
Abstract
Study Design
Prospective Cohort Study of 108 cases.
Objective
Prone Transpsoas (PTP) fusion is a minimally invasive surgical technique using a single-position prone lateral approach to augment the anterior column of the lumbar spine. Degenerative spondylolisthesis (DS) is a common pathology where anterior-posterior access can be advantageous. This study aimed to evaluate operative, radiological and functional outcomes of PTP fusion in the management of symptomatic DS.
Methods
A multi-centre cohort study was conducted, involving 108 consecutive patients who underwent PTP fusion for low-grade (Grade I–II) DS. Descriptive statistical analysis was used to evaluate clinical, radiological and functional outcomes.
Results
In all 108 cases, anterior column fusion was combined with posterior percutaneous pedicle screw fixation to optimise spinal realignment. The cohort’s average operative time was 115 minutes, and the psoas retraction time was 14 minutes. The cohort had an average slip of 5.9 mm, which was reduced to 0.8 mm (P < 0.001) postoperatively. Statistically significant radiological improvements were observed in lumbar lordosis (Δ5°), segmental lordosis (Δ4°), anterior disc height (Δ 4.2 mm) and posterior disc height (Δ 2.1 mm). No major vascular or visceral complications were encountered. The sustained neurological complication rate was 1.9%, and patients maintained improved functional outcomes through the 1-year follow-up.
Conclusions
PTP is a safe approach for managing low-grade DS, showing significant postoperative correction of spinal alignment. These results support the use of PTP fusion for treating spondylolisthesis and add to the growing evidence of its safety and efficacy as a minimally invasive technique.
Keywords
Introduction
Prone Transpsoas (PTP) is a minimally invasive spinal (MIS) fusion technique used to address various spinal pathologies, including degenerative spinal conditions, deformity, trauma, and pathological conditions.1-3 The benefits of MIS techniques include reduced patient morbidity, minimised tissue damage, and decreased blood loss, all of which contribute to faster patient recovery while achieving the goals of surgery. 4 The minimally invasive PTP technique also offers the advantage of single-position surgery in the familiar prone position, leveraging a natural lordotic curvature. 5 Furthermore, it provides simultaneous access to both the anterior and posterior columns of the spine, allowing for anterior-posterior (360-degree) fusion, reduction, and decompression. 6 This can be particularly advantageous in cases of spondylolisthesis.
Spondylolisthesis can be classified according to aetiology (Wiltse)
7
and radiological severity (Meyerding).
8
Degenerative (Type III) low-grade spondylolisthesis, commonly observed at L4/5, is more prevalent in older adults (over 50 years of age) and in females.
9
The pathophysiology of the disease can involve facet joint arthropathy, leading to decreased structural support, ligamentous laxity, and intervertebral disc degeneration, all of which contribute to instability and slippage.
10
A symmetrical slippage at L4/5 can result in bilateral lateral recess narrowing and a decrease in disc height, affecting both the exiting L4 and traversing L5 nerve roots (Figure 1). However, spondylolisthesis with a rotatory component can present with unilateral compression symptoms and coronal deformity (Figure 2). Both these presentations can also lead to central canal stenosis with ligamentous hypertrophy or facet arthropathy, necessitating posterior decompression. The PTP fusion technique enables simultaneous access to reconstruct the anterior column via interbody work and to decompress, reduce, and fixate the posterior column, thereby helping realign the spine (Figure 3). (A) Axial T2-weighted MRI of the L-spine shows canal stenosis and lateral recess narrowing at L4/5, compressing both the exiting L4 and traversing L5 nerve roots bilaterally. (B) Lateral standing X-ray of the L-spine reveals Meyerding grade II spondylolisthesis at L4/5. (C) Sagittal T2-weighted MRI of the L-spine displays anterolisthesis of L4 on L5 with disc collapse and associated canal narrowing. (D) Post-operative CT of the L-spine shows complete reduction of the slip and re-alignment. (E) Post-operative EOS whole body standing X-ray. A 71-year-old woman presented with claudication symptoms, left-sided anterior thigh radicular pain, and mechanical back pain. (A) Sagittal T2-weighted MRI of the lumbar spine showing grade I spondylolisthesis at L3/4 and associated canal narrowing. (B) Axial T2-weighted MRI of the lumbar spine demonstrating canal stenosis, an asymmetric disc bulge, and lateral recess narrowing at L3/4. (C) EOS whole-body standing X-ray revealing dynamic instability at L3/4 and sagittal imbalance of 131 mm. (D) Post-operative EOS showing reduction of sagittal imbalance to 64 mm following single-level fusion at L3/4 and decreased slip at the index level. Coronal (E) and sagittal (F) post-operative CT images displaying the final implant position spanning the epiphyseal cortical rim. IVC: inferior vena cava, AA: abdominal aorta (A) Pre-operative sagittal T2-weighted MRI of the lumbar spine showing grade II anterolisthesis of L4 on L5. (B) Post-operative sagittal T2-weighted MRI of the lumbar spine demonstrating reduction of the slip and spine realignment. (C) Pre-operative axial T2-weighted MRI of the lumbar spine, revealing lateral recess narrowing at L4/5 and a “Mickey Mouse” Psoas. (D) Post-operative axial T2-weighted MRI of the lumbar spine showing indirect decompression with an interbody cage. (E) Pre-operative EOS full body standing X-ray displaying sagittal imbalance of 35 mm. (F) Post-operative EOS scan indicating sagittal imbalance reduced to 14 mm.


