
Abstract
Study Design
Retrospective case series.
Objective
The single-position prone lateral lumbar interbody fusion (P-LLIF), which eliminates the need to change patient decubitus during the procedure, represents a modification of the traditional lateral lumbar interbody fusion (LLIF). This pioneering study aims to investigate the positional shifts of retroperitoneal organs and changes in lumbar lordosis angle across different decubitus, providing novel insights into the biomechanics of LLIF.
Methods
Eighteen patients scheduled for LLIF were included. CT scans were performed in 3 positions: prone, right lateral, and oblique decubitus. Measurements included the anatomical positions of the psoas major, abdominal aorta, left common iliac artery, and left kidney at intervertebral disc levels, as well as changes in lumbar lordosis angle across the 3 positions.
Results
In the prone decubitus compared to the lateral decubitus: The thickness of the psoas major increased by 4.07 ± 3.41 mm. The abdominal aorta shifted laterally by 2.29 ± 2.79 mm. The left common iliac artery shifted laterally by 1.98 ± 3.54 mm. The kidney moved anteriorly by 6.97 ± 5.84 mm. The lumbar lordosis angle increased by 7.73 ± 3.76°. In the oblique decubitus compared to the lateral decubitus: The thickness of the psoas major increased by 3.14 ± 3.36 mm. The abdominal aorta shifted laterally by 1.59 ± 2.82 mm. The left common iliac artery shifted laterally by 2.45 ± 4.51 mm. The kidney moved anteriorly by 3.92 ± 4.70 mm. The lumbar lordosis angle increased by 3.04 ± 3.55°.
Conclusion
P-LLIF induces significant positional changes in retroperitoneal organs and increases lumbar lordosis angle compared to traditional LLIF. These findings offer critical insights for preoperative planning and underscore the importance of optimizing safety protocols in P-LLIF procedures.
Keywords
Introduction
Lateral lumbar interbody fusion (LLIF) stands as a prevalent minimally invasive surgical approach for the management of lumbar degenerative disorders. 1 Traditional LLIF necessitates patient repositioning from lateral to prone decubitus for intervertebral fusion and posterior instrumentation, respectively. 2 This procedure prolongs surgery and anesthesia time and increases the number of intraoperative fluoroscopies to some extent. In 2020, Lamartina et al 3 first introduced the single-position prone lateral lumbar interbody fusion (P-LLIF), 2 a technique that maintains the patient’s position throughout the procedure, thereby enhancing surgical efficiency and safety. P-LLIF has many theoretical advantages, including reduced surgery time, improved operating room efficiency, 3 lower risk of lumbar plexus nerve injury,4-6 increased lumbar curvature, and a more accessible retroperitoneal approach. 7
During single-position prone LLIF, the operating table needs to be rotated to the opposite side (5-30°)8-12 to adapt to the surgeon’s line of sight and facilitate the operation. The rotation of the operating table allows the patient to switch positions between prone decubitus and oblique decubitus, and previous studies were based on changes in the position of retroperitoneal organs in healthy individuals in prone, left lateral, and supine decubitus. 13 In actual clinical practice, the left-sided lumbar surgical approach with the patient in a right lateral decubitus is often utilized. This is because the inferior vena cava is located on the right front of the vertebral body. An approach from the right side may risk damaging the inferior vena cava, which, if injured, can be very difficult to repair.14,15 Additionally, the surgical window for the left-sided approach is larger than that for the right side. 16 Currently, there are no reports on the positional changes of retroperitoneal organs in the oblique and right lateral decubitus.
