analyzed in relation to patient sex, mean age, scoliosis etiology, location relative to the curve apex, location within the scoliotic curve (convex or concave side), direction of malposition relative to the midline (medial or lateral), and pedicle thickness and HU values. Measurements of pedicle thickness and HU values were initially performed by a single neurosurgeon with more than 10 years of experience. The same measurements were then independently repeated by a second neurosurgeon with more than 5 years of experience, and no clinically significant discrepancies were identified. Therefore, the original measurements were retained as the final data set for analysis. Because only a single final set of measurements was included in the statistical analysis, intraclass correlation coefficient (ICC) values could not be calculated.
Measurement Methods
The pedicle of the malpositioned screw was evaluated on preoperative CT images. Pedicle thickness and HU values were measured on axial CT slices (Figure 1). (A) Pedicle HU measurement method, (B) Pedicle thickness measurement method (mm)
Evaluators were provided with a detailed measurement guide defining anatomical landmarks, slice selection criteria, and ROI placement for HU and diameter measurements. The prepared measurement guide was as follows: 1. In spinal computed tomography, the pedicle measurement area should be determined from the axial image corresponding to the screw projection of the desired pedicle in sagittal sections. 2. The sclerotic structure of the bone cortex should not be included in the measurements (especially to ensure that the HU measurement represents the spongy bone, care should be taken to measure the pedicle from inside the spongy bone).
Assessment Criteria: • Position of the malpositioned screw relative to the apex (above, at, or below the apex) • Comparison of pedicle thickness and HU values of malpositioned screws with control pedicles • Differences in these parameters between degenerative and idiopathic scoliosis groups
Statistical Analysis
All statistical analyses were performed using SPSS version 22 (SPSS Inc., Chicago, IL, USA). Data normality was assessed using the Shapiro–Wilk test. Comparisons of categorical variables were conducted using Pearson’s chi-square test or Fisher’s exact test, as appropriate. Continuous variables that were not normally distributed were compared between groups using the Mann–Whitney U test. A P value of <0.05 was considered statistically significant.
A power analysis based on the observed AUC of 0.796 demonstrated that a minimum of 23 patients would be required to achieve 80% power at α = 0.05; therefore, our cohort of 121 patients was adequately powered for ROC analysis.
Given the exploratory nature of subgroup analyses, no formal adjustment for multiple comparisons was applied. Subgroup findings are interpreted with caution; these analyses were performed to assess the consistency and potential generalizability of the HU threshold (≥479) across anatomical contexts.
Inter-measurement reliability was assessed using the Intraclass Correlation Coefficient (ICC), calculated using a two-way random effects model. The absolute agreement approach was adopted in the analysis, and single-measure ICC values were reported along with 95% confidence intervals (CI). ICC values were interpreted as: <0.50 low, 0.50-0.75 moderate, 0.75-0.90 good, and >0.90 excellent reliability. Interobserver measurement agreement was evaluated using Bland–Altman analysis. In this analysis, the mean difference (bias) and 95% agreement limits were calculated. The presence of proportional bias was examined by evaluating the relationship between the differences and the magnitude of the measurements in the Bland–Altman plots.
