
Abstract
Study Design:
Retrospective case series.
Objective:
To determine predictive factors of overall survival (OS) and local recurrence (LR), report complications, and assess the impact of complications on survival, recurrence, and function in patients undergoing en bloc resection of sacral chordoma.
Methods:
This retrospective case series was obtained from a prospective database (1995-2016). All patients underwent en bloc resection of sacral chordoma. Demographic, perioperative, and complication data were collected. Outcomes included: overall survival(OS), local recurrence(LR), and complications. Survival analysis with multivariable cox regression was performed.
Results:
Among 50 patients, median follow-up was 5.3 years (range = 1.3-17.2). The majority (82%) underwent a negative margin resection.
Conclusions:
Negative margin resection was associated with decreased LR. Neither major complication nor reoperation significantly impacted OS, LR, or functional outcome. Though additional studies are needed, it appears that despite the morbidity associated with sacral chordoma resection, the long-term clinical outcomes are favorable.
Keywords
Introduction
Chordomas are primary bone tumors that arise from remnants of the embryonic notochord and are found along the axial skeleton, most commonly in the sacrococcygeal region. 1,2 The incidence of chordoma is approximately 1 per 1,000,000. 3,4 Sacral chordomas have limited response to radiation and chemotherapy, and surgical resection has been the preferred treatment. En bloc resection has been shown to decrease local recurrence rates. 1,5 -7 Chordomas grow slowly and are often diagnosed at large sizes making en bloc resection challenging. 8 Moreover, the complex anatomy of the sacropelvic region and juxtaposition of vital neural, vascular, and visceral structures imbues these procedures with significant potential morbidity.
Though prior studies have reported predictive factors of overall survival (OS) and local recurrence (LR), large series of patients undergoing en bloc resection of sacral chordomas are rare. 5,6,9 -24 Previously described predictive factors of OS and LR have included high sacral location, age, extent of tumor invasion, and previous intralesional surgery. 10,11,14,17,25 Few studies have focused on the perioperative morbidity associated with these procedures, 13 and several do not report complication rates at all. 12,15 Commonly reported complications include wound dehiscence and/or wound infections, 15,16 sacral fractures, 9 and perioperative mortality. 11 The impact of perioperative morbidity on OS and LR is unknown. 13
In a group of patients undergoing en bloc resection of sacral chordomas, the current study aimed to: 1) determine predictive factors of overall survival (OS) and local recurrence (LR), 2) report perioperative complications, and 3) assess the impact of complications on OS, LR, and functional outcomes.
Methods
Study Design
The current single-institution, retrospective case series was obtained from a prospectively maintained database between January 1995 and June 2016. This ambispective design with cross-sectional follow-up has been utilized in similar reports. 15 Patients who underwent en bloc surgical resection of a pathologically confirmed sacral chordoma were included. Patients with a chordoma of the mobile-spine, evidence of metastatic disease, or non-chordoma sacral tumors were excluded. All patients had a minimum of one-year follow-up. The study was approved by the institutional review board, and the manuscript adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 26
Data Collection
Preoperative demographic and disease specific data points were obtained. Chordoma staging was performed according to the Enneking surgical staging system. 27
Intraoperative and tumor specific variables were collected, including operative time, estimated blood loss (EBL), fixation, and length of stay (LOS). In the setting of staged operations, total EBL and total operative time were summed. Though often confused, the term en bloc resection refers to the surgeon’s preoperative strategy to take out the tumor in 1 piece without tumor capsule violation. Postoperatively, tumor resections are evaluated pathologically with 1 of 3 terms: wide (tumor capsule not violated with layer of surrounding tissue intact), marginal (tumor capsule not violated with no surrounding tissue), or intralesional (tumor capsule violated). In keeping with prior studies, tumor resection was classified as either Enneking appropriate (EA), defined as a wide or marginal resection with the tumor capsule intact, or Enneking inappropriate (EI), defined as an intralesional resection with tumor capsule violated. 15,27 The term gross total resection means the tumor was taken out in its entirety but does not comment on tumor caspule violation, and thus was not used in our study. Resection margins were independently assessed by a fellowship trained pathologist. Level of nerve root sacrifice was noted, and in the case of unilateral sacrifice, the most caudal level with bilateral preserved nerve roots was reported.
All patients followed up on a regularly scheduled basis. Magnetic resonance imaging (MRI) scans were obtained postoperatively at 3 months, 6 months, 1 year, and yearly, thereafter. Pre—or post-surgical chemotherapy and/or radiation were classified as adjuvant therapy. Pre and postoperative functional outcomes were defined in 2 ways: motor (using Frankel grade) and bowel/bladder function. Motor and bowel/bladder function were also dichotomized into normal versus abnormal function, and expected or unexpected, in keeping with the method described by Biagini et al 28,29 If the S1 nerve roots were sacrificed, both motor and bowel/bladder deficits were expected. If the S1 or S2 nerve roots were intact, no motor deficits were expected, only loss of bowel/bladder function. If the S3 nerve roots were the lowest preserved roots, no motor or bowel/bladder deficits were expected.
To fully assess the magnitude of each complication, a major and minor complication classification system was used. 30 Complications were recorded as early (within 6 weeks) or delayed (6 weeks or after). 15 Reoperation was defined as surgical intervention due to a complication from the index surgery and similarly classified as early or delayed based on the same time criteria. Wound-related complications were considered major only if they required reoperation. Neuropathic pain was considered major only if a pain-related surgery was pursued.
Operative Approach
While the operative technique of sacral chordoma resection has been described elsewhere 31 and is beyond the scope of this paper, the nuances of our multi-team approach warrant further discussion. For medium sized tumors involving S2 and below, a single-stage, posterior-only approach is typically utilized. Along with the lead spine team, a colorectal surgeon assists with mobilization of the rectum away from the presacral portion of the tumor, known as the Kraske approach. 32 The lateral musculoligamentous structures including the gluteus and piriformis muscles, as well as the sacrotuberous and sacrospinous ligmaments are divided to free the soft tissue attachments to the sacrum. The bony amputation is then completed at the appropriate level, sparing the most caudal uninvolved nerve roots. The plastic surgery team then closes with a gluteal advancement flap.