The objective of this study was to assess the operative, clinical, and radiological outcomes of PTP fusions specifically in patients with symptomatic low-grade (Meyerding grade I-II) degenerative spondylolisthesis (DS). Primarily, the radiological assessments aimed to quantify the pre-operative degree of slippage and the effectiveness of the surgery in achieving post-operative spinal realignment and optimisation of lordosis.
Methods
We conducted a prospective cohort study across 4 centres in Sydney and Melbourne, Australia, with 2 lead surgeons. The study received ethical approval from AHCL Human Resources Ethics Committee [ID 2024-007] in accordance with NHMRC guidelines. The study adhered to the STROBE guidelines. 11
Cohort Population
Consecutive patients who underwent PTP fusions for DS from March 2023 to March 2025. Inclusion criteria were all patients who underwent PTP for symptomatic degenerative spondylolisthesis with at least 3 months of clinical and radiological follow-up. The patients had radiological evidence of spondylolisthesis and associated neurological sequelae, such as radiculopathy or neurogenic claudication with central or foraminal stenosis. Exclusion criteria included patients with adjacent segment disease or revision surgery, greater than 2 levels of instrumentation, Meyerding grade III or IV spondylolisthesis, or radiological evidence of vertebral fractures at the index level (osteoporotic or pathological). All patients who met these criteria were successfully enrolled in the study after providing written informed consent.
Surgical Technique
The PTP surgical technique used by the primary operators has been previously described.
12
First, the side of approach is determined to facilitate surgical setup and planning.
13
Patients are given intravenous anaesthesia, then electrodes are placed on the patient’s limbs and scalp for intraoperative neuromonitoring. This includes monitoring of femoral nerve health through somatosensory evoked potentials (SSEPs) of the saphenous nerve, the terminal sensory branch of the femoral nerve.
14
Patients are positioned prone and secured onto the patient positioners. The Image Intensifier (II) fluoroscopy is used to mark the skin incision for the lateral approach and to target the relevant disc space (Figure 4). The patient is prepped and draped widely in routine sterile technique to allow for simultaneous access to the lateral flank and the posterior elements for screw placement and decompression. In our experience, low-grade spondylolisthesis may be reduced, either partially or entirely, once the patient is anaesthetised in the prone position. For Grade I spondylolisthesis, interbody cage placement is completed first, followed by percutaneous pedicle screw placement and then direct decompression as required. An 80-year-old woman presented with a 2-year history of back pain, claudication symptoms, and right-sided paraesthesia on a background of rheumatoid arthritis. (A) Sagittal T2-weighted MRI of the L-spine showing grade II spondylolisthesis at L4/5. (B) Axial T2-weighted MRI of the L-spine demonstrating canal stenosis, facet arthropathy, and lateral recess narrowing at L4/5 with ligamentous hypertrophy. (C) Erect L-spine X-ray displaying L4/5 spondylolisthesis. (D) Intra-operative II targeting of the L4/5 disc space aimed at the overlapping area of the cranial and caudal vertebrae. (E) Lateral II of the PTP retractor, open at the index level, providing access to the disc space. (F) Post-operative sagittal CT scan showing the final position of the interbody cage in a mid-sagittal view, with complete reduction of the slip and posterior decompression
The skin incision is made on the lateral flank, followed by blunt dissection through the 3 layers of the abdominal wall into the retroperitoneal space. The psoas muscle is located with either direct vision or digital palpation to guide the first dilator onto the relevant disc space, dorsal to the hand, helping protect the abdominal contents. Fluoroscopy is used to confirm the dilator position in both anteroposterior (AP) and lateral views. In cases of spondylolisthesis, the safe landing zone is further narrowed to the overlapping region between the cranial and caudal vertebral bodies. Triggered electromyography (tEMG) is then used to verify proximity to neural structures, both dorsally and ventrally. Subsequent dilators are inserted with tEMG checks, and the lateral retractor is finally inserted and secured onto the patient and table. The retractor is opened in the dorsoventral plane, and the perimeter is rechecked with tEMG before securing the retractor into the disc space with anterior and posterior shims. Then, annulotomy and discectomy are performed, and the endplates are prepped routinely (Figure 5). The appropriate cage sizes are trialled under fluoroscopy guidance, and the final implant is inserted. After the final position is confirmed in AP/lateral views, the retractor is removed under direct vision, and any necessary haemostasis is achieved. The lateral incision is closed in routine layered fashion while the posterior component of the surgery is performed simultaneously. A 73-year-old woman presented with claudication, left-sided radicular pain, and longstanding mechanical back pain that did not improve with conservative management, including analgesia, physiotherapy, and corticosteroid injections. (A) Sagittal T2-weighted MRI of the lumbar spine showing grade I anterolisthesis of L4 on L5 and canal narrowing. (B) Axial T2-weighted MRI of the lumbar spine demonstrating canal stenosis and lateral recess narrowing at L4/5, compressing both exiting L4 and traversing L5 nerve roots bilaterally. (C) EOS whole-body standing X-ray showing sagittal imbalance of −34 mm. (D) Lateral intraoperative Image Intensifier (II) image depicting targeting of the L4/5 disc space with the patient in a prone position, assisting in reducing the slip. (E) Anteroposterior (AP) II image of angled cob insertion for disc preparation. Final intraoperative II images show the cage position in AP (F) and lateral (G) views. Note. IVC, inferior vena cava; RCIA, right common iliac artery; LCIA, left common iliac artery
In circumstances where the safe landing zone is limited by the degree of spondylolisthesis or if intraoperative neuromonitoring alerts preclude safe docking of the dilators, reduction of the spondylolisthesis may be performed before placement of a prone lateral cage. Pedicle screws are navigated into the appropriate spinal levels using intraoperative navigation, with the cranial screws countersunk relative to the caudal screws. Simultaneous bilateral reduction of the cranial level is then performed using the reduction towers once the caudal screws are torqued off over a lordotic rod. If reduction is not complete in this manner, a facectomy is performed bilaterally using pedicle-based retractors before reduction of the cranial vertebra. Upon full reduction, the PTP approach is then completed safely, with the placement of an interbody cage before final torque-off of the cranial screws.