Results
Demographic and Clinical Characteristics According to Etiology
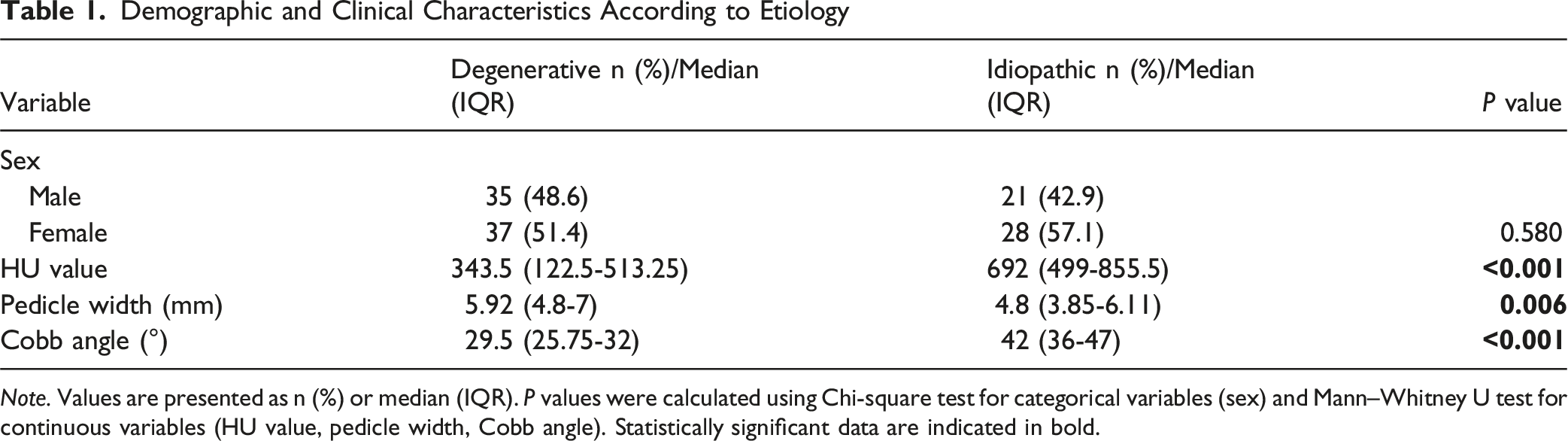
Note. Values are presented as n (%) or median (IQR). P values were calculated using Chi-square test for categorical variables (sex) and Mann–Whitney U test for continuous variables (HU value, pedicle width, Cobb angle). Statistically significant data are indicated in bold.
The regional distribution of scoliosis in the patients included in the study was 62.8% (n: 76) thoracolumbar, 36.3% (n: 44) lumbar and 0.8% (n: 1) thoracic, while in the degenerative group this distribution was 38.8% (n: 28) thoracolumbar, 61.1% (n: 44) lumbar region. In the idiopathic group, 97.9% (n: 48) thoracolumbar and 2.04% (n: 1) thoracic region.
The distribution of malpositioned screws in the degenerative and idiopathic groups was as follows; in the degenerative group, there was 48.6% (n: 35) convex, 51.3% (n: 37) concave screw malposition, while in the idiopathic group, there was 53.06% (n: 26) convex, 46.9% (n: 23) concave screw malposition. This distribution according to the apex of scoliosis was as follows; in the degenerative group, there were 40.2% (n: 29) malpositioned screws above the apex, 47.2% (n: 34) below the apex, 12.5% (n: 9) at the apex, while in the idiopathic group, this rate was as follows; 53.06% (n: 26) malpositioned screws above the apex, 42.8% (n: 21) below the apex, and 4.08% (n: 2) at the apex. No statistically significant difference was detected in these distributions.
