
Abstract
Study Design
Biomechanical analysis of lateral mass screw pullout strength.
Objective
We compare the pullout strength of our bone cement–revised lateral mass screw with the standard lateral mass screw.
Methods
In cadaveric cervical spines, we simulated lateral mass screw “cutouts” unilaterally from C3 to C7. We salvaged fixation in the cutout side with polymethyl methacrylate (PMMA) or Cortoss cement (Orthovita, Malvern, Pennsylvania, United States), allowed the cement to harden, and then drilled and placed lateral mass screws back into the cement-augmented lateral masses. On the contralateral side, we placed standard lateral mass screws into the native, or normal lateral, masses and then compared pullout strength of the cement-augmented side to the standard lateral mass screw. For pullout testing, each augmentation group was fixed to a servohydraulic load frame and a specially designed pullout fixture was attached to each lateral mass screw head.
Results
Quick-mix PMMA-salvaged lateral mass screws required greater force to fail when compared with native lateral mass screws. Cortoss cement and PMMA standard-mix cement-augmented screws demonstrated less strength of fixation when compared with control-side lateral mass screws. Attempts at a second round of cement salvage of the same lateral masses led to more variations in load to failure, but quick-mix PMMA again demonstrated greater load to failure when compared with the nonaugmented control lateral mass screws.
Conclusion
Quick-mix PMMA cement revision equips the spinal surgeon with a much needed salvage option for a failed lateral mass screw in the subaxial cervical spine.
Keywords
Introduction
Various techniques exist for posterior fixation of the subaxial cervical spine, but by far the most common form of fixation in this region involves placement of lateral mass screws. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 The popularity of lateral mass screws arose from the ability to place screws under direct visualization, 4 , 5 , 9 , 10 , 11 , 12 , 13 the low risk of neurovascular injury, 1 , 2 , 3 and screw placement being less technically challenging than other fixation techniques. 9 , 10 , 11 , 12 The biomechanical strength of a lateral mass screw construct provides significant stability that may preclude the need for rigid immobilization during the postoperative period. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 Due to these advantages, lateral mass screws have become the treatment of choice for many spine surgeons when performing posterior fixation of the subaxial cervical spine.
Unfortunately, surgeons may encounter situations where lateral mass screws fail and are unable to be placed. Such instances include lateral mass screw cutout, screw loosening, or malpositioning. 3 , 12 , 13 In these situations, salvage techniques are required by the surgeon to achieve stable cervical fixation. Several salvage options exist for fixation, which include adding an extra level of fusion, anterior fixation, spinous process wiring, transfacet screw placement, intralaminar screw placement, and other revision screw techniques.
Although adding an extra level of fusion is a common salvage option, significant drawbacks exist with this option. Extending the fusion typically leads to longer operating room time with associated increased morbidity. There is certainly less postoperative motion, and longer fusions are thought to have greater potential for adjacent segment degeneration. 14 , 15 Anterior fixation is another option for salvage but requires a separate approach, which adds significant time and potential morbidity. Spinous process wiring techniques can be useful if no central decompression has been performed, but wiring does not provide rigid fixation and is associated with reduced fusion rates. 16 , 17 , 18 , 19 Translaminar screw fixation has proven to be a viable option for posterior stabilization at C2 and C7 13 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 ; however, this option is typically not available due to the thin lamina and anatomic variability found in the C3 to C6 segments of the subaxial cervical spine.
Other revision screw strategies include conversion of the failed lateral mass screw to a pedicle screw, placement of a larger-diameter and longer-depth lateral mass screw, and revision of the trajectory of the failed lateral mass screw. 7 , 29 , 30 , 31 Conversion to a pedicle screw construct is technically challenging and associated with an increased neurovascular risk due to the small and often cortical pedicles that are surrounded by the spinal cord centrally, the exiting nerve in the foramen, and the vertebral artery anterolaterally. 9 , 10 , 11 , 12 Placement of a larger-diameter lateral mass screw with a longer depth is certainly an option in some patients but often is not anatomically possible in patients with failed lateral mass screws. Revision of the trajectory of a failed screw carries a risk of nerve or arterial damage with each attempt, especially when the screw deviates from the typical “up-and-out” trajectory. In many cases where a lateral mass screw cuts out, a revision trajectory is not safe or is not possible. In these instances, surgeons would benefit from another salvage option.