Clinical and Radiological Measures
Patient demographics, intraoperative data, clinical, radiological, and functional outcomes were collected. Intraoperative data collected include the number of interbody levels operated, the type of decompression (indirect vs direct), total anaesthesia time, total operative time, lateral surgical time, psoas retraction time, and neuromonitoring alerts.
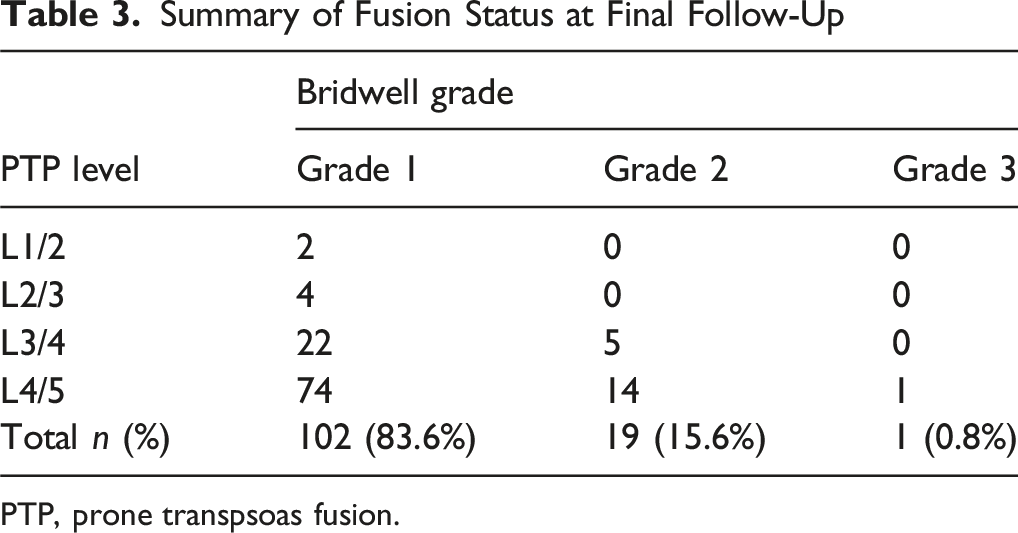
Radiological parameters, including lumbar lordosis (LL), segmental lordosis (SL), anterior disc height (ADH), posterior disc height (PDH), and spondylolisthesis/slip, were measured with radiographs preoperatively and postoperatively at the 3-month follow-up, up to 1-year follow-up. Furthermore, the average cage placement in the mid-vertebral sagittal plane relative to the caudal vertebral body was evaluated on postoperative imaging. Early and delayed subsidence was assessed with Marchi scores. 15 Lastly, fusion status is evaluated with follow-up thin-slice CT L-spine and graded according to the Bridwell classification system. 16 Two independent assessors performed radiological measurements to mitigate potential sources of bias.
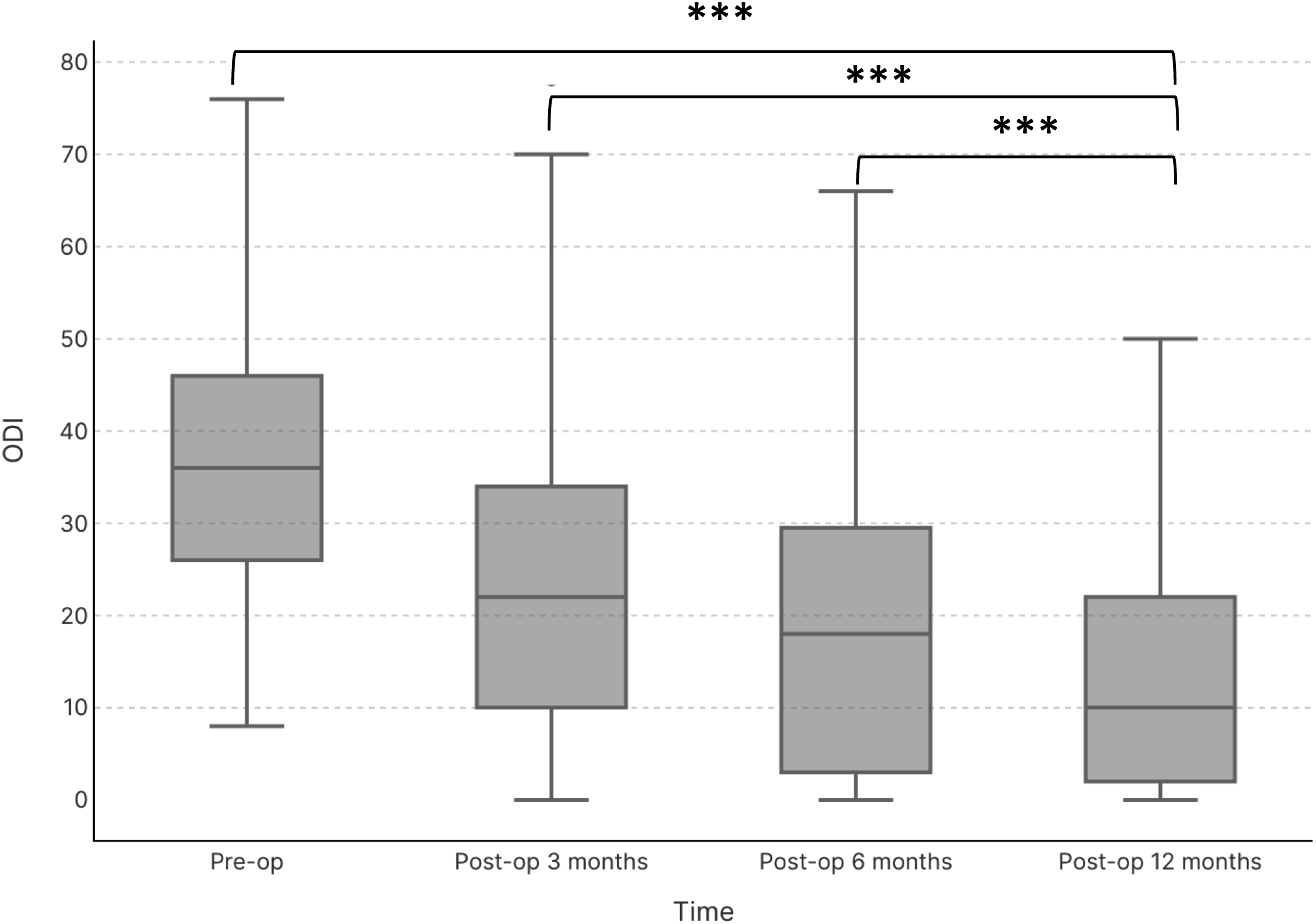
Functional outcomes were quantified using the 12-item Short Form Survey (SF-12) 17 and Oswestry Disability Index (ODI) 18 preoperatively and postoperatively at 3-month, 6-month, and 12-month intervals.
Statistics
Descriptive statistics were used to analyse operative and radiological data. Means, standard deviations, and paired t-tests, with α set at P ≤ 0.05, were used to evaluate radiological changes in LL, SL, ADH, PDH, and slip degree. Box plots were created to visualise average cage placement on the vertebral body of the caudal vertebra. Similarly, ODI and SF-12 data were analysed for mean and standard deviation, paired t-tests were used to evaluate the data at the predefined timepoints, and follow-up rates were calculated. Box plots were created to visualise the data and trends over time.