For larger tumors involving S1 and above, a two-stage approach is used. The first stage is anterior, with sacrifice of the internal iliac vessels by our vascular surgeons. This is crucial to avoid catastrophic bleeding during the second posterior stage. After vessel sacrifice, the spine surgeon can make anterior sacral cuts, as indicated, at the superior and lateral aspects of the tumor. Care is taken to avoid injury to the lumbosacral trunks running along the anterior sacrum. Lastly, the plastic surgery team will harvest a vascularized rectus abdominus myocutaneous (VRAM) flap, procured anteriorly and kept deep in the pelvis for the second stage. 33 The second stage is similar to the posterior only approach, and involves a multi-surgeon team carefully removing the tumor to avoid capsule violation, and the VRAM flap is pulled posteriorly from the pelvis to close the large soft tissue defect. All 2 stage resections require lumbo-pelvic reconstruction.
Statistical Analysis
Descriptive statistical analysis was performed. Medians, interquartile ranges (IQR), and ranges were calculated for continuous variables. A survival analysis was completed according to the method described by Kaplan and Meier. 34 OS was defined as the time from index operation to death. LR was defined as time from index operation to radiographic recurrence. Observations were censored when patients were alive or tumor free. Log-rank tests followed by univariate and multivariable cox regression analyzes were completed to assess for predictors and the impact of major complication and reoperation on OS and LR. Logistic regression was used to assess for predictors of reoperation and the impact of major complication and reoperation on functional outcomes, controlling for age. Known covariates that have been shown to affect OS and LR in sacral chordomas were controlled for, including age and motor function for OS and previous surgery and intralesional resection for LR. 15 In all models, any univariate P-value of <0.20 was placed in the multivariable model. Odds ratios (ORs) for logistic regression and hazard ratios (HRs) for cox regression with 95% confidence intervals (CIs) not containing 1.0 and P-value of <0.05 were considered statistically significant. All statistical analysis was performed in STATA version 14 (College Station, TX: StataCorp LP).
Results
Demographics & Perioperative Variables
Over half of the cohort was male (58%) with a median age of 60 years. Median follow-up was 5.3 years (1.3-17.2). The majority of patients (82%) underwent an EA resection. Full demographic, perioperative, and functional outcomes data are described in Table 1.
Preoperative and Perioperative Variables; Functional Motor and Bowel/Bladder Outcomes; Complication and Long-Term Follow-Up.
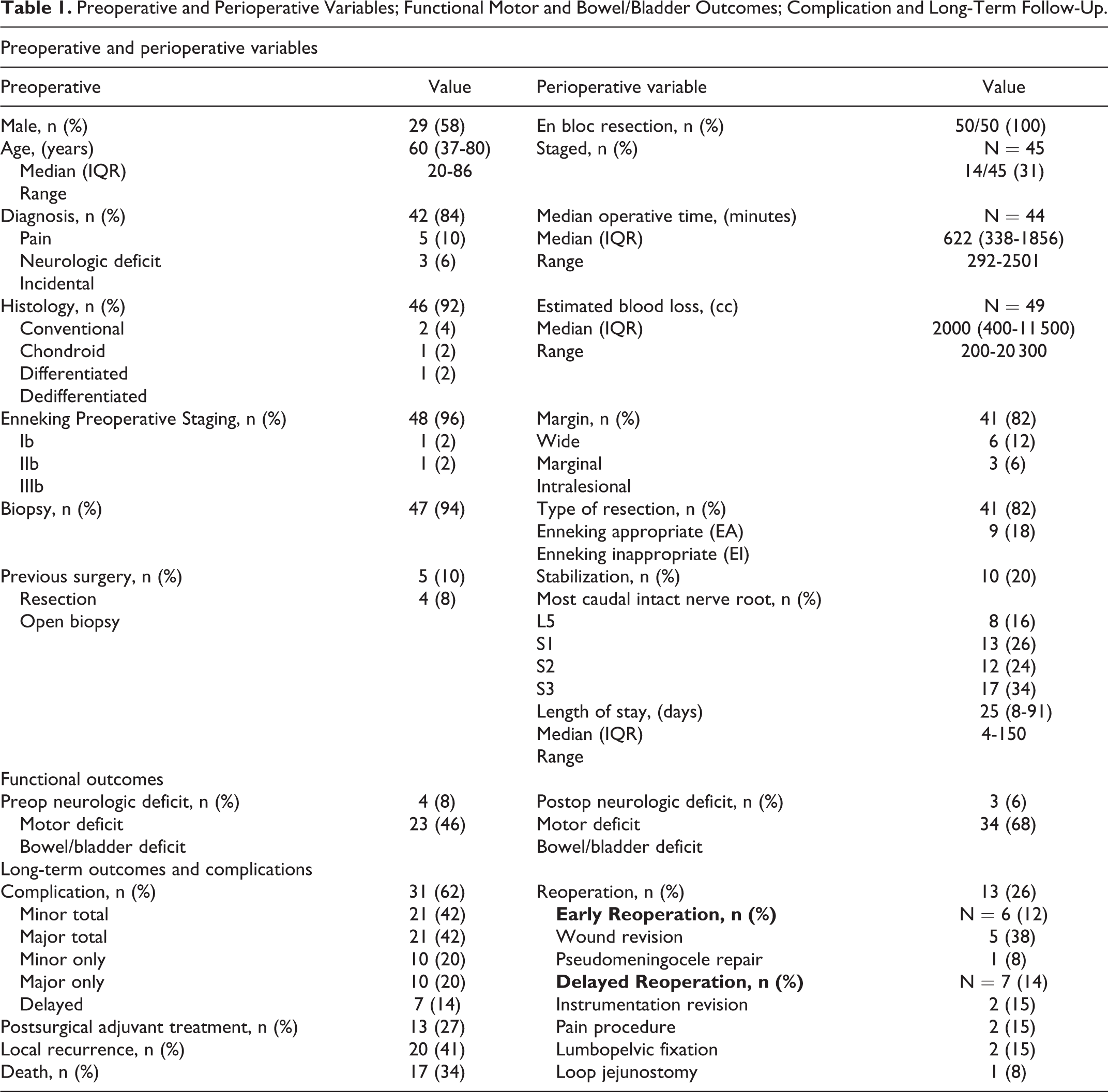
In terms of functional outcomes, the number of patients with motor deficits decreased from 8% preoperatively to 6% postoperatively. Though 8 patients (16%) were expected to have motor deficit given S1 nerve root sacrifice, only 3 patients (6%) had persistent motor deficits at last follow-up. With intensive physical therapy and rehabilitation, the remaining 5 patients regained plantar flexion and were able to ambulate independently.
