
Abstract
Study Design
Retrospective analysis and case series.
Objectives
This study evaluates the differences in electromyography (EMG) recordings when using a novel table rotation technique for the placement of dilators and retractors compared to the standard technique for a prone transpsoas (PTP) lateral lumbar interbody fusion at L4-5.
Methods
Ten patients underwent single-level PTP surgery at L4-5, with EMG recordings anteriorly and posteriorly on top of the psoas muscle and at the disc space. EMG recordings were evaluated with the bed in a neutral position and again after the operating table was rotated 30° away from the surgeon.
Results
All 10 patients had significantly improved EMG values at all points after table rotation. Before table rotation, the posterior EMG values were in the risk zone (<6 mA) for 7 of 10 patients when measured on top of the psoas and for 5 of 10 patients when measured at the disc space. After the table rotation, no patient had posterior EMG recordings in the risk zone. Similarly, all anterior EMG recordings demonstrated improvement after table rotation.
Conclusions
The table rotation technique was effectively used with the PTP approach to safely access the L4-5 disc space farther from the lumbar plexus in our patients, with EMG recordings at safer thresholds.
Keywords
Introduction
The transpsoas approach for lateral lumbar interbody fusion (LLIF) has gained popularity as a minimally invasive technique for accessing the anterior column of the lumbar spine. Stand-alone LLIF is an effective treatment modality for a multitude of spinal pathologies, including adjacent segment disease,1,2 but supplementation with posterior pedicle screw fixation offers additional support and biomechanical stability that is necessary for certain patients.3,4 One of the disadvantages of supplemental posterior fixation has been the need for repositioning in the operating room between the LLIF, which is performed in the lateral decubitus position, and the pedicle screw placement, which is performed in the prone position. The prone transpsoas (PTP) approach circumvents this disadvantage and allows the lateral interbody and percutaneous pedicle screws to be placed simultaneously in the prone position.
As surgeons adopt the PTP approach, the technique continues to be improved and modified to overcome its unique challenges.5-7 One of the challenges with the transpsoas approach in the lateral decubitus and prone positions has been the risk of femoral nerve injury at the L4-5 level,8-10 where the lumbar plexus tends to have a more anterior position and can narrow the safe entry zone.11,12 A retrospective study by Cahill et al 13 reported postoperative femoral nerve injury in 4.8% of LLIFs performed at L4-5, with no femoral nerve injury observed with LLIF at any other level. The anterior positioning of the lumbar plexus tends to migrate the docking of the retractor more anteriorly along the vertebral body, because attempting to dock in an ideal position posteriorly tends to place the entry too close to the lumbar plexus and introduces a higher risk for neural injury. Table rotation can benefit the surgeon when accessing the L4-5 disc space with the PTP approach and allows for safer docking posteriorly without putting the lumbar plexus and femoral nerve at increased risk of injury.
This article describes and reports the results of a table rotation technique used with the PTP approach to improve access to anatomically complex L4-5 cases.
Methods
A retrospective analysis of prospectively collected data from 10 consecutive patients undergoing single-level PTP at the L4-5 level for degenerative spondylolisthesis in 2021 and 2022 was performed. The table rotation technique was used to access the disc space. Institutional review board approval was not required because the study solely reports intraoperative findings that did not deviate from the standard of care. All patients consented to the operation, and the senior author (B.S.L.) performed all the procedures. Patients requiring multilevel procedures, patients undergoing stand-alone interbody fusions, patients with prior fusions, or patients with psoas/vascular anatomy that would prevent a lateral approach were excluded from the study. Ten consecutive patients were enrolled, and no patient met the exclusion criteria. All patients underwent preoperative imaging, including magnetic resonance imaging, computed tomography, and standing plain films. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) reporting guidelines were implemented in this study. 14
Electromyography (EMG) values were collected with the retractor positioned on top of the psoas muscle and again at the disc space. At each position, EMG thresholds were recorded both anteriorly and posteriorly. EMG threshold values were categorized into 3 zones: the risk zone (<6 mA), the warning zone (6-11 mA), or the safety zone (>11 mA), as previously described by Tohmeh et al. 15 EMG values were recorded first using the standard approach with the bed in a neutral position. EMG values were then recorded using the table rotation technique, with each patient acting as their own control group.