Comparison of Characteristics of Medial and Lateral Screw Malpositions
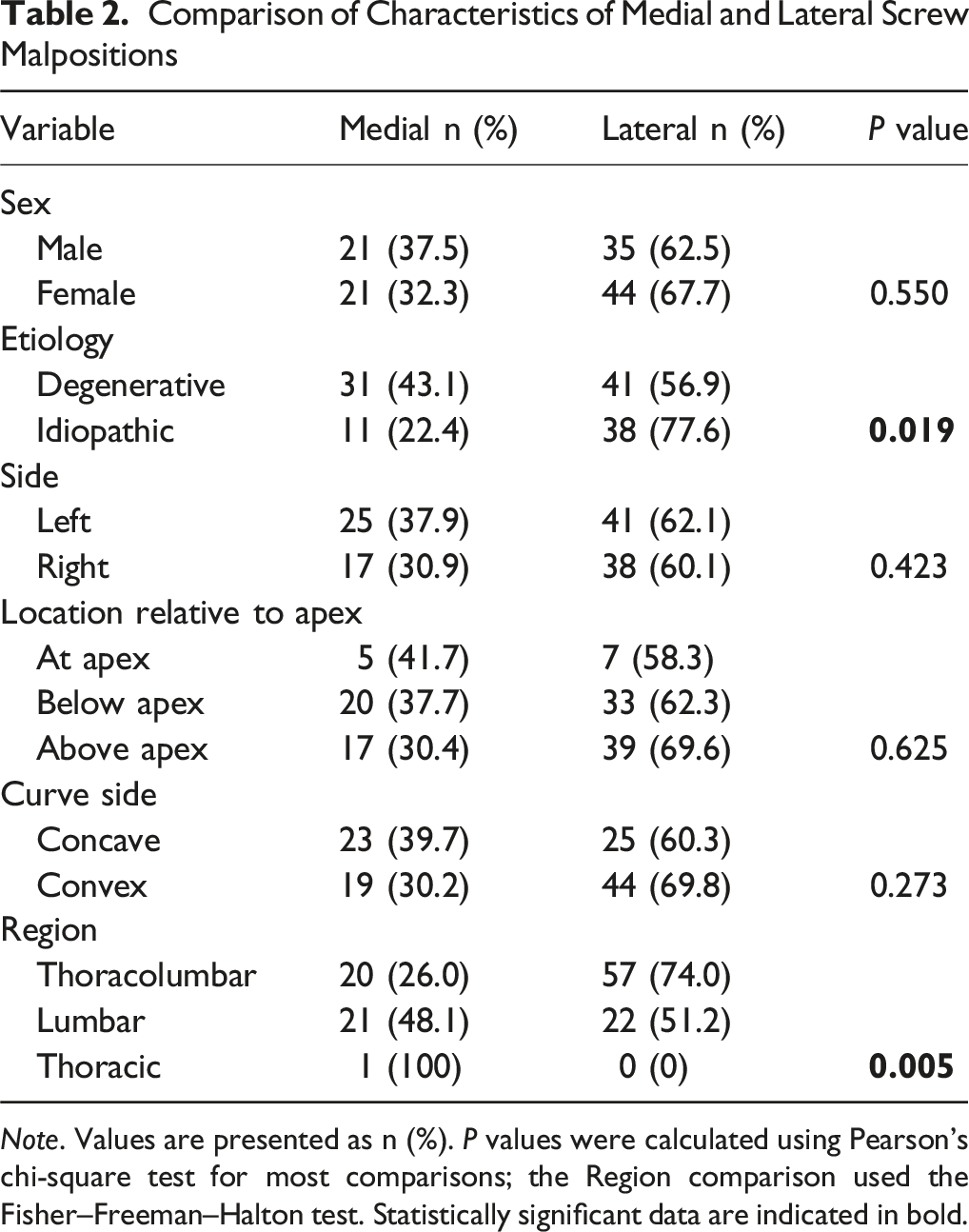
Note. Values are presented as n (%). P values were calculated using Pearson’s chi-square test for most comparisons; the Region comparison used the Fisher–Freeman–Halton test. Statistically significant data are indicated in bold.