Similarly, many patients had pre-existing bowel/bladder dysfunction, which increased postoperatively (46% to 68%). Though 33 patients (66%) were expected to have bowel/bladder dysfunction given S3 nerve root sacrifice, this number was 34 (68%). Of the 34 patients with post-op bowel/bladder dysfunction, new, unexpected bowel/bladder dysfunction occurred in 1 patient (2%). Despite intact S3 nerve roots, this patient harbored a large, low-lying pelvic tumor, and distal injury to the pudendal nerves was likely responsible for the unexpected, persistent bowel/bladder deficits. Despite the aim of surgery to be curative, 17 patients (34%) unfortunately succumbed to their disease at the time of census.
Overall Survival and Local Recurrence
Median OS was 10.0 years (range 1.3-17.2). For OS, log-rank testing revealed a significant association between EA resection and OS (P = 0.016) (Figure 1A). Although no variables were significant on multivariable analysis, type of resection approached statistical significance, where EI resection (intralesional margin) was associated with an increased risk of death (HR = 3.35, 95%CI 0.87, 12.80, P = 0.078).
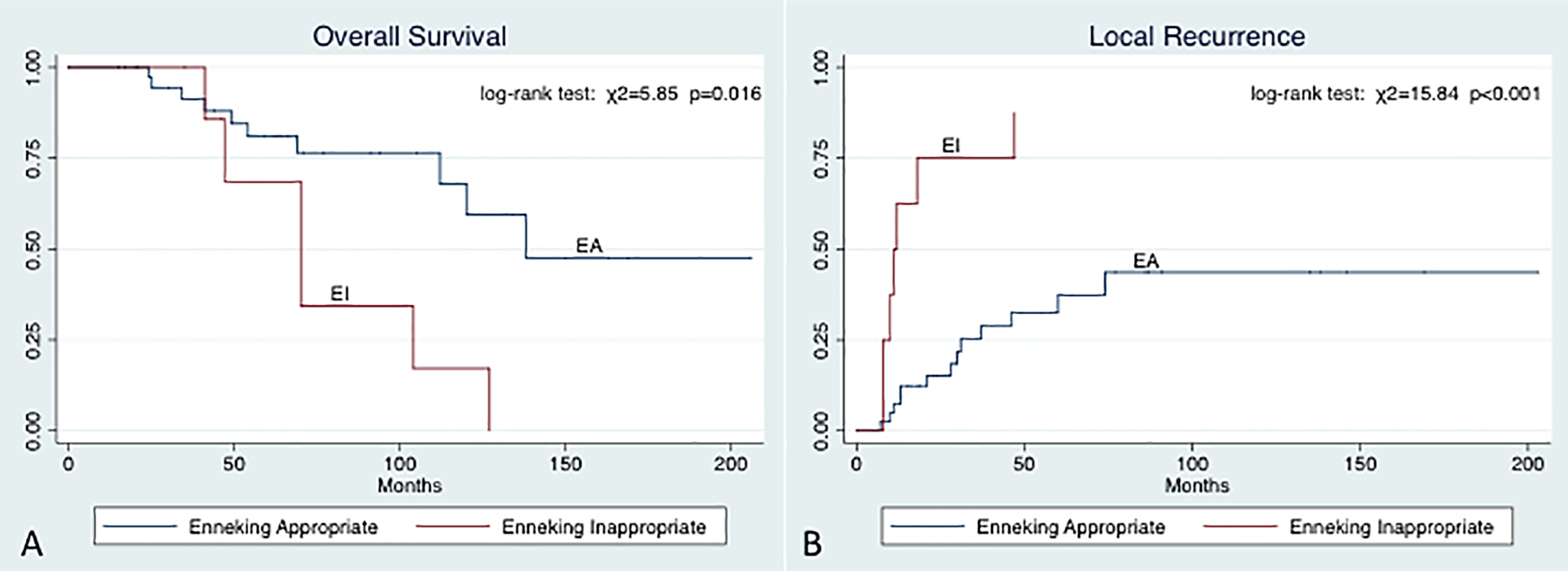
(A) Type of resection versus OS; (B) Type of resection versus LR.
Median time to LR was 6.2 years (range 0-16.9). For LR, log-rank testing also revealed a significant association between EA resection and LR (P < 0.001) (Figure 1B). On multivariable analysis, only type of resection remained significant (HR = 4.96 95%CI 1.84, 13.34, P = 0.002), where EI resection (intralesional margin) was associated with an increased risk of LR. Univariate and multivariable models of prognostic factors are summarized Table 2.
Predictors of OS and LR.
