
Abstract
Study Design
Retrospective Cohort Study.
Objective
Restoration of lumbar lordosis (LL) is a principal objective during spinal fusion procedures, traditionally focusing on achieving an LL within 10° of the pelvic incidence (PI). Recent studies have demonstrated a relatively constant L4-S1 alignment of 35-40° at L4-S1 and at least 15° at L4-5, regardless of PI. Based on these results, this study was created to examine the success rate of achieving a minimum of 15° at L4-5 through two differing prone-based techniques: Prone Lateral (pLLIF) and Trans Foraminal Interbody Fusion (TLIF).
Methods
One hundred patients with a primary single-level L4-5 interbody fusion (50 pLLIF and 50 TLIF) were retrospectively analyzed. Pre and post-operative radiographs were measured to examine the segmental change at each level in the lumbar spine and calculate the success rate for achieving a minimum L4-5 segmental lordosis of 15° at the final follow-up.
Results
The overall success rate of achieving an L4-5 segmental alignment >15° at the final follow-up was 70%. Prone LLIF was significantly more likely than TLIF to achieve this goal, achieving L4-5 > 15° 84% of the time vs TLIFs 56% (P = 0.002). Prone LLIF demonstrated an average L4-5 increase of 5.6 ± 5.9° which was larger than the mean increase for TLIF 0.4 ± 3.8° (P < 0.001). In both techniques, there was an inverse correlation between pre-operative L4-5 angle and L4-5 angle change.
Conclusion
Prone lateral lumbar interbody fusion demonstrates a high success rate for achieving a post-operative L4-5 angle >15° and achieves this at a higher rate than TLIF.
Introduction
Restoration of lumbar lordosis (LL) is essential for treating degenerative spinal disease, as proper realignment has been shown to improve patient’s quality of life and reduce adjacent segment disease.1–5 Historically, lumbar realignment has been based upon achieving an LL within 10° pelvic incidence (LL = PI ± 10°). This is an extremely pragmatic approach in the clinical setting. Recent studies have shown the benefit of focusing on the restoration of each; proximal and distal lumbar lordosis, or even individual lumbar segments.3,6 Previously it was thought that restoring distal lumbar lordosis L4-S1 depended heavily on the PI. (L4-S1 = (2/3) PI). Increasing PI would mean greater L4-S1 lordosis. However, Pesenti et al 7 recently demonstrated a relatively stable L4-S1 of 35-40° regardless of PI.3,7,8 These studies highlight the importance of L4-5 and L5-S1 segmental angles during spinal fusion surgery to achieve proper L4-S1 SA and reported a mean SA angle of 15.8° at the L4-5 segment.
Using the results of these studies, an alignment goal can be established for the distal lumbar segments, aiming for 35-40° of lordosis at L4-S1, with a minimum of 15° at L4-5. Posterior, anterior, and lateral approaches may all be used for the reconstruction of L4-5; each with varying degrees of success reported in the literature.9–18 These papers describe the average segmental alignment change expected with these techniques without analyzing the success of reaching their post-operative alignment goals. Traditional lateral lumbar interbody fusion (LLIF) has shown a consistent pattern of increasing the L4-5 SA by a mean of 2.4°; surgeons performing the entire position in lateral decubitus observed a similar mean of 2.9-4.0° increase.9,11 Single-position prone LLIF (pLLIF) has recently been described, and studies have reported an average increase of 6.6-6.8° at L4-5 SA.11–13 Intuitively, the greater increase in L4-5 SA during pLLIF makes sense. The prone position is the optimal position to induce lordosis in the distal lumbar spine. While the early data on segmental alignment reconstruction at L4-5 performing prone lateral surgery is promising, more research is necessary to delineate if goal segmental alignment at L4-5 is achieved. The aim of this study is to introduce segmental alignment goals as a method for proper sagittal realignment and examine the success rate of achieving a minimum of 15° L4-5 segmental lordosis using two prone-based interbody fusion techniques: transforaminal interbody fusion (TLIF) and prone lateral lumbar interbody fusion.
Materials and Methods
A single-center retrospective cohort was established, including patients who had undergone single-level L4-5 fusions between August 2019 and April 2023. Since the nature of this study was purely retrospective, participation resulted in no more than minimal risk to the patients and informed consent and the need for an IRB were deemed not necessary. Inclusion criteria included any patient who underwent a single level L4-5 pLLIF or TLIF. Patients were excluded if they were multilevel surgery, lost to follow-up, or had previous L4-5 surgery. The goal of the study was to examine the ability to achieve an L4-5 segmental angle >15° through two different single-position prone techniques: pLLIF or TLIF. The choice of pLLIF or TLIF was at the discretion of the operating surgeon based on their surgical preferences. The indications for these procedures included pathologies such as degenerative scoliosis, degenerative disc disease, foraminal/lumbar stenosis, and spondylolisthesis. All operative data, including preoperative diagnosis and patient demographics, were recorded. Patients included if they followed for a minimum of two post-operative appointments. At each appointment, weight-bearing lumbar radiographic imaging was obtained. The preoperative and latest follow-up anterior-posterior (AP) and Lateral films were then measured using Surgimap (Nemaris Inc, New York, NY, USA) to determine the individual alignment of each lumbar segmental angle (SA), pelvic incidence (PI), and lumbar lordosis (LL) on all images. SA was obtained by measuring the Cobb angle from the superior endplate of L4 to the inferior endplate of the L5 body. PI was obtained by taking the angle between the center of the two femoral heads to the midpoint of the sacral endplate and the line perpendicular to the sacral end plate. LL was obtained by measuring the Cobb angle from the sacral endplate to the L1 superior endplate. Subsidence at the final follow-up was defined as a 2 mm or greater penetration of the implant into the vertebral endplate. All measurements were recorded for statistical analysis.
Surgical Techniques
For each pLLIF and TLIF, patients were placed in a traditional prone position with chest and hip pads. Patients undergoing TLIF were placed on a pro-axis table. First, in 20° of kyphosis, to access the disc space and to perform the entire procedure until rod placement. At the time of rod placement, the proaxis bed is placed into 5° of lordosis, and the rods are placed and construct finally tightened. The pLLIF patients were placed on a standard Jackson frame. The hip pads were located at the level of the greater trochanter bilaterally. This would allow access to the L4-5 level during the flank approach. For this study, the success rate of each technique was assessed when using the most common implant for each approach, and a brief outline of each surgical technique is detailed below.
Transforaminal Lumbar Interbody Fusion
A minimally invasive TLIF was conducted via a unilateral pedicle screw-based retractor. Perc screws were placed on the contralateral side via a Wiltse incision. A unilateral inferior and superior facetectomy was conducted to access the disc space. Standard wide discectomy was conducted with intradiscal distraction using paddle sizers. Disc space was filled with bone graft and a turn and rotate style oblique implant of 12°. As mentioned, the proaxis table was then used to create positional lordosis, and rods were locked down. No additional compression was applied over the percutaneous screws.
