
Abstract
Study Design
Retrospective cohort study.
Objectives
This study aimed to compare the clinical efficacies of endoscopic surgery and nonsurgical treatment in patients with extruded or sequestered lumbar disc herniation (LDH).
Population
613 patients with extruded or sequestrated LDH were included (endoscopic: n = 276; nonsurgical: n = 337).
Methods
Patients received either endoscopic discectomy or structured nonsurgical management. Longitudinal VAS and ODI trajectories were analyzed using linear mixed-effects models. Return to work (RTW) outcomes were evaluated using Kaplan–Meier survival curves and Cox proportional hazards models. Spearman correlation was used to assess the association between resorption and symptom improvement.
Results
Both cohorts had comparable sex, BMI, and herniation levels (P > .05), but differed in age (P < .001), which did not influence outcomes after adjustment. VAS and ODI improved in both groups over time (P < .001). Endoscopic discectomy provided faster symptom relief within 6 months (P < .001), whereas mid to long-term outcomes were comparable between groups (P > .05). Disc resorption occurred in 58.2% of nonsurgical patients (median time 6.9 months). Resorption was correlated with greater improvements in ODI and VAS (P < .05). Surgical complications included transient neurological deficits (17.4%), dural tears (1.1%), and epidural hematomas (0.7%). Postoperative recurrence occurred in 8.3% of patients. RTW time was unaffected by treatment, sex, BMI, or herniation level (P > .05), but was influenced by age (HR = 0.948, P < .001) and occupational demands (HR = 0.697, P < .001).
Conclusions
Endoscopic discectomy provides faster early pain and functional improvement (≤6 months), while nonsurgical management achieves comparable outcomes thereafter. Disc resorption contributes to symptom recovery. RTW time is determined primarily by age and occupational demands.
Introduction
Lumbar disc herniation (LDH) involves pathological displacement of intervertebral disc components, including the nucleus pulposus, annulus fibrosus, and/or cartilaginous endplates, beyond their anatomical confines. The herniated material induces neurological symptoms, which manifest as radicular pain, dermatomal sensory deficits, and myotomal weakness, by mechanical compression or chemical irritation of lumbosacral nerve roots and adjacent structures. These symptoms distinguish LDH from discogenic or myofascial pain syndromes.1,2 On the basis of morphological criteria, 3 herniations (annular bulges or protrusions with an intact posterior longitudinal ligament) are classified as extrusions (nucleus pulposus ruptures) and sequestrations (migrated free fragments) and are different from noncontained types, which involve annular rupture. Notably, the extrusion and sequestration subtypes constitute severe forms of LDH and are characterized by intraspinal nucleus pulposus displacement. These subtypes often induce refractory radiculopathy and progressive neurological deficits and carry risks of cauda equina syndrome. Although they may cause irreversible injury, if untreated, significant functional recovery remains achievable through conservative management in selected cohorts.4,5
Spontaneous regression represents an established phenomenon in the natural history of LDH. Systematic conservative management can lead to significant resorption of intraspinal sequestered fragments in approximately 67% of cases. Interestingly, compared with smaller herniations, larger herniations exhibit accelerated resorption kinetics, which is likely due to enhanced macrophage-mediated phagocytosis.6-8 A prospective trial by Albert et al 9 reported 100% radiographic resorption of herniated fragments in patients receiving gabapentin or acupuncture monotherapy (an NSAID-free protocol), which correlated with substantial clinical improvement. These findings validate our 2013 hypothesis proposing restricted NSAID use in such clinical contexts. 10 This noninvasive decompression mechanism—reducing neural compression through biological resorption—has critical clinical value in managing extruded or sequestered LDH. Complementing conservative management, spinal endoscopy has become a cornerstone minimally invasive intervention for LDH. Compared with open discectomy, endoscopic techniques yield superior outcomes, including reduced iatrogenic trauma, shorter hospital stays, lower healthcare costs, and accelerated functional rehabilitation. With these advantages, endoscopic discectomy has increasingly become the preferred surgical option for most patients with LDH. 11 Contemporary methodologies primarily include the following three approaches: percutaneous endoscopic lumbar discectomy (PELD), unilateral biportal endoscopy (UBE), and one-hole split endoscopy (OSE). For patients with persistent symptoms after extended conservative therapy or those who exhibit neurological deterioration, timely endoscopic intervention mitigates the risk of irreversible deficits from progressive neural compression.12-14
Current evidence lacks direct comparisons between established spinal endoscopic techniques and nonsurgical interventions for extruded or sequestered LDH. Therefore, this retrospective cohort study examined the comparative clinical effectiveness of endoscopic surgery vs conservative management for this specific pathology to generate evidence-based guidance for clinical decision making.
