
Abstract
Study Design
Narrative Review.
Objectives
To summarize the scientific contributions generated from the AO Spine Knowledge Forum Tumor (AOSKFT) databases, focusing on primary spine tumors, and highlight key findings, research trends, and future directions.
Methods
Data from the Primary Tumor Retrospective (PT-Retro) and Primary Tumor Research Outcome Network (PTRON) registries were analyzed. The nineteen studies included were peer-reviewed manuscripts focused on primary spine tumors, excluding abstracts, book chapters, systematic reviews, and metastatic studies.
Results
The PT-Retro registry compiled data from 1495 patients across 18 primary tumor histologies, offering insights into recurrence, survival, and treatment paradigms. Key findings emphasize the importance of Enneking-appropriate (EA) resection in improving survival and reducing recurrence in tumors such as chordoma, chondrosarcoma, and osteosarcoma. Genetic markers, including hTERT promoter mutations and rs2305089 SNP, were linked to prognosis in specific histologies. Benign tumors, such as giant cell tumors and aneurysmal bone cysts, demonstrated variable outcomes with different surgical approaches and selective arterial embolization.
Conclusions
The AOSKFT registries have significantly advanced knowledge in primary spine tumor management, emphasizing preoperative staging, surgical margins, and multidisciplinary approaches. International, multicentric registries are essential for studying rare diseases like primary spine tumors, enabling robust data collection, improved statistical power, and broader applicability of findings across diverse clinical settings. Ongoing prospective data collection through PTRON will further refine evidence-based care for these rare and challenging conditions.
Keywords
Introduction
The AO Foundation was started in 1958 with the intent to improve musculoskeletal health through research, education and surgical innovation. AO Spine is a specialty community within the AO Foundation to specifically address spine pathology and surgery. In 2011 AO Spine created 5 pathology-based Knowledge Forums, each populated with key opinion leaders charged with conducting cutting-edge multicenter research. The mandate for the AO Spine Knowledge Forum Tumor (AOSKFT) is unique because primary tumors of the spine are rare and both primary and metastatic spine disease require multidisciplinary input.
The rarity of primary spine tumors and heterogeneity of regional treatment practices has been a historical limitation of research efforts to improve best practices and patient outcomes. Based on review of the recommendations from the National Institutes of Health (NIH) for the study of orphan diseases, 1 the AOSKFT addressed these shortcomings with the creation of a comprehensive, international research network and registries. In 2012, the Primary Tumor Retrospective (PT-Retro) study was initiated (Clincaltrials.gov NCT01643174) to further understand the variables associated with local recurrence and overall survival for defined groups of benign and malignant spine tumor histologies. As a retrospective effort, PT-Retro provided an opportunity to collate data on a faster timeline than prospective study designs. Yet, given the advantages of prospective data, the Primary Tumor Research Outcome Network (PTRON, Clinicaltrials.gov NCT02790983) was created as a prospective repository for the clinical data associated with the myriad primary spine tumor histologies and their comprehensive treatment paradigms. The PTRON includes data from 16 institutions across the world. The ethical boards of both the AO Foundation and individual participating institutions provide oversight on data submission. As such, the participating institutions represent high-volume spine tumor centers of AOSKFT members.
Summary of Peer-Reviewed Scientific Articles Utilizing Data From AO Spine Knowledge Forum Tumor Primary Tumor Databases
Background of PT-Retro
Primary tumors of the spine and sacrum are rare pathologies and treatment involves substantial complexity across multiple specialties. The morbidity of aggressive treatment ranges widely and can sometimes outweigh the oncologic benefit depending on the frailty of the host and extent of the surgery. Therefore, a critical examination of clinical outcomes helps build consensus on treatment. With this in mind, the AOSKFT began a thoughtful, four-stage approach for this examination. The framework for data accumulation was guided by the National Institutes of Health recommendations and summarized by Fisher et al. 1
The development of PT-Retro began with a planning phase where data were canvassed from relatively large volume centers. There was agreement on terminology and creation of a data dictionary. Second, the centers with appropriate data were recruited and provided resources for data abstraction. The final phase involved data pooling, which yielded 1495 surgically-treated tumor cases across 18 different primary tumor histologies from 1981 to 2012 to form the PT-Retro database. The largest represented histology was chordoma (344 tumors, 23%) and the cohort mean age was 43 years ± 19 years with 5- and 10-year survival of 71.9% and 53.3%, respectively. 2
The granular clinical variables obtained through the global PT-Retro effort was a meaningful improvement over prior datasets based on administrative coding. Further, it established a network of relatively high-volume centers involving orthopedics and neurosurgeons, radiotherapists, medical oncologists and researchers, which provided a foundation for hypothesis generation and the fourth phase of AOSKFT effort towards primary tumor data—prospective collection. The AOSKFT provides funding for the ongoing PTRON data collection effort, which is structured through 6 modules: demographic, clinical, diagnostic, therapeutic, local recurrence/survival and perioperative morbidity.