Prone Lateral Lumbar Interbody Fusion
A minimally invasive pLLIF was conducted via a retroperitoneal approach. Standard docking, discectomy, distraction, and implant placement were conducted as described previously. 14 A wide annular/disc release was pursued to accommodate a 22 mm wide 15° implant 95% of the time. In this series, the ALL was maintained in all patients. Percutaneous screws were placed via standard Wiltse incision. No additional screw-based compression was pursued in these patients.
Statistical Analysis
A comparison of the spinal realignment capacity of pLLIF and TLIF was established by comparing preoperative and final follow-up measurements. Initially, preoperative segmental angle measurements were subjected to a Kolmogorov-Smirnov test. Next, with the threshold for significance set at P = 0.05, a 2-way ANOVA was performed with multivariate analysis of the variables. Further analysis of the L4-5 segmental angle was completed to examine the change in the L4-5 angle from pre-operation to follow-up based on the preoperative L4-5 angle. For this analysis, the patients were grouped based upon preoperative angle into <10°, 10-15°, 15-20°, or >20° with angles falling on exactly 15 being grouped into the 15-20° group. The change post-operatively was then recorded for both pLLIF and TLIF and analyzed in the same manner as above. Initially, a multiple linear regression model was used to assess the association between clinical, demographic, and operative variables and change in L4-5 using Pearson’s correlation coefficients. The remainder of the analysis was conducted using linear regression, logistic regression, or Chi-Square analysis, depending on the presence of continuous or discrete variables. All tests were two-sided, and P ≤ 0.05 was considered statistically significant for every test, and all statistical computations were performed using GraphPad Prism (v10.1) (GraphPad Software, La Jolla, CA, USA).
Results
Cohort Characteristics
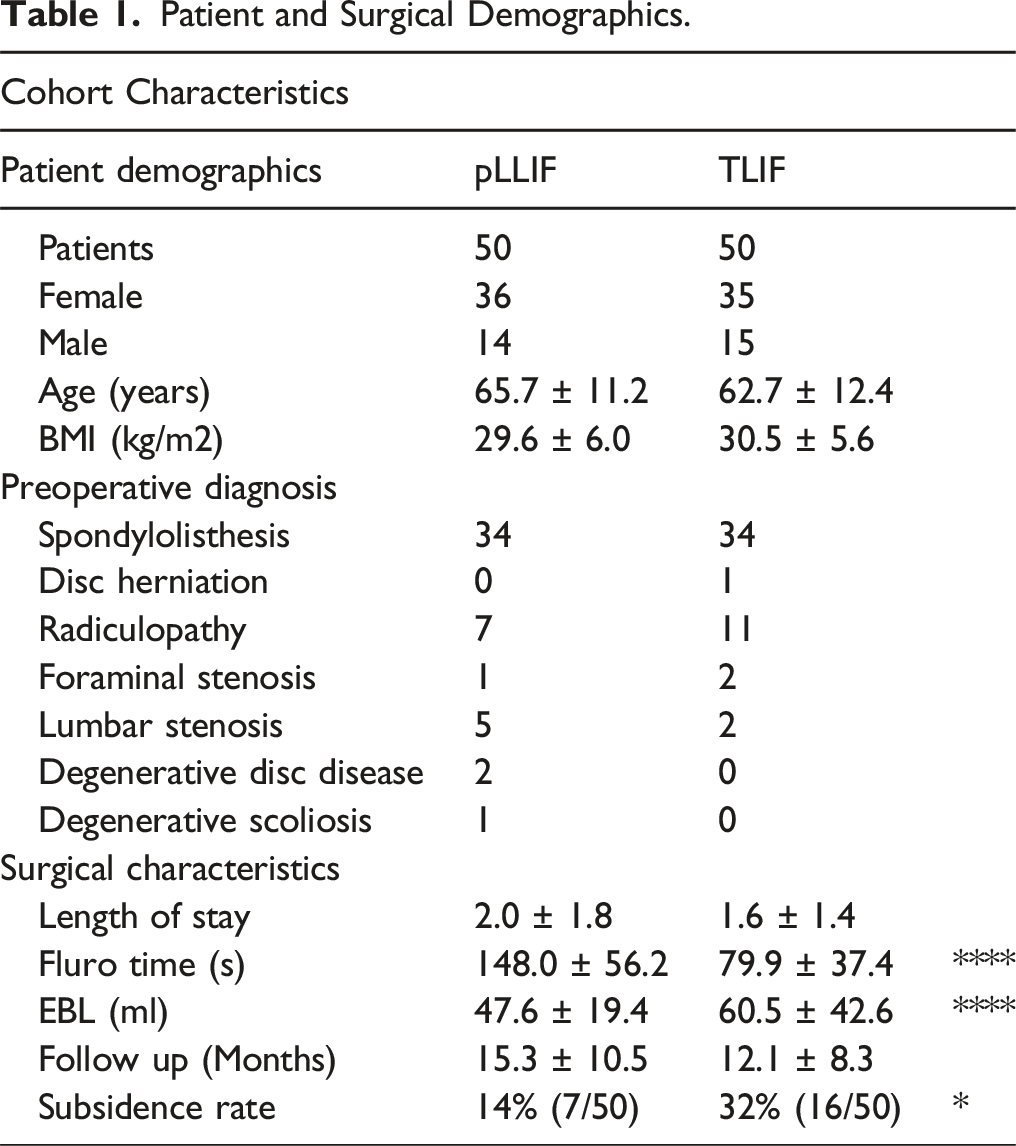
Patient and Surgical Demographics.
Radiographic Measurements of Sagittal Spinopelvic Alignment
Radiographic Measurements of Preoperative Films and Final Post-operative Films, Represented as Mean ± Standard Deviation. The P Value for pLLIF vs TLIF is Signified by a *, While the P Value for Pre-operation vs Final Follow-Up is Signified With a #.
