
Abstract
Study Design
Retrospective study.
Objective
To compare the clinical outcomes of the biportal endoscopic technique for primary lumbar discectomy (BE-LD) and revision lumbar discectomy (BE-RLD).
Methods
Eighty-one consecutive patients who underwent BE-LD or BE-RLD, and could be followed up for at least 12 months were divided into two groups: Group A (BE-LD; n = 59) and Group B (BE-RLD; n = 22). Clinical outcomes included the visual analog scale (VAS), Oswestry Disability Index (ODI), and modified MacNab’s criteria. Perioperative results included operation time (OT), length of hospital stay (LOS), amount of surgical drain, and kinetics of serum creatine phosphokinase (CPK) and C-reactive protein (CRP). Clinical and perioperative outcomes were assessed preoperatively and postoperatively at 2 days and at 3, 6, and 12 months. Postoperative complications were noted.
Results
Both groups showed significant improvement in pain (VAS) and disability (ODI) compared to baseline values at postoperative day 2, which lasted until the final follow-up. There were no significant differences in the improvement of the VAS and ODI scores between the groups. According to the modified MacNab’s criteria, 88.1 and 90.9% of the patients were excellent or good in groups A and B, respectively. OT, LOS, amount of surgical drain, and kinetics in serum CRP and CPK levels were comparable. Complications in Group A included incidental durotomy (n = 2), epidural hematoma (n = 1), and local recurrence (n = 1) and in Group B incidental durotomy (n = 1) and epidural hematoma (n = 1).
Conclusion
BE-RLD showed favorable clinical outcomes, less postoperative pain, and early laboratory recovery equivalent to BE-LD.
Keywords
Introduction
Microscopic lumbar discectomy (Micro-LD) is a predictable and successful treatment for symptomatic lumbar disc herniation (LDH), but the proportion of patients having a secondary surgery varies in the literature between .5 and 24%.1-3 In particular, recurrent lumbar disc herniation (RLDH), which is defined as the presence of herniated disc material at the same level as previously operated upon in patients who experienced a pain-free phase for more than 6 months, is known to be the most common cause of surgical failure of lumbar discectomy.
The Spine Patient Outcomes Research Trial (SPORT), which was designed as a prospective, observational, and randomized controlled trial to demonstrate clinical evidence for adult spine surgery, evaluated 810 patients who had at least 8 years of follow-up and found a total RLDH rate of 38% and a total reoperation rate of 15%; the reoperation rate for RLDH at 8 years was 9.1%. 4 Furthermore, other studies have reported a 1–13% incidence of surgical revision due to RLDH.5,6
Although local recurrence of lumbar disc herniation does not always require surgery, symptomatic RLDH often fails with conservative treatments. However, the surgical treatment of RLDH, which includes revision lumbar discectomy (RLD) either assisted by a conventional or minimally invasive technique, with or without lumbar instrumented spinal fusion, remains controversial. Results of the microscopic RLD (Micro-RLD) to treat RLDH are reported to be acceptable but inferior and incur greater per-patient costs compared to those of primary Micro-LD.2,7,8 In addition, the percutaneous endoscopic (PE) technique for RLD has advantages in terms of the shorter hospital stay, less bleeding, and lower total cost compared with Micro-RLD. However, PE-RLD has also been associated with a higher recurrence rate and a demanding learning curve.9-13
The biportal endoscopic (BE) technique for spine surgery is a recently introduced endoscopic modality, with features that include a water reservoir as the working space that is created over a posterior vertebra using 2 independent viewing and working ports, and the procedure is performed under continuous fluid irrigation through the water reservoir and the two surgical ports. Moreover, it has been reported that the BE technique for LD yielded similar outcomes to Micro-LD, including pain reduction, functional recovery, and patient satisfaction, but incurred less bleeding loss, a shorter hospital stay, less postoperative pain, early functional recovery, and required a less demanding learning curve.14-17 Although RLD assisted with the BE technique (BE-RLD) has recently been introduced, clinical evidence of BE-RLD is still lacking. 18 The purpose of this study was to compare the clinical outcomes of BE-LD and BE-RLD.