Bone cement has previously been used to strengthen the bone–implant interface in the vertebral column. 32 , 33 , 34 , 35 Pitzen et al showed that a polymethyl methacrylate (PMMA) bone–cement screw interface provided a pullout strength and insertional torque that was greater than a bone–screw interface in the cervical spine using a bicortical 3.5-mm facet screw of 14-mm length (Spine System Evolution Cervical, Aesculap, Tuttlingen, Germany). 36 Based on this work, we postulate that bone cement may provide an interface that would allow for salvage of a failed lateral mass screw secondary to lateral cutout. To our knowledge, no study has analyzed the use of bone cement as a salvage option for a failed lateral mass screw.
The primary objective of this study was to create a lateral mass cutout at each level in the subaxial cervical spine, C3–C7; augment this defect with different types of cement and cementation techniques; and compare the pullout strength of this revision lateral mass screw with a nonaugmented lateral mass screw on the contralateral side.
Materials and Methods
Three fresh frozen osteoporotic human cadaveric cervical spines used in this study were stored in double plastic bags at –20°C. Considerable variability was found between the three cadavers, but all were scanned with dual-energy X-ray absorptiometry (DXA) to ensure T-scores were less than −2.5 (average DXA T-score −3.9 with standard deviation 0.8). Osteoporotic specimens were chosen because this patient population would most likely suffer the complication of lateral mass screw cutout. Each cervical spine had a control and test side. This allowed the best comparison of pullout strength of an augmented versus nonaugmented lateral mass screw. Use of osteoporotic spines also served as an internal control to more accurately account for the anatomic variability between each specimen.
These three specimens produced 15 subaxial cervical segments from C3–C7. On the control side, we placed lateral mass screws from C3–C7 in a standard fashion in all three specimens. We used an awl for the starting point, then a pilot hole was drilled with a 2.8-mm drill directed 30 degrees cranially and 20 degrees laterally to avoid the vertebral artery. 37 We placed 3.5 × 14-mm Oasys polyaxial screws (Stryker, Kalamazoo, Michigan, United States) into the lateral masses. We chose 14-mm-long screws for standardization purposes as this is a very commonly used length in vivo and is longer than the average depth of the lateral mass (12.83 ± 1.28 mm). 38
On the test side, a cutout was simulated at each of the levels extending from C3 to C7 (Fig. 1). The cutout model was defined by a defect in the lateral wall of the lateral mass such that a well-placed screw could no longer be maintained. This was done by drilling a bicortical pilot hole using the same starting point and trajectory as our control side, but a 3.5-mm drill was used instead to simulate the size of the lateral mass screw.
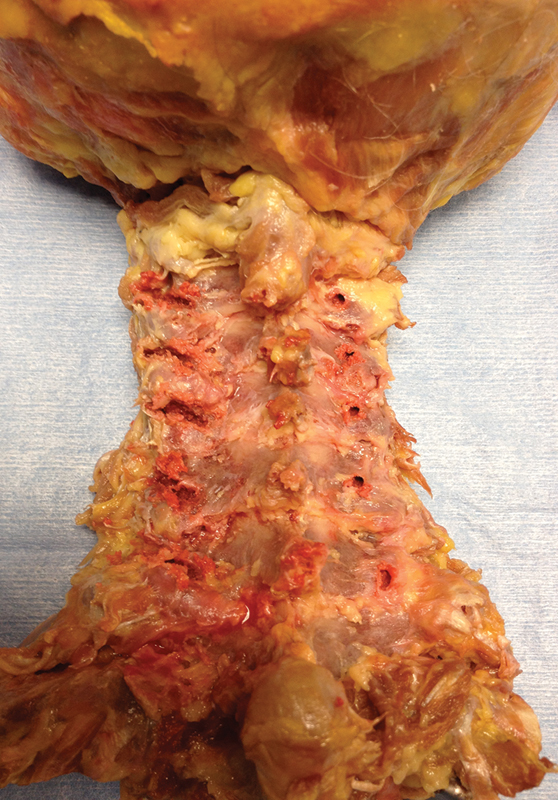
A cadaver specimen with failed lateral mass screw simulation in the contralateral lateral mass.
It was our intent to create a cutout model of the lateral mass with the resultant defect that often occurs in this situation, where the lateral wall of the lateral mass can no longer contain a well-placed screw. We also wanted to create a worse-case scenario so we used a 3.5-mm drill and made multiple passes, starting with a normal screw trajectory and then angling more cephalad and lateral until the lateral border of the lateral mass was a significant defect.