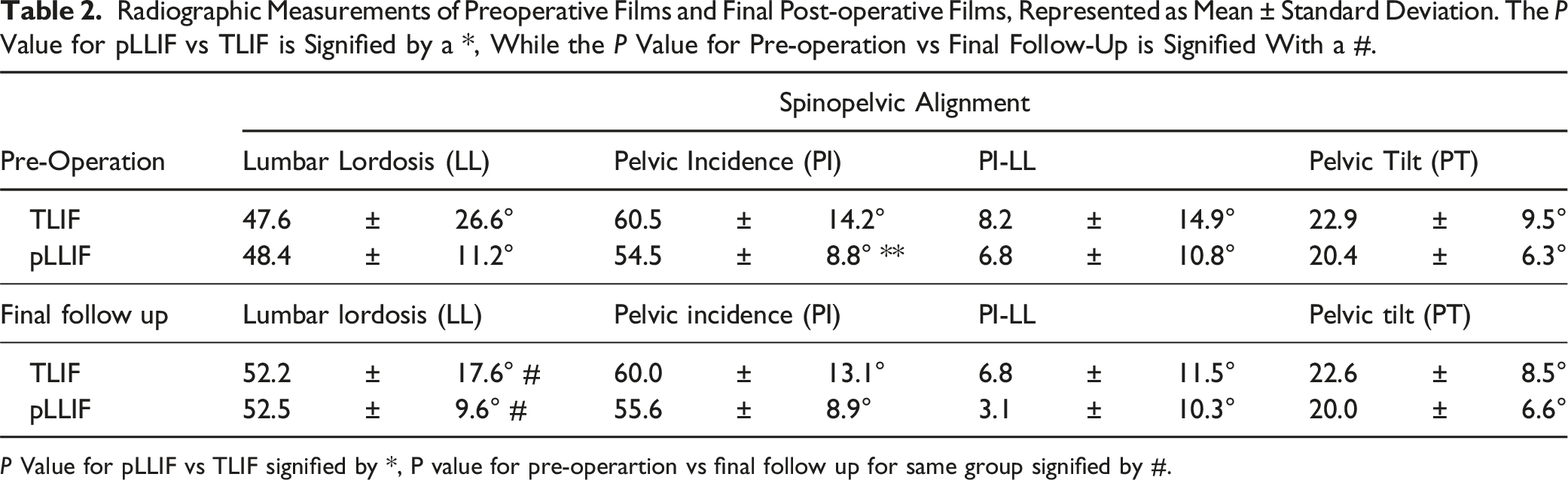
P Value for pLLIF vs TLIF signified by *, P value for pre-operartion vs final follow up for same group signified by #.
Radiographic Segmental Angle Analysis
Individual Segmental Angle Radiographic Measurements of the Preoperative Films and Final Post-operative Films, Represented as Mean ± Standard Deviation. The P Value for pLLIF vs TLIF is Signified by a *, While the P Value for Pre-operation vs Final Follow-Up is by a #.
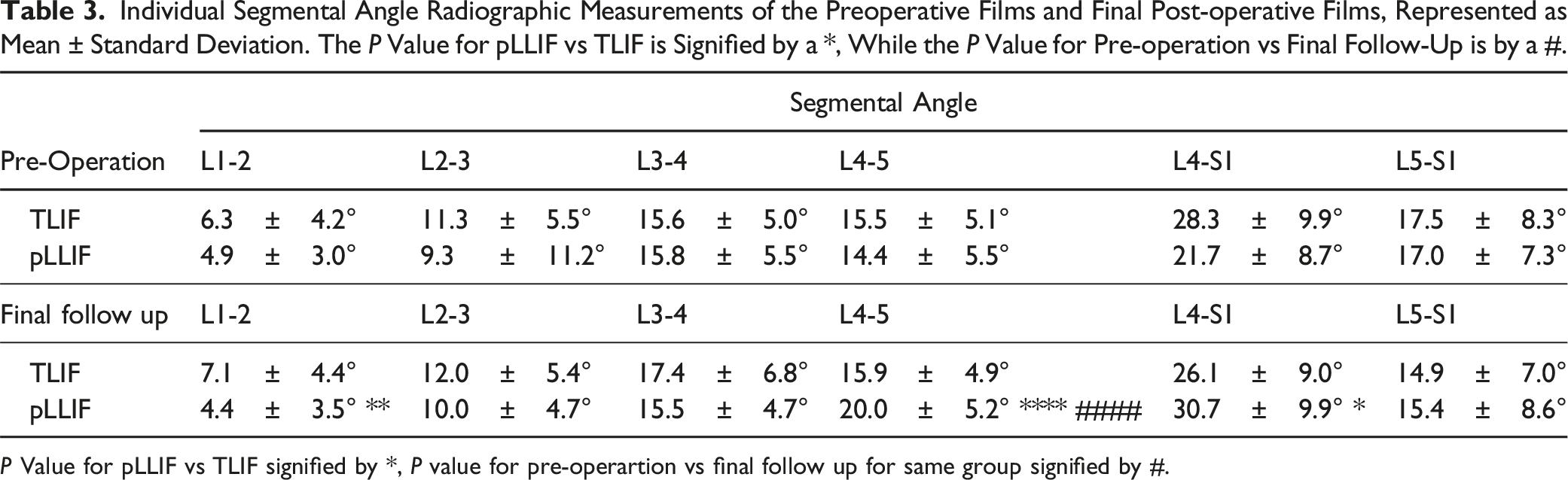
P Value for pLLIF vs TLIF signified by *, P value for pre-operartion vs final follow up for same group signified by #.