Methods
The use of PT-Retro and PTRON data for analysis and manuscript preparation requires approval by the regulatory statutes of the AO Foundation. As such, all publications utilizing PT-Retro and PTRON data received prior approval and this approval process was queried to generate a list of publications to date for this narrative review (Table 1). Additionally, AOSKFT members were polled to confirm the included list was comprehensive, to their knowledge.
Summary Median Survival and Risk Factors for Malignant and Benign Spine Tumors
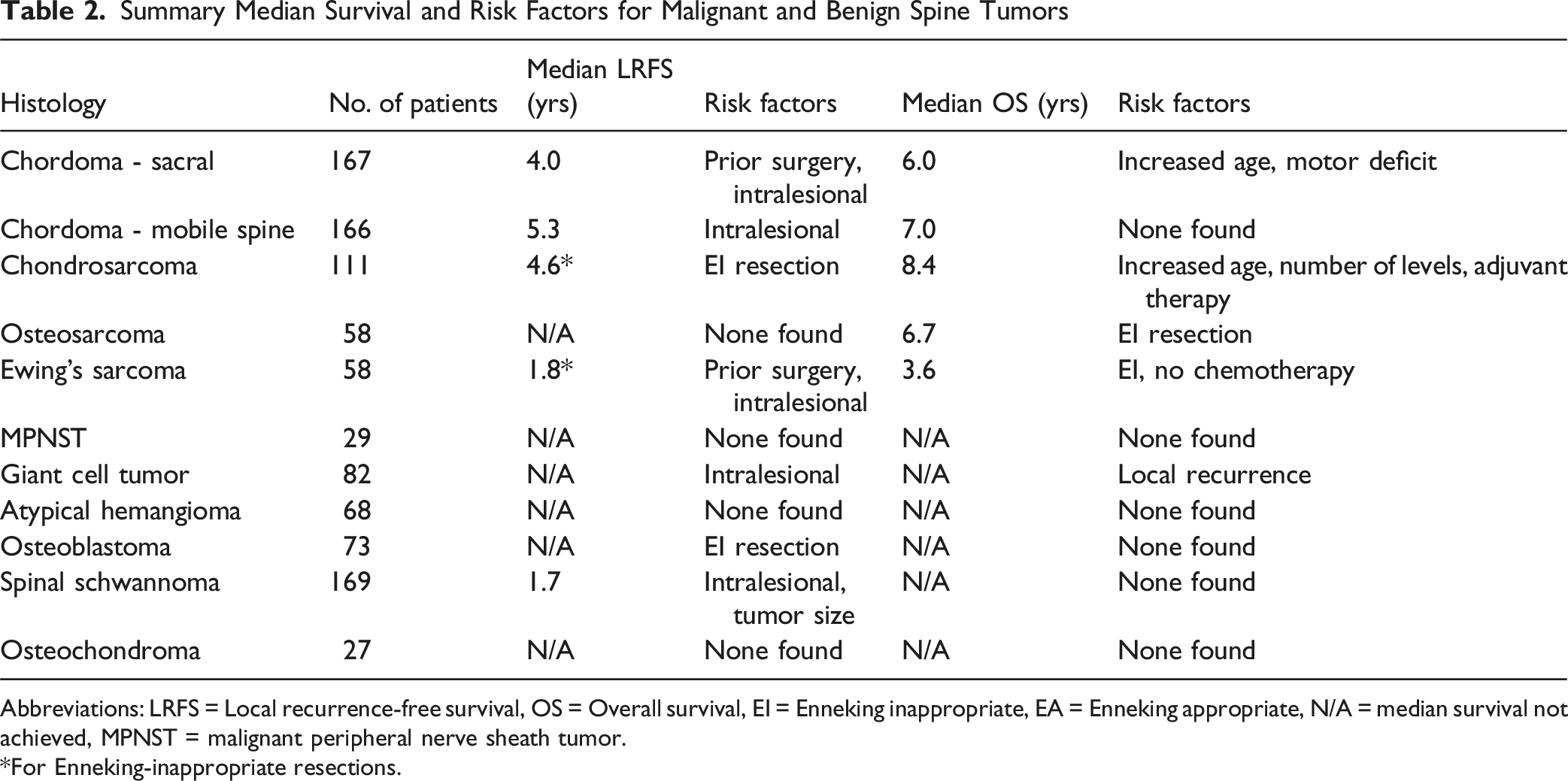
Abbreviations: LRFS = Local recurrence-free survival, OS = Overall survival, EI = Enneking inappropriate, EA = Enneking appropriate, N/A = median survival not achieved, MPNST = malignant peripheral nerve sheath tumor.