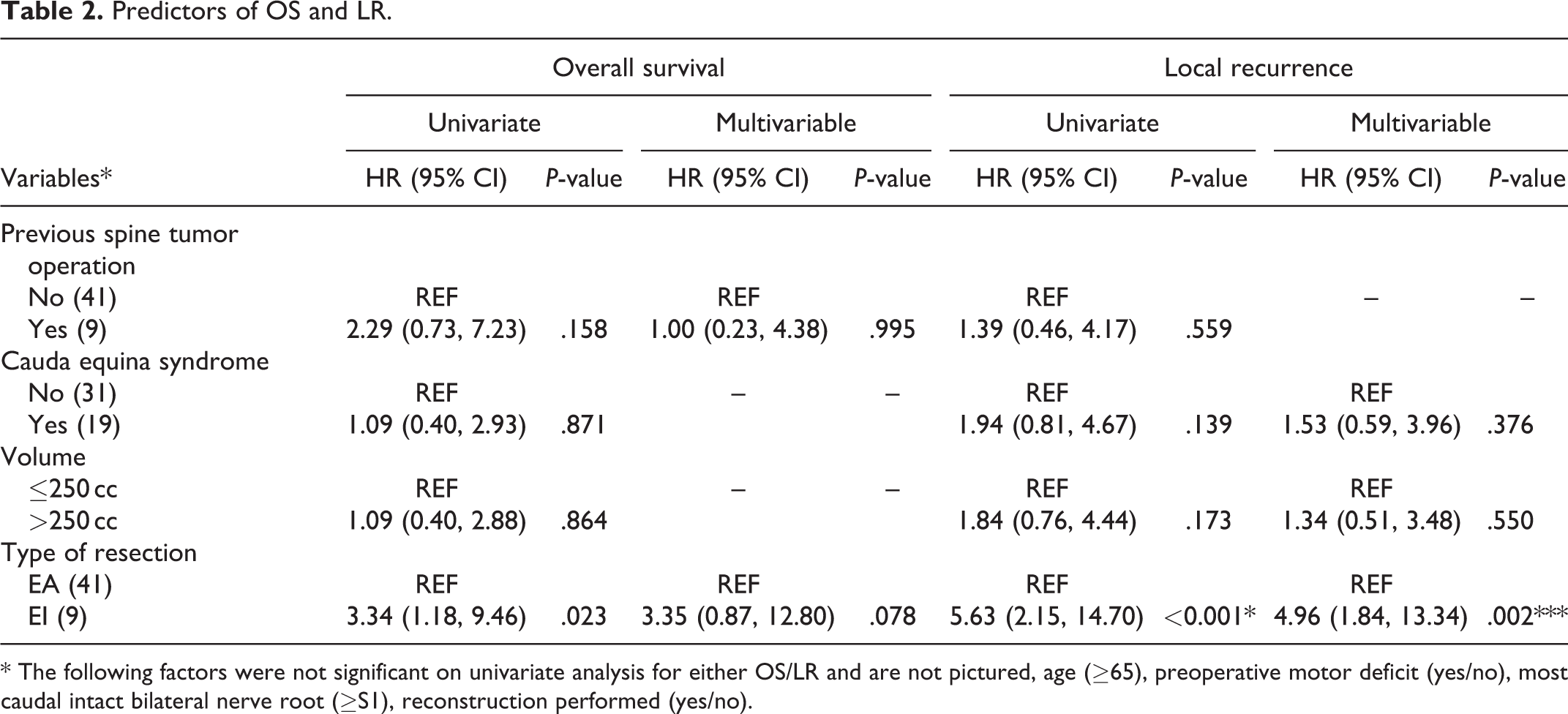
* The following factors were not significant on univariate analysis for either OS/LR and are not pictured, age (≥65), preoperative motor deficit (yes/no), most caudal intact bilateral nerve root (≥S1), reconstruction performed (yes/no).
Complications
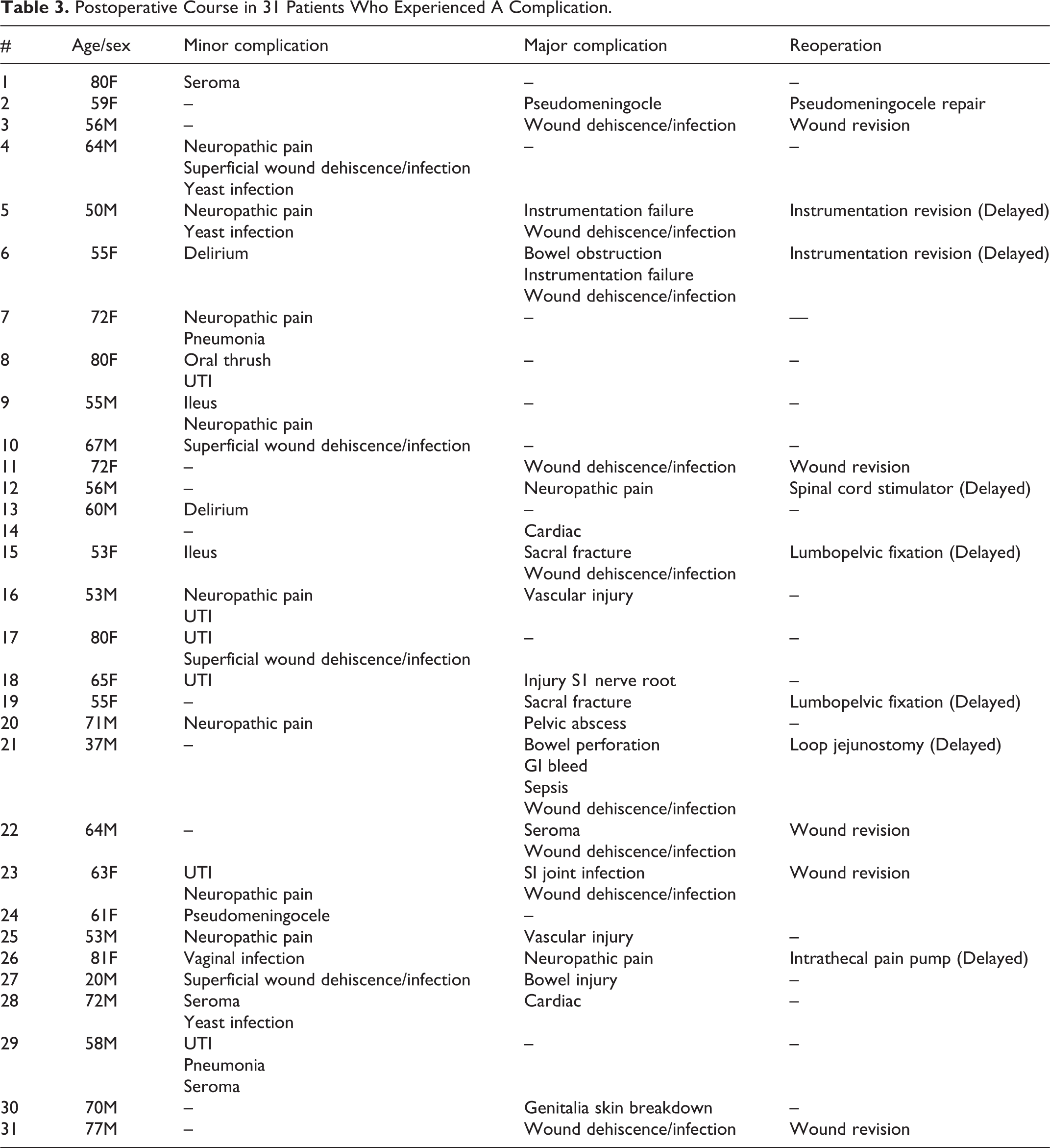
All types of complications—major, minor, early, delayed—were included in the final analysis (Table 1). An overall complication rate of 62% was observed in 31 patients, and 21 patients (42%) experienced a major complication. Thirteen patients (26%) required reoperation related to the index surgery, 7 of which (14%) were delayed reoperation (>6 weeks post operatively). All 7 delayed complications required reoperation: instrumentation revision (2), lumbopelvic fixation after sacral insufficiency fracture (2), pain procedures (2), and loop jejunostomy for a bowel perforation (1). Sixteen patients (32%) experienced wound dehiscence/infection or seroma at the surgical site, 5 of which required reoperation. Two patients (4%) experienced a symptomatic pseudomeningocele, 1 of which required surgical repair. Ten patients (20%) experienced neuropathic pain postoperatively, and 