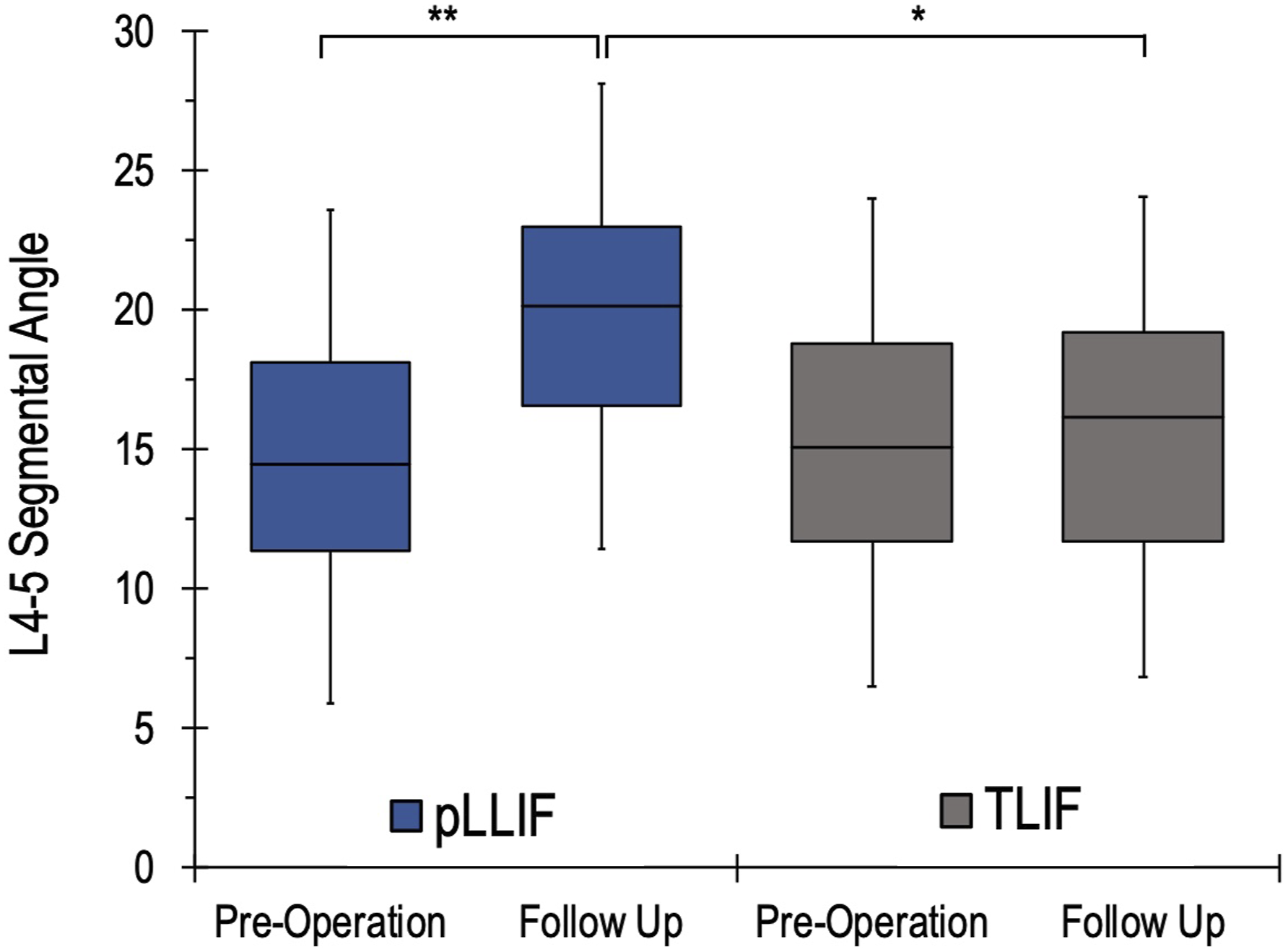
L4-5 segmental angle measurements of the preoperative films and final post-operative films for both pLLIF and TLIF groups. For each group, the box plot represents the 25th quartile, median, and 75th quartile segmental angles, and the bars demonstrate the standard deviation.
Understanding the L4-5 Segmental Angle Change
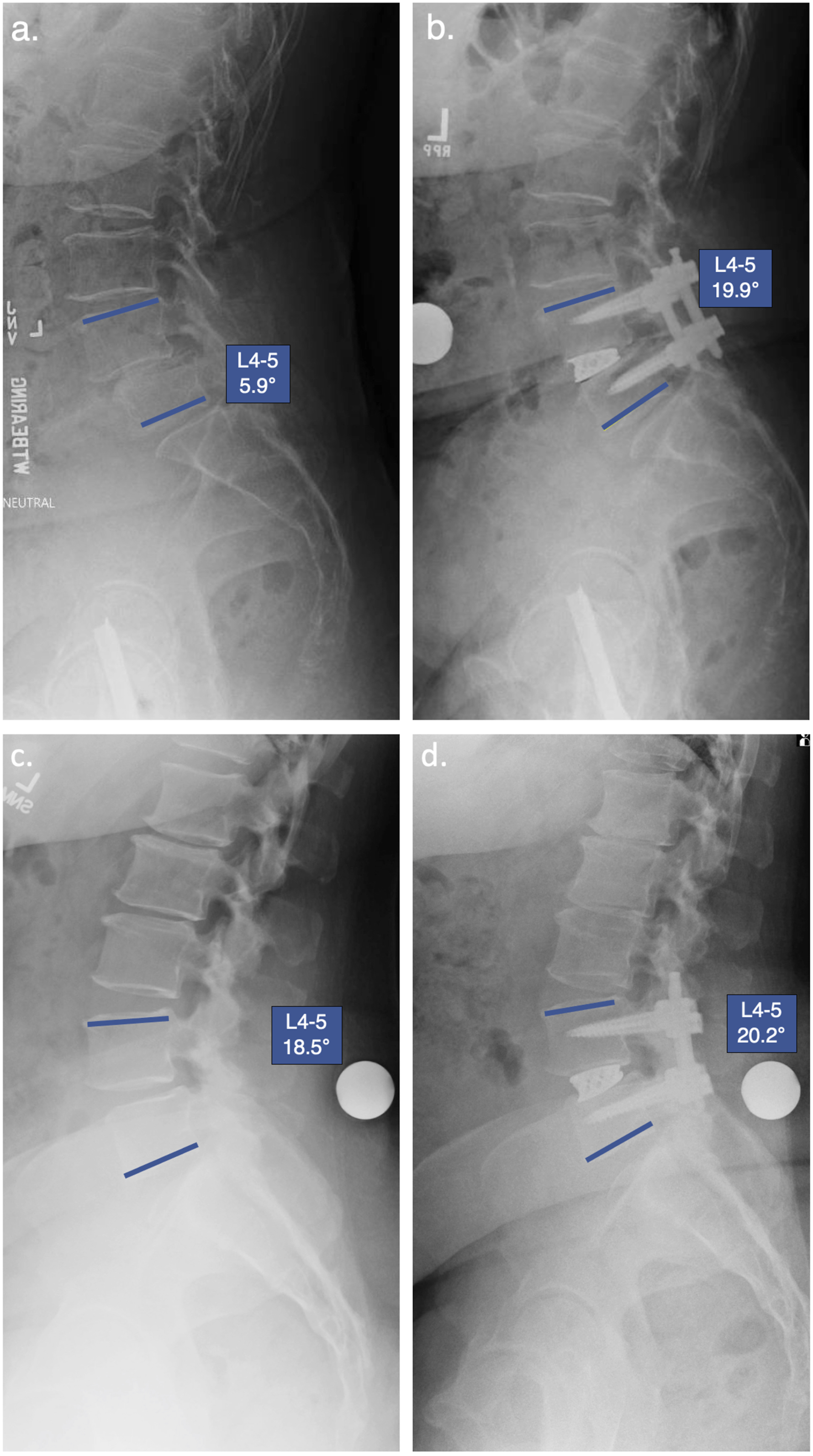
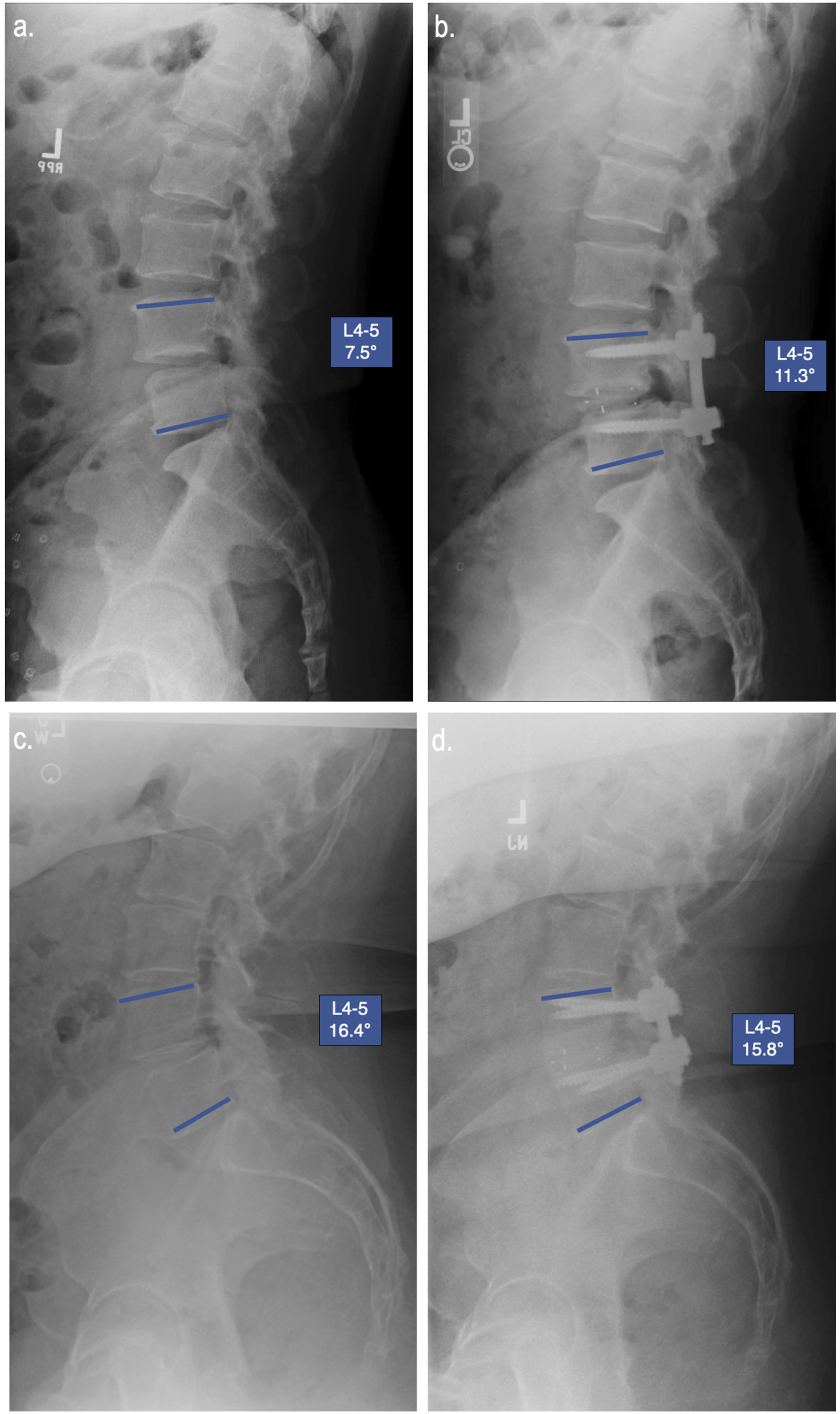
Linear regression analysis of pLLIF and TLIF groups revealed that there was no strong correlation between final L4-5 angle and age, BMI, EBL, fluoroscopy time, gender, pain scores, preoperative diagnosis, or subsidence. The change in L4-5 segmental angle was significantly higher for pLLIF compared to TLIF (5.6 ± 5.9° vs 0.4 ± 3.8° respectively, P < 0.001). In an effort to better understand the capacity of pLLIF and TLIF for adjusting the L4-5 segmental angle, a secondary analysis of the L4-5 angle was conducted. Patients were grouped based on their pre-operative L4-5 segmental angle into <10°, 10-14.9°, 15-19.9° and >20°, with the sample size of each group averaging 11.9 ± 6.6 (range 6-22). The L4-5 change at the final follow-up was then compared for each group (Figure 2). For patients with a pre-operative L4-5 segmental angle below 10°, pLLIF demonstrated a significantly higher increase than TLIF at the final follow-up (12.3 ± 6.1° vs 3.4 ± 3.1° respectively, P < 0.001). For patients with a pre-operative L4-5 segmental angle between 10-14.9°, pLLIF demonstrated a significantly higher increase than TLIF at the final follow-up (5.5 ± 4.5° vs 0.5 ± 3.8° respectively, P = 0.005). For patients with a pre-operative L4-5 segmental angle between 