For the first time, we used patients scheduled for LLIF surgery as research subjects and performed CT measurements in 3 different decubitus: prone, right lateral, and oblique (30°), ensuring that the abdomen was freely hanging to best replicate the patient’s intraoperative state. We analyzed the positional changes of retroperitoneal organs such as the psoas major, blood vessels, and left kidneys, as well as the lumbar lordosis angle in the 3 different decubitus. Accurately mastering the positional changes of retroperitoneal organs in different positions is crucial for the selection of surgical approach and surgical safety.
Methods
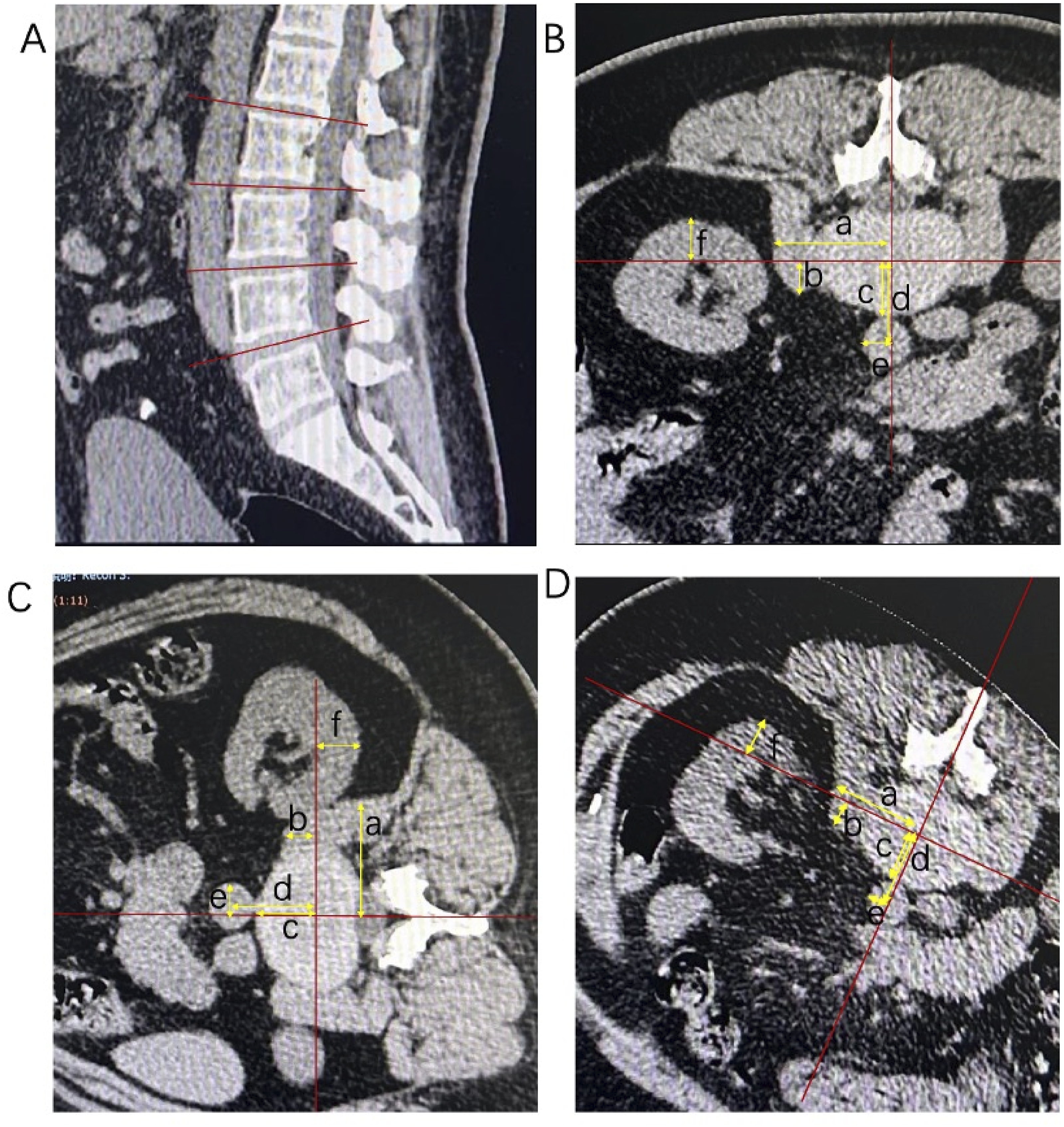
This prospective investigation, conducted in a tertiary care facility, amassed anatomical imaging data from patients scheduled for LLIF surgery. A cohort of 18 patients (mean age: 54 years) underwent 3 CT scans—prone, right lateral, and oblique decubitus—calibrated to replicate intraoperative conditions. Informed consent was obtained from all patients. In the prone decubitus, small pillows were placed under the chest and pelvis to allow the abdomen to hang freely, with a slight flexion of the hip joints (Figure 1(A, B)); in the lateral decubitus, a small pillow was placed under the waist, with a slight flexion of the hip joints (Figure 1(C, D)); in the oblique decubitus, patients were positioned on a pre-prepared inclined mold, with small pillows placed under the chest and pelvis to allow the abdomen to hang freely, and a slight flexion of the hip joints (Figure 1(E, F)). To ensure the accuracy of the anatomical positions, the cross-sectional images selected for measurement were parallel to the intervertebral space and passed through the midpoint of the intervertebral disc (Figure 2). Two baselines were first set as reference lines for measurement. The coronal line: parallel to the intervertebral space, passing through the center of the intervertebral disc and parallel to the anterior and posterior edges of the vertebral body. The sagittal line: parallel to the intervertebral space, passing through the center of the intervertebral disc and perpendicular to the anterior and posterior edges of the vertebral body. Both the coronal and sagittal lines pass through the center of the intervertebral disc and are perpendicular to each other. The midpoint of an organ is defined as the intersection of the greatest transverse diameter parallel to the coronal line and the greatest longitudinal diameter parallel to the sagittal line. The outer edge of the psoas major muscle: at the disc level, the vertical distance from the outermost edge of the psoas major muscle to the sagittal line; the anterior edge of the psoas major muscle: the vertical distance from the anterior edge of the psoas major muscle to the coronal line. The midpoint of the abdominal aorta and left common iliac arteries: the distance from the midpoint of the abdominal aorta and left common iliac arteries to the coronal line; the posterior edge of the abdominal aorta and left common iliac arteries: the distance from the posterior edge of the abdominal aorta and left common iliac arteries to the coronal line; the left outer edge of the abdominal aorta and left common iliac arteries: the distance from the left outer edge of the abdominal aorta and iliac arteries to the sagittal line. The posterior edge of the kidney: the vertical distance from the posterior edge of the kidney to the coronal line. Lumbar