2 patients required a spinal cord stimulator and intrathecal pain pump, respectively. Neuropathic pain was primarily managed with medications. Nine patients (18%) experienced yeast infections or urinary tract infections (UTIs). All complications are itemized in Table 3. There were no mortalities.
Postoperative Course in 31 Patients Who Experienced A Complication.
Several a-priori factors were chosen to assess their association with a complication requiring reoperation on univariate and multivariable analyzes (Table 4). Three variables achieved a P-value of <0.20 and were included in a multivariable analysis, yet none achieved statistical significance. The same analysis was done to test an association with any general complication and no significant predictors were found.
Predictors of Complication Requiring Reoperation.
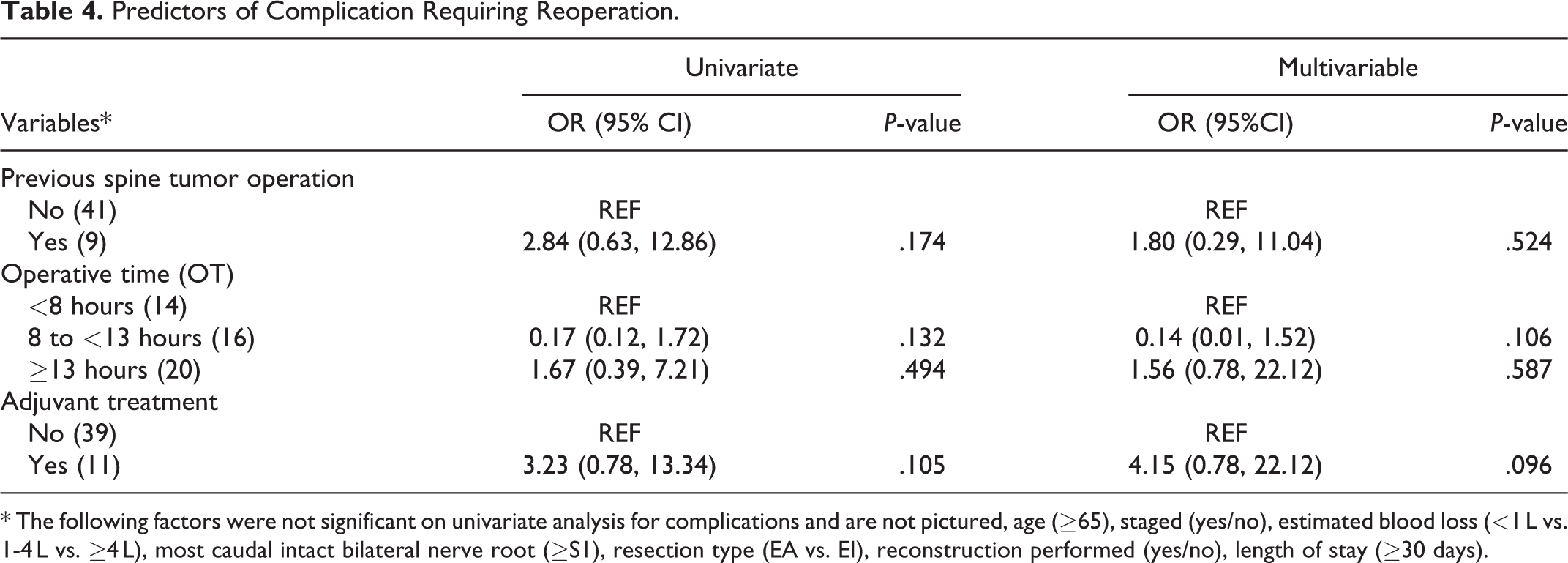
* The following factors were not significant on univariate analysis for complications and are not pictured, age (≥65), staged (yes/no), estimated blood loss (<1 L vs. 1-4 L vs. ≥4 L), most caudal intact bilateral nerve root (≥S1), resection type (EA vs. EI), reconstruction performed (yes/no), length of stay (≥30 days).