Results
Demographics
Demographics of Study Participants

PTP, prone transpsoas fusion.
Operative Outcomes
The average anaesthetic time was 170 (±72) minutes, with a total operative time of 115 (±63) minutes; from skin incision to last skin closure after completing all components of the surgery. More specifically, the total operative time for indirect decompression is 100 minutes, whereas the total operative time with posterior decompression is 130 minutes. The lateral operative time for the anterior column fusion was 39 (±16) minutes, which is from lateral skin incision to lateral skin closure. Lastly, the average psoas retraction time is 14 (±6) minutes, measured from the time the retractors are secured onto the patient at the index level to the time the retractor is closed and removed. There were 7 intraoperative SSEP alerts from the saphenous nerve, for which rescue measures were used, including closing the retractor and reducing the stretch on the psoas.
Clinical Outcomes and Complications
Summary of Surgical Complications

PTP, prone transpsoas fusion.
Radiographic Outcomes
A total of 122 levels with spondylolisthesis were treated across 108 patients. This included 98 levels of Grade I spondylolisthesis with an average slip of 5.0 mm (15%), and 24 levels of Grade II with an average slip of 9.3 mm (30%).
Radiological analysis demonstrated a significant reduction in spondylolisthesis: the average slip decreased from 5.9 mm (±2.4) pre-operatively to 0.8 mm (±1.3) post-operatively (P < 0.001) (Figure 6). The average interbody cage placement in the mid-sagittal plane is 46% from the ventral edge of the caudal vertebral body (Figure 7).