curvature (lumbar lordosis angle) is defined as the angle between the upper endplate of L1 and the endplate of the sacrum. In the measured transaxial plane, the coronal line with the ventral side is defined as positive values, and the dorsal side is defined as negative values. The sagittal line with the left side is defined as positive values, and the right side is defined as negative values. The measurements were independently completed by 2 spinal surgeons and the final verification was done by the author. This study was approved by the Ethics Committee of Tianjin Hospital of Tianjin University (Ethics No.: 2023 Medical Ethics Review 160). (A) Prone decubitus (lateral view): Small pillows are placed under the chest and pelvis to allow the abdomen to hang freely, with a slight flexion of the hip joints. (B) Prone decubitus (posterior view), C) Right lateral decubitus (lateral view): a small pillow is placed under the waist, with a slight flexion of the hip joints. (D) Right lateral decubitus (posterior view), E) Right oblique decubitus (lateral view): The patient lies on a prepared inclined mold, with small pillows placed under the chest and pelvis to allow the abdomen to hang freely, and a slight flexion of the hip joints. (F) Right oblique decubitus (posterior view). (A) Methods for measuring the positions of the psoas major, arteries, and kidneys. All measurements are taken at the intervertebral disc level. (B) Schematic diagram of data measurement in prone decubitus. Coronal line: Parallel to the intervertebral space passing through the center of the intervertebral disc and parallel to the anterior and posterior edges of the vertebral body. Sagittal line: Parallel to the intervertebral space passing through the center of the intervertebral disc and perpendicular to the anterior and posterior edges of the vertebral body. Both the coronal and sagittal lines pass through the center of the intervertebral disc and are perpendicular to each other. (C) Schematic diagram of data measurement in lateral decubitus. Outer edge of the psoas major (A): At the disc level, the vertical distance from the outermost edge of the psoas major to the sagittal line. Anterior edge of the psoas major muscle (B): The vertical distance from the most anterior edge of the psoas major muscle to the coronal line. Posterior edge of the abdominal aorta and iliac arteries (C): The distance from the posterior edge of the abdominal aorta and iliac arteries to the coronal line. Midpoint of the abdominal aorta and iliac arteries (D): The distance from the midpoint of the abdominal aorta and iliac arteries to the coronal line. Left outer edge of the abdominal aorta and iliac arteries (E): The distance from the left outer edge of the abdominal aorta and iliac arteries to the sagittal line. Posterior edge of the kidney (F): The vertical distance from the posterior edge of the kidney to the coronal line. (D) Schematic diagram of data measurement in oblique decubitus.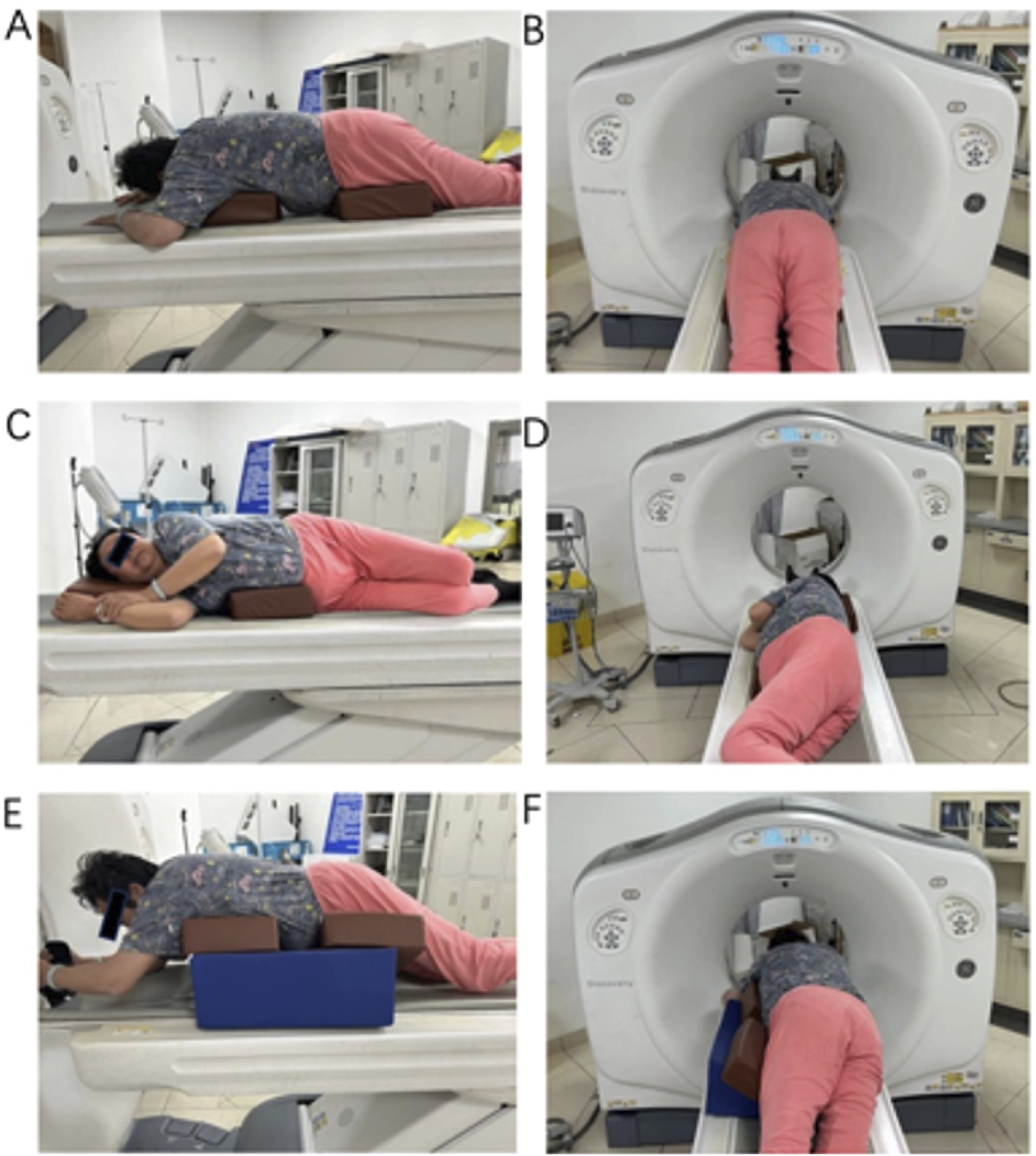
Statistics
The measurements of the psoas major, arteries, kidneys, and lumbar lordosis angle in the 3 decubitus were compared with each other. Paired t-tests were conducted respectively, with a P-value of less than 0.05 indicating a significant difference. All analyses were performed using the Statistical Package for the Social Sciences (SPSS).
Results
Changes in the Position of the Psoas Major
Changes in the Anterior Edge and Outer Edge Positions of the Psoas Major Muscle Among 3 Different Decubitus
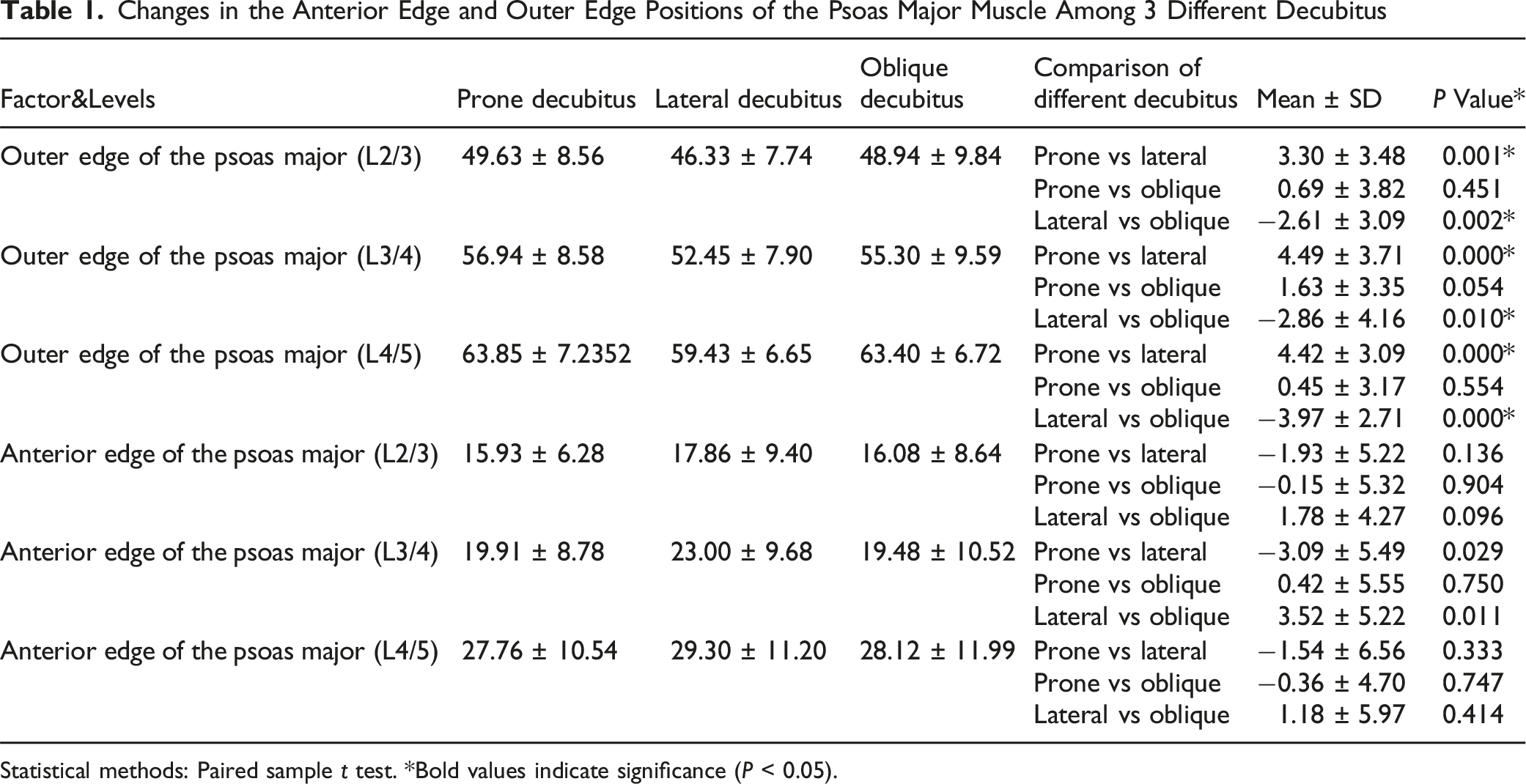
Statistical methods: Paired sample t test. *Bold values indicate significance (P < 0.05).