Impact of Complications on Survival, Recurrence, and Function
No significant difference was found in OS between those who experienced a major complication (P = 0.795) or reoperation (P = 0.647) compared to those without on log-rank testing (Figure 2A-B). Controlling for age and motor function, 15 no significant effect was found of major complication (HR 0.62, 95%CI 0.22-1.79, P = 0.380) or reoperation on OS (HR 0.51, 95%CI 0.16-1.63, P = 0.253).
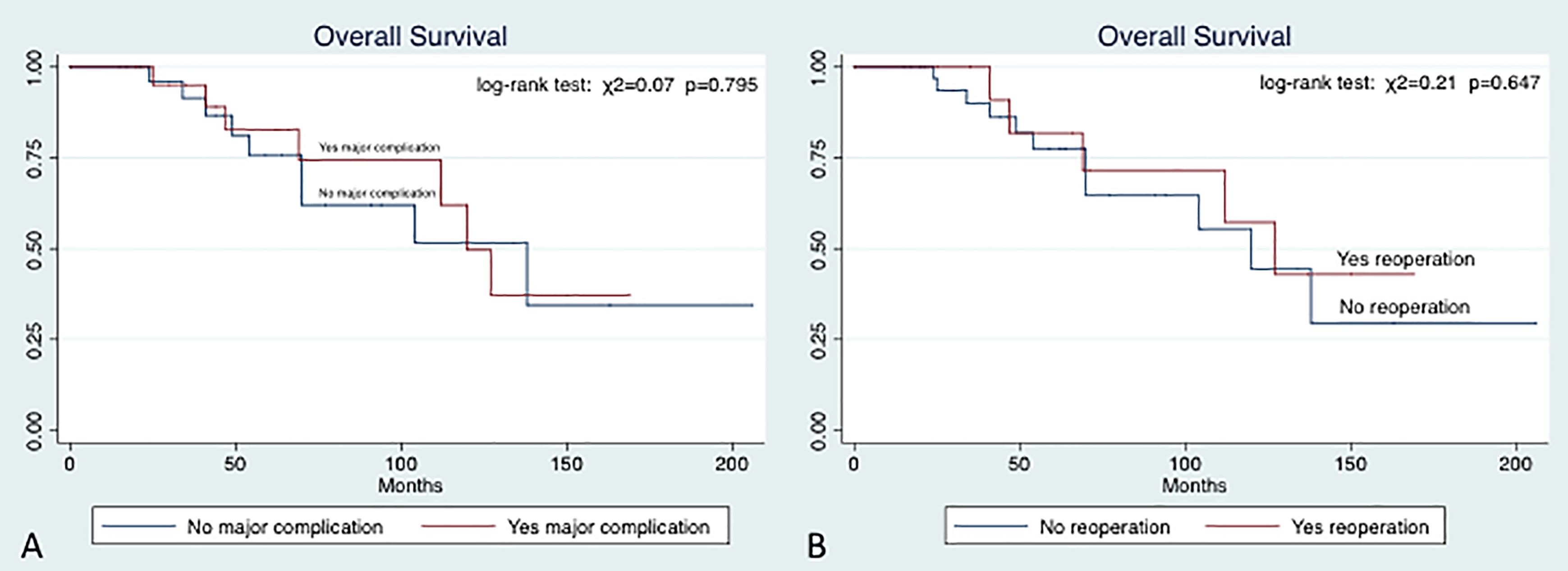
(A) Impact of major complication on OS; (B) impact of reoperation on OS.
For LR, there was no difference among those who experienced a major complication (P = 0.537) or reoperation (P = 0.632) compared to those without on log-rank testing (Figure 3A-B). Controlling for previous surgery and intralesional resection, 15 no significant difference was found of major complication (HR 1.28, 95%CI 0.49-3.36, P = 0.611) or reoperation (HR 0.55, 95%CI 0.17-1.79, P = 0.320) on LR.
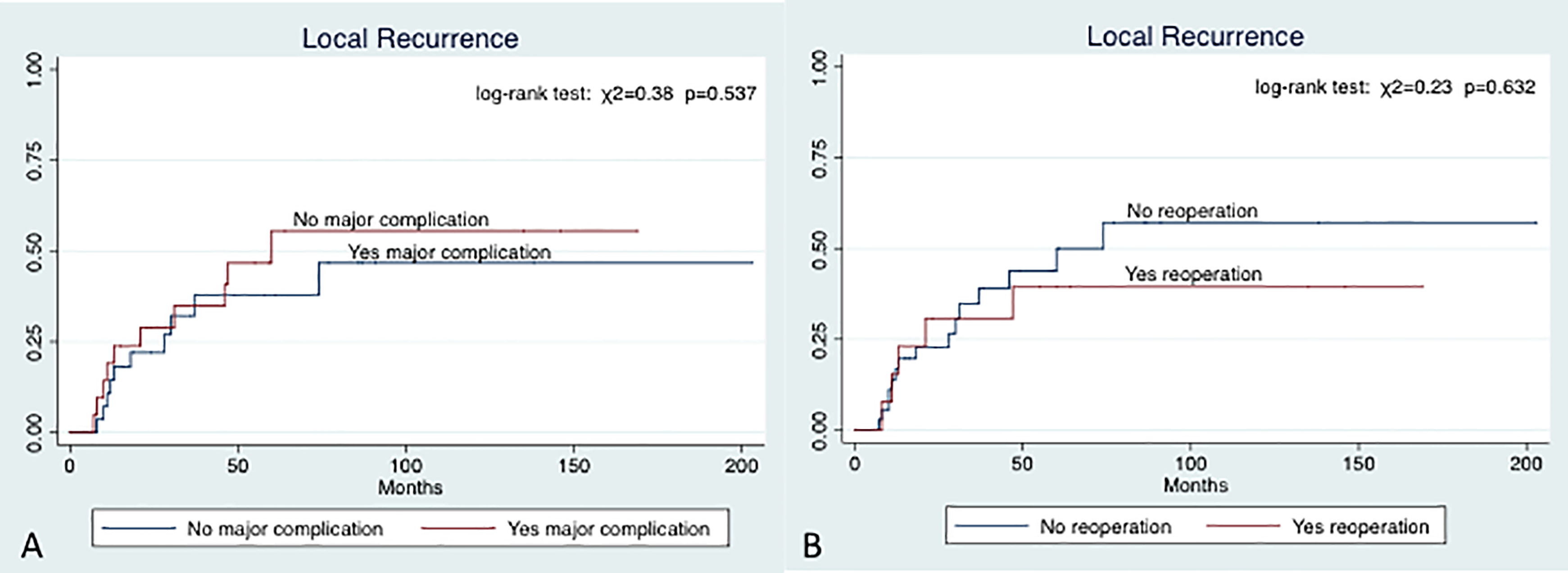
(A) Impact of major complication on LR; (B) impact of reoperation on LR.