*For Enneking-inappropriate resections.
Malignant Primary Spine Tumors
Chordoma
Amongst the rare pathologies that arise from structures within the spine, chordoma is the most common malignant tumor of the spine (Figure 1A). The incidence is approximately 0.1 per 100 000 and most often arises in the sacrum followed by the skull base, lumbar, thoracic and cervical mobile spine segments.
22
For much of the modern era, the understanding of chordoma was informed by single-institution studies.23–26 These studies provide an invaluable longitudinal perspective to chordoma treatment from experienced surgeons and multi-disciplinary teams. However, these efforts are prone to expertise and institutional bias. Additionally, the availability of contemporary adjunctive treatments such as proton radiotherapy was siloed which raises generalizability concerns for other studies.
27
This point is underscored in a survey study of PT-Retro members for newly diagnosed chordoma of the spine and sacrum. Here, Dea et al demonstrated variability amongst those commonly treating chordoma with the majority (80%) foregoing neoadjuvant radiotherapy and heterogeneous approaches to radiotherapy administration in relation to surgical margins.
3
Representative imaging of malignant spine and sacral tumors. (A) MRI of a Chordoma of L1. The neoplastic mass is extracompartimental (Layers A to E, according to the Weinstein-Boriani-Biagini classification), compressing the spinal cord and extruding in the psoas muscle bilaterally. (B) Extracompartimental Chondrosarcoma involving the thoracic spine from T9 to L1, on the left side. The tumor mass has clearly a non-homogeneous matrix at the MRI, typical of Chondrosarcoma. (C) Osteosarcoma of C2 seen at a sagittal MRI image, T2-weighted, with an epidural extension (Layer E according to the Weinstein-Boriani-Biagini classification) causing a compression of the spinal cord. (D) Sagittal MRI of an Ewing Sarcoma originating from L1 and expanding in the canal. (E–F) Coronal (E) and axial (F) MRI views of a huge Malignant Peripheral Nerve Sheath Tumor arising in the lumbar region and extending from L2 to L5
The PT-Retro database was queried to understand factors associated with local recurrence and overall survival for sacral chordoma. In this worldwide cohort, the multivariable model identified prior surgery and intralesional resection associated with increased local recurrence whereas increasing age and a motor deficit was associated with worse overall survival. 4 A subsequent study by Gokaslan et al analyzed 166 patients with chordoma of the mobile spine. 5 The authors found a 35% local recurrence rate and a 34% mortality rate (follow-up ranged from less than 1 year to 22.5 years). Median survival was 7 years postoperatively, with a significant difference between Enneking-appropriate (EA, negative margin) and Enneking-inappropriate (EI, intralesional) surgeries (8.4 years vs 6.4 years, respectively). Intralesional excision was associated with an increased rate of local recurrence. This is considered in the context of feasibility for negative margin resection since 35% to 65% of sacral chordomas and around 80% of mobile spine chordomas are thought to be amenable to aggressive resection with negative margins. 6
Patient prognosis can also be linked to factors strictly related to the genetic features of chordoma. AOSKFT demonstrated how gene SNP rs2305089 and specific mutations of human telomerase reverse transcriptase promoter region can affect prognosis.7,8 Specifically, certain SNP edits are associated with overall survival of patients but not to their local recurrence-free survival. Genotypes GA and GG were associated with a significantly higher mortality when compared to genotype AA. Those patients with an A variant were found to have a statistically significant increase in survival (median overall survival of 7.6 years vs 3.8 years). Also, mutations of the telomerase reverse transcriptase (hTERT) were found in 8.7% of patients and are associated with improved prognosis. Independent from tumor histology, patients that display a hTERT promoter mutation were alive at 10 years postoperatively, compared to 67% of patients without the mutation.