Intraoperative neuromonitoring was performed using the AlphaTec Safe-Op Neural InformatiX system. This system included free-run EMG with electrodes in the vastus lateralis, vastus medialis, tibialis anterior, medial gastrocnemius, and abductor hallicus muscles. All EMG electrodes were placed by a neuromonitoring technician under the supervision of a neurophysiologist.
The data were compiled into Excel spreadsheets and analyzed using R software. The Shapiro-Wilk test was used to assess the normality of the data. Welch’s t test was used for variables with normal distributions. For variables that were not normally distributed, the Yuen-Welch t test was used, with a trimming of 0.1. Data were reported as counts and percentages for categorical variables, and Fisher’s exact test was used to assess differences between groups. The effect size of Welch’s t test was calculated using Cohen’s d. The robust effect size technique was used to calculate the effect size using the Yuen-Welch t test. Statistical significance was set at P < 0.05.
Table Rotation Technique
Patient positioning and setup are performed as previously described with the standard PTP approach.
5
Before inserting the dilator at the L4-5 level, emphasis should be placed on obtaining accurate anteroposterior and lateral fluoroscopy images, indicated by parallel endplates and spinous processes located at the midline between the pedicles. The skin is marked accordingly using these lateral images. The table is then rotated away from the surgeon using the anteroposterior images. If the width of the vertebral body on anteroposterior fluoroscopy is visually divided into thirds, the table should be rotated until the spinous process moves from the midline upward toward the contralateral pedicle at the two-thirds mark on repeated fluoroscopy images (Figure 1). The initial dilator is then inserted under fluoroscopic guidance, using lateral images, until it is positioned on top of the psoas muscle. Because the table is rotated, the dilator will not be perfectly orthogonal to the disc space but at a slight angle. Directional EMG is then performed. If the EMG thresholds are within the risk zone (<6 mA), the table can be further rotated and the dilator reinserted. If the EMG thresholds are within the warning zone (6-11 mA) or the safety zone (>11 mA), the dilator is advanced through the psoas on the disc space, and directional EMG is performed again. If EMG thresholds remain in the warning or safe zones, the surgeon inserts the Kirshner wire into the disc space. Sequential dilators are then inserted under fluoroscopic guidance, and repeated directional EMG is performed after each dilation. The retractor is then inserted. The table is rotated back to the neutral position while maintaining pressure on the dilator to hold its position on the disc space. Once the table is back in a neutral position, the dilator should be positioned orthogonally to the disc space and affixed to the table via the articulating arm. Lateral fluoroscopy can be used to ensure adequate positioning in the anteroposterior dimensions. The spinal surgeon performs the remainder of the procedure using the standard PTP technique, as described elsewhere.