Methods
Patient Characteristics
Between July 2015 and May 2023, 613 consecutive patients with confirmed extruded or sequestered LDH who met the inclusion criteria were enrolled at the Suzhou TCM Hospital Affiliated with Nanjing University of Chinese Medicine. Among them, 276 patients, including 123 females and 153 males, with ages ranging from 17 to 89 years, underwent surgical treatment. The nonsurgical cohort included 337 patients—133 females and 204 males—aged 17-77 years (Figure 1). Demographic and clinical parameters (sex, age, body mass index (BMI), herniation level, time to return to work, resorption time, and resorption rate) were systematically documented. Data were collected prospectively and analyzed retrospectively Figures 2 and 3. Flow diagram of patient enrollment Case 1 (Female, 43 years). (A) The patient initially presented with 1 week of low back pain and radiating pain with sensory disturbance along the posterior aspect of the left calf. Lumbar MRI showed an L5/S1 disc extrusion with a fragment volume of 742.8 mm3; ODI was 46.0%. Symptoms improved with conservative management; (B) Two years later, symptoms recurred and worsened after heavy physical work. Repeat MRI demonstrated progression of the L5/S1 extrusion with a fragment volume of 1593.8 mm3; ODI increased to 60.2%; (C) After 3 months of nonsurgical treatment, contrast-enhanced MRI showed mild linear enhancement without significant volume change; symptoms partially improved (ODI 42.5%); (D) At 6 months, contrast-enhanced MRI showed marked enhancement with volume reduction to 628.62 mm3; ODI improved to 27.0%, with substantial symptom relief; (E) At the 1-year final follow-up, MRI demonstrated further regression with a residual fragment volume of 236.5 mm3 (resorption rate 85.2%). Low back and left leg symptoms had nearly resolved, with an ODI of 10.0% Case 2 (Male, 36 years). (A) The patient initially presented with a 2-year history of low back pain and left buttock-leg pain, which markedly worsened after strenuous activity 3 days prior. He also reported sensory loss over the left posterior calf and plantar region, with left toe-flexor strength graded as 4/6. Lumbar MRI demonstrated a left-sided L5/S1 disc extrusion; ODI was 71.0%; (B) Symptoms did not improve after conservative treatment; therefore, unilateral biportal endoscopic discectomy with annular repair was performed. At 1 week postoperatively, pain improved markedly, and ODI decreased to 33.5%; (C) At the 6-month follow-up, MRI showed no residual compression of the left S1 nerve root. ODI had further improved to 21.2%, and left toe-flexor strength recovered to 5/6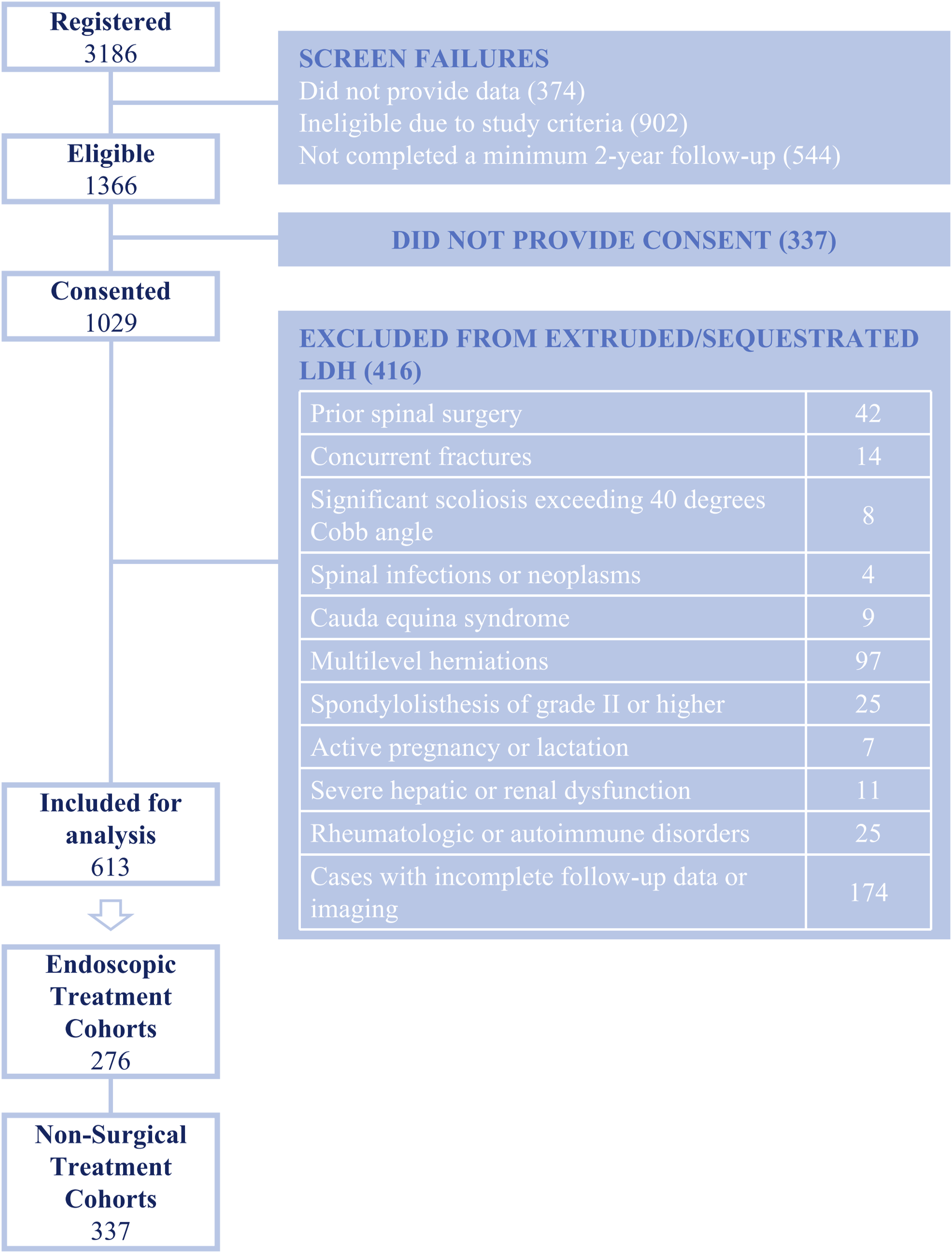


Inclusion and Exclusion Criteria
Inclusion required meeting established diagnostic criteria for lumbar disc herniation, with magnetic resonance imaging (MRI) confirmation of the extrusion or sequestration subtype per standardized classification.3,12 The key MRI features included the interruption of the hypointense posterior vertebral margin line on sagittal T2-weighted sequences with irregular nuclear margins, coupled with the disc material extending beyond the native interspace, demonstrating superior or inferior migration—either pedunculated or fully isolated as a rounded mass. All the enrolled patients completed a minimum 24-month follow-up. All patients underwent flexion–extension radiographs before inclusion. Patients with clinical symptoms attributable to lumbar instability or spondylolisthesis were excluded or referred for fusion procedure. The exclusion criteria also included prior spinal surgery, concurrent fractures, significant scoliosis, spinal infection or neoplasm, cauda equina syndrome, multilevel herniations, active pregnancy or lactation, severe hepatic or renal dysfunction, rheumatologic or autoimmune disorders, and incomplete follow-up or imaging data.
Treatment Cohorts