Other Malignant Spine and Sacral Tumors
Chondrosarcoma is the second most common primary malignant spine tumor (Figure 1B). This disease was the subject of a 2016 PT-Retro publication by Fisher et al, that examined 111 patients that received surgery for the disease. 9 The authors observed a median survival of 8.4 years after surgery, with a mortality rate of 32% at 10 years post-operatively and a local recurrence rate of 35% over the study time period. Local recurrence was closely related to mortality as 62% of patients with a LR died, which underlines the importance of EA resection given its reductive effect LR rate. This led to a recommendation that en bloc resection of the tumor mass should be performed whenever feasible and reasonable from an expected morbidity standpoint.
The remaining malignant disease categories that were investigated by PT-Retro data are exceptionally rare. In osteosarcoma (Figure 1C), which is the most common primary malignant tumor of bone, only 3 to 5% of cases are localized to the spine. The low incidence of the disease has produced only small series and case reports, impacting the scientific knowledge on this disease.28,29 In a paper from 2015, Dekutoski and colleagues presented a series of 58 patients affected by osteosarcoma of the spine that were collected in the AOSKFT registries. 10 They observed a median survival of 6.7 years postoperatively with a mortality rate of 41%. A fundamental observation of this study is the association of EA resection with optimal oncologic outcomes. An EI surgery was associated with a significant reduction of life expectancy with median survival decreasing from 6.8 years (in EA surgeries) to 3.7 years (with EI resection). Additionally, this study did not find an association between age, previous surgery, tumor size or chemotherapy timing on local recurrence or survival.
Ewing Sarcoma (Figure 1D) of the spine has been analyzed in detail in a paper from Charest-Morin et al, in which the authors extracted the data of 55 patients. 11 They observed a significant benefit in terms of local recurrence and survival when comparing EA to EI surgeries. The results also confirm the role of preoperative neoadjuvant chemotherapy is strongly recommended in this set of patients.
Finally, evaluation of malignant peripheral nerve sheath tumor (Figure 1EandF) cases in the AOSKFT international multicenter database was provided by Chou and colleagues. 12 They grouped 29 patients with a median follow-up of 1.3 years (range 42 days to 11.2 years). These lesions showed aggressive behavior with 14 (48%) patients died and 14 (48%) patients suffered a local recurrence, 10 (71%) of whom died. Unlike other tumors analyzed in the PT-Retro database, margin status did not show a significant influence on local recurrence or survival. Further, adjuvant therapy modalities did not improve recurrence or survival. Given the aggressive behavior, the Authors still recommend considering the lesion as a sarcoma and favor en bloc resection when morbidity is acceptable for the patient.
The depth of the AOSKFT registries allowed an evaluation of malignant extradural spine tumors in a subpopulation younger than 25 years. 30 Disch et al found a prevalence of Ewing sarcoma, osteosarcoma and chondrosarcoma histologies, with a local recurrence rate of 36.4%. Over one-third of patients died in a 10-year follow-up. The study highlights the importance of a multidisciplinary evaluation of these patients and the centralization of these patients in high volume hospitals, as half of EI surgeries were obtained in patients that already received a previous operation. This challenging scenario is associated with a more complicated course even in successful revision surgeries.
Benign Primary Spine Tumors
Benign histologies are often prone to aggressive local recurrence that can lead to significant morbidity and, in some cases, mortality. This speaks to importance of research into these rare tumors despite their seemingly innocuous title.