Comparison of Pedicle HU Values and Widths According to Etiology
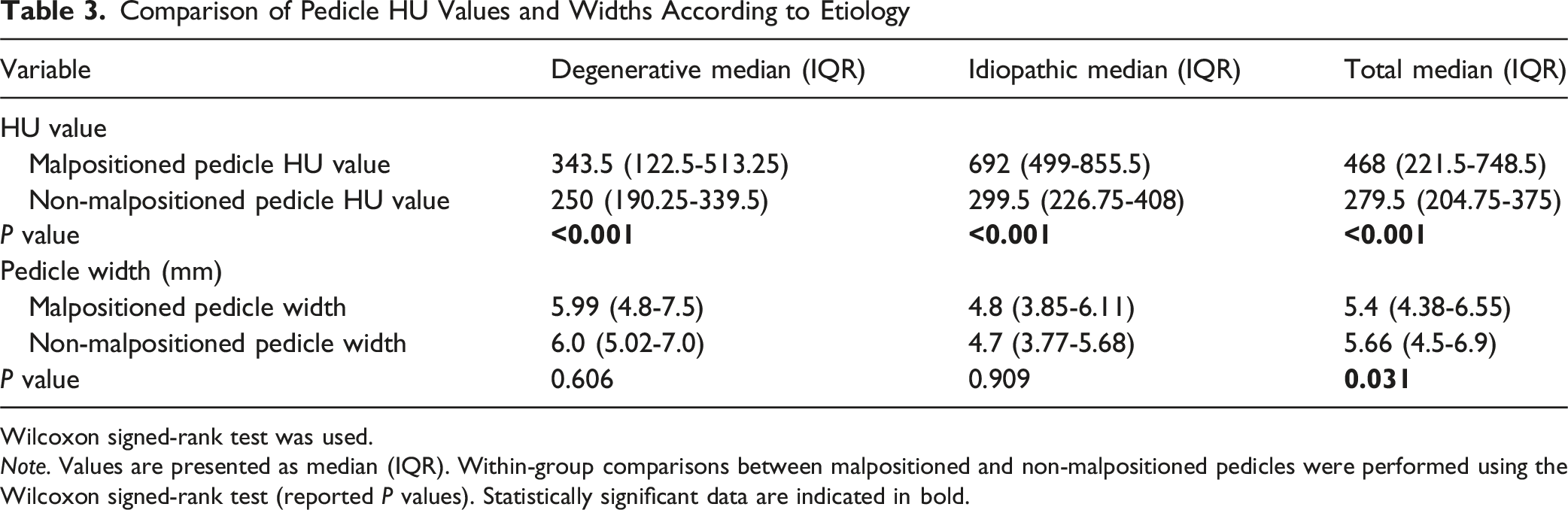
Wilcoxon signed-rank test was used.
Note. Values are presented as median (IQR). Within-group comparisons between malpositioned and non-malpositioned pedicles were performed using the Wilcoxon signed-rank test (reported P values). Statistically significant data are indicated in bold.
Because the mean HU values of pedicles with malpositioned screws were statistically significantly higher when evaluated both across all patients and within groups, a predictive HU value was investigated. In this study of all pedicles, the malpositioned pedicle HU value was calculated as AUC: 0.796 (95% confidence interval: 0.717-0.876, P < 0.001) according to ROC analysis, and when analyzed with the Youden index, the predictive HU value for pedicle malpositioned screws was calculated as 479 (79.6% specificity, 73.6% sensitivity) (Figure 2). Roc curve of pedicle HU value of malpositioned screw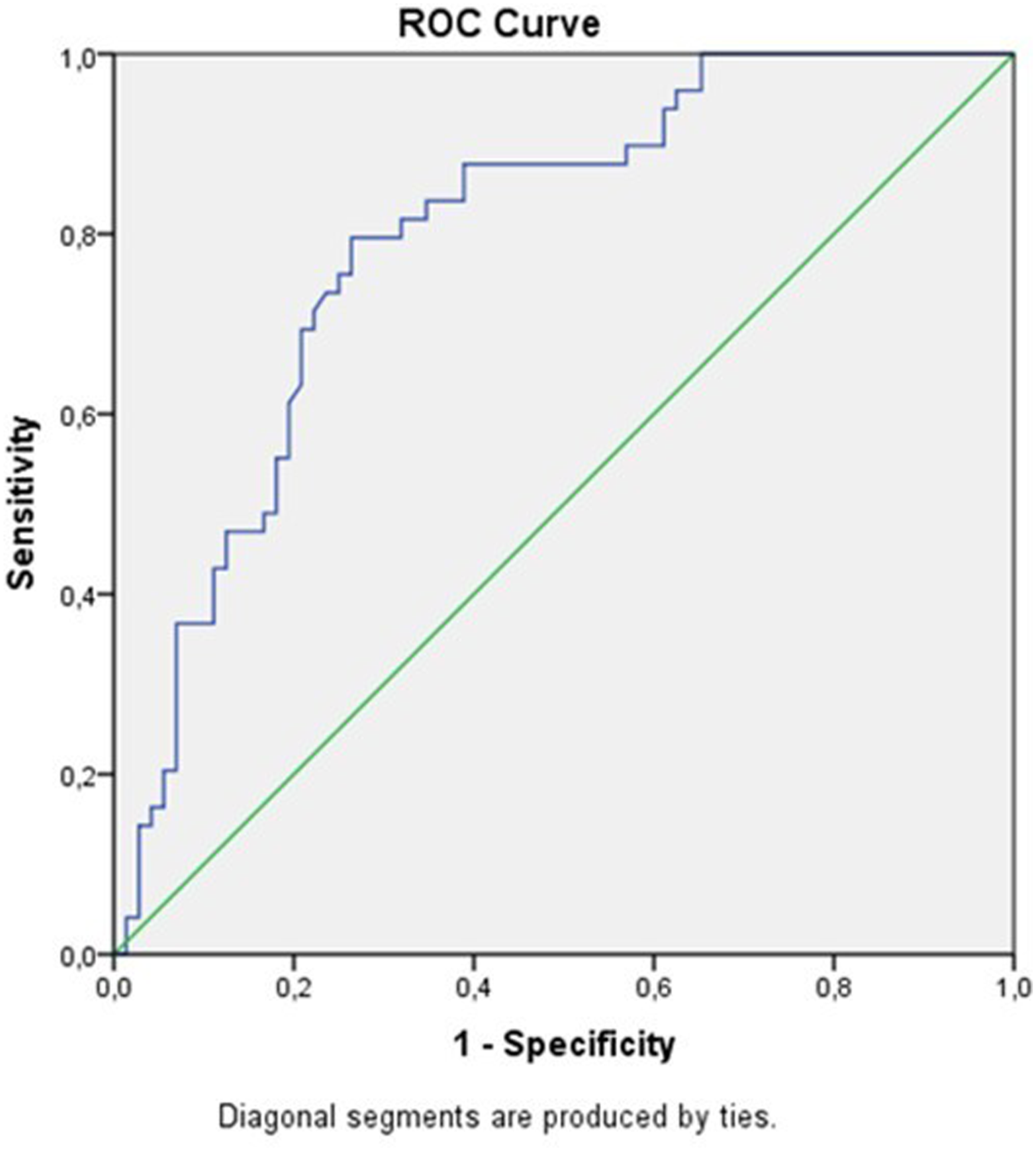
Our measurement technique was evaluated in independent data for Intraclass Correlation Coefficient (ICC) assessment. Measurements were performed by 2 independent neurosurgeons with 10 years of experience and repeated after 2 weeks. For the first evaluator, the intra-observer ICC value for the HU value measurement was found to be 0.992 (95% CI: 0.986-0.996), and for the second evaluator, the intra-observer ICC value was 0.997 (95% CI: 0.995-0.998). The inter-observer ICC value for the first HU value was found to be 0.982 (95% CI: 0.969-0.990). The inter-observer ICC value for the second HU value was found to be 0.992 (95% CI: 0.985-0.995). For the first evaluator, the