Methods
Study Design and Patient Population
This retrospective study of prospectively collected data was conducted on 81 consecutive patients who underwent BE-LD or BE-RLD between March 2018 and June 2019. Magnetic resonance imaging (MRI) was performed prior to surgery in all cases to confirm LDH. RLDH was defined as a case in which lumbosacral radicular pain recurred after a pain-free period for more than 6 months after primary micro-LD, and a re-herniation in the same direction as in the past was observed on MRI. Eligible patients were 18 years or older, did not respond to more than one selective nerve root block, and had at least 12 months of postoperative follow-up. Patients with chronic discogenic pain without leg radicular pain and definite segmental instability combined with spondylolisthesis were excluded. The study protocol was approved by the University Institutional Review Board (IRB file no. 2020-12-018) and the study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants.
Surgical Procedure
All surgeries were performed by two spine surgeons (MSK and HJP) with more than 2 years’ experience in BE spine surgery. All surgical procedures and the postoperative protocol were carried out as directed in our previous work. 18 In particular, in the case of BE-RLD, where laminotomy was excessively performed in the primary LD, RLD was performed by exfoliating the epidural scar tissue from the vertebral lamina and inferior articular process without additional laminotomy (Supplementary Video Clip S1).
Measurement Data
Demographic and relevant medical history data, including sex, age, body mass index, and American Society of Anesthesiologists Physical Status Classification System (ASA class) were recorded. Clinical outcomes were analyzed using the VAS (a score of 0 indicated no pain and 10 represented the worst pain), the Oswestry Disability Index (ODI), and the modified MacNab’s criteria. The operation time (OT; skin to skin), length of hospital stay (LOS; the duration of the hospital stay after surgery), amount of surgical drain, surgery-related complications, and kinetics of serum creatine phosphokinase (CPK) and C-reactive protein (CRP) were recorded as secondary outcomes. The outcomes were assessed preoperatively and postoperatively at 2 days, and at 3, 6, and 12 months. In addition, surgery-related complications were collected.
Statistical Analysis
Patients were divided into 2 groups: group A (BE-LD) and group B (BE-RLD). All categorical data were compared using the chi-squared test, and independent t-tests were performed for comparison of continuous variables between the 2 groups. Analyses of perioperative data, the modified Macnab’s criteria, and surgery-related complications were performed using Fisher’s exact test. A P-value of less than or equal to .05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 26.0; SPSS, Inc, Chicago, IL, USA).
Results
Demographic and Preoperative Data.
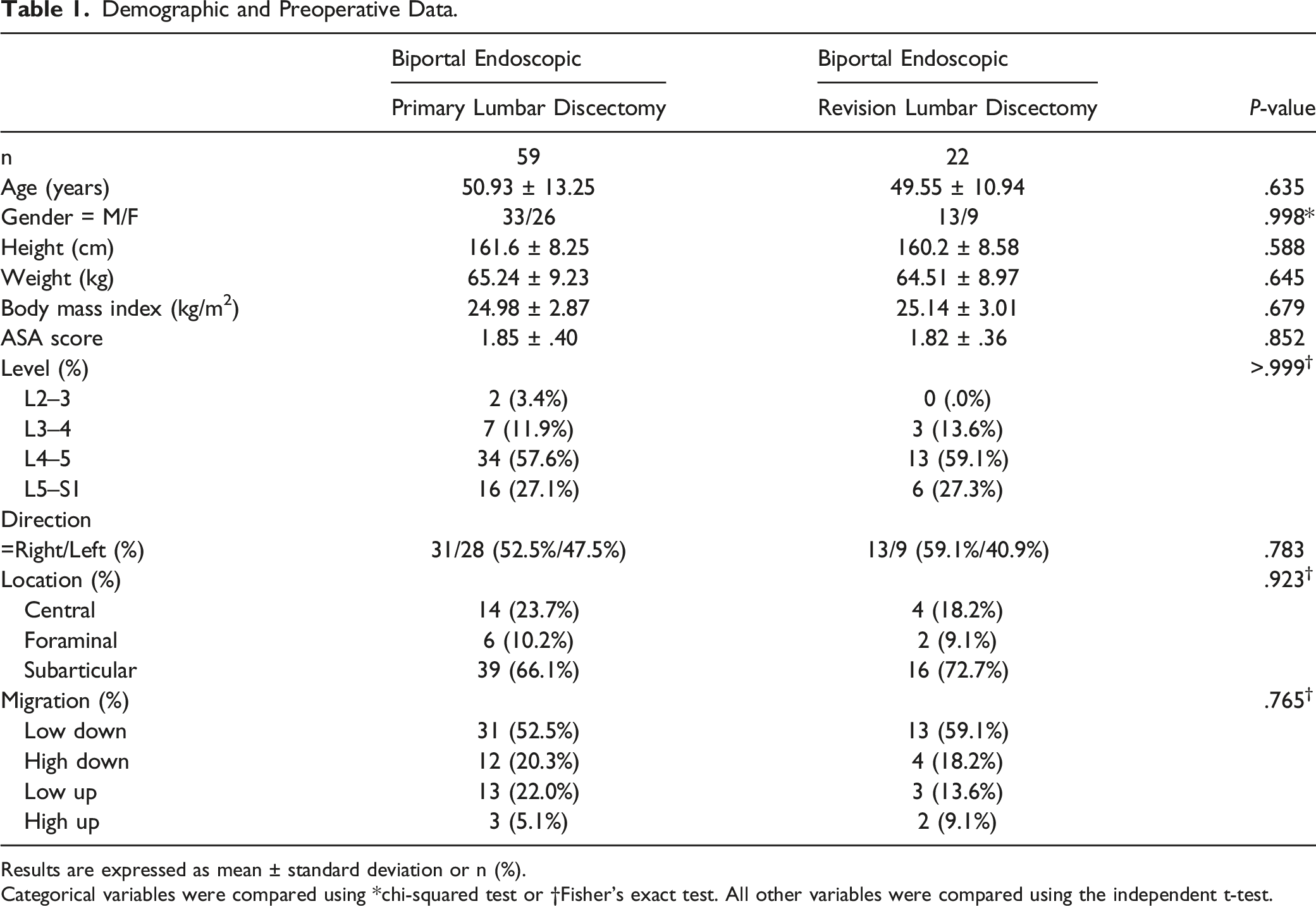
Results are expressed as mean ± standard deviation or n (%).
Categorical variables were compared using *chi-squared test or †Fisher’s exact test. All other variables were compared using the independent t-test.
Clinical Outcomes
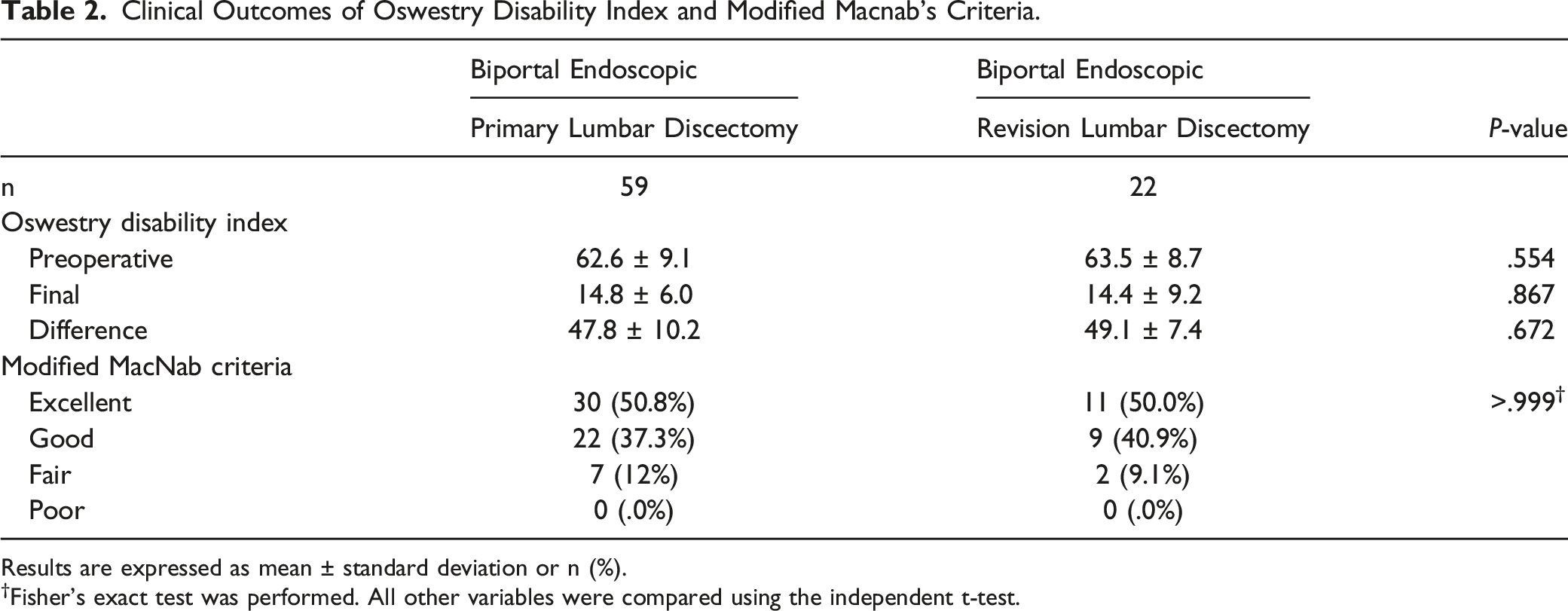
In both groups, the VAS scores improved significantly compared to the baseline values at 2 days after surgery, which lasted until the final follow-up (P < .05), and there was no difference in the VAS score between the 2 groups before and after surgery (P > .05) (Figure 1). In addition, the mean ODI score in group A was 62.6 ± 9.1 preoperatively and 14.8 ± 6.0 at 12 months