Endoscopic Treatment Cohort: A total of 276 patients who demonstrated insufficient clinical improvement after ≥3 months of standardized conservative management underwent spinal endoscopic surgery. All the surgical procedures were performed by two highly experienced spinal surgeons. Postoperative care comprised the following three components: (1) pharmacotherapy: nonsteroidal anti-inflammatory drugs (NSAIDs), osmotic agents, neurotrophic agents, and proton pump inhibitors for gastric protection; (2) activity protocol: bed rest for 1-3 days (adjusted per pain tolerance) with mandatory lumbar bracing during ambulation; and (3) rehabilitation, which was initiated 48 hours postsurgery and featured core stabilization exercises targeting the lumbar‒abdominal musculature (transversus abdominis and multifidus activation).
Nonsurgical Treatment Cohort: A total of 337 eligible patients were managed conservatively according to a standardized protocol. 15 The regimens included the following: (1) general management with bed rest and lumbar bracing during activities in the acute phase, transitioning to progressive functional exercises for lumbar paraspinal strengthening in the chronic phase; (2) individualized pharmacotherapy, comprising NSAIDs, osmotic agents, corticosteroids, ion channel modulators, central muscle relaxants, neurotrophic agents; and (3) physical modalities, such as lumbar traction, thermotherapy, medicinal fumigation, intermediate or low-frequency electrotherapy, physical therapy (including massage and manipulation), and acupuncture.
Treatment allocation was non-randomized and based on a standardized clinical decision-making pathway used at our institution. Patients were initially recommended to undergo at least 6-12 weeks of structured nonsurgical management, unless absolute surgical indications were present. Surgical indications included: (1) persistent or worsening radicular pain despite ≥3 months of standardized conservative therapy; (2) radiographic evidence of nerve root compression correlating with symptoms; (3) intolerance to persistent severe radiculopathy affecting daily activities; (4) patient preference after shared decision-making. Absolute surgical indications, including cauda equina syndrome, progressive motor deficit, or rapidly deteriorating neurological function, were excluded from the nonsurgical cohort and were not included in this study. Nonsurgical management indications included newly diagnosed extruded or sequestrated LDH without neurological deterioration and patient willingness to continue conservative care.
Calculation of the Resorption Rate and Resorption Time
The volume of the herniated nucleus pulposus (HNP) was calculated using the following formula:
V (mm3) = (slice thickness + interslice gap) (mm) × Σ (protrusion area per slice) (mm2). Follow-up MRI was performed at ≥3 months after initiating systematic treatment. Resorption rate (%) = [(pretreatment volume - final follow-up volume)/pretreatment volume] × 100. 16 Resorption was defined as a resorption rate >30%. 17 The resorption time was calculated as the interval between the initial MRI diagnosis of extruded or sequestered LDH and the follow-up MRI confirmation of resorption.
Recurrence and Complications
Postoperative recurrence was defined as significant alleviation or complete resolution of clinical symptoms after surgery, followed by the reappearance of LDH ≥6 months postoperatively at the same spinal segment (ipsilateral or contralateral) with corresponding clinical manifestations, excluding other potential causes. 18
We assessed postoperative recurrence and reoperation rates in surgically treated patients, along with complications, including nerve root injury, cerebrospinal fluid (CSF) leakage, surgical site infection, and hematoma formation. Severe nonsurgical complications (e.g., cauda equina syndrome and permanent neurological deficits) were also documented.