intra-observer ICC value for pedicle thickness (mm) was found to be 0.968 (95% CI: 0.945-0.982), and for the second evaluator, the inter-observer ICC value was 0.992 (95% CI: 0.985-0.995). The intra-observer ICC value was determined to be 0.930 (95% CI: 0.880-0.960). For the first pedicle thickness (mm) measurement, the inter-observer ICC value was found to be 0.896 (95% CI: 0.824-0.940). For the second pedicle thickness (mm) measurement, the inter-observer ICC value was found to be 0.940 (95% CI: 0.897-0.965). The mean deviation between HU value measurements was found to be 9.34 (95% confidence interval: 137.01-118.33). The mean deviation between pedicle thickness (mm) measurements was found to be 0.16 (95% confidence interval: 2.06-1.74) (Figures 3-4). The ICC ranges of our study are between good and excellent. Bland–Altman plot for pedicle thickness (mm) measurement Bland–Altman plot for HU measurement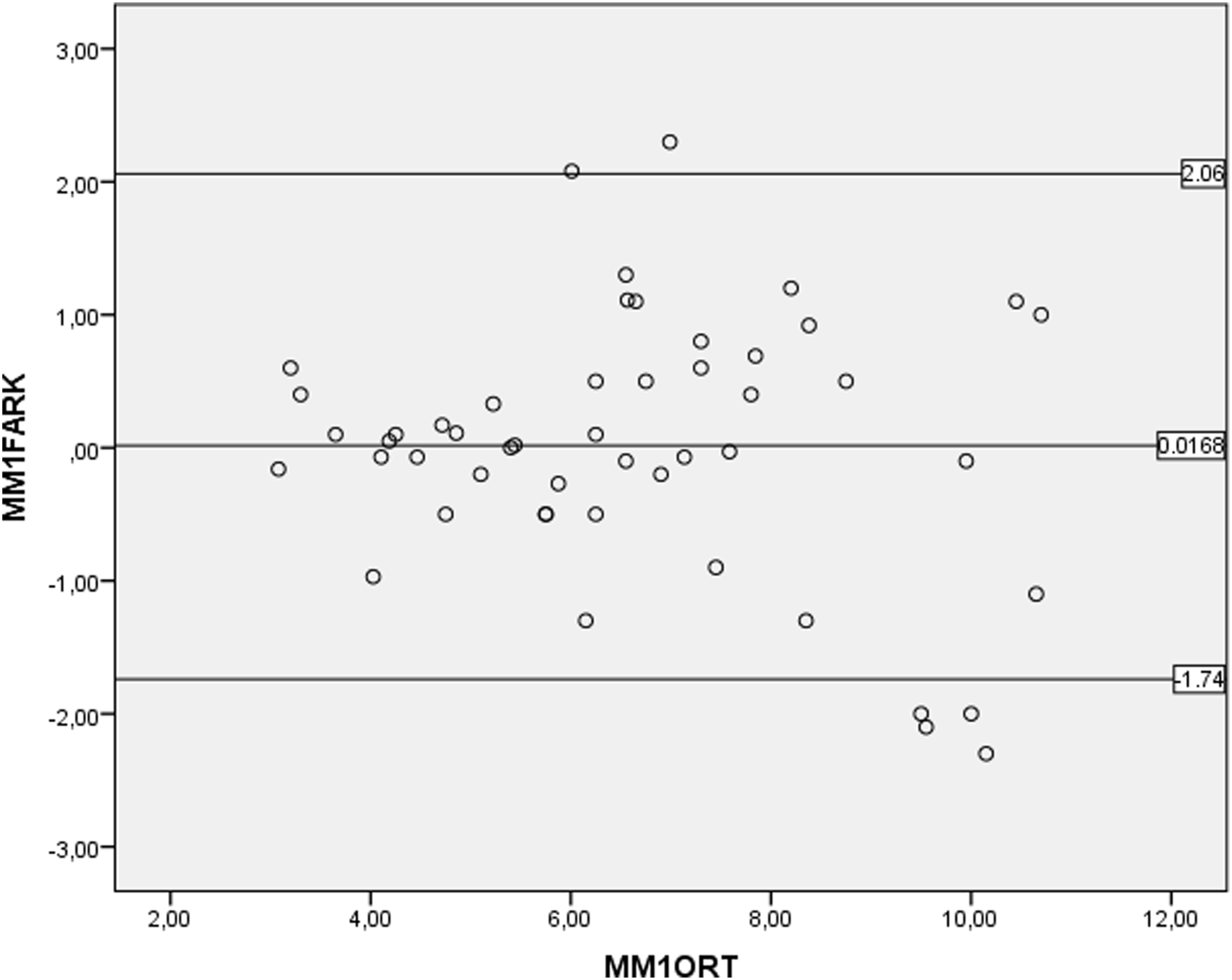

Discussion
In this retrospective study, which included patients with idiopathic and degenerative scoliosis who were operated on by a single surgeon and whose screw malposition was detected on routine postoperative spinal CT scans, our primary finding was that higher pedicle HU values were associated with an increased risk of pedicle screw malposition during freehand scoliosis surgery, with a predictive threshold of ≥479 (AUC 0.796) obtained from ROC analysis. This threshold remained consistent across anatomic and etiologic subgroups, supporting its potential utility as a practical preoperative marker for identifying high-risk pedicles. Clinically, preoperative identification of pedicles with a HU ≥479 can help surgeons anticipate