15-20°, pLLIF demonstrated a significantly higher increase than TLIF at the final follow-up (3.7 ± 5.8° vs 0.3 ± 1.6° respectively, P = 0.026). At L4-5 preoperative angles >20°, pLLIF provides a small increase in segmental angle (1.9 ± 2.3°) while TLIF leads to a decrease in segmental angle (−2.3 ± 2.5°); these results were significantly different (P = 0.005). When examining all of the patients with >10° L4-5 pre-operative angle, there was a significant difference in the post-operative change caused by pLLIF vs TLIF (P = <0.001). For these patients, pLLIF provided an average increase of 4.1 ± 4.7°, while TLIF provided an average increase of 0.0 ± 3.7°. An example of the change observed with pLLIF and TLIF for a patient with <10° and >10° preoperative L4-5 segmental angle can be seen in Figures 3 and 4, respectively. Subgroup analysis of patients with implant subsidence revealed a post-operative average change of 3.3 ± 6.3° for pLLIF and 0.4 ± 3.3° for TLIF, although neither of these were statistically significant from the non-subsidence groups (P = 0.164 and 0.819 respectively). L4-5 Segmental angle change for pLLIF (blue) and TLIF (grey) based on pre-operative L4-5 segmental angle. Statistical significance for pLLIF vs TLIF designated by *. (A) Example of a patient with a pre-operative L4-5 segmental angle <10° and final follow-up L4-5 angle following L4-5 pLLIF (B). (C) Example of a patient with a pre-operative L4-5 segmental angle >10° and final follow-up L4-5 angle following L4-5 pLLIF (D). (A) Example of a patient with a pre-operative L4-5 segmental angle <10° and final follow-up L4-5 angle following L4-5 TLIF (B). (C) Example of a patient with a pre-operative L4-5 segmental angle >10° and final follow-up L4-5 angle following L4-5 TLIF (D).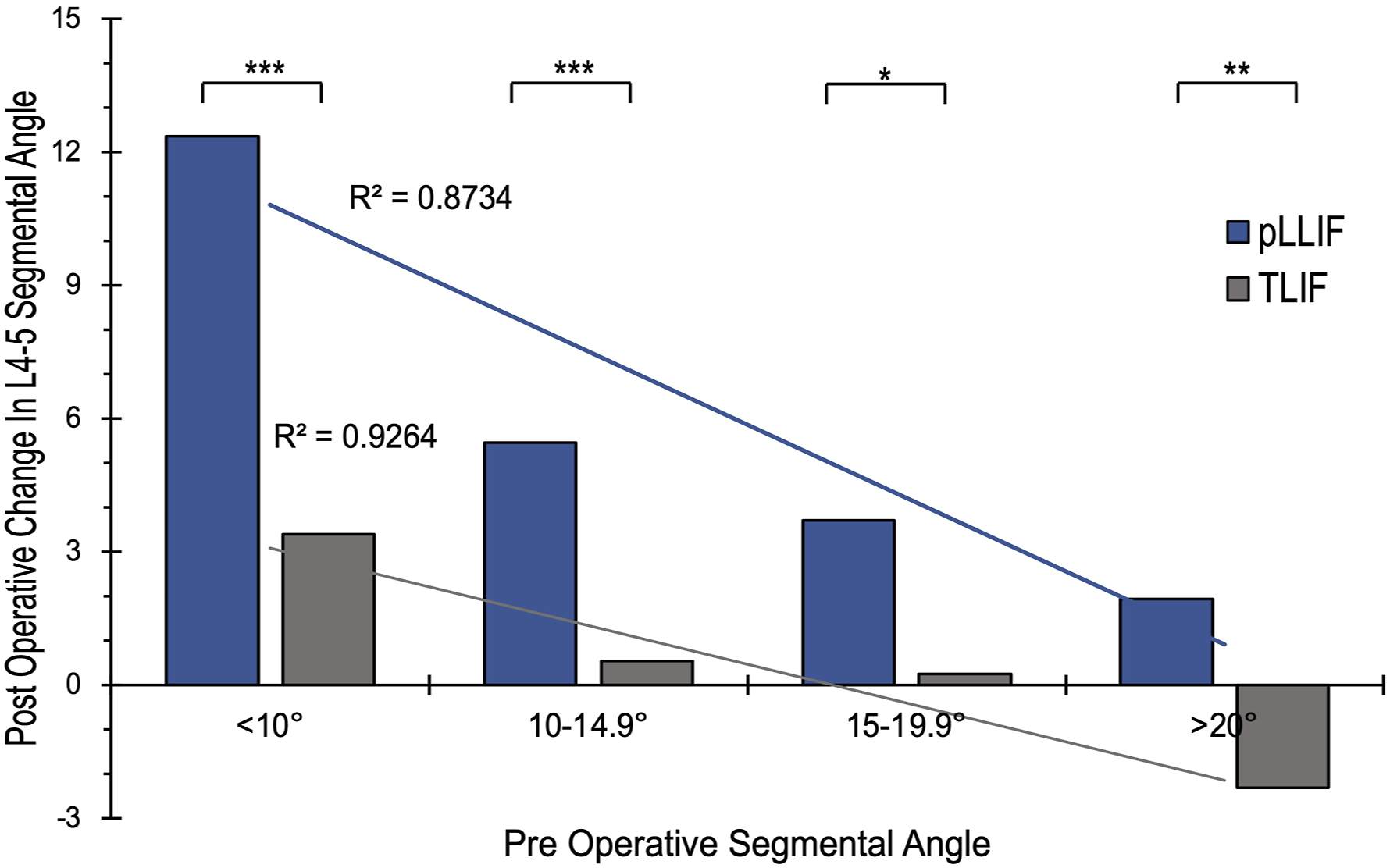