5
The described technique is performed without direct visualization and instead relies on palpation of anatomical structures such as the psoas muscle, transverse process, and quadratus lumborum confirmed with fluoroscopy. (A) Anteroposterior radiograph before table rotation, showing that the spinous processes at the operative level are directly aligned (black line) with the midline between the pedicles. (B) Anteroposterior radiograph showing the spinous processes at the operative level at the “30% line” (black line) between the pedicles, indicating that the table has been rotated enough. Used with permission from Barrow Neurological Institute, St. Joseph's Hospital and Medical Center, Phoenix, Arizona.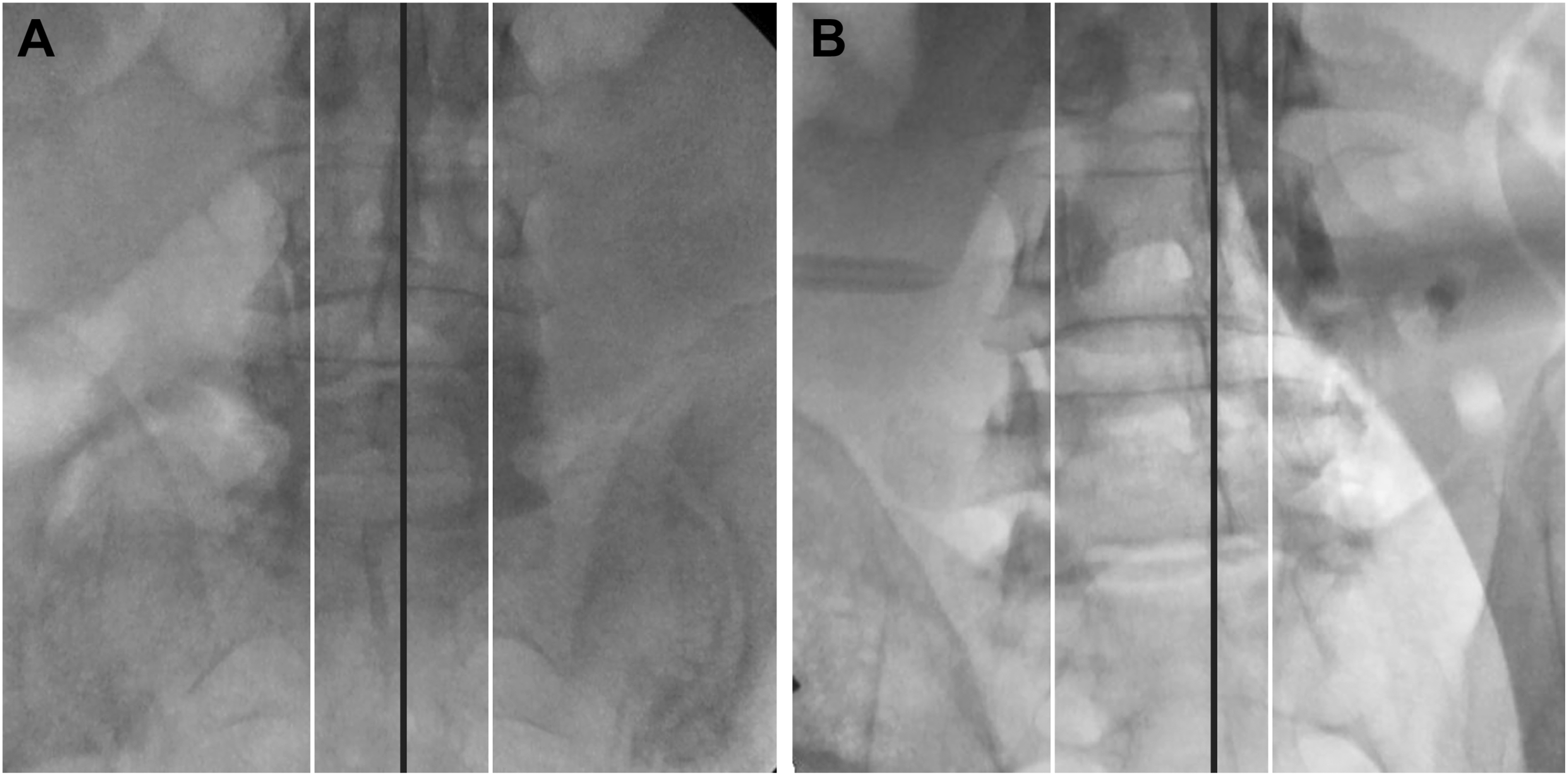
The mechanism by which this technique places the dilator farther from the lumbar plexus while allowing a more posterior docking position is due to the anterior-to-posterior insertion angle of the initial dilators. The dilators enter the psoas more anteriorly but can dock closer to the “50-yard line” on the disc space because of the oblique angle of entry. When the table is rotated back to neutral, the retractor is then orthogonal to the disc space. The tip of the dilator on the disc space remains around the 50-yard line, but there is more muscle between the posterior blade of the retractor and the lumbar plexus because the dilators initially went through the psoas more anteriorly and farther away from the plexus. The concept behind the table rotation technique is illustrated in Figures 2 and 3. Illustration of how the table rotation maneuver improves access to the L4-5 disc space (purple shading), farther from the femoral nerve during the PTP approach (green arrow). The top panel illustrates the standard PTP approach with the table in neutral position and the retractor docked close to the femoral nerve (red circle). The middle panel shows the approach to the disc space with the table rotated, which allows the initial docking to occur farther from the femoral nerve, with more muscle between the retractor and the nerve (blue circle). The bottom panel shows the table returned to the neutral position while maintaining pressure on the retractor to hold its position on the disc space (blue circle). Abbreviation: PTP, prone transpsoas. Used with permission from Barrow Neurological Institute, St. Joseph's Hospital and Medical Center, Phoenix, Arizona. Operative view down the retractor after rotating the table back to the neutral position and final positioning on the L4-5 disc space. Used with permission from Barrow Neurological Institute, St. Joseph's Hospital and Medical Center, Phoenix, Arizona.