Hemangioma (Figure 2A) is definitively the most commonly observed benign spine tumor, and rarely needs treatment. Surgical treatment is usually reserved for aggressive subtypes presenting with canal invasion or spinal instability and consequent risk of fracture. Goldstein et al reviewed 68 patients treated surgically with this aggressive subtype of hemangioma to better understand local recurrence and long-term outcomes.
13
They found epidural extension of the disease in 55% of cases, with local recurrence in only 2 cases (3%) in a long-term follow-up. One case recurred at 4.4 years after intralesional excision and postoperative radiotherapy, while the second recurred 5.3 years after intralesional resection without adjuvant RT. Based on the findings, the authors recommended a gross-total intralesional resection without the need of adjuvant radiotherapy. Representative imaging of benign primary spine tumors. (A) MRI showing a Hemangioma of T9, with a typical “salt and pepper” image of the vertebral body. (B) Axial MRI image of multiple Aneurysmal Bone Cysts that rose at T12, causing a cord compression in a 16 years-old male. (C) Axial MRI of a Giant Cell Tumor arising from the vertebral body of L5. (D) CT scan of a Osteoid Osteoma of the posterior laminate, with a huge sclerotic reaction surrounding the nidus of the tumor. (E) Axial MRI of an Osteoblastoma in the vertebral body in the lumbar region, with a partial erosion of the posterior vertebral wall. (F) MRI showing a Schwannoma of the cervical spine, with a huge extension in the paravertebral soft tissues on the right side, dislocating the neurovascular bundle
Aneurysmal Bone Cyst (ABC, Figure 2B) tumor is another relatively common benign tumor of the spine, as 10 to 30% of all ABCs are observed in the spine. It can be locally aggressive and eventually reach considerable size requiring extensive surgery. In the spine, intralesional resection has a recurrence rate up to 25%, while en bloc resection significantly reduces the recurrence rate but increases morbidity. Unfortunately, medical treatments for ABC are very limited, as denosumab is not recommended as a first-line treatment (weak recommendation, very low-quality evidence). 31 However, newer less-invasive techniques as stem cells instillation may help in the management of these lesions. In an AOSKFT paper Boriani et al compared selective arterial embolization (SAE) to surgical excision in ABC treatment without finding statistically significant difference in local recurrence and survival rates. 14 However, the authors found local recurrences only after intralesional Enneking inappropriate resections and demonstrated that SAEs alone could be effective in treating the tumor but required more than 5 procedures in over a third of patients. Local injection of bone marrow aspirate (BMA) or doxycycline are not recommended as a first-line treatment options.
Giant cell tumor (GCT, Figure 2C) is another primary benign tumor that can affect the spine. Given the high rate of local recurrence with intralesional surgery, en bloc resection is frequently recommended. This was demonstrated in a paper from Charest-Morin et al, in which en bloc resection with wide or marginal resection margins was related to a decreased rate of local recurrence in a review of 82 patients. 15 Denosumab is a medical treatment indicated for inoperable GCT (strong recommendation, very low quality evidence) or as a neoadjuvant therapy (strong recommendation, very low quality evidence), while the use of interferon alpha-2B or bisphosphonates is not supported (weak recommendation, very low quality evidence). On the other hand, SAE is recommended preoperatively in these hypervascular lesions (strong recommendation, very low quality evidence) of the mobile spine, while is not recommended for sacral lesions (weak recommendation, very low quality evidence). 31 The increasing role of Denosumab has however reduced the application of SAE as neoadjuvant therapy. Osteoid osteoma (OO, Figure 2D) has also been the subject of PT-Retro data analysis. Similar to other musculoskeletal sarcomas, OO is much more common in the appendicular skeleton. While thermal ablation is the primary treatment in the extremities, the risk of thermal injury to neural tissue limits universal application to the spine. It is recommended in selected OO spinal lesions with intact cortical bone and >5 mm from neural tissue (strong recommendation, very low quality evidence). 31 The PT-Retro database provided analysis of 81 mobile spine by Quraishi et al. 16 This paper demonstrates that complete resection of the nidus, whether en bloc or intralesional, is the most strongly associated variable in local recurrence. This is a clinically helpful finding as it can save the patient substantial morbidity of en bloc resection depending on the location of the lesion.