Changes in the Position of the Vascular Midpoint, Lateral Edge, and Posterior Edge Among 3 Different Decubitus.
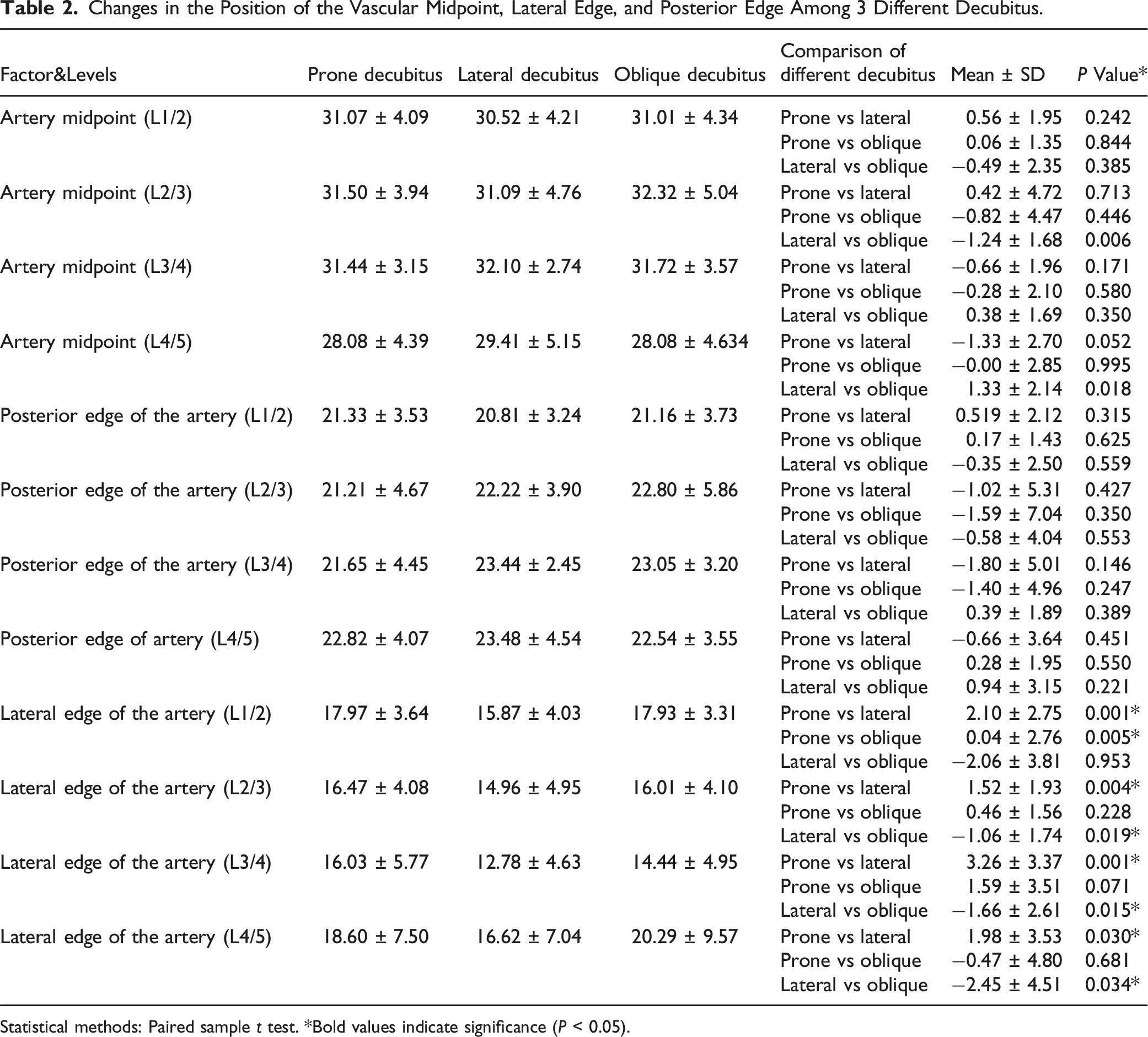
Statistical methods: Paired sample t test. *Bold values indicate significance (P < 0.05).