technical difficulties during free screw placement. This threshold can guide adjustments in entry point selection, trajectory planning, guiding technique, or selective use of fluoroscopy/navigation in high-risk pedicles. Therefore, HU-based risk estimation has the potential to improve intraoperative safety, reduce malposition rates, and contribute to personalized deformity surgery planning. In practical application, basing pedicle screw placement decisions on pedicles on preoperative spinal CT scans is an idea inspired by the work of Gertzbein and Robbins, who pioneered this study and demonstrated the validity and reproducibility of pedicle assessment on spinal CT. 36
When the pedicle characteristics of the malpositioned screws were evaluated together with their thickness, location relative to the scoliosis (e.g., convex vs concave side; supra-apical vs infra-apical vs apical), and scoliosis characteristics (idiopathic, degenerative, Cobb angles, etc.), no significant differences were detected, making the obtained information clinically applicable to other patients. When pedicle thickness was evaluated in all patients, pedicle thicknesses were significantly less in the idiopathic group. However, when analyzed within each group, there was no statistically significant difference in thickness between the malpositioned and control pedicles (Table 3). When all pedicles, including controls, were evaluated, idiopathic scoliosis patients showed significantly higher HU values but significantly lower pedicle thicknesses. This finding, consistent with previous literature,24,25,28 may be attributed to the younger age of idiopathic scoliosis patients and the absence of significant