after surgery. In group B, the mean ODI score was 63.5 ± 8.7 preoperatively and 14.4 ± 9.2 at 12 months after surgery. There was no difference in the improvement of ODI score between groups A and B (P = .672). During the entire follow-up period, both groups showed comparable outcomes of VAS and ODI scores (P > .05). According to the modified Macnab’s criteria on follow-up, 88.1 and 90.9% of the patients were excellent or good in groups A and B, respectively, and the results also showed that the two groups were comparable in the Macnab’s criteria (Table 2). Clinical outcomes as represented by the VAS scores. Graph showing no difference in the VAS scores between the biportal endoscopic primary and revision lumbar discectomy up to 1 year after surgery. VAS, visual analog scale; preop, preoperative; PO, postoperative. Clinical Outcomes of Oswestry Disability Index and Modified Macnab’s Criteria. Results are expressed as mean ± standard deviation or n (%). †Fisher’s exact test was performed. All other variables were compared using the independent t-test.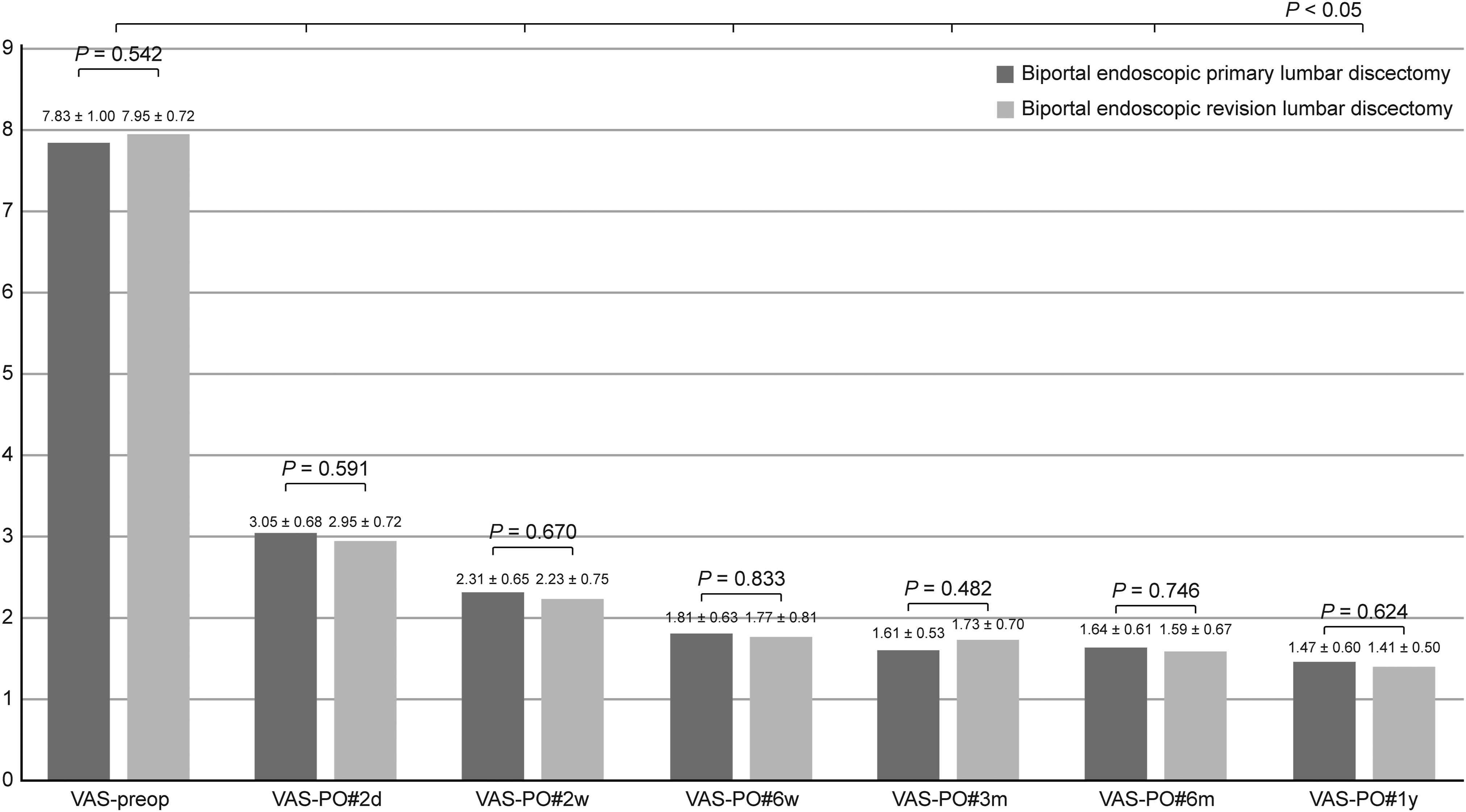
Operative Data, Laboratory Outcomes, and Complications
There were no significant differences between the 2 groups in terms of total operation time, the amount of surgical drain, and the LOS. Perioperative kinetics of serum CRP, lactate dehydrogenase, and CPK were comparable in both groups (P > .05), and the levels of CRP and CPK increased to the highest level on day 1 after surgery and recovered to the normal range on day 2 after surgery.
Operative Data, Laboratory Outcomes, and Complications.
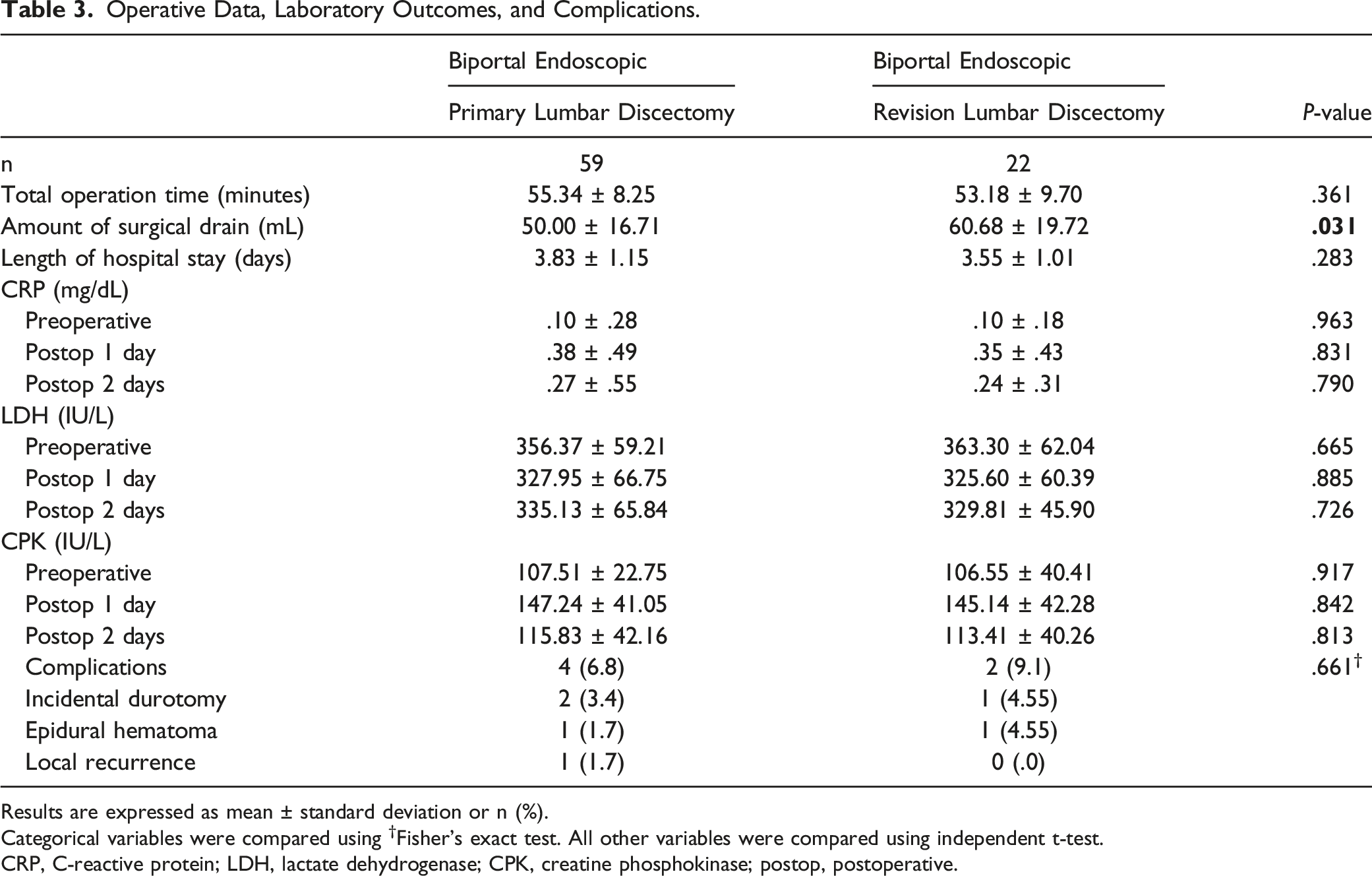
Results are expressed as mean ± standard deviation or n (%).
Categorical variables were compared using †Fisher’s exact test. All other variables were compared using independent t-test.