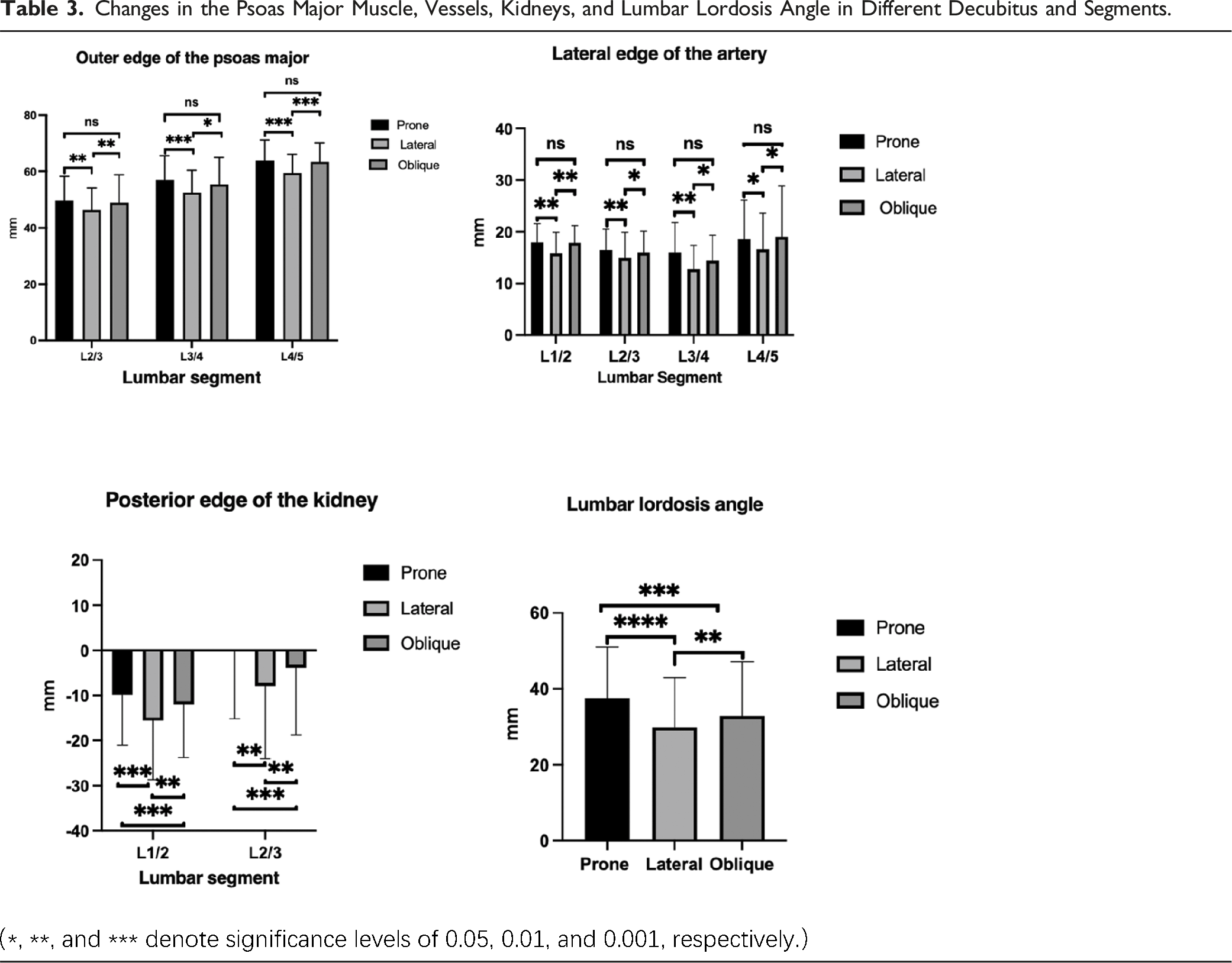
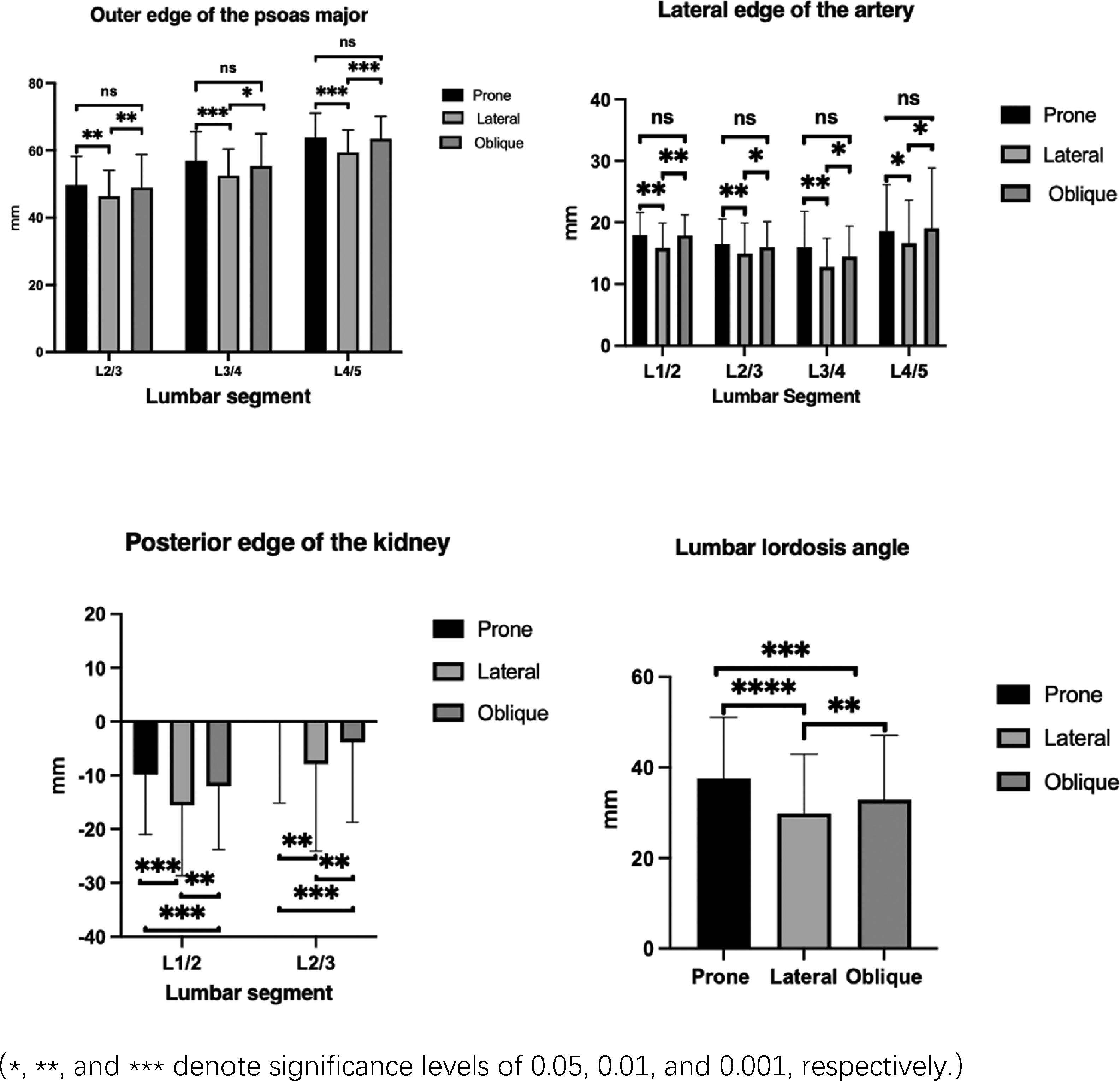
Changes in the Psoas Major Muscle, Vessels, Kidneys, and Lumbar Lordosis Angle in Different Decubitus and Segments.