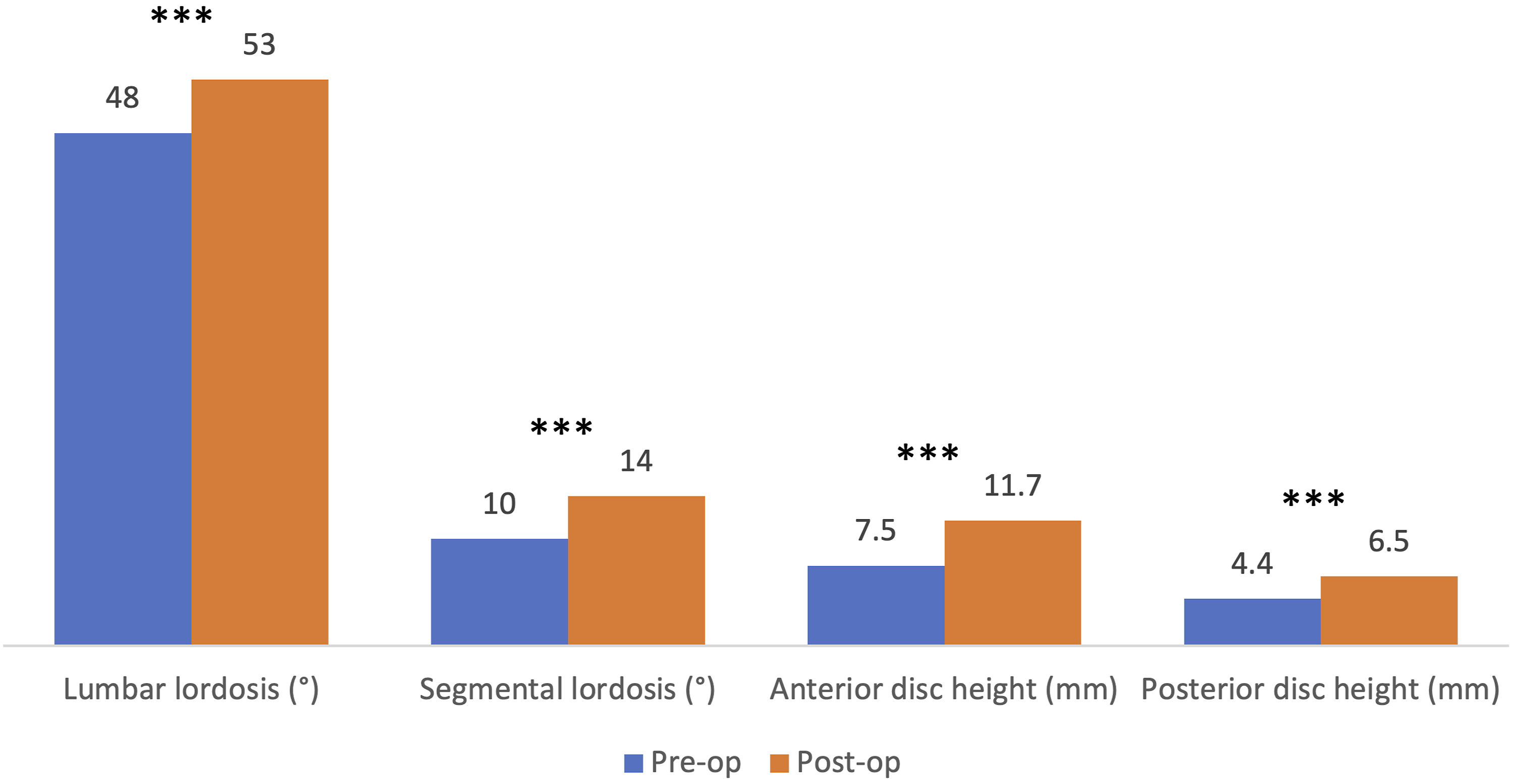
Lumbar lordosis improved significantly from 48° (±13°) pre-operatively to 53° (±13°) post-operatively (P < 0.001). Segmental lordosis increased from 10° (±5°) to 14° (±7°) (P < 0.001). Anterior disc height (ADH) improved from 7.5 mm (±2.8) to 11.7 mm (±2.0) (P < 0.001), and posterior disc height (PDH) increased from 4.4 mm (±1.8) to 6.5 mm (±1.9) (P < 0.001) (Figure 8). Average pre-operative slip of 5.9 mm, reducing to 0.8 mm post-operatively, P < 0.001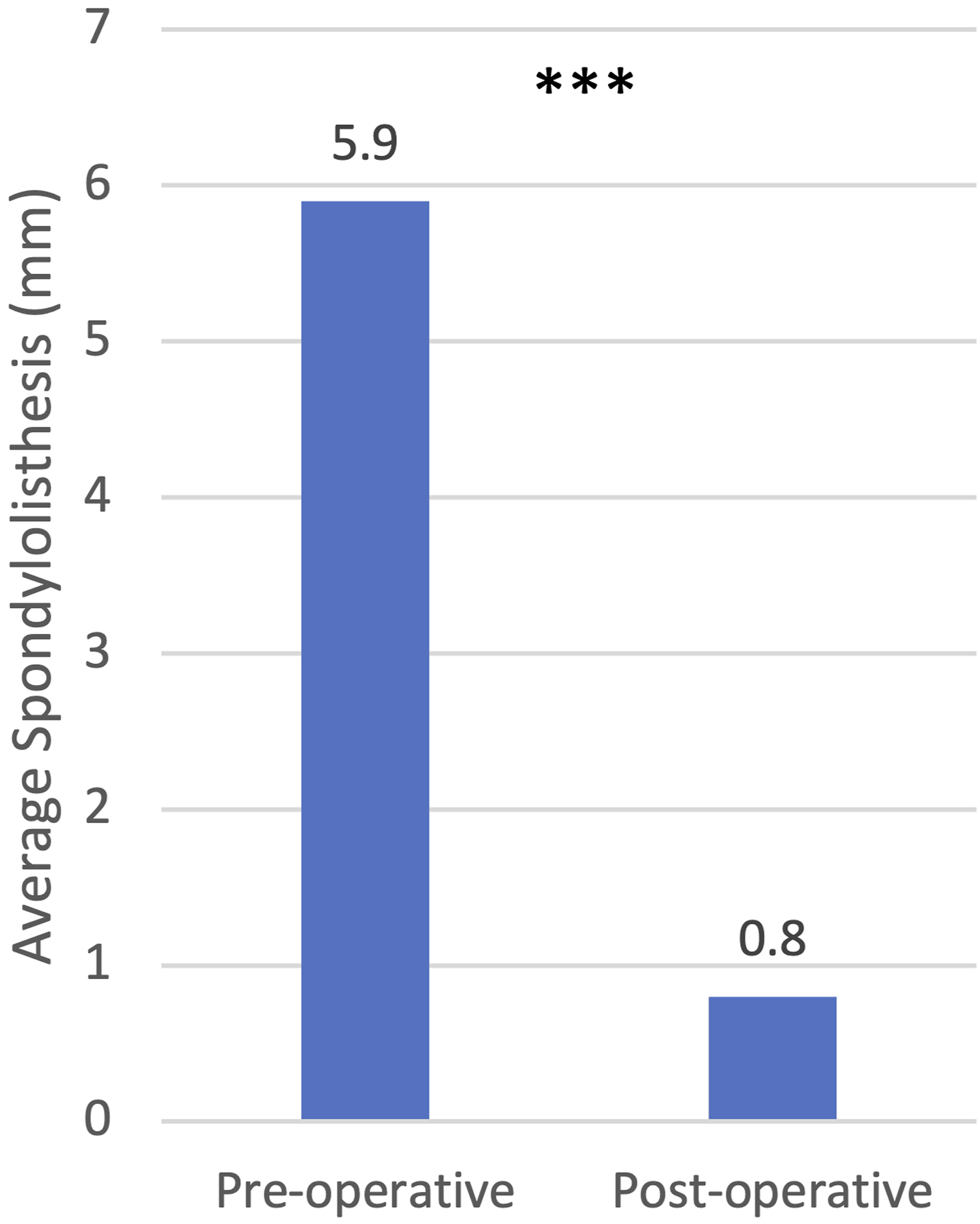
Summary of Fusion Status at Final Follow-Up
PTP, prone transpsoas fusion.
Functional outcomes, assessed by the SF-12, improved from a pre-operative average of 34.7 (±8.9) to 39.5 (±8.7, P = 0.03) at 3 months and 44.5 (±9.7, P = 0.004) at 6-12 months post-operatively (Figure 9), with follow-up rates of 93% and 96% respectively. ODI scores showed a consistent reduction in disability, decreasing from 36.8% pre-operatively to 23.4% at 3 months (P < 0.001), 19.9% at 6 months (P = 0.001), and 14.7% at 1 year (P < 0.001) (Figure 10), with follow-up rates of 72%, 39%, and 44% respectively. A 71-year-old female presented with claudication symptoms and mechanical back pain. (A) Axial T2-weighted MRI of the L-spine showing severe canal narrowing and facet arthropathy at L3/4. (B) Sagittal T2-weighted MRI of the L-spine revealing grade I anterolisthesis at L3/4. (C) Post-operative CT with final cage placement, spinal re-alignment, and indirect decompression using a titanium cage. (D) Box plot showing the average position of the intervertebral cage in the mid-sagittal plane at 46% (range 28-68%) from the ventral edge of the caudal vertebral body Graph comparing pre-operative and post-operative radiological parameters. Lumbar lordosis increased from 48° to 53° (P < 0.001), segmental lordosis increased from 10° to 14° (P < 0.001), anterior disc height increased from 7.5 to 11.7 mm (P < 0.001), and posterior disc height increased from 4.4 mm to 6.5 mm (P < 0.001)