Segmental Alignment Goals
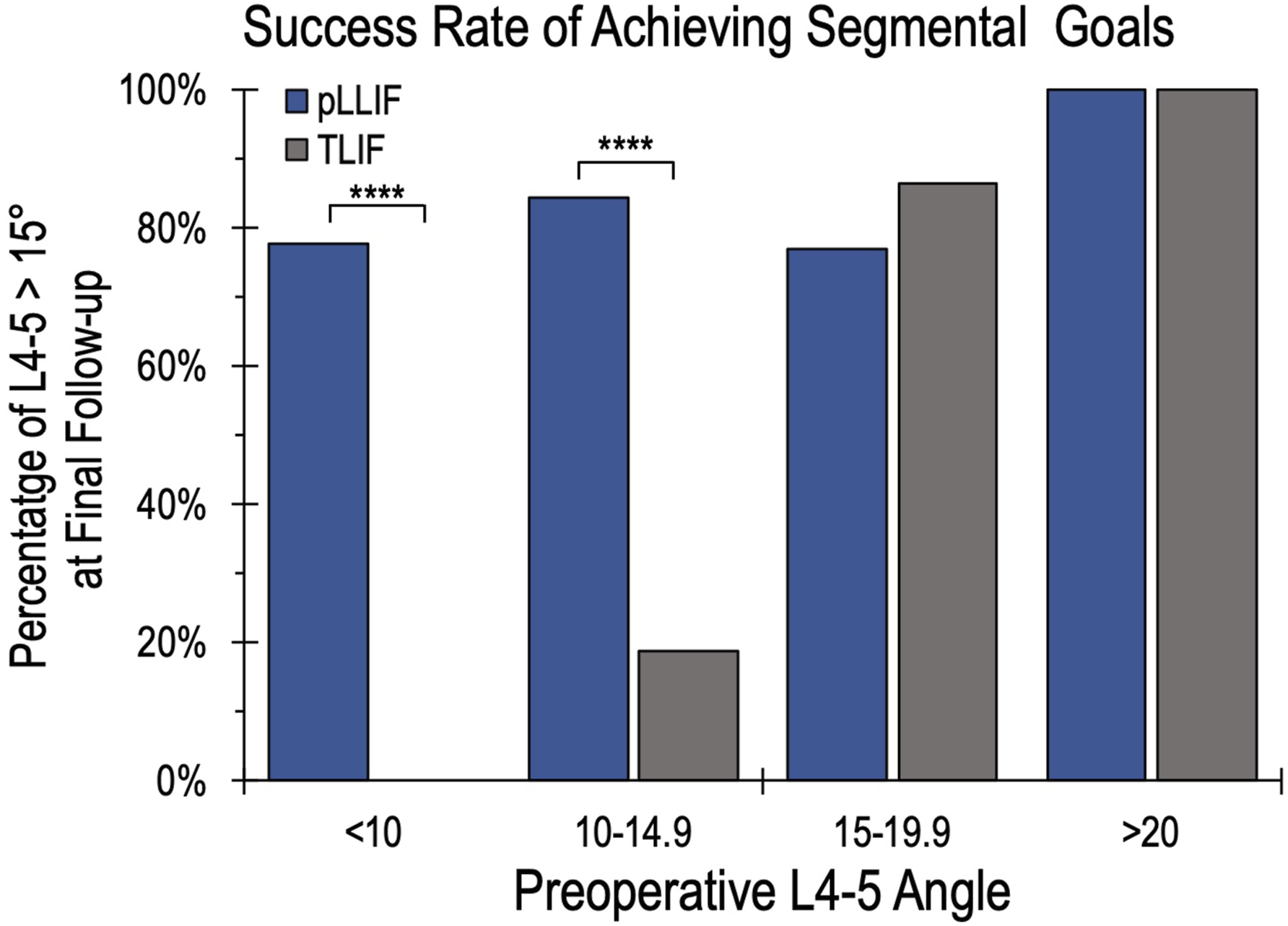
The goal of this study was to examine the ability of pLLIF and TLIF to achieve a goal segmental angle of at least 15°. For the entire cohort, the overall success rate of achieving an L4-5 segmental angle was 70%. pLLIF was significantly more likely to achieve this segmental angle goal compared to TLIF, successfully achieving it at a rate of 84% vs 56% respectively (P = 0.002). This data was further divided into subgroups based on implant subsidence (Figure 5). In the group without implant subsidence, pLLIF demonstrated a significantly higher rate of achieving the L4-5 segmental angle goal than TLIF (88.4% vs 61.8%, respectively, P = 0.011). There was no statistical difference between pLLIF or TLIF for achieving L4-5 alignment goals when implant subsidence was present (57.1% vs 43.8% respectively, P = 0.575). Implant subsidence did not significantly change the rate of achieving L4-5 segmental alignment goals for either procedure (pLLIF n = 7, P = 0.408; TLIF, n = 16, P = 0.252, n = 16). Lastly, the success rate of each technique was examined based on the preoperative L4-5 segmental angle (Figure 6). For patients with <10° pre-operatively, pLLIF achieved a post-operative L4-5 angle >15° 77.8% of the time, compared to 0% in the TLIF group (P < 0.001). pLLIF also demonstrated a significantly higher rate than TLIF in patients with 10-14.9° pre-operatively (84.2% vs 18.8%, P < 0.001). For patients who were above 15° pre-operatively, there was no difference between pLLIF and TLIF for achieving a segmental