Results
Patient (n = 10) Demographic and Clinical Data
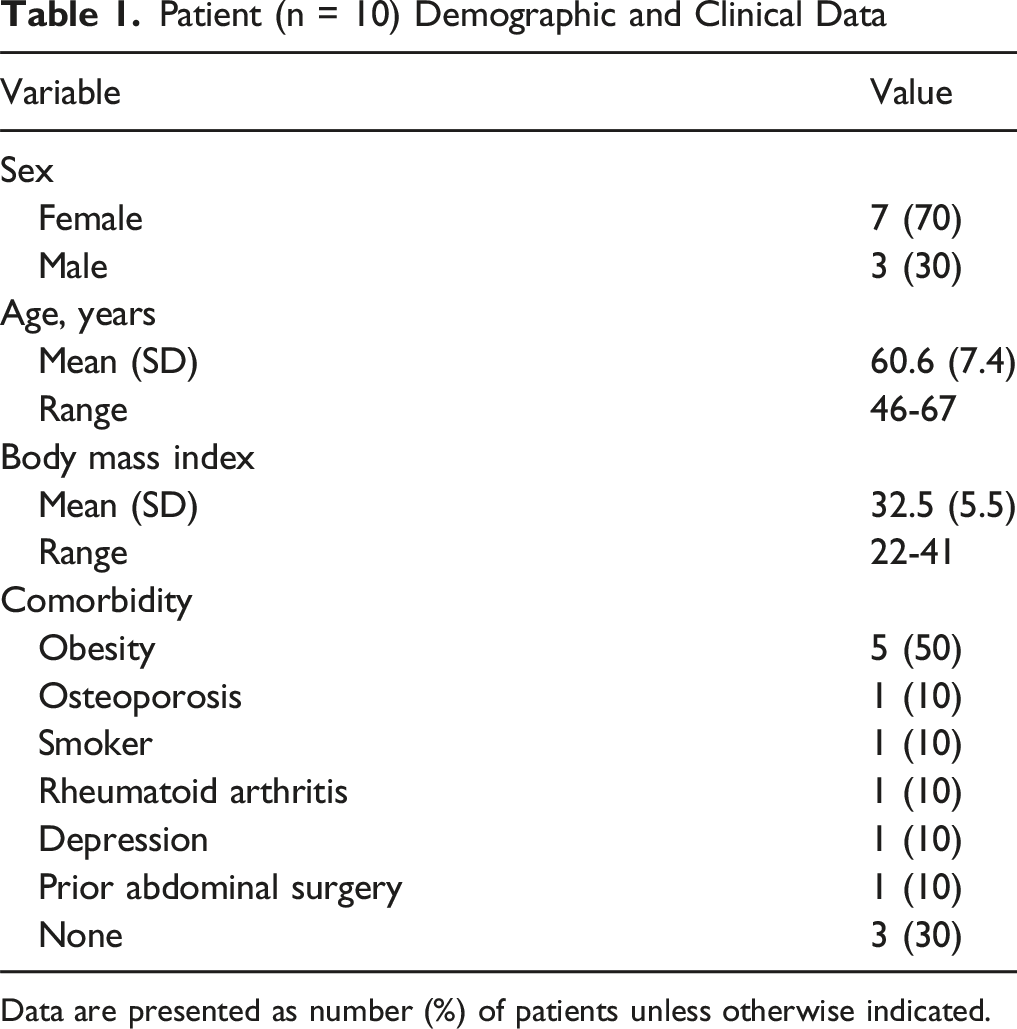
Data are presented as number (%) of patients unless otherwise indicated.