After drilling this bicortical pilot hole, the 3.5-mm drill was then used to make sequential bicortical passes progressively more cephalad and lateral until the drill no longer had purchase and the tract “cut out” with extension from the normal trajectory out the lateral portion of the lateral mass. We tried at every level to place a 3.5-mm screw, confirming that the screw would not have purchase and indeed would slide or cut out cephalad and lateral to the attempted trajectory. The medial portion of each canal was probed to assess for foraminal breach, confirming that no foraminal extravasation of the cement would occur after cement application.
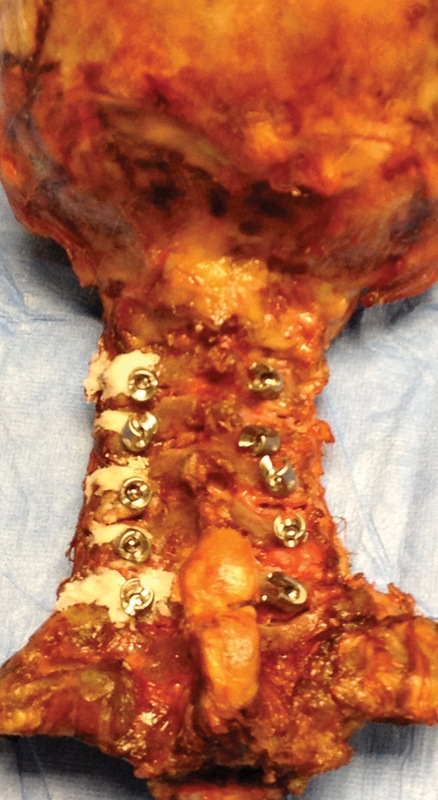
Cement was used to salvage the lateral masses (Fig. 2). In some cases, the cement went beyond simply filling the bony defect with some extravasation covering some of the lateral mass dorsally and laterally. Close three-dimensional visual inspection after cement application revealed no extravasation into the facet joints or ventrally into the vertebral or neural foramen. The same PMMA (Howmedica Osteonics Simplex P Bone Cement, Stryker) was used throughout our study with varying mixing times.

Cement on the left side of the cadaver was used to salvage the lateral masses after the simulated screw cutout.
In the first group, we used PMMA that was mixed for the recommended 2 minutes (standard-mix group). This PMMA was then placed in a large-bore syringe and injected to fill the defects in the lateral masses. The cement was allowed to harden 10 minutes prior to reinstrumentation. In the second group, we used PMMA that was mixed quickly just until homogeneous (∼30 seconds) and immediately placed in a large-bore syringe and injected to fill the defects in the lateral masses (PMMA quick-mix group). This “runny” quick mix allowed the cement to better fill the lateral mass cutout tract. The setting time prior to screw placement was ∼15 minutes in this second group (quick-mix). In third group, we used Cortoss (Orthovita, Malvern, Pennsylvania, United States) to augment the defects; it came with its own injection delivery device, which we used to apply the cement to the defects in the lateral masses. The setting time was nearly 1 hour for the Cortoss and yet grossly it still failed to achieve the hardness of the PMMA groups. In the augmented groups, a 2.8-mm drill was then used to drill a standard pilot hole through the cement in the lateral mass using the aforementioned typical lateral mass screw starting point and trajectory. No cracking of the cement was experienced during the cement drilling, although debonding at the bone cement interface occurred in some specimens. After drilling, 3.5 × 14-mm Oasys polyaxial screws (Stryker) were placed into the cement-augmented lateral masses (Fig. 3).
Final placement of the augmented and nonaugmented (control) lateral mass screws.
Groups instrumented with primary fixation included nonaugmented control (n = 15); augmented with PMMA and standard-mix (n = 5); augmented with Cortoss (n = 5); augmented with PMMA and quick-mix (n = 5).
After instrumentation, each spine was fixed rigidly to the table of a servohydraulic load frame (Instron 8821s, Norwood, Massachusetts, United States). A specially designed pullout fixture was attached to the head of the lateral mass screw (Fig. 4). Pure dorsal pullout force in line with the axis of the screw was applied to each lateral mass screw at a constant displacement rate of 0.2 mm/s until failure. Maximum pullout force at failure was recorded for each sample. Mean force to failure between native and augmented screws was compared for statistical significance using a Student t test with p < 0.05 considered significant.