angle >15° at the final follow-up. A bar graph demonstrating the success rate of achieving an L4-5 segmental angle of >15° at the final follow-up for pLLIF vs TLIF. With subgroup analysis showing the success rates in the presence of implant subsidence. The success rate of achieving a minimum L4-5 angle of 15° for pLLIF (blue) and TLIF (grey) based on pre-operative L4-5 segmental angle. Statistical significance for pLLIF vs TLIF designated by *.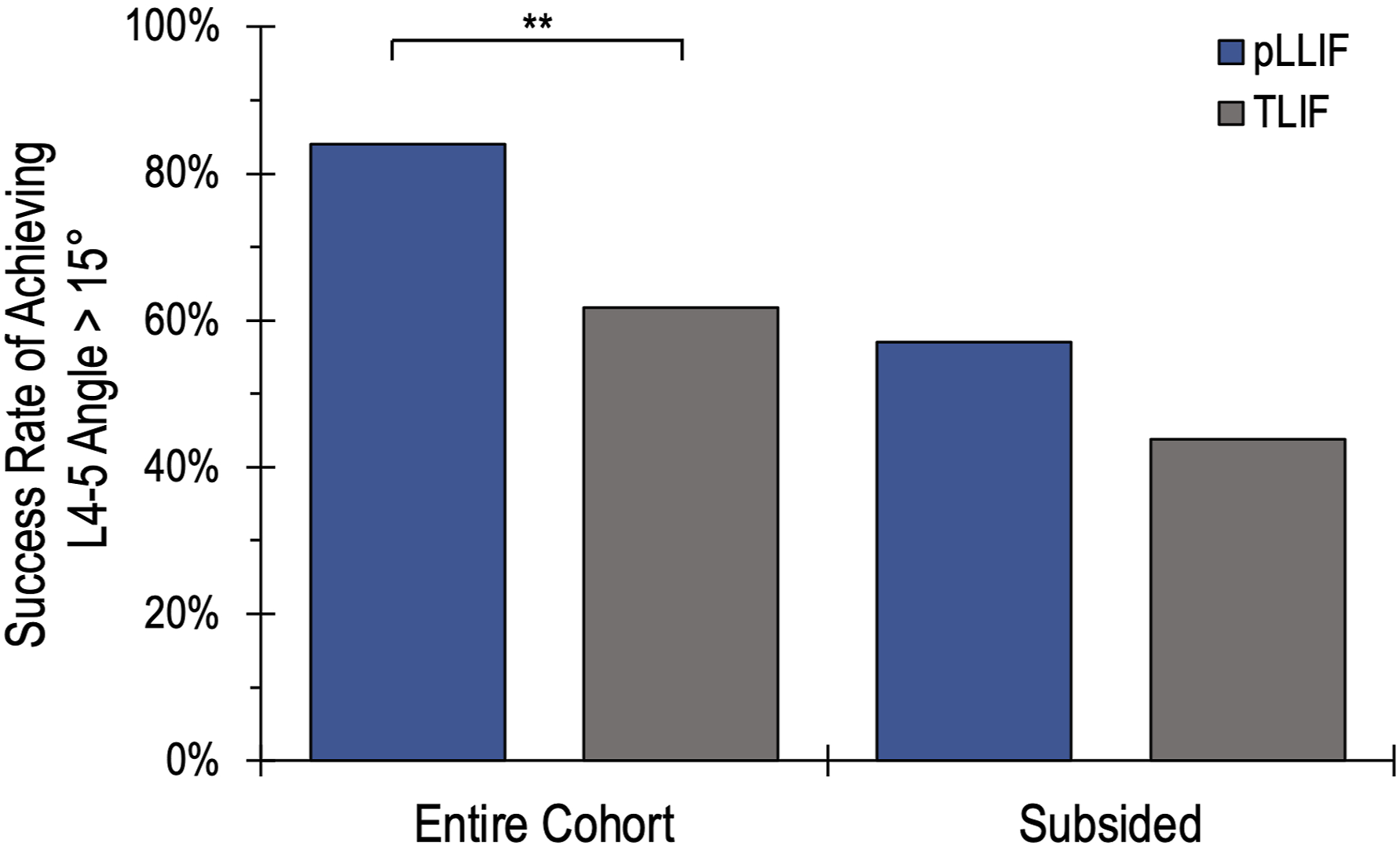
Discussion
Distribution of lumbar lordosis (LL) is an important concept to consider when treating single-level degenerative spinal disease. The inability to correct LL and realign segmental angles (SA) results in an increased risk of adjacent segment disease and reoperation. 8 Roussouly et al 1 proposed a classification system based on Pelvic Incidence (PI)) and the apex of lordosis . This data has since provided exceptional insight into the physiological alignment of the lumbar spine and paved the way for further research on the influence of pelvic morphology on LL distribution. Pesenti et al 8 sought to further investigate this relationship and observed a relatively constant L4-S1 SA of 36° ± 8.1° across patients with PI’s of <45°, 45°-60°, and >60°. Pesenti also showed an average physiological segmental lordosis of 15.8° ± 4.4° at L4-L5 . Using these studies to establish our goal criteria, this study introduces segmental angle goals as a new concept for properly realigning the distal lumbar spine. This study was designed to examine the rate at which we achieve a minimum L4-5 lordosis of >15° in each patient and to identify which prone-based technique is more successful at achieving this goal.