CRP, C-reactive protein; LDH, lactate dehydrogenase; CPK, creatine phosphokinase; postop, postoperative.
Discussion
This study showed the following results: (1) the BE technique delivers comparable and good clinical outcomes and patient satisfaction in both primary and recurrent LDH. In both groups, a significant improvement in VAS and ODI scores at each time point was observed during the 1 year postoperative follow-up compared to the preoperative values, and improvement of VAS and ODI scores were comparable in the 2 groups, (2) the kinetics of CRP and CPK recovered to the normal range 2 days after surgery, and showed no inter-group differences, and (3) the OT, LOS, amount of surgical drain, and postoperative complications were not significantly different between the 2 groups.
Micro-LD is a predictable and successful surgical option. However, open decompressive laminotomy may damage the normal spinal structure, including the paraspinal musculature, vertebral posterior bony arch, and ligamentous complex, and it can cause secondary instability and persistent low back pain.19,20 Peridural fibrotic tissue is inevitably formed to make up for the deficit of ligamentum flavum and bone from the primary LD. However, there is usually minimal formation of fibrotic scar tissue between the facet joints and the dural sac left behind. In RLD, the medial border of the preserved facet articular processes and lateral margin of the peridural fibrotic tissue must be separated first to allow access to the ventral epidural space without nerve injury. Therefore, Micro-RLD often requires more extensive surgical dissection, more paravertebral muscle retraction, and additional resection of the vertebral posterior arch and facet joint due to the existence of peridural fibrotic tissue. These may