In terms of functional outcomes, we found no significant difference in motor function in those who experienced a major complication (OR 2.94, 95%CI 0.25, 34.8, P = 0.393) or those who required reoperation. There were no patients with motor deficits who required reoperation. In comparing those who experienced a postoperative bowel/bladder deficit, we found no significant difference in those who experienced a major complication (OR 0.62, 95%CI 0.19, 2.05, P = 0.430) or required revision surgery (OR 1.81, 95%CI 0.42, 7.75, P = 0.426).
Discussion
En bloc resection of sacral chordoma is a technically demanding operation with potential for long term benefit but high morbidity. Many single and multi-institution studies have reported predictors of OS and LR 5,6,9 -24 ; however, complication data and their effect on survival, recurrence, and functional outcome are rarely included. In the present series, a negative margin resection was associated with a significantly decreased risk of LR but did not maintain significance for OS. Sixty-two percent of patients experienced a complication and 26% required reoperation. However, neither major complication nor reoperation significantly impacted OS, LR, or functional outcome. Thus, in this single-institution series from a major cancer center with long-term follow-up, it appears that the inherently high surgical morbidity associated with these operations does not significantly alter the benefit of en bloc resection with respect to survival, recurrence, and functional outcome.
In 1 of the largest studies to date of 167 patients with surgically treated sacral chordomas, Varga et al 15 found that age and impaired motor function predicted OS, and previous tumor surgery and type of surgical resection predicted LR. 15 The type of resection (EA vs. EI) was not significantly associated with OS, but this may have been due to short mean follow-up of 3.2 years. Their results are similar to our analysis, in that the margin of resection trended toward a significant impact on OS yet was found to significantly influence LR. As earlier studies have confirmed, we believe that LR is more easily impacted than OS because surgery has the greatest ability to affect tumor recurrence locally, at the site where the operation was performed. However, OS is a much harder variable to impact because many factors have an impact on one’s lifespan, such as age, comorbidities, overall health state, other cancers, and metastatic spread of the chordoma itself. Despite fewer patients, our median and average follow-up was longer at 5.3 years and 5.8 years, respectively. Other prognostic factors reported in large series include high sacral localization, 17 age, 10,14 and extent of tumor invasion 14 for OS, and age, 10,17 lack of radiotherapy, 19 and previous intralesional surgery 25 for LR. In our series, while previous operation for OS and functional deficits and tumor size for LR were significant after univariate cox regression analysis, none of these factors maintained significance on multivariable testing.
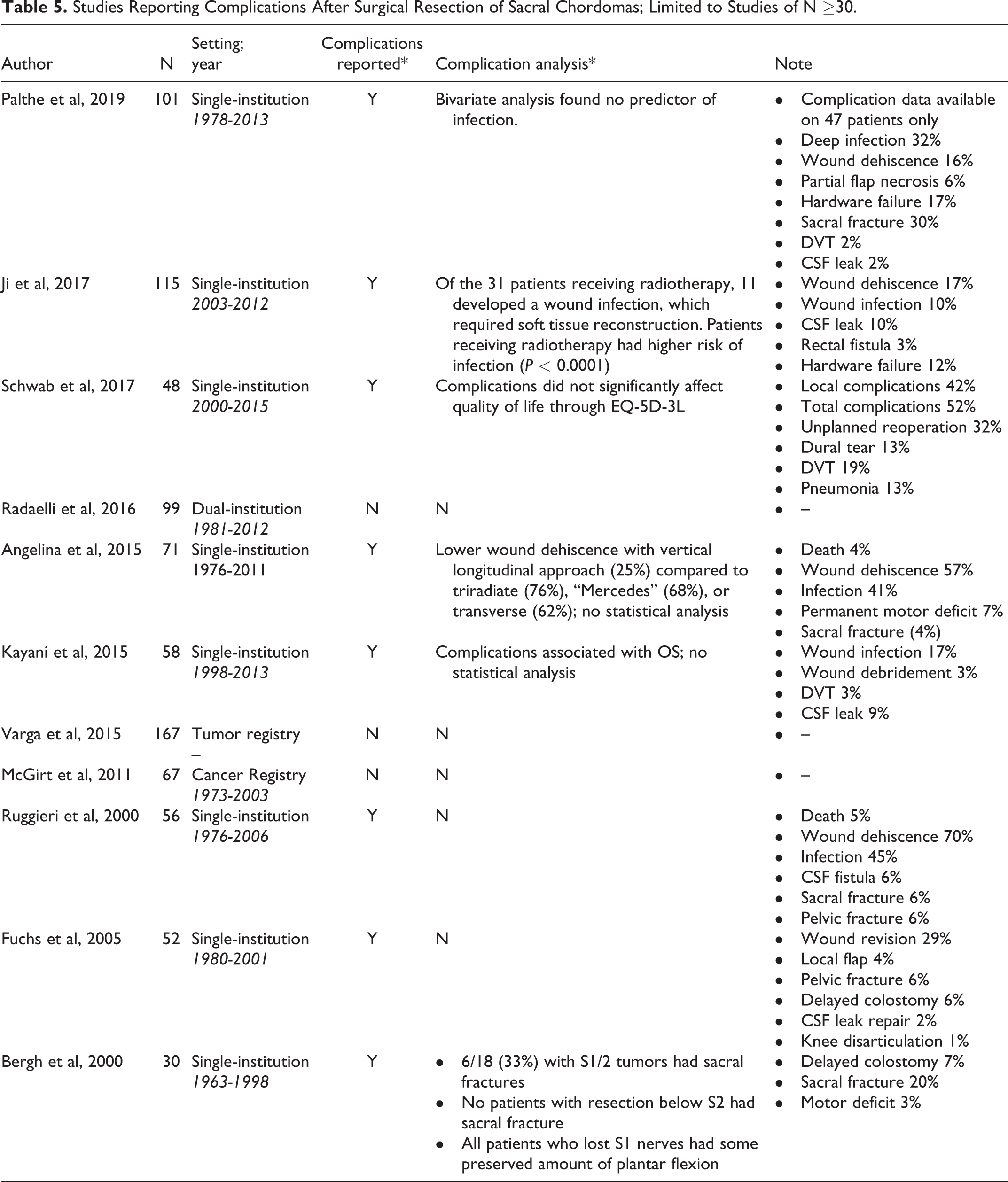
Despite robust prognostic survival and recurrence data, the surgical morbidity of these operations remains relatively understudied; however, more recent studies have begun to report more complete complication data. In our review of studies reporting surgical treatment of sacral chordomas with a minimum of 30 patients, 8 of 11 studies reported complications and 6 had some form of complication analyzes
Studies Reporting Complications After Surgical Resection of Sacral Chordomas; Limited to Studies of N ≥30.
We were not able to detect any statistically significant predictors of complications, in general, nor those that required reoperation. Patients who received neoadjuvant/adjuvant therapy had an increased likelihood of reoperation compared to those who did not receive therapy, but this did not reach statistical significance. Similar to other reports, 13 neither intralesional resection, tumor volume, nor age significantly influenced the risk of reoperation. 13 Two patients in our series required lumbopelvic fixation in a delayed fashion. Early biomechanical studies by Gunterberg 38 and others 39,40 have shown that lumbopelvic stabilization should be strongly considered after sacral amputations extending above the S1-2 junction. The 2 patients in our series who required lumbopelvic fixation both had high sacral amputations at the S1-2 junction and were left with a thin isthmus. Our experience has caused us to be more aggressive in placing instrumentation for tumor resections at the S1-2 level, particularly in patients anticipated to receive postoperative radiation.