Electromyography Values (mA) of 10 Patients Recorded at Each Location for the Standard Neutral Position and the Oblique Approach Using the Table Rotation Technique
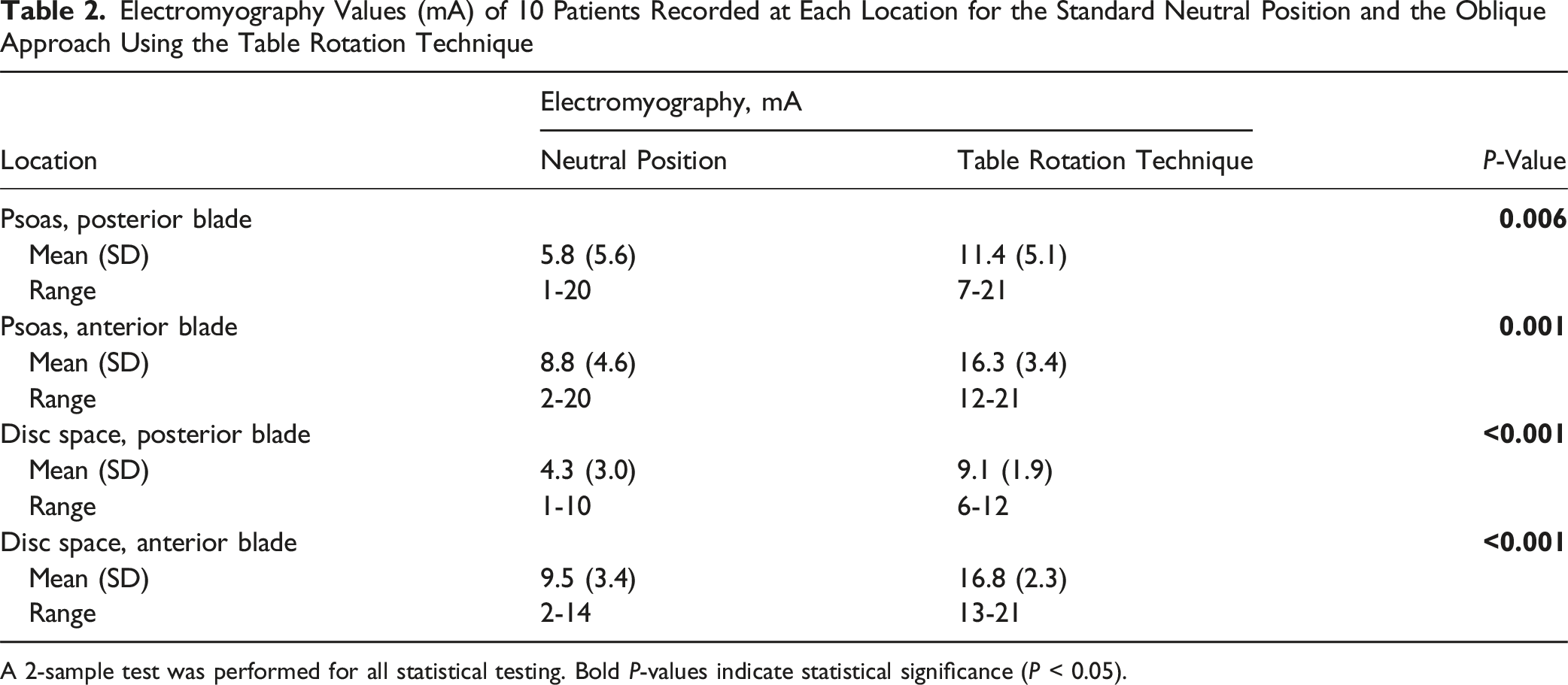
A 2-sample test was performed for all statistical testing. Bold P-values indicate statistical significance (P < 0.05).