lead to the risk of secondary instability and persistent postsurgical pain increases. This is the main reason why Micro-RLD is more difficult, increasing the risk of complications such as unintended durotomy and nerve injury leading to worse clinical outcomes than that of primary Micro-LD.
The BE technique for symptomatic LDH uses 2 independent trans-muscular tracts as viewing and working portals and has characteristics that allow continuous fluid irrigation through the fluid inflow channel within the endoscope sheath and working portal. In literature, the BE technique has been shown to have the following advantages: (1) magnified clear surgical images are provided in real time, (2) familiar surgical anatomy can be obtained without paravertebral muscle retraction, (3) free movement of the surgical view and dynamic handling of surgical instruments, (4) less thermal injury to the paravertebral musculature and systemic inflammation than using an electrocautery,21-23 and (5) efficient vascular cauterization without nerve injury can be obtained if there is bleeding in the microvasculature around the dural sac or in the blood vessels growing into the peridural fibrotic tissue. Furthermore, good clinical outcomes from these advantages have been reported in several studies.14,15,24,25 Kang et al. 15 reported in a retrospective review of 262 patients who had been diagnosed with symptomatic primary LDH that BE-LD exhibited satisfactory clinical outcomes regardless of the grade of disc migration. Park et al. 25 reported in a prospective randomized controlled study of 64 patients who underwent decompressive laminectomy that the BE technique was associated with more rapid pain recovery until 48 hours, lower opioid usage, and earlier discharge after surgery compared to mini-open microscopic surgery.