Discussion
Our study investigated the clinical, radiographic, and functional outcomes of PTP fusion in a prospective cohort of 108 consecutive patients with symptomatic low-grade (Grade I–II) DS. All patients presented with back pain and associated neurological sequelae with claudication symptoms or radiculopathy, which affected their quality of life. While surgery has been shown to be superior to non-operative management,
19
the role of fusion remains a topic of debate.20,21 Furthermore, the safety and efficacy of various fusion approaches in treating symptomatic DS are active areas of research. Box plot comparing the short form 12-item health survey (SF-12) pre-operatively, with an average physical and mental component score of 34.7 (±8.9) out of 50, to post-operative improvements at 3 months, increasing to 39.5 (±8.7, P = 0.03), and further improvement at 6-12 months to an average score of 44.5 (±9.7, P = 0.004) Box plot comparing oswestry disability index (ODI) scores pre-operatively, with an average of 36.8%, to 3 months post-operatively at 23.4% (P < 0.001). Scores decreased again at 6 months to 19.9% (P = 0.001) and further dropped to 14.7% (P < 0.001) at one year follow-up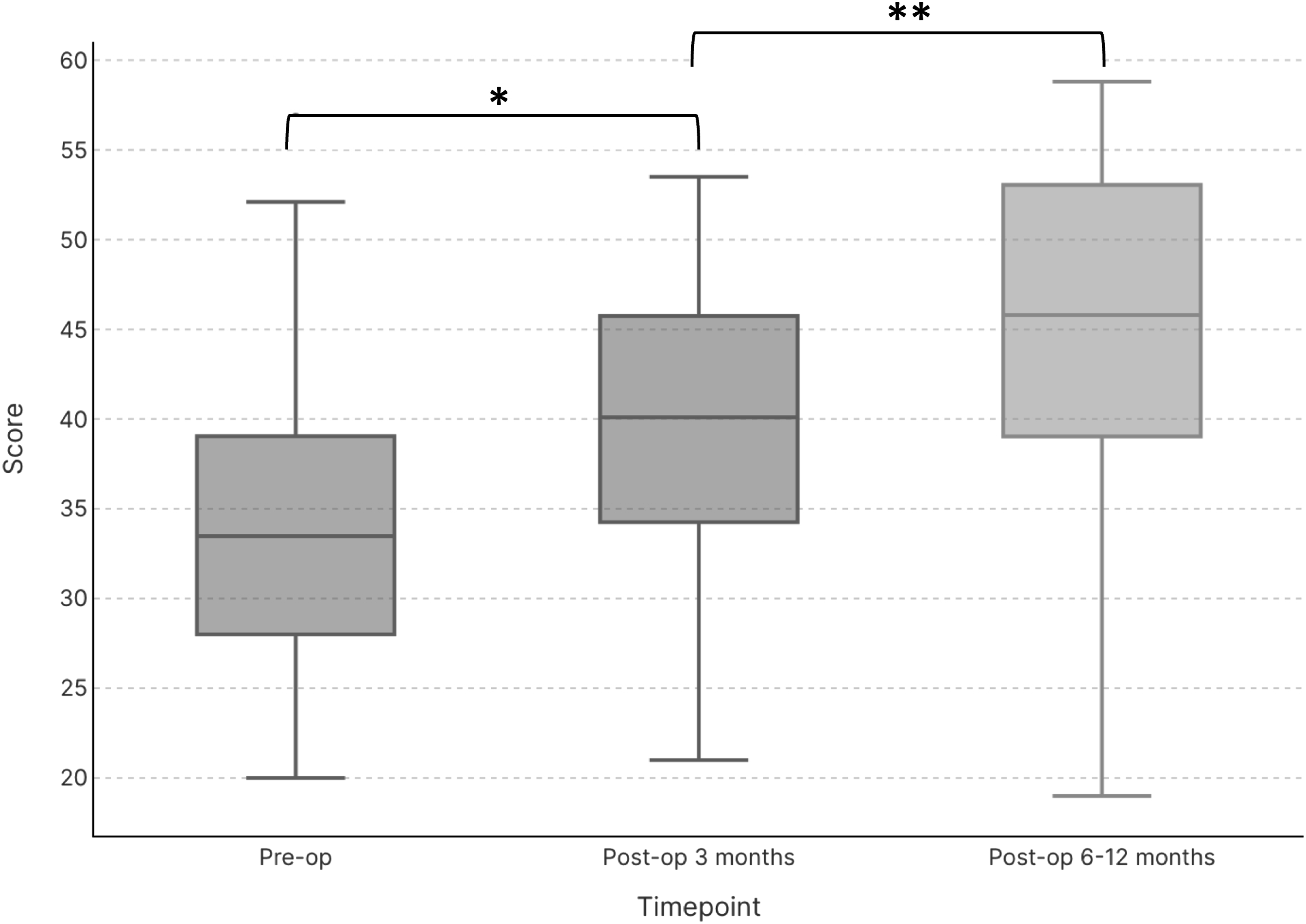
Spondylolisthesis introduces the challenge of spinal misalignment alongside compressive pathology. The various fusion techniques ideally aim to address multiple surgical goals, including neural decompression, spinal realignment, restoration of disc height, and optimisation of global alignment. Open posterior interbody fusion techniques, used for decades, have paved the way for anterior-posterior or 360-degree lumbar fusions. However, the newer minimally invasive spinal fusion techniques offer several advantages over the traditional open approach, including decreased tissue damage, blood loss, and a shorter average hospital stay.22-24 The lateral approach for lumbar interbody fusion employs a minimally invasive