Arterial Position Changes
The outer edges of the abdominal aorta and left common iliac arteries exhibit significant positional changes in the 3 different decubitus. An increase in the numerical value of the artery’s outer edge indicates a leftward shift of the artery. An increase in the numerical value of the artery’s midpoint indicates a ventral shift of the vessel; an increase in the numerical value of the artery’s posterior edge also indicates a ventral shift. Compared to the lateral decubitus, in the prone decubitus, the outer edge of the abdominal aorta shifted laterally by 2.29 ± 2.79 mm (P < 0.05), and the left common iliac artery shifted laterally by 1.97 ± 3.53 mm (P < 0.05). Compared to the lateral decubitus, in the oblique decubitus, the outer edge of the abdominal aorta increased by 1.59 ± 2.82 mm (P < 0.05), and the left common iliac artery shifted laterally by 2.45 ± 4.51 mm (P < 0.05). When comparing the prone decubitus with the oblique decubitus, there was no statistically significant change in the arterial outer edge values (P > 0.05). Additionally, there were no statistically significant differences in the values of the arterial midpoint and posterior edge among the prone decubitus, oblique decubitus, and lateral decubitus (P > 0.05). The measurement results are summarized in Tables 2 and 3.
Kidney Position Changes
The position of the kidneys significantly changes in the 3 different decubitus. An increase in the distance of the posterior edge of the kidney indicates a ventral shift of the kidney. Compared to the lateral decubitus, the posterior edge of the kidney in the prone decubitus increased by 6.97 ± 5.84 mm (P < 0.05), and in the oblique decubitus, it increased by 3.92 ± 4.70 mm (P < 0.05). When comparing the prone decubitus with the oblique decubitus, the posterior edge of the kidney increased by 3.06 ± 3.74 mm (P < 0.05). The measurement results are summarized in Table 3.
Lumbar Lordosis Angle Changes
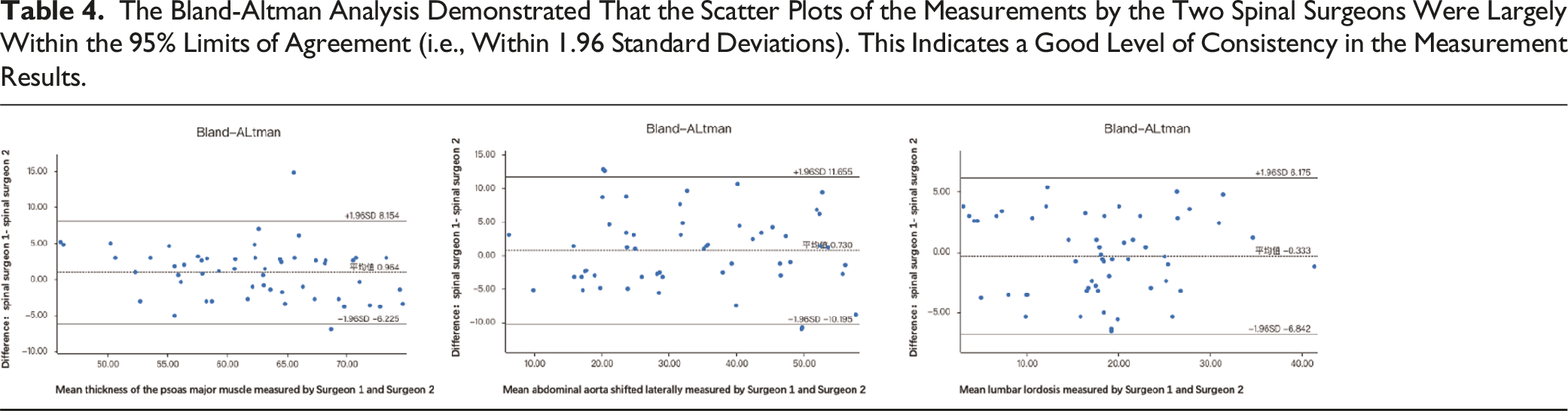
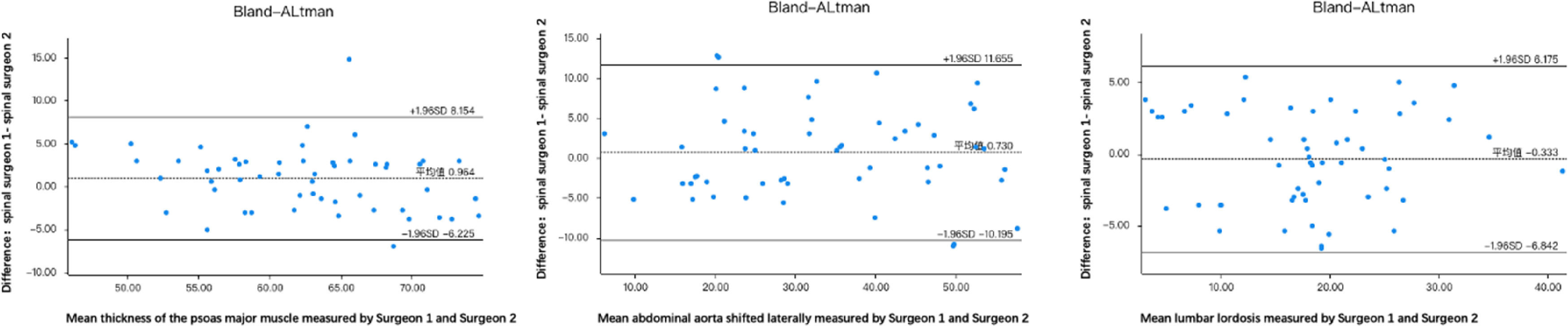
The Bland-Altman Analysis Demonstrated That the Scatter Plots of the Measurements by the Two Spinal Surgeons Were Largely Within the 95% Limits of Agreement (i.e., Within 1.96 Standard Deviations). This Indicates a Good Level of Consistency in the Measurement Results.