Clinical Efficacy Evaluation
All the patients were evaluated pretreatment and followed up at the following time points: pretreatment, short-term post-treatment (≤6 months), midterm posttreatment (7-24 months), and long-term posttreatment(over 24 months at the final follow-up). The clinical efficacy was evaluated using the visual analogue scale (VAS) 19 and oswestry disability index (ODI) 20 scores, which were assessed for both cohorts during pretreatment and at the short-term, midterm, and long-term follow-ups. If multiple assessments were conducted within the same period, the highest score recorded within each time interval was used for analysis. Symptom improvement was quantified as the change in ODI and VAS scores from baseline to the final follow-up (ΔODI and ΔVAS). The clinical effectiveness of the two treatment modalities for extruded or sequestered LDH was then comprehensively compared on the basis of these results.
Time to Return to Work (RTW)
The time to RTW was analyzed in both treatment cohorts, with the sick leave duration calculated in weeks from the initial treatment date. For patients with multiple sick leave episodes, the cumulative duration was recorded as the RTW time. Patients who returned to work were stratified by occupational demands into the physical labor group (≥70% physically demanding tasks) or the cognitive work group (≥70% cognitively demanding tasks). Cognitive work included occupations requiring predominantly mental activities, such as scientific research, education, design, administration, and other roles emphasizing analysis, decision-making, and innovation. Physical labor included occupations characterized by sustained muscular exertion or manual tasks, such as industrial and construction work, agricultural labor, and other jobs involving substantial physical effort.
Study Size
A priori power analysis (GPower 3.1) by using documented 21 2-year ODI improvements (surgical: −31.4, interquartile range (IQR) 1.7; nonsurgical: −28.7, IQR 1.7) yielded Cohen’s d = 1.587 for a power of 95% (α = 0.05, two-tailed Mann‒Whitney U test, 1:1 allocation). A power calculation suggested that 12 patients/group were needed. To increase generalizability and allow for subgroup analyses, 613 patients (surgery = 276, nonsurgery = 337) were enrolled.
Statistics
All analyses were performed using SPSS (version 26.0, IBM, Chicago, USA). Intergroup comparisons of baseline characteristics were performed by independent t tests, Mann‒Whitney U tests, or chi‒square tests. Longitudinal changes in VAS and ODI scores were analyzed using linear mixed-effects models incorporating fixed effects for the treatment group, timepoint, group-by-time interaction, and baseline age, with subject-specific random intercepts and random time slopes to account for individual variations. Simple-effects analysis was used to evaluate significant interaction effects. To investigate the relationship between disc resorption and clinical symptom improvement, Spearman’s rank correlation analysis was performed. Disc resorption was evaluated using resorption status and resorption rate.
Kaplan‒Meier analysis was used to compare the RTW time distributions between the treatment cohorts. Patients who were unemployed, retired, full-time homemakers, or otherwise not engaged in the workforce at baseline were not eligible for a RTW event and were therefore treated as censored observations in the survival analysis. Cox proportional hazards regression was subsequently employed to evaluate associations between the RTW time and covariates, including the treatment cohort, age, sex, BMI, herniation level, and occupation type. The event status was defined as return to work (1 = event occurred, 0 = censored). This approach quantified the impacts of covariates on the probability of RTW over time. Statistical significance was set at α = 0.05.
Results
Comparison of Baseline Characteristics

Continuous variables are presented as mean ± standard deviation (SD) (normally distributed) or the median [IQR] (nonnormally distributed), and categorical variables are presented as n (%).
aResorption parameters were calculated for 196/337 (58.2%) nonsurgical patients who achieved a volume reduction >30%.