Osteoblastoma (OBL. Figure 2E) is the histologic cousin to OO and also reviewed in a study of PT-Retro data from 2017. Versteeg et al reviewed 102 patients with osteoblastoma treated surgically between 1991 and 2012. The authors report an 18% local recurrence rate and 8% mortality throughout the study period. 17 A strong correlation between local recurrence and patient mortality was demonstrated. However, no significant differences were found between the Enneking appropriate (EA) and inappropriate (EI) surgeries in terms of local recurrence and mortality. However, given the local aggressivenes shown in specific cases, en bloc or marginal resection is recommended when the morbidity is acceptable. This has been confirmed also in another AOSKFT paper from Disch et al. 23 The authors demonstrated a similar rate of recurrence between EA and EI surgeries with an increased disease-free-survival in the EA group, while in EI surgeries recurrences were observed after an average time lapse of 1-2 years. 30
A paper from Fehlings et al analyzed 169 patients affected from spinal schwannoma (Figure 2F) from the PT-retro database seeking to identify risk factors for local recurrence. 18 They found a 5.2% rate of local recurrence, with a higher rate in younger patients, cervical or sacral locations, and larger tumor dimensions. The cranial-caudal dimensions were associated to the greatest hazard and for every 1 cm increase in tumor size the recurrence hazard increased by 15.7%. Additionally, intralesional resection and an increased number of involved vertebral levels were also associated with recurrence.
The optimal treatment for spinal solitary plasmacytoma (SP, Figure 3A–C) continues to be sought after. Given the susceptibility to radiotherapy, that is often the first line treatment as it affords the patient the possibility of avoiding surgery. In a study of 39 patients with spinal SP, Ouyang et al investigated after radiotherapy the association of re-ossification on imaging with progression to multiple myeloma (MM).
19
The authors report those with re-ossification (defined as >30% increase in bone formation at 12 months) had a better prognosis with a much lower progression to MM. Sagittal MRI (T2 and T1 sequences) with standing lateral XR showing plasmacytoma at L3 with resultant pathologic fracture and severe, symptomatic spinal stenosis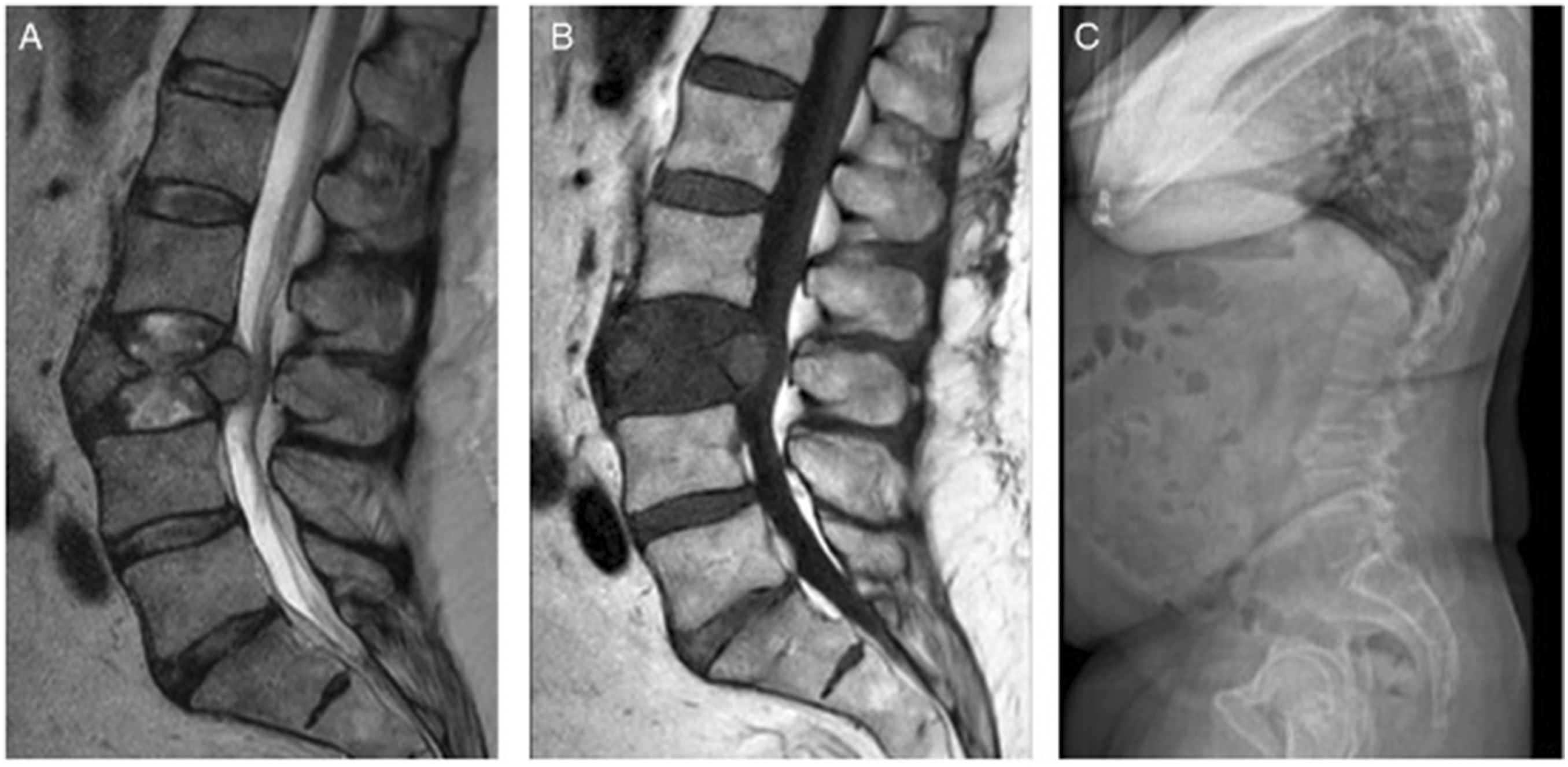
Finally, osteochondroma was evaluated in a 2015 paper by Sciubba et al using long-term follow-up of 27 patients in the PT-Retro database. 20 The authors reported malignant transformation in 12% of patients with an 8% rate of local recurrence after resection and no related deaths. Both the recurrences happened in Enneking latent Stage 1 tumors despite EA resections. This finding highlights the need to maintain adequate follow-up after resection.