To our knowledge, only 2 studies have correlated complications with survival, recurrence, or functional outcome. Ruggieri et al 13 reported actuarial survival and infection data but comparison between those with infection to those without was not included. In a study of 58 patients undergoing operative management of sacral chordomas, Kayani et al 16 stated that though the incidence of complications did not influence LR or metastases, complications were associated with reduced survival. No statistical analysis was included and limited information was reported regarding complications. With respect to functional outcomes in our series, no unexpected motor deficits were seen, and in many instances, total sacrectomy patients with sectioning of the S1 nerve root maintained/regained plantar flexion and were able to ambulate independently. One patient had unexpected bowel/bladder dysfunction despite maintenance of the S3 nerve roots, likely due to inadvertent injury to the distal pudendal nerves. Our results indicate that though deficits occurred, no added decrease in function was seen if a major complication or revision operation occurred.
The current study is not without limitation. This case series was drawn from a prospectively maintained spine database; however, the data was retrospectively analyzed. The inherent limitations of a retrospective analysis were present in our study, including missing data and reliance on routine clinical visits to extract specific data points. Some treatment information dated back to the late 1990s, and paper charts were reviewed to collect necessary data, which is likely less reliable than an electronic medical record. Secular trends in sacral chordoma management were not accounted for in our statistical modeling. Another limitation is that all patients were treated at a single institution, thus all clinical decision-making is subject to institutional treatment preferences/biases. It must be mentioned that while we were able to record whether adjuvant therapy was administered, detailed information about this therapy (type, dose, timing) was unfortunately not available. Adjuvant treatment of chordoma is heavily reliant on proton beam and/or stereotactic radiation, and not knowing this information significantly hinders our conclusions. In future studies, all adjuvant therapies should be noted in detail, especially what type is given, before or after surgical intervention, and any radiation associated complications. Lastly, the sample size was small for a multivariate analysis, which may have led to an underpowered study, wide confidence intervals, and a lack of precision. With a larger sample size, different statistical findings may be seen.
Conclusions
In considering patients for en bloc resection of sacral chordoma, it is important to understand the rationale for these aggressive procedures and to appreciate the potential for complications. In the current single-institution series, a negative margin resection significantly reduced the rate of local recurrence. In assessing the impact of major, minor, early, and delayed complications, neither major complication nor reoperation significantly impacted OS, LR, or functional outcome. Thus, it appears that the inherently high surgical morbidity associated with these invasive operations does not adversely alter the trajectory of survival and recurrence.
Footnotes
Author’s Note
This work was presented at the 2017 AANS/CNS Spine concerning the materials or methods used in this study or the findings specified in this paper. The authors have no personal or institutional financial interest in drugs, materials, or devices described in their submissions. Section Meeting in Las Vegas, NV.
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.