Fixed Effects Testing in Linear Mixed-Effects Models for VAS and ODI Scores
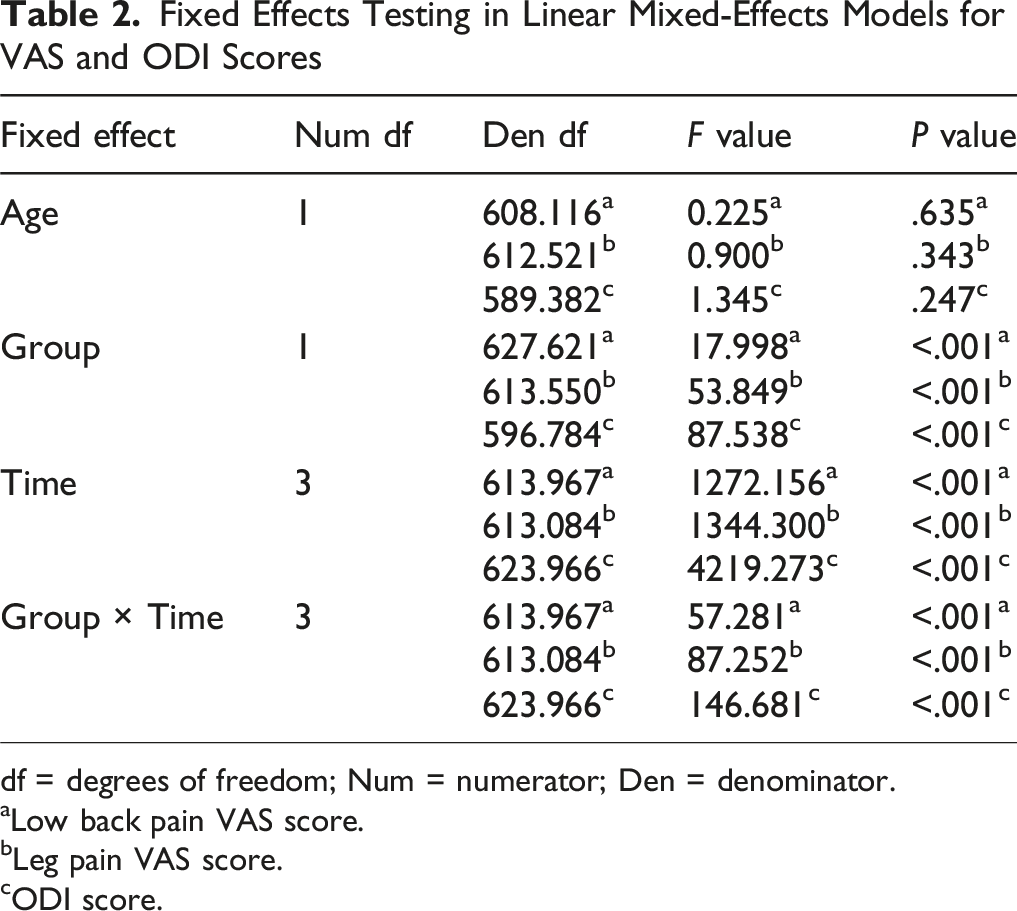
df = degrees of freedom; Num = numerator; Den = denominator.
aLow back pain VAS score.
bLeg pain VAS score.
cODI score.
Simple Effects Analysis of the Group × Time Interaction for Low Back Pain VAS Scores
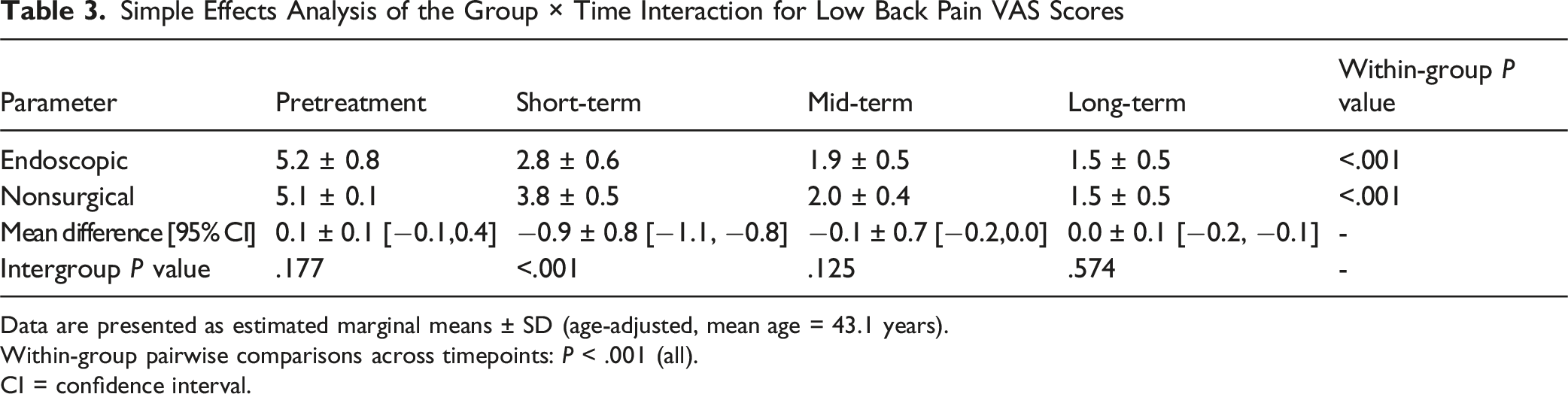
Data are presented as estimated marginal means ± SD (age-adjusted, mean age = 43.1 years).
Within-group pairwise comparisons across timepoints: P < .001 (all).
CI = confidence interval.