bone mineral density loss. In degenerative scoliosis, age-related bone loss and degenerative trabecular changes appear to reduce HU values.27,30,32,34,35 Although the mean Cobb angle was higher in the idiopathic group, no significant difference in Cobb angle was observed between patients with malpositioned screws and controls. Contrary to some reports,25,27 increasing the Cobb angle was not associated with a higher risk of malposition in our series. Similarly, screw malposition was not significantly associated with being located at, above, or below the curve apex, likely reflecting the effect of all procedures being performed by a single experienced surgeon.
One notable finding was the predominance of screw malposition in the thoracic region and a tendency toward lateral breaches. A majority of patients had thoracolumbar scoliosis (63.6%). All idiopathic scoliosis patients (100%, n = 49) underwent surgery involving the thoracolumbar region, compared with 38.8% (n = 28) of degenerative scoliosis patients. In the idiopathic group, the higher frequency of malpositioned screws in the thoracic region was considered related to differences in stabilization site distribution between groups. The lateral bias in the idiopathic group may be explained by the surgeon’s deliberate avoidance of medial penetration in the thoracic region. In a previously published study by the same surgeon, no postoperative complications were observed with lateral pedicle wall breaches, whereas medial breaches resulted in neurological complications in 44.4% of cases (radicular pain and motor weakness). 26 This tendency to avoid the medial wall may have contributed to the increased lateral malposition rate.