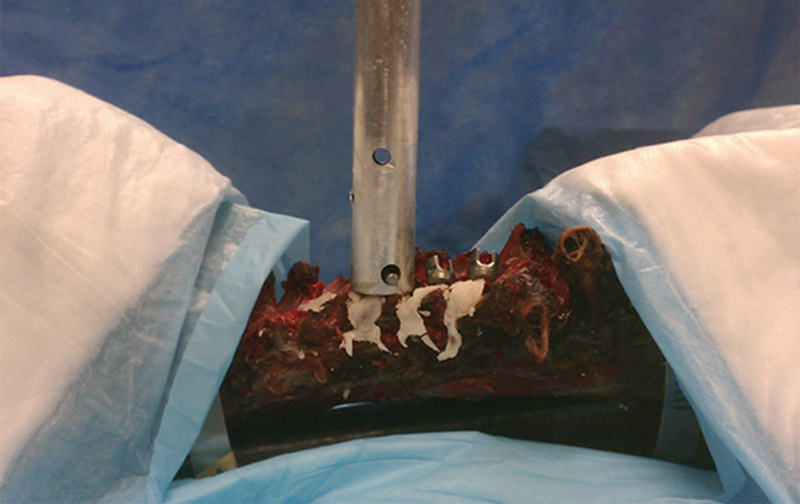
Test setup for pure pullout testing of lateral mass screws.
Results
Maximum load at failure for the three groups tested for primary fixation as compared with nonaugmented controls are shown in Fig. 5. Post hoc power analysis was performed for all groups using G*Power 3.0.10 with an α of 0.05. 39 Using samples sizes of five per group, the effect size determined by the mean and standard deviation allowed the power to be calculated for each group. The standard-mix PMMA (power: 0.99) and quick-mix PMMA (power: 0.96) obtained an adequate power when compared with the control group. The Cortoss group (power: 0.33) was underpowered and statistical conclusions cannot be drawn from our study. The nonaugmented control exhibited a significantly higher pullout strength than the primary cement augmentation repair for both the PMMA standard-mix (174.6 ± 26.6 N versus 61.8 ± 30.1 N, p = 0.001) and Cortoss cement (108.6 ± 13.0 N versus 79.0 ± 35.7 N, p = 0.04). Conversely, the nonaugmented control (standard native lateral mass screw) demonstrated a significantly lower force at failure as compared with the PMMA quick-mix (66.4 ± 42.1 N versus 151.0 ± 35.7 ± 13.4 N, p = 0.02).
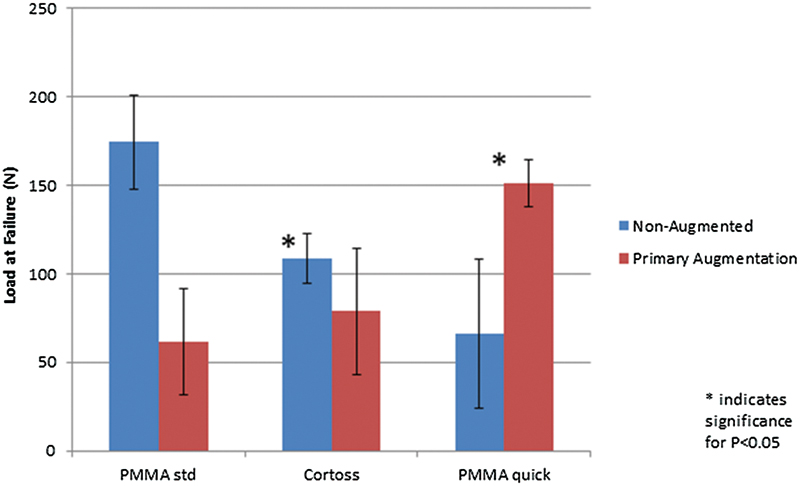
Maximum load to failure measured for three primary augmentation groups compared with nonaugmented contralateral controls (n = 5 per group). Abbreviations: PMMA, polymethyl methacrylate; std, standard.
Discussion
Benefits of bone cement revision of the lateral mass include quick and easy access to bone cement in most hospitals; minimal increase in operative time; no reliance on posterior elements such as lamina or spinous processes, which may be absent in a decompressed cervical spine; and direct visualization of screw placement. To our knowledge, no study has analyzed the use of bone cement as a salvage technique for lateral mass screw failure.