Simple Effects Analysis of the Group × Time Interaction for Leg Pain VAS Scores
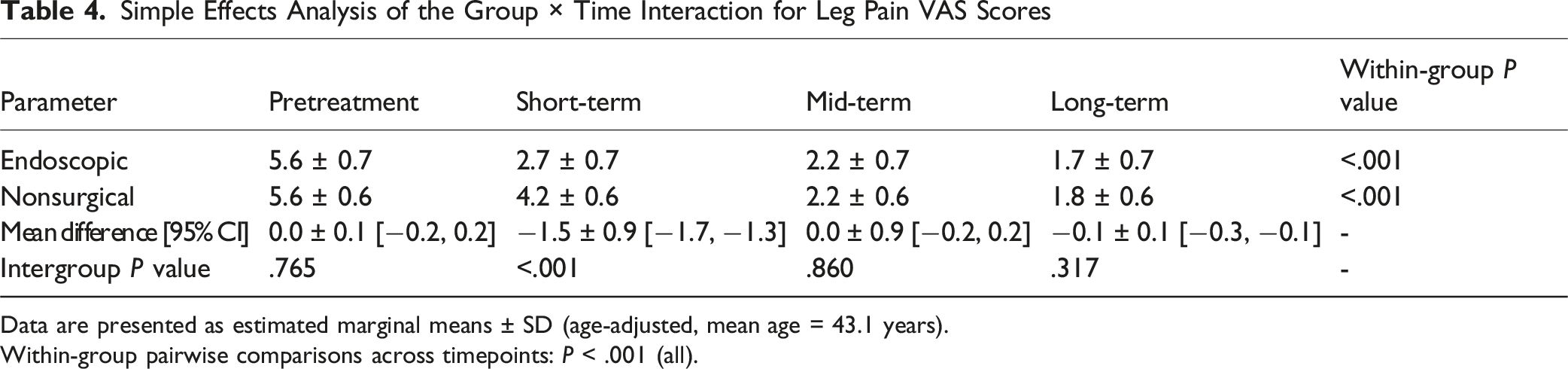
Data are presented as estimated marginal means ± SD (age-adjusted, mean age = 43.1 years).
Within-group pairwise comparisons across timepoints: P < .001 (all).
Simple Effects Analysis of the Group × Time Interaction for ODI Scores
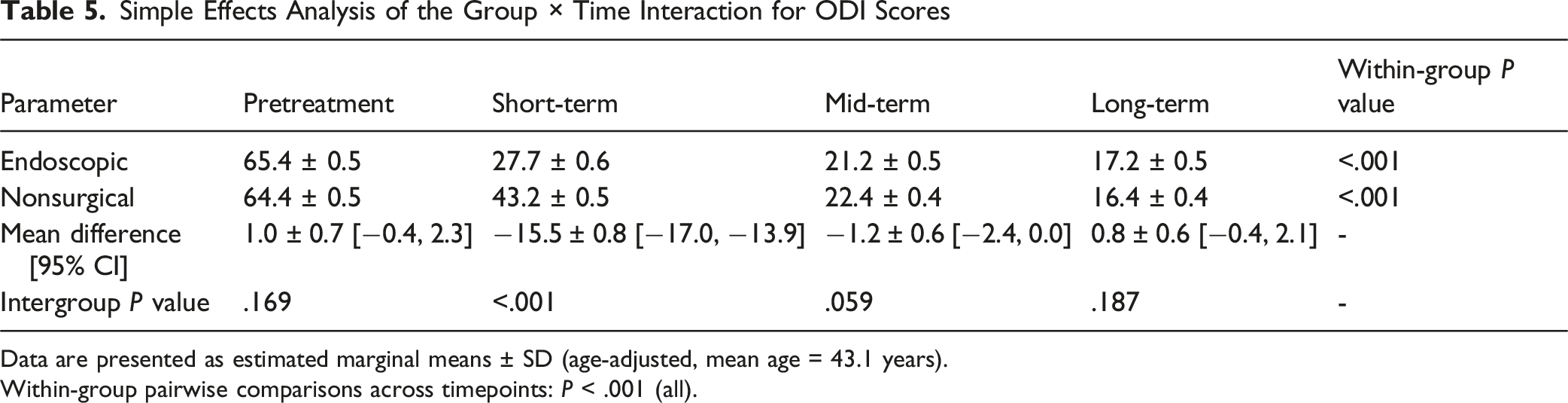
Data are presented as estimated marginal means ± SD (age-adjusted, mean age = 43.1 years).
Within-group pairwise comparisons across timepoints: P < .001 (all).
Spearman correlation analysis showed that the resorption rate was positively correlated with ΔODI (ρ = 0.277, P < .001), leg pain ΔVAS (ρ = 0.124, P = .023), and low back pain ΔVAS (ρ = 0.139, P = .011). Resorption status (>30% volume reduction) was also associated with greater improvements, with significant correlations observed for ΔODI (ρ = −0.292, P < .001), leg pain ΔVAS (ρ = −0.125, P = .022), and low back pain ΔVAS (ρ = −0.121, P = .026).
Complications in the endoscopic surgery group included 3 cases of dural tears (1.1%), 2 cases of symptomatic epidural hematomas (0.7%), and 48 cases of transient postoperative neurological deficits (17.4%). Recurrence occurred in 23 patients (8.3%), 8 of whom underwent revision surgery, while 15 opted for nonsurgical management. No severe complications occurred in the nonsurgical group.
Cox Proportional Hazards Model Analysis of the Time to Return to Work

HR = hazard ratio. Reference categories: sex (male), treatment cohort (endoscopic surgery cohort), level (L5/S1), occupation type (cognitive work).
Overall model test: χ 2 = 123.211, df = 6, P < .001.