Similar to a previously published study, our study also observed early pain relief and functional recovery after BE-LD. In addition, good clinical outcomes were also observed in BE-RLD, which were comparable to that of BE-LD. In the authors’ experience, the biportal endoscopic trans-muscular approach, with fascio-muscular release using an arthroscopic tissue shaver and tissue cauterization using a bRFa (bipolar Radio Frequency ablator). Helped identify and preserved the facet articular process and peridural fibrotic tissue without excessive muscle dissection and retraction, and allowed relatively easy access to the ventral epidural space using a dissector or small curved curets. Furthermore, it was estimated that surgical invasiveness of BE-RLD would be comparable to BE-LD.
Choi et al. 26 prospectively evaluated the surgical invasiveness of LD based on Micro, uniportal endoscopic, and BE techniques through the kinetics of CPK and CRP, and reported that the endoscopic discectomy technique was less invasive than microscopic discectomy. In particular, the kinetics of CPK and CRP showed a characteristic increase-and-decrease pattern. The CPK levels reached a maximum on postoperative day 1 and returned to the normal range on postoperative day 3 in all the surgical techniques. The CRP levels reached a maximum on postoperative day 3 and returned to the normal range on postoperative day 5 using endoscopic techniques but returned to the normal range on postoperative day 7 using the Micro technique. The uniportal endoscopic technique was reported to show significantly lower variation in CPK and CRP levels than the BE technique (CPK: P = .038, CRP: P = .04) as well as the Micro technique (CPK, P < .01; CRP, P < .01). In our study, the kinetics of CPK and CRP also showed a characteristic increase-and-decrease pattern. Unlike this previous report, however, both CPK and CRP levels in our study reached a maximum on postoperative day 1 and returned to the normal range on postoperative day 2 in both groups.
Creatine phosphokinase is known to be an indicator of muscle injury and is strongly associated with surgical invasiveness. 27 The kinetics of CPK are known to be related to retraction pressure and retraction time of the posterior spinal approach. 28 In addition, CRP reflects the acute postoperative systemic inflammatory response, and the peak response is affected by the amount of iatrogenic tissue injury and blood loss during surgery and by the wound healing process of surgery-related paravertebral muscle injury accompanied by exudate postoperatively.29-32 In spine surgery, the kinetics of perioperative CRP depends on the type of surgery.26,30 Therefore, our results suggest that the BE technique uses 2 independent trans-muscular tracts that do not require prolonged retraction time and excessive retraction pressure of the paravertebral musculature, and that the BE technique causes less postoperative systemic inflammatory response than the Micro technique. In particular, BE-RLD had comparable kinetics of CPK and CRP to BE-LD. The results indicated that the BE technique, regardless of primary and revision LD, caused less iatrogenic muscle injury, reduced postoperative inflammatory response, and related disability.
This study has certain limitations. First, our study involved a small sample size and a short follow-up period. Second, there was heterogeneity in the type and length of conservative treatment, such as oral medication, physical therapy, and selective nerve root block, conducted on all participants prior to surgery. Third, radiological data regarding segmental instability and alignment was not considered. Lastly, the baseline conditions of the patients were quite different in those with primary and recurrent lumbar disc herniation. However, in our previous study of Micro-RLD and BE-RLD, although it is a technical note, the BE-RLD showed equivalent outcomes to the Micro-RLD at 1 year after surgery, and it also showed that the BE-RLD had the advantage of early pain reduction and functional recovery. 18 Therefore, this study was conducted to evaluate the feasibility and effectiveness of the BE technique in the treatment of both symptomatic primary and recurrent LDH. Furthermore, this study had the strength of confirming that clinical indices and biomarkers of BE-LD ad BE-RLD achieved equivalent results. A prospective randomized controlled trial with a longer follow-up period and a larger sample size is necessary to provide more helpful information on the assessment of the BE technique for symptomatic LDH.
Conclusion
This study compared the outcomes of the BE technique for primary and recurrent LDH. Both BE-LD and BE-RLD were associated with less postoperative pain, acceptable functional recovery, and greater patient satisfaction. In addition, the BE technique had the advantages of less paravertebral muscle injury and less systemic inflammation in the perioperative period. Therefore, it can be considered that the BE technique is an effective treatment option for RLDH.
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.