The data show that using the PMMA in a quick-mix technique to salvage lateral mass screws yields statistically higher pullout strength when compared with the control side (native lateral mass screws). We hypothesize that the quick-mix cement better fills the bony void of the cutout lateral mass with better interdigitation and therefore a stronger bone–cement interface. Although not directly evaluated in this study, the porosity of the lateral mass would likely affect the cement interdigitation and the strength of a revision or salvage screw. The quick-mix PMMA likely has a better permeability into the bony architecture of the lateral mass, thus creating a better bond. This effect may even be greater in osteoporotic specimens in which porous bony architecture will allow enhanced interdigitations. Further studies are needed to compare osteoporotic and nonosteoporotic cement lateral mass salvage.
The PMMA with the standard-mix technique yielded relatively high-viscosity cement and was more difficult to apply evenly throughout the cutout defects, which likely contributed to the lower pullout strength. The Cortoss mix had ideal working characteristics with reasonable viscosity and long working time allowing for ease of application and adequate filling of the bony defects in the lateral mass. Unfortunately, the Cortoss group was underpowered in our study, and no conclusions can be drawn from its data; however, grossly the Cortoss appeared loose at the bone–cement interface. We also waited much longer for the Cortoss to harden in our specimens, which may or may not be a problem in a clinical scenario. Although we made great attempts to warm the specimens in warm water baths prior to cement application, the specimens were closer to room temperature rather than normal body temperature. The Cortoss and PMMA cement may have different binding properties in vivo that we were not able to elucidate in this study.
Although no extravasation of the cement into the vertebral or neural foramen was witnessed during our study, it is known that PMMA expands as it hardens, increasing the risk for extravasation. It is the authors’ beliefs that this risk would be greatly increased if cement was placed with pressurization and thus should not be done. When considering the use of cement augmentation for salvage, the defect should be carefully probed. Any concern for violation of the vertebral or neural foramen should steer the physician to another salvage option. In our study, we modeled a typical lateral cutout of the lateral mass and therefore had little concern about a medial breach.
Limitations of this study include anatomic variabilities among the cadaveric specimens. We did our best to control for this by evaluating DXA scans, making sure all specimens were osteoporotic, and utilizing each specimen as its own internal control. Unfortunately, there still may be variances that were not controlled for such as porosity within a lateral mass. Although we did consider a synthetic or sawbones model to help standardize our controls, we felt that this synthetic model would yield faulty conclusions. The ability to salvage a cutout lateral mass has everything to do with cement augmentation and the strength of the bone–cement interface. Testing the strength of a synthetic–cement interface would not make sense as it likely has different bonding characteristics when compared with bone. Bone cement has previously been used to strengthen the bone–implant interface in the vertebral column. 32 , 33 , 34 , 35 Pitzen et al showed that a PMMA bone cement–screw interface with bicortical purchase provided a pullout strength and insertional torque that was greater than a bone–screw interface in the cervical spine in a cortically placed screw. 36 Although we did not use computed tomography to confirm that our screws were bicortical, our method attempted to simulate in vivo screw placement with a commonly utilized screw size and to test this in a lateral mass screw salvage model. This concern is partially addressed by using each specimen as its own internal control. The 14-mm screw length was chosen because it is a commonly used length and we wanted to mimic what would be encountered in a typical clinical scenario.
We were also not able to simulate in vivo temperature within the cadaveric specimens, which may alter time to setting and possibly bonding potential of the different cements utilized in this study. Another limitation of the study is that we were not able to standardize the amount of cement we placed in the lateral mass defects prior to salvaging with a revision screw. The amount of cement was determined by differences in cervical morphology, cutout sizes, and changes in defect after failure loading during primary augmentation testing. Finally, because this is a cadaveric study, active bleeding was not simulated and therefore in a real clinical case there might be further interference with the bonding potential of the cement.
In conclusion, this study shows that quick-mix PMMA revision of a lateral mass screw cutout provided a statistically higher pullout strength than the tradition lateral mass screw in osteoporotic vertebrae. Therefore, the quick-mix PMMA revision technique equips the spinal surgeon with another salvage option for lateral mass screw failure.
Disclosures
Michael A. Gallizzi, none
Craig A. Kuhns, Consultant: Stryker Spine
Tyler J. Jenkins, none
Ferris M. Pfeiffer, none
Footnotes
Notes
Cadaveric specimens and bone cement were purchased through departmental research funds. Stryker donated the lateral mass screws used for this study. No other outside external funding source was used to execute this study. Dr. Kuhns is a consultant for Stryker Spine but did not receive any payments related to this study.