Discussion
Despite the significantly younger baseline age in the nonsurgical cohort than in the endoscopic surgery cohort (P < .001), linear mixed-effects modeling (age-adjusted) confirmed that age was not a critical determinant of the efficacy. Both cohorts demonstrated clinically meaningful functional improvements at the ≥24-month follow-up; however, surgery yielded superior short-term outcomes with steeper early VAS and ODI improvement curves—an advantage not sustained during the mid-to long-term observations. Notably, 196 nonsurgical patients (58.2%) exhibited spontaneous disc resorption (median rate: 60.4%, IQR 36.0; median time: 6.9 months, IQR 12.1), which indicates significant natural repair potential, although resorption progression varied substantially among individuals.
Liu et al. 22 reported that discectomy outperformed nonsurgical management in alleviating leg pain and disability in sciatica patients with surgical indications, although the very low certainty of evidence precluded direct clinical application, as efficacy differences diminished over time. For sciatica caused by lumbar disc extrusion, discectomy provides faster acute symptom relief than nonoperative approaches do. 23 In patients with chronic LDH (>4 months), microdiscectomy yields superior pain improvement within 6 months compared with nonsurgical care, although a longer-term follow-up is lacking. 24 Nonsurgical management results in attenuated short-term improvement but enhanced medium-to long-term gains, achieving clinical outcomes comparable to those of surgery,25,26 with favorable 5-year results for complementary and alternative therapies. 27 Despite variations in intervention specifics across studies, our findings align with this expected trajectory.23-27 Surgery remains a double-edged sword, with invasive procedures accelerating lumbar degeneration (>80% incidence) and the risk of secondary instability through disc height loss—a primary contributor to persistent postoperative pain.28,29 Although endoscopic surgery offers confirmed efficacy for extruded or migrated discs, with minimal invasiveness, 30 judicious avoidance of unnecessary surgical exposure remains imperative. Thus, spine surgeons should neither rush to operate nor arbitrarily recommend conservative management.
The biological mechanisms underlying disc resorption remain incompletely understood and primarily involve macrophage infiltration, inflammatory responses, matrix remodeling, neovascularization, and the apoptosis and autophagy of nucleus pulposus cells. 7 While Sucuoğlu and Barut 31 reported clinical and radiological improvements in ∼90% of patients with extruded or migrated LDH after 6 months of conservative management, which is substantially higher than the 58.2% resorption rate in our cohort, long-term evidence confirms that most such patients exhibit a reduced herniation size, along with symptomatic and functional improvements, under nonoperative care. 32 Larger extrusions demonstrate more robust macrophage infiltration, correlating with not only a greater likelihood of resorption but also with accelerated resorption kinetics.17,33 A prospective study reported that approximately 72% of patients developed radiographic resorption only after the first 3 months of conservative treatment, indicating that delayed rather than immediate regression is the predominant pattern in LDH 34 Albert et al 9 observed disc regression within 1 year in all patients, with an average resorption time of 4.4 months. In our cohort, the median time to radiographic resorption was 6.9 months, further demonstrating that the natural course of LDH regression typically unfolds over several months rather than in the early acute phase. Crucially, promoting resorption represents a validated noninvasive therapeutic paradigm for extruded or migrated LDH. Intriguingly, symptom improvement occurs in some conservatively managed patients without radiologically confirmed resorption, suggesting that resorption is not the sole determinant of clinical success and potentially implicating psychological factors, inflammatory cytokine modulation, or cumulative nonsurgical effects—mechanisms requiring further validation. 31 Nevertheless, our correlation analysis demonstrated that disc resorption provided a measurable clinical advantage: both resorption rate and resorption status were significantly associated with greater improvements in ODI and VAS scores. This indicates that although symptomatic relief can occur through multiple nonresorptive pathways, patients who experience radiographic resorption generally achieve a more substantial magnitude of pain relief and functional recovery than those without resorption.
Twenty-three surgical patients (8.3%) recurred, 15 of whom were managed conservatively and 8 of whom required revision surgery. Previous studies have indicated that the incidence of recurrent lumbar disc herniation (rLDH) can reach 6.05%, 35 with multiple risk factors involved, including heavy labor, early ambulation, herniation morphology, diabetes, and inexperienced surgeons, while obesity and smoking directly increase the risk of recurrence.35-37 Over 25% of migrated disc herniations require revision surgery, with recurrent extrusions being the primary indication. 38 For patients with these established high-risk factors, surgical decision making warrants exceptional caution, and proactive nonsurgical protocols should be considered vital alternatives to mitigate the recurrence and reoperation risks inherent to initial surgery. In addition to recurrence, complications significantly impact endoscopic outcomes, with dural tears being the most common complication (incidence: 2%). 39 In our cohort, three patients developed CSF leaks, which were managed successfully with drainage and pharmacotherapy, while two patients exhibited acute postoperative leg pain from epidural hematomas, which were confirmed by MRI and both of which were resolved endoscopically. Transient nerve root symptoms (manifesting as dermatomal pain/hypoesthesia) occurred in 48 patients and were attributed to intraoperative instrument irritation during nucleus pulposus exposure 40 ; most symptoms resolved within 3 days with medication, although five patients retained residual symptoms. Crucially, nonsurgical management, despite possible symptom fluctuations without resorption, resulted in no severe complications, confirming its safety profile for extruded or migrated discs. Patient decisions reflect dual tensions; concerns about neural compromise from prolonged disc compression increase surgical uptake, whereas aversion to surgical complications and recurrence and resorption expectations favor nonoperative approaches.24,32 Multidisciplinary nonsurgical protocols significantly reduce surgical rates, 41 underscoring how therapeutic approach variations influence patient preferences.