Discussion
Registries are increasingly involved in healthcare, which improves the generalizability and quality of research. The value of data repositories is perhaps most realized in rare pathologies, such as primary spine tumors. The sum of local experiences can provide a wider set of data that answers questions that were previously unattainable. One important variable is follow-up, which can be optimized with a larger dataset to allow closer scrutiny of different treatment paradigms. The AOSpine Knowledge Forum Tumor established 2 large international registries--PT-Retro and the PTRON—the most comprehensive source of primary spine tumor data (Table 2) to date. Furthermore, the AOSKFT created a research network of spine tumor centers and key multi-disciplinary opinion leaders dedicated to improving the care of these challenging patients. The network integrated with the registry is an important distinction and represents something beyond a generic registry. The sharing of experiences, collaborative generation of research questions and the ability to take advantage of centers already linked with common data fields to do prospective studies is invaluable.
This current review of scientific output from AOSKFT registries offers a summary of the main findings regarding primary spine tumors. Three trends that emerge from this analysis are: the importance of preoperative staging, the value of surgical margins and the relevance of adjuvant therapies. Application of Enneking concepts and staging system is an effective way to improve survival and reduce local recurrence in spine tumors. For this reason, a proper preoperative staging of the patient’s oncological status is mandatory. This provides an accurate oncologic understanding of the patient and informs preoperative decision regarding the most appropriate type of resection. This has been further demonstrated by PT-Retro and PTRON based studies, where Enneking appropriateness or inappropriateness of surgical procedure significantly affects survival in patients affected by chordomas of the spine (8.4 years in EA vs 6.4 years in EI surgeries). This was further observed in chondrosarcoma, where local recurrence is closely related to mortality, and in osteosarcomas (6.8 years in EA vs 3.7 years in EI). The value of Enneking classification is evident also in benign tumors, where intralesional surgeries and gross total resections demonstrated less effective control.