Previous scoliosis studies have shown that one pedicle of a given vertebral body may exhibit denser cancellous bone, while the contralateral pedicle may exhibit softer or more normal trabecular structure.27-32 This is primarily explained by Wolff’s law, which states that bone tissue remodels in response to mechanical loading and that changes in bone mass distribution occur to adapt to the load without microdamage or fracture.23-38 In our study, we did not attempt to validate our findings with Wolff’s law. Conversely, if Wolff’s law were the dominant mechanism, we would expect increased pedicle density on the convex side and, consequently, a higher concentration of malposition on the convex side.37-39 However, neither the convex-concave comparison nor the distribution based on the apex (above/beside/below) showed significant differences in our cohort. In the entire sample, HU values were significantly higher in malpositioned pedicles compared to non-malpositioned controls (Table 3). These observations suggest that Wolff’s law alone is insufficient to explain this phenomenon. Instead, we propose that localized sclerotic pedicles (HU ≥479) may impede the smooth advancement of the pedicle probe and make it difficult to reach the vertebral body; even if the initial trajectory is correct, the increased resistance may cause slight stripping or reorientation during free screw insertion, predisposing to malposition. Subgroup comparisons (apex location, concavity/convexity, pedicle thickness) were intentionally conducted to test whether the HU cutoff value (≥479) retains its validity in different anatomical contexts. The absence of significant subgroup effects supports the robustness and potential generalizability of this cutoff value for routine application.
The HU values obtained in our study and our clinical experience should not be compared to the better implant retention or lower risk of loosening found in previous studies with higher HU.30-35 The final point here is initial technical accuracy: in very dense (sclerotic) pedicles, advancement of the probe along the ideal cancellous trajectory may be more difficult and may predispose to slight stripping or redirection despite an accurate entry point; these mechanisms are more relevant to freehand techniques and can be mitigated by navigation.10-14 Therefore, we interpret the HU threshold as a warning sign of intraoperative difficulty, not as a marker of poor fixation quality.
Importantly, most HU loosening studies measure HU from the vertebral body and assess postoperative stability (looseness)15-35; However, this study targeted an intraoperative endpoint (initial malposition) and measured HU specifically within the pedicles, that is, in the actual transpedicular corridor used during screw placement. The numerical HU values obtained in this article and their clinical interpretations are not directly comparable across these literatures.15-35 Therefore, our findings complement, rather than contradict, previous studies focusing on loosening by highlighting a different mechanism and measurement domain related to freehand trajectory control.
Conclusion
This is an original study evaluating the relationship between pedicle characteristics and screw malposition during transpedicular screw placement in scoliosis surgery. In the literature, HU values are generally examined for the identification of osteoporotic vertebrae or the malposition of fusion instruments such as intervertebral cages. However, a specific threshold value for using pedicle HU to predict the risk of malposition during transpedicular screw placement has not been previously reported in the literature.
Pedicle HU ≥479 predicts increased malposition risk during freehand scoliosis surgery (AUC 0.796) and appears applicable across subgroups. Surgeons should consider added trajectory safeguards when HU is high; external validation is warranted.
Limitations
This study has limitations. Its retrospective design is a primary limitation. While the fact that all surgeries were performed by a single experienced surgeon ensures procedural consistency, it may limit the generalizability of the results to less experienced operators or different surgical techniques.
Footnotes
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Ethics Committee of the Charité University Hospital in Berlin, Germany; EA4/046/16) and with the Declaration of Helsinki (1964) and its later amendments or comparable ethical standards.
Author Contributions
Concept and design: DKG, EK, FH, MS. Data collection: DKG, MS, SUA, FMÖ, EYO, MSŞ, NR. Data interpretation: DKG, EK, FH, HK. Statistical analysis: DKG. Writing of the manuscript: DKG, NR. Critical revision of the manuscript for important intellectual content: all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.