retroperitoneal technique to position a large lateral cage on the cortical rim, thereby leveraging ligamentotaxis for indirect decompression. Although single-position lateral interbody fusion with percutaneous pedicle screws in the lateral decubitus position has been described, 25 the evolution of lateral surgery to the prone lateral technique offers several advantages. The prone position provides easier access to the facets, facilitating reduction compared to the lateral decubitus position. In this study, the prone position is preferred by the primary operators due to the ability to complete pedicle screws first, thereby increasing the safe landing zone with prior reduction when required. This aids in the placement of a wider footprint cage for interbody fusion. PTP offers the same benefits as the lateral approach in the familiar prone position, allowing simultaneous posterior access for decompression. By eliminating repositioning time, it improves operative efficiency, decreasing total anaesthetic time. 3
Next, the duration of operation is an independent risk factor for post-operative complications in lumbar fusions. 26 This study’s average operative time of 115 minutes for the anterior-posterior fusion is comparable and slightly better than published systematic reviews comparing open posterior lumbar interbody fusion (PLIF) studies, 148-203 minutes, and MIS PLIF/transforaminal lumbar interbody fusion (TLIF) studies averaging 148-275 minutes.27-29 The PTP technique leverages the benefits of both lateral and posterior approaches in the familiar prone position, improving operative efficiency.30,31 Furthermore, the single-stage procedure, even in multilevel cases, reduces anaesthetic exposure, an essential consideration in elderly patients who are at a higher risk of anaesthetic-related complications. 32 The average hospital stay of 4 days further highlights the benefits of a minimally invasive spinal approach and its positive implications for patient recovery.