Discussion
The purpose of this study was to clarify the positional changes of retroperitoneal organs and the lumbar lordosis angle in different decubitus by comparing the anatomical locations of retroperitoneal organs and the lumbar lordosis angle in patients in the prone decubitus, right lateral decubitus, and oblique decubitus. The study found that compared with the lateral position, the thickness of the psoas major muscle increased in the prone decubitus, with the abdominal aorta and left common iliac artery shifting laterally, the kidneys moving anteriorly, and an increase in the lumbar lordosis angle; compared with the lateral decubitus, the thickness of the psoas major muscle increased in the oblique decubitus, with the abdominal aorta and left common iliac artery shifting laterally, the kidneys moving anteriorly, and an increase in the lumbar lordosis angle; compared with the oblique decubitus, there was anterior movement of the kidneys and an increase in the lumbar lordosis angle in the prone position. The greatest changes were observed in the thickness of the psoas major muscle, the lumbar lordosis angle, and the position of the kidneys. The conclusion is that, compared with the lateral decubitus, the increased thickness of the psoas major muscle in the prone and oblique decubitus is beneficial for surgical operations; the lateral shift of the abdominal aorta and iliac common arteries may increase the risk of injury; the anterior movement of the kidneys increases the range of surgical operation, and the increase in the lumbar lordosis angle is beneficial for reconstructing lumbar lordosis.
Since Lamartina et al. 3 proposed the single-position prone lateral lumbar interbody fusion (P-LLIF) procedure, a significant number of studies on cases involving this surgical technique have been reported. The advantages of this procedure include the elimination of the need to change patient position and repositioning during surgery, which saves operating and anesthesia time,17-19 reduces intraoperative X-ray exposure, and is more conducive to restoring lumbar lordosis. 20 Furthermore, if the lateral approach is not successful, it is easier to switch to a posterior approach.8,21 With the patient in a prone position during surgery, the effect of gravity and the free hanging of the abdominal contents leads to corresponding changes in the retroperitoneal organs and the lumbar lordosis angle. 22 Retractors and fusion devices also shift anteriorly due to gravity, 8 and neglecting these changes can increase the risk of anterior longitudinal ligament rupture. 21 This could potentially lead to damage to the major vessels located anterior to the anterior longitudinal ligament. 8
Mastering the patient’s accurate anatomical structure preoperatively is a key factor in ensuring the safety of the surgery. In minimally invasive surgery, changes in anatomical structures are particularly important. For patients undergoing (P-LLIF), preoperative imaging data is often obtained with the patient in a supine decubitus, while the surgery is performed in the prone and oblique decubitus. There will be some changes in the position of the retroperitoneal organs of the patient during surgery compared to preoperative imaging. Especially the changes in blood vessels and nerves have a significant impact on the safety of the surgery. For the first time, we studied the changes in the position of retroperitoneal organs and lumbar lordosis angle in 3 positions: prone, right lateral, and oblique decubitus (30°). Patients scheduled for LLIF surgery were included as research subjects. During CT measurement, the abdomen was allowed to hang freely to analyze the changes in the position of the major muscle, arteries, kidneys, and other retroperitoneal organs, as well as the lumbar lordosis angle in 3 different decubitus. Currently, there have been no reports on the positional changes of retroperitoneal organs in the oblique and right lateral decubitus.
The lumbar plexus is located within the psoas major and extends distally along it.23,24 Kepler et al, 25 after analyzing 43 cases of lumbar MRI, suggested that the psoas major muscle can serve as a landmark for the position of the lumbar plexus; when the position of the psoas major muscle changes, the lumbar plexus also changes accordingly Uribe et al. 26 divided the area between the anterior and posterior edges of the vertebrae into 4 equal regions, designated from ventral to dorsal as Zone I, Zone II, Zone III, and Zone IV. The safe anatomical area for the L1-2 and L3-4 intervertebral disc spaces is located in the middle posterior quarter of the vertebra (the midpoint of Zone III), and the safe anatomical area for the L4-5 intervertebral disc space is at the midpoint of the vertebra (the boundary line between Zone II and Zone III). There is a risk of direct damage to the genitofemoral nerve in Zone II at the L2-3 interspace and in Zone I at the L3-4 and L4-5 lumbar levels. If the psoas major muscle is normally developed, its position can be used to determine the location of the zones, which can then be used to assess changes in the position of the lumbar plexus and blood vessels. This is significant for avoiding nerve and vascular damage. Hu et al. 27 believe that the thickness of the psoas major muscle affects the safety of surgery. A thick psoas major muscle facilitates easier dissection of the peritoneum, provides a larger retroperitoneal space, is beneficial for surgical manipulation, and reduces the risk of peritoneal and intra-abdominal organ damage. Our study found that the thickness of the psoas major increased in the prone decubitus compared to the lateral decubitus and in the oblique decubitus compared to the lateral decubitus. There was no significant difference in the thickness of the psoas major between the prone and oblique decubitus, indicating no significant change in the thickness of the psoas major when switching between the prone and oblique decubitus during surgery. The thickness of the psoas major muscle in P-LLIF is significantly greater than in traditional LLIF. Combined with previous research, it is concluded that the prone position is more conducive to accessing the retroperitoneal space. The change in thickness of the psoas major muscle is consistent with the findings of Gandhi et al. 13 However, the changes in the anterior edge and the anteroposterior length of the psoas major muscle in the prone, oblique, and lateral conducive were not statistically significant. In contrast, Gandhi et al. 13 suggested that the anteroposterior length of the psoas major increases in the lateral decubitus.
The abdominal aorta and the left external edge of the left common iliac artery undergo significant changes in the 3 decubitus. Compared to the lateral decubitus, the left external edge of the abdominal aorta (L1/2-L3/4) and the left common iliac artery (L4/5) significantly shifts to the left in the prone and oblique decubitus. There is no significant difference in the movement of the left external edge of the abdominal aorta and left common iliac artery when comparing the prone and oblique decubitus. The midpoint and posterior edge of the artery show no statistically significant changes among the prone, lateral, and oblique decubitus. This indicates that there is no significant change in the position of the abdominal aorta and left common iliac artery when the patient’s operating table is changed between the prone and oblique decubitus during surgery. However, compared to the lateral decubitus, the left external edge of the abdominal aorta and left common iliac artery shifts to the left. The change in the position of the vessel midpoint is consistent with the conclusions of Gandhi et al. 13 on the positional changes of retroperitoneal organs in 10 healthy adults. There are currently no literature reports on the changes in the distance of the arterial external edge. During LLIF surgery, the external edge of the artery is closer to the surgical operating area, and the movement of the left external edge of the artery has more clinical significance in actual surgical operations. The leftward shift of the abdominal aorta and iliac artery in the prone decubitus could increase the risk of vascular injury, particularly during retractor placement. This emphasizes the importance of preoperative vascular imaging to assess vessel displacement and minimize intraoperative complications. The position of the kidneys significantly changes in the 3 different decubitus. Compared with the lateral decubitus, the kidneys significantly shift anteriorly in the prone decubitus, and they also significantly shift anteriorly in the oblique decubitus compared to the prone decubitus, and similarly, they significantly shift anteriorly in the oblique decubitus compared to the lateral decubitus. This indicates that under P-LLIF, the kidneys can significantly shift anteriorly, increasing the space for the surgical operating channel.