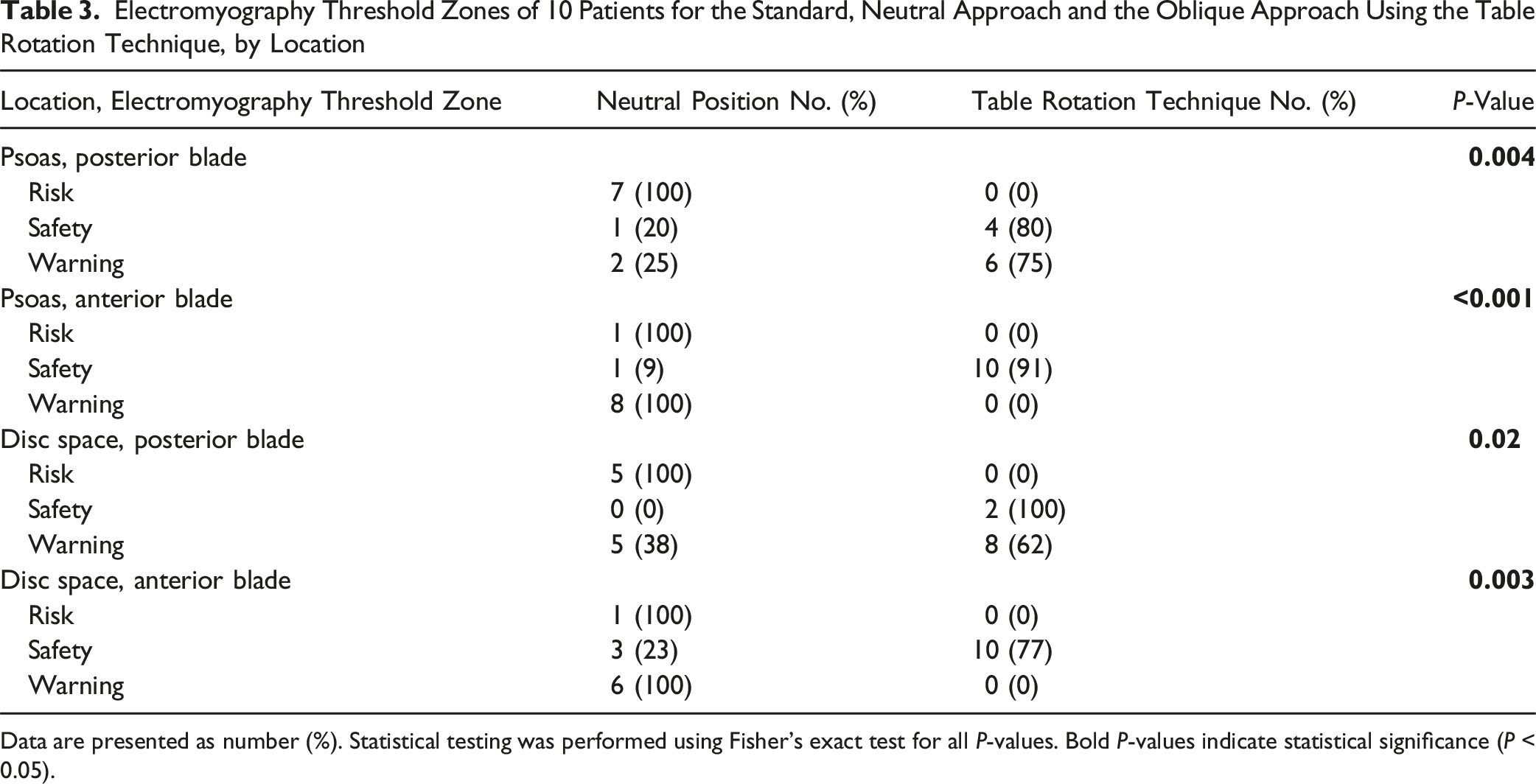
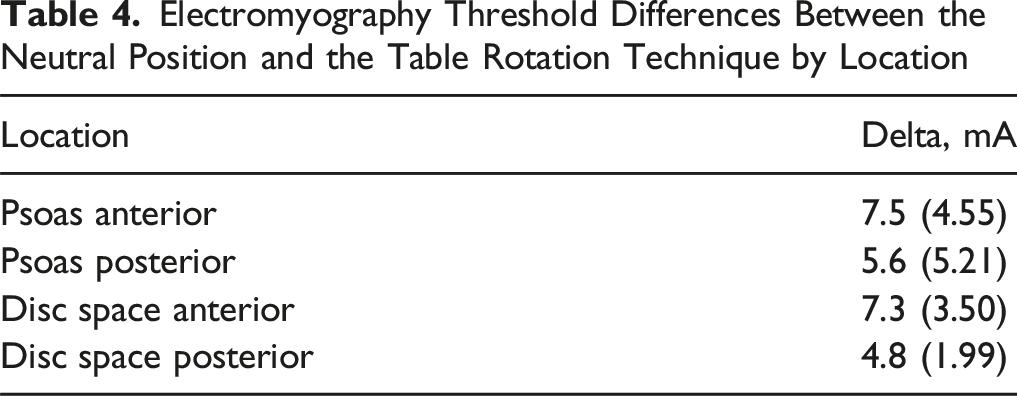
After table rotation, EMG recordings on top of the psoas muscle showed significant improvements. The mean EMG values improved from 5.8 mA to 11.4 mA posteriorly and from 8.8 mA to 16.3 mA anteriorly. The mean psoas EMG values were within the safety zone (>11 mA) for all patients, both anteriorly and posteriorly, after table rotation. Similar improvements were observed for EMG recordings at the disc space, with posterior EMG values improving from 4.3 mA to 9.1 mA and anterior EMG values improving from 9.5 mA to 16.8 mA. The mean posterior EMG values were in the risk zone before table rotation and improved to be in the warning zone after rotation (Figure 4 and Table 3). Dumbbell plot showing the changes in electromyography (EMG) readings for 10 patients before and after table rotation. Used with permission from Barrow Neurological Institute, St. Joseph's Hospital and Medical Center, Phoenix, Arizona. Electromyography Threshold Zones of 10 Patients for the Standard, Neutral Approach and the Oblique Approach Using the Table Rotation Technique, by Location Data are presented as number (%). Statistical testing was performed using Fisher’s exact test for all P-values. Bold P-values indicate statistical significance (P < 0.05).
Electromyography Threshold Differences Between the Neutral Position and the Table Rotation Technique by Location
All 10 patients in the study had a minimum of 6 months of postoperative clinical follow-up. None of the patients had a new weakness, paresthesia, or other neurological deficit indicative of injury to the lumbar plexus immediately postoperatively or during clinical follow-up.
Discussion
The LLIF and PTP techniques are safe and effective for treating many spinal pathologies. However, due to an anterior position of the lumbar plexus and femoral nerve at the L4-5 level, some cases may pose a greater risk of postoperative thigh symptoms and neurological injuries. This study describes a table rotation technique that enables the insertion of dilators and retractors at a greater distance from the femoral nerve than in a neutral table position.
Feasibility of Performing LLIF at L4-5