The results of this study demonstrated a 70% success rate at achieving a goal segmental angle >15° at L4-5 for the entire cohort. Each patient was placed in the prone position for either a pLLIF or TLIF procedure. Prone positioning with the hips and knees extended on a Jackson frame is a powerful position to induce distal lumbar lordosis. For the pLLIF, the hip support is placed 2-4 inches further distally than during TLIF. This further induces passive distal lumbar lordosis. 15 and may allow for a contributing factor to higher segmental change. pLLIF demonstrated a higher success rate than TLIF at achieving an L4-5 angle >15° in 84% of cases, compared to 56% for the TLIF group. This disparity in success rates appears to be driven by the segmental angle increase influenced by each technique. pLLIF demonstrated an average L4-5 segmental angle increase of 5.7 ± 6.0°, which was significantly higher than the TLIF average increase of 0.5 ± 3.8°. The favorable segmental angle increase during prone lateral has been previously observed.11–13
Pre-operative L4-5 segmental angle was an influential factor in the observed increase from either procedure. The segmental change from a pLLIF is inversely correlated with the pre-operative L4-5 angle. Patients with pre-operative L4-5 angle <10° experienced an average increase of 12.3 ± 6.1° from a pLLIF, while those >10° saw an average increase of 4.1 ± 4.7°. This was not the same for TLIF, as it was observed to have a significantly lower change for both groups. While those with <10° pre-operatively experienced an increase of 3.4 ± 3.1°, those with pre-operative angles >10° saw little change, averaging 0.0 ± 3.7°. There is a general opinion that TLIF is a kyphogenic procedure. 16 However, this subgroup analysis demonstrates that TLIF is capable of improving segmental angle in patients with <10° of pre-operative segmental alignment. Due to the small changes in segmental angle from TLIF, the pre-operative L4-5 segmental angle was a large factor in the success rate of achieving a minimum L4-5 angle of 15°. While TLIF proved to increase lordosis in patients with <10° pre-operatively, zero of them were able to reach goal alignment of 15°. For patients whose preoperative angles were 10-14.9°, TLIF was only able to achieve goal alignment 18% of the time. This was not the case for pLLIF, as it demonstrated a success rate of 76% or higher for all of the pre-operative angle subgroups. Both TLIF and pLLIF had high rates of maintaining goal alignment when the pre-operative angle was above 15°.
There was a significantly lower rate of implant subsidence in the pLLIF group compared to TLIF. However, the differences in achieving goal alignment in patients with subsidence vs those without subsidence were not statistically significant. Intuitively, a subsided implant, whether LLIF or TLIF, would lead to a decrease in segmental lordosis. The current study is underpowered to demonstrate a difference in the subsidence vs the non-subsided group. This study finds that pLLIF subsides at a lower rate than the TLIF group. The larger implant sitting across the apophyseal ring with maintained posterior elements is likely protective over post-operative subsidence. This study also demonstrates that pLLIF is a more reliable option for achieving the L4-5 segmental angle goal than TLIF, even in the setting of a subsided graft. A systematic review by Parisien et al 17 , in 2022 examined the subsidence rates of different spinal fusion techniques, reporting a varying subsidence rate for TLIF between 0%–51.2%, with a median subsidence rate of 21.4% from the 14 different studies . This is in line with our observed TLIF subsidence rate of 32%. The same is true for our pLLIF subsidence rate of 14%, as a recent systematic review by Batheja et al 18 reported an LLIF subsidence rate in 22.4% of patients after compiling the results from 9 different studies.
While the pLLIF demonstrates a high success rate in this study and outperforms TLIF for average segmental increase, it is important to consider how other fusion approaches change the SA.12,19–26 Other studies have demonstrated similar results for TLIF, showing an average L4-5 segmental angle increase of 1-1.8° with a static implant and 1-5° using an expandable implant through a minimally invasive approach.18,27,28 Hong et al observed a greater segmental gain (6.5°; 15° implant) utilizing an open TLIF with bilateral facetectomies and a subtotal laminectomy. 29 The technique in this study involves a unilateral approach and may not create enough of a release to compress posteriorly. Introducing greater posterior bony release does destabilize the segment further to achieve alignment goals, potentially increasing the rate of subsidence or reducing fusion rates. Another disadvantage of the TLIF approach is the inability to release the lateral annulus bilaterally. The wide circumferential release is typically easier to achieve during the lateral interbody technique. Additionally, the ability to maintain distraction of the disc space with the longer and wider lateral implant is more reliable than the smaller interbody footprint that TLIF offers.
Limitations
The design of this study is a limitation as it is a retrospective review of a single center’s cases, which could introduce some sampling bias. This study only examines two prone-based techniques, which does not allow us to make direct comparisons to other fusion techniques. A multi-center study is underway to compare the segmental angle goal principle based on ALIF, TLIF, LLIF, and pLLIF. This will further identify the success rate of each type, the segmental increases, as well as if there is any statistical difference between the outcomes of the fusion procedures. In addition, and most importantly, there are specific reasons a TLIF or a pLLIF procedure may be performed. These include but are not limited to, the following: surgeon training/comfort, site of service, need for direct posterior decompression, and patient neurovascular anatomy at L4-5. Nevertheless, the study was an objective measure of radiographic segmental alignment findings after the pLLIF vs unilateral MIS pedicle screw-based TLIF technique.
Conclusion
This study introduces segmental angle goals for proper realignment of the distal lumbar spine. Prone lateral interbody fusion has a higher success rate of achieving goal realignment and induces a larger average L4-5 segmental angle change than TLIF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (August,2024):
pLLIF and TLIF labels in Table 3 were inverted, and have now been corrected to display TLIF above pLLIF in both instances in the left column.