The PTP approach successfully reduced the average slip from 5.9 mm to 0.8 mm, achieving realignment at the index level. The large lateral lordotic cage, positioned onto the cortical rim of the vertebral body, contributes to robust anterior column reconstruction. Radiographic outcomes demonstrated a significant restoration of sagittal alignment, with an improvement in lumbar lordosis from 48° to 53° (Δ5°), and a corresponding increase in segmental lordosis from 10° to 14° (Δ4°). This is comparable to the existing meta-analysis of MIS fusions, which shows improvements in both LL (Δ5.2°) and SL (Δ2.3°).33,34 Our data also compare well with a 1-year follow-up PTP cohort study, which reported improvements in LL of Δ3° and SL of Δ5°. 5 Notably, these improvements were observed in a cohort in which the majority underwent single-level L4/5 fusion, highlighting the value of segmental correction in shaping overall spinal alignment. 35
Furthermore, the increases in anterior and posterior disc height underscore the importance of reconstructing the anterior column. Specifically, the average gain in PDH from 4.4 mm to 6.5 mm contributes to restoring foraminal height. This, along with reduced slip, allowed surgeons to avoid direct decompression in 47 cases in this study, thereby preserving the posterior tension bands.
The average cage position, located 46% from the ventral vertebral border in the sagittal plane, aligns with previously described safe landing zones. 36 The surgeons target the midpoint of the overlapping disc space between the cranial and caudal vertebrae at the operative level using intraoperative fluoroscopy. Accurate targeting of the L4/5 disc space is critical, especially in spondylolisthesis, where the landing zone is further narrowed. The ability to consistently achieve this position across cases emphasises the technical reproducibility of the approach.
There was no early subsidence in the cohort. This is attributed to the lateral technique and care during disc preparation, ensuring that the endplates are not violated, especially caudally. Furthermore, the lateral cage spanning the epiphyseal ring also helps mitigate the risk of implant subsidence, in conjunction with percutaneous pedicle screw fixation, to achieve a robust anterior-posterior fusion. The surgical approach, disc preparation technique, implant biomechanics, and 360-degree fusion contribute to the high fusion rates observed in the cohort.
The delayed subsidence rate for the cohort is 2.8%. Notably, the reasons for subsidence included endocrinopathies such as osteoporosis and Vitamin D deficiencies in 2 of the 3 cases, resulting in fractures post-falls. Bone mineral density scans were not routinely performed in the cohort, underscoring the importance of a comprehensive bone health work-up in patients experiencing these complications in the post-operative setting.
Functionally, patients experienced significant improvements in both SF-12 and ODI scores. The SF-12 scores improved from 34.7 preoperatively to 44.5 at 6-12 months, while ODI scores decreased from 36.8% to 14.7% (Δ22.1%) at one year. These gains are clinically meaningful and align with the primary surgical goal of relieving neurological symptoms and improving patients’ quality of life. The change in ODI scores from baseline also compares well with the NORDSTEN trial, which reported an average decrease of 21.3% in the fusion cohort. 20
Lastly, this study reports no major vascular or visceral complications, with a sustained neurological complication rate of 1.9%, which is comparable to the 2.8% complication rate reported in a meta-analysis of transpsoas fusions. 37 Transient sensory deficits of 6.5% with complete resolution by 3 months are encouraging for patients experiencing neurological symptoms in the acute postoperative period. Furthermore, the resolution of sustained motor deficits by the 1-year follow-up in our cohort has also been observed in patients with femoral plexopathies in another extended follow-up PTP study. 5 Transient motor and sensory deficits are known risks associated with transpsoas procedures, with complication rates ranging from 2.4% to 36.07% reported in the literature.2,37,38 In this cohort, transient motor weakness was not assessed due to multifactorial causes, including pure psoas cause secondary to transpsoas approach and muscle stretch, psoas haematomas, and iliopsoas tendonitis that can mimic plexopathies.
Importantly, this cohort includes the initial learning curve for surgeons following the introduction of PTP in Australia in March 2023, suggesting a favourable safety profile for this technique. 12
Limitations
This study focused on patients with degenerative Grade I and II spondylolisthesis, which, while allowing for a homogenous pathological cohort, limits generalizability to higher-grade cases. Additionally, while the data were collected prospectively, the absence of a control group introduces potential selection bias. The study also reflects early experience with the PTP technique, which may affect complication rates or surgical efficiency during the initial learning curve. Finally, while short-term and mid-term outcomes were assessed, long-term results beyond one year were not evaluated.
Conclusion
This multi-centre study demonstrates that among a symptomatic low-grade DS cohort, the PTP fusion technique was a safe treatment option. The realignment of spondylolisthesis at the index level further shows the efficacy of PTP in this cohort. The sustained rate of neurological complications of 1.9%, radiological improvements in spinal alignment, and the improvements in function and disability reported here are comparable to results in the existing literature. The study provides support for the single-position, minimally invasive approach in improving operative efficiency while maintaining a low complication profile.
Footnotes
Ethical Considerations
Multicentre study approval was obtained through AHCL Human Research Ethics Committee (NHMRC ID: VR00025, Project ID: 2024-007).
Consent to Participate
All patients provided informed written consent for the study.
Consent for Publication
All patients provided publication of associated case details, data, and imaging.
Author Contributions
(I) Conception and design: VSR.
(II) Administrative support: BO, YYW, KP, DA.
(III) Provision of study materials or patients: BO, YYW.
(IV) Collection and assembly of data: VSR, YYW.
(V) Data analysis and interpretation: VSR.
(VI) Manuscript writing: All authors
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ATEC Research Grant.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VSR is funded as a Research Fellow at O SPINE through ATEC Research Grant. BO holds consultancy positions with Globus Medical and ATEC. YYW holds consultancy position with ATEC. KP and DA have nothing to declare.
Data Availability Statement
The authors agree to the journal’s data sharing policy.