Comparison of Prone, Lateral, and Oblique Decubitus Positions in Medical Surgery.

The limitation of this study is that, due to concerns regarding the radiation from CT scans, a relatively small number of subjects were included, which may lack representativeness of the overall sample. This could, in turn, reduce the accuracy of the results estimated through the sample.
A 59-year-old female with lumbar lordosis straightening underwent P-LLIF in the prone decubitus, which resulted in a +8° increase in lumbar lordosis, highlighting its effectiveness in sagittal correction (Figure 3). (A) 59-year-old female with lumbar lordosis straightening underwent P-LLIF in the prone decubitus, which resulted in a +8° increase in lumbar lordosis, highlighting its effectiveness in sagittal correction. (A and B) represent the patient’s intraoperative positions. (C) is the preoperative lateral radiograph of the lumbar spine, with a lumbar lordosis of 16.3° and a lumbar segmental lordosis of 6.9°. (D)is the postoperative lateral radiograph of the lumbar spine, with a lumbar lordosis of 24.3° and a lumbar segmental lordosis of 13.3°.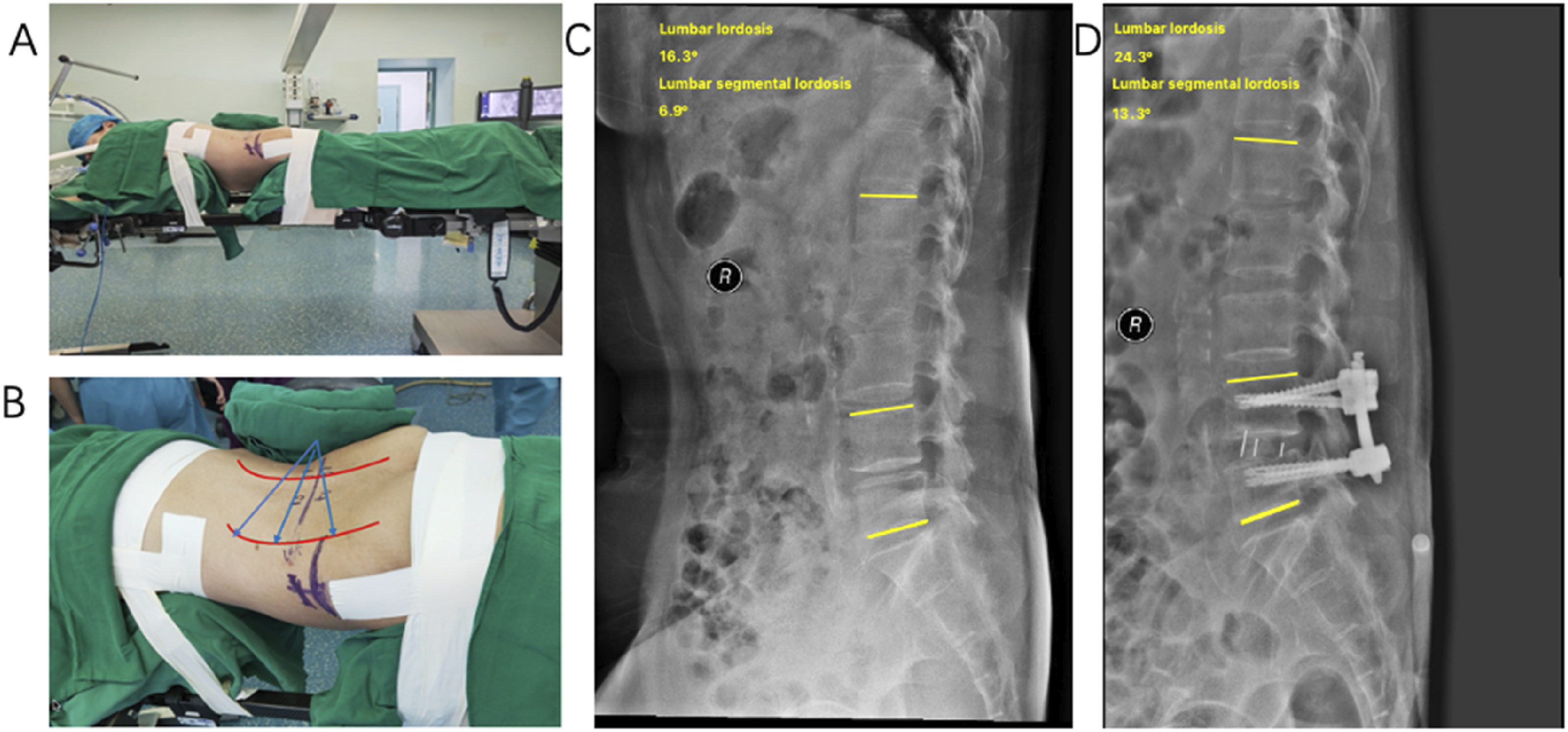
Conclusion
This article provides the first description of the positional changes of retroperitoneal organs in the oblique decubitus and, for the first time, uses the right lateral decubitus in patients to assess the changes in the position of retroperitoneal organs during P-LLIF. The CT imaging analysis of patients in 3 different decubitus shows that important retroperitoneal structures significantly shift with changes in position. In both the prone and oblique decubitus, the thickness of the psoas major increases, the left lateral edge of the abdominal aorta and the left lateral edge of the left common iliac artery move laterally, the kidneys move anteriorly, and the lumbar lordosis angle increases. The results of this study not only provide anatomical evidence for the feasibility of P-LLIF but also confirm that P-LLIF can offer a better surgical operating space and an increased lumbar lordosis angle.
In conclusion, this study’s findings provide a seminal anatomical perspective for P-LLIF, elucidating the significant positional shifts of retroperitoneal organs and the implications for surgical practice. The pronounced lordosis angle in the prone decubitus position presents a compelling case for the optimization of surgical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Natural Science Foundation of China (82372419), Tianjin Science and Technology Major projects and projects “unveiled” major projects (21ZXJBSY00130) and Beijing-TianJin-HeBei Cooperation Project (J230020).