On the other hand, when radical surgeries are planned, the margins of our resection are pivotal in determining the risk of local recurrences and consequently the overall survival. It has been demonstrated also in PT-Retro and PTRON patients how intralesional excisions increase the risk of local recurrences in chordomas, chondrosarcomas, osteosarcomas and Ewing sarcomas. Although some histologies (osteoblastoma and MPNST) did not demonstrate an association between resection type and local recurrence, the oncologic principles obtained from other histologies lead us to recommend en bloc resection if feasible. Since local recurrence is closely related to overall survival, it follows to set local control as the primary goal of a surgical resection. The spine creates unique considerations in this endeavor due to sensitive neurologic and vascular structures in proximity, coupled with the foundational support to physical function conferred by the vertebral column. En bloc resection is technically challenging and often includes sacrifice of relevant neurologic structures or inadvertent damage to them. A meticulous preoperative plan is fundamental in these cases, but does not guarantee a negative margin resection in every surgery. Tumor location and morphology are 2 factors that can influence the feasibility of an en bloc resection. A tumor with circumferential cord involvement would require cordotomy, which is rarely considered in spine oncology treatment plans. The advent of contemporary systemic therapy and radiotherapies may provide hope to patients who choose to undergo a carefully planned intralesional resection, or to those who had an unplanned positive margin of the resected specimen.
The retrospective analysis of 300 patients in the PT-Retro database reviewed attainment of planned margins in 74.7% of patients. 21 None of the variables included in this analysis demonstrated a statistically significant association with successful achievement of surgical margins. However, tumor size, previous radiation therapy and number of involved vertebrae trended towards significance while fewer involved vertebrae have been shown to be significantly associated with intraoperative surgeon perception of margins achieved. In this study, the authors suggest that higher statistical power would likely move some of these variables into statistically significant associations. This highlights the need for an ongoing meticulous international data collection in order to continually improve the quality of data for this complex patient population. The results also underscore the recommendation for treatment in high-volume centers with experienced staff.
We recognize limitations to the data and results of these studies, which include selection, indication and expertise bias inherent to the nature of retrospective data that exist in PT-Retro. Further, while the outcome measures generally align, they are not standardized across histologies, which makes interpretation less seamless. Finally, this manuscript does not represent a systematic review on primary spine tumors and databases outside of the AO Spine networks were not queried.
Future Work and Conclusions
Recent innovations in spinal oncology have transformed the diagnosis and treatment of spinal tumors, enhancing precision, reducing invasiveness, and improving patient outcomes. Targeted therapies, stereotactic radiosurgery, and robotic-assisted surgery, are shaping a new era in spinal oncology, offering more precise and personalized treatment strategies.
Among these advancements, liquid biopsies have emerged as a powerful tool for real-time, non-invasive tumor monitoring. By detecting circulating tumor DNA (ctDNA) and other biomarkers, liquid biopsies enable early diagnosis, assessment of treatment response, and detection of minimal residual disease, reducing the need for repeated surgical biopsies and potentially increasing early detection of recurrences or metastases. 32 Another significant improvement is the use of carbon fiber-based implants and surgical instruments. Unlike traditional metal implants, carbon fiber materials are radiolucent, minimizing imaging artifacts and improving visualization in postoperative monitoring and radiation therapy planning. 33 All these advancements will hopefully lead to improvements in quality of life and a longer life expectancy for our patients. Furthermore, advancements in genetic and immunotherapy approaches, such as tumor-specific gene targeting and immune checkpoint inhibitors, are opening new avenues for personalized treatments, improving survival rates in selected spinal tumor patients. These advancements must, however, be based on scientific evidence and international registries are a central component to that effort.
In summary, the PT-Retro study provided significant data for the spine oncology community over a relatively short time period of 10 years (Table 1). The use of multi-institutional data substantially increased the generalizability of results and increased the statistical power to investigate diseases that, in some cases, only had limited and institution-specific case series for pre-existing clinical recommendations. The advantages of prospective research will be realized in PTRON studies. These rare diseases need a continued multi-institutional collaborative effort and we are hopeful the experienced research relationships amongst AOSKFT will provide even more impactful research in the coming years.
Footnotes
Acknowledgements
This study was organized by AO Spine through the AO Spine Knowledge Forum Tumor, a focused group of international spine tumor experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.