RTW constitutes a critical outcome metric in LDH management, impacting both individual well-being and socioeconomic development. 42 While Khan et al. 43 identified age, sex, occupation type, and symptom resolution as key RTW determinants and Laasik et al. 42 corroborated advanced age and physical labor as RTW barriers (although without sex differences), this study specifically addressed the RTW time, revealing that age and occupation influence not only RTW likelihood but also the time to RTW. In contrast to Dandurand et al's 44 report of surgical cost-effectiveness, we observed no significant treatment modality effect on RTW timing; this difference is potentially attributable to heterogeneous study designs and populations and substantial variations in treatment intensity and patient compliance across the trials. Crucially, our analysis revealed that each 1-year increase in age reduced the RTW rate by 5.2%, and physical laborers presented 30.3% lower RTW rates than did cognitive workers. These findings confirmed age and occupation effects, whereas the treatment cohort, BMI, sex, and spine level demonstrated no significant differences. Thus, rather than focusing solely on treatment selection, implementing personalized intensive rehabilitation protocols with enhanced compliance support, particularly for older physical workers, proves more consequential for accelerating safe and sustainable RTW.
Study Limitations
This study was inherently limited by its single-center retrospective design, and treatment allocation was determined by routine clinical decision-making rather than randomization, with patient preference also playing an important role in the choice between surgical and nonsurgical management. Such selection bias is unavoidable in real-world observational studies; however, it reflects genuine clinical practice rather than an idealized treatment assignment.
A further limitation is the heterogeneity of nonsurgical treatments. Conservative care is inherently multimodal in routine practice, and the variations observed here largely represent individualized management rather than methodological inconsistency. Although this reduces standardization, all interventions fall within accepted nonsurgical strategies for lumbar disc herniation and therefore do not fundamentally compromise the comparison between surgical and nonsurgical approaches. Future prospective studies with standardized or stratified nonsurgical protocols are needed to clarify the relative contributions of specific conservative modalities to symptom improvement and disc resorption.
Although age was adjusted for in the mixed-effects models, residual confounding from unmeasured factors cannot be excluded. Nonetheless, the consistent improvement trajectories and stable group-by-time interactions suggest that these limitations do not materially affect the principal conclusions of the study.
Conclusion
Endoscopic discectomy provides faster pain relief and functional recovery within the first 6 months; however, nonsurgical management achieves comparable outcomes thereafter. In the nonsurgical cohort, disc resorption occurred in 58.2% of patients, with a median resorption time of 6.9 months. Resorption was significantly associated with greater improvements in pain and disability. RTW outcomes were not influenced by treatment modality but were strongly dependent on age and occupational demands. Each incremental year of age independently reduced return-to-work rates by 5.2%, and physical laborers exhibited 30.3% lower work resumption rates than did cognitive workers. These findings highlight the importance of individualized treatment selection and shared decision-making to avoid unnecessary early surgery while ensuring timely intervention when indicated.
Footnotes
Acknowledgments
The authors gratefully acknowledge the financial support. We also thank all contributors for their invaluable efforts in this research.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine (No. 2024−018) on November 29, 2024, with the need for written informed consent waived.
CRediT authorship contribution statement
Zhenyu Tang:Writing−original draf, Writing−review & editing, Supervision, Methodology, Data curation, Conceptualization. Xiaorong Li:Writing−original draf, Supervision, Methodology, Investigation,Data curation, Conceptualization. Yucheng Wang:Formal analysis,Conceptualization, Investigation, Conceptualization. Zhijia Ma:Writing−review & editing,Methodology. Zihang Li:Data curation, Conceptualization. Kaiyang Xu:Investigation, Methodology. Hong Jiang:Methodology, Conceptualization. Yuxiang Dai:Writing−review & editing, Formal analysis, Conceptualization, Methodology. Jintao Liu:Methodology, Conceptualization, Supervision, Writing−review & editing. Pengfei Yu:Writing−review & editing, Supervision, Methodology, Conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by National Natural Science Foundation of China (Grant Number: 82474529, 82374220, 82405427). Suzhou Science and Technology Development Plan Project (Grant Number: SKY2023066). Administration of Traditional Chinese Medicine of Jiangsu Province (Grant Number: QN202222, QN202419). Natural Science Foundation of Jiangsu Province (Grant Number: BK20250396、BK20241802). The general project of the Health Commission of Jiangsu Province (Grant Number: H2023059). The Clinical Specialized Disease Research Institute of Nanjing University of Traditional Chinese Medicine (Grant Number: LCZBYJYZZ2024-007).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the cur-rent study are available from the corresponding author upon reasonable request.