Several studies have explored the feasibility and safety of LLIF at L4-5. Uribe et al 16 were among the first to investigate the safe working zone (SWZ) for the LLIF technique, showing that the zone was more anterior at the L4-5 level. Additionally, a morphometric study by Guerin et al 17 showed that the SWZ at L4-5 was significantly narrower than the upper levels of the lumbar spine. Their study found that the SWZ at L4-5 included only 38.7% of the endplate, compared to 75.3% at L1-2 or 51.9% at L3-4. 17 Additionally, Garg et al 18 analyzed several factors at the L4-5 level. They showed that the plexus resides in Moro zone III in most cases (60%), with the vena cava or the right common iliac vein residing in Moro zone I in 80% of cases, further reducing the SWZ. When considering other aspects of LLIF at L4-5, such as iliac crest height, the necessary angulation to reach the disc, and the SWZs proposed by Uribe et al, 16 A study suggested that LLIF may be contraindicated in up to 27% of cases. 19 The unique anatomy and challenges associated with LLIF at L4-5 necessitate a careful review of preoperative magnetic resonance and computed tomographic images to assess the vascular and retroperitoneal structures related to the psoas and to avoid injury to these structures during the approach. This careful imaging review is imperative when using the table rotation technique, due to the more anterior-to-posterior angle of approach with the dilator and retractor when the table is rotated (Figure 2).
Preventing Nerve Injury
The most prominent risk of performing LLIF at L4-5 is postoperative quadriceps weakness from retraction injury to the femoral nerve. Injury to the femoral nerve can be caused by either direct or indirect injury. Direct injury occurs with blunt injury or laceration of the nerve during the dissection, retraction, discectomy, or placement of the interbody cage. These injuries are usually more severe and have poorer prognoses than indirect injuries. 20 Intraoperative monitoring with directional EMG can assist in locating the relative position of the femoral nerve to avoid direct injury.20,21 Indirect injury can occur through a combination of compression against the nerve and deformation along the long axis of the nerve with retraction. Multiple studies have indicated that total retraction time during LLIF can predict postoperative weakness.21,22 In vivo animal studies suggest that nerve impairment is a product of both the magnitude and duration of nerve compression. 23 Because of this phenomenon, the proximity of the posterior retractor blade to the femoral nerve likely plays a role in postoperative femoral nerve injury, with increased nerve proximity and retraction time leading to nerve injury.
The introduction of the table rotation technique we describe can help surgeons work around the inherent limitations of the PTP approach at the L4-5 disc space and reduce the overall risk of nerve injury. First, higher EMG thresholds demonstrated with this technique compared to the standard approach indicate that this technique can access the disc space at a safer distance from the plexus. The risk for direct nerve injury during docking of the retractor, discectomy, and interbody cage placement is reduced when the nerves are farther from the posterior blade. Second, the table rotation technique can also help circumvent some of the risk factors for indirect nerve injury. Because this technique allows access to the L4-5 disc space more posteriorly than traditional docking of the retractor, the posterior blade does not need to be retracted as far to ensure access to the optimal position within the disc space. Without the table rotation technique, the retractor is usually docked more anteriorly to avoid the plexus, which requires the posterior blade to be opened more in the posterior direction before placing the posterior shim. This anterior docking position increases the pressure applied to the femoral nerve while it is retracted. Although retraction time was not evaluated in the current study, it was expected to be similar to that of the standard approaches. However, by positioning the retractor in a more favorable location relative to the plexus, with improved EMG thresholds, the technique allows for safer retraction while working in the disc space.
Optimal Positioning of the Interbody Cage
The anterior location of the lumbar plexus and femoral nerve at L4-5, compared to higher lumbar levels, often results in a more anterior placement of the interbody cage at this level. Directional EMG is commonly used as a guide for the safe docking of the retractor and to ensure the retractor blades remain in safe proximity to the traversing nerves. Lower EMG values that fall within the risk zone can bias the placement of the retractor more anteriorly to avoid possible postoperative neuropraxia. This situation can increase the risk of anterior longitudinal ligament (ALL) rupture or vascular injury to the great vessels. Inadvertent rupture of the ALL is a concern when placing the interbody in a more ventral position. 24 Intraoperative rupture may necessitate the placement of a lateral-plating system that can increase the risk of vertebral body fractures or lead to postoperative cage migration if the rupture goes unnoticed intraoperatively. 25 The risk of major vascular complications with the transpsoas approach is remarkably low. 26 Nonetheless, when the surgical corridor is more anterior on the vertebral body, it introduces a greater risk of injury to the great vessels. In addition to the advantage of farther separation of the posterior blade from the lumbar plexus, the table rotation technique can also prevent the need to dock more anteriorly on the vertebral body, given the more favorable EMG value obtained at the initial docking of the retractor.
Table Rotation
This study is one of the first to describe the table rotation technique used to approach the L4-5 disc space in detail. Safely accessing the L4-5 disc space through the transpsoas approach is challenging in the lateral decubitus position and can be exacerbated in the prone position due to anatomical changes in the psoas muscle and lumbar plexus. As seen in the present work, 7 out of 10 patients had risk zone EMG thresholds before table rotation; however, all thresholds significantly improved to the warning zone or safety zone after table rotation.
Limitations
The study’s limitations include its small sample size and retrospective nature. Future studies with larger cohorts and prospective data are needed to assess the effects of the table rotation technique on patient outcomes. Additionally, the small sample size limits the ability to perform statistical testing with subgroup analysis to identify confounding variables. Finally, all procedures were performed by the senior author, which may limit the generalizability of the study.
Conclusion
The table rotation technique facilitated safe access to the L4-5 disc space, which is often difficult to access due to the complex regional anatomy of the psoas muscle and lumbar plexus. The technique increased the distance between the entry point of the retractor and the nerves of the lumbar plexus in our patients, as shown by significantly higher EMG thresholds compared to when the table remained in a neutral position. Our results showed that, in selected patients, the table rotation technique can be safely performed to achieve improved retractor positioning relative to the lumbar plexus, preventing unnecessary injury to the lumbar plexus or femoral nerve.
Footnotes
Acknowledgments
We thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
B.S.L., R.A., and L.P. are consultants for ATEC Spine. The other authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this manuscript.