
Abstract
Study Design
Retrospective Comparative Study.
Objectives
To compare the outcomes of microendoscopic discectomy (MED) versus full-endoscopic discectomy (FED) for treating L4/5 lumbar disc herniation (LDH).
Methods
A retrospective study was performed on patients with L4/5 LDH treated using MED (n = 249) or FED (n = 124). A 16-mm tubular retractor and endoscope was used for MED, while a 4.1-mm working channel endoscope was used for FED. Patient background and operative data were collected. The Oswestry Disability Index (ODI) and European Quality of Life-5 Dimensions (EQ-5D) scores were recorded preoperatively and at 1 and 2 years postsurgery.
Results
The background data of the two groups were similar. The mean operation times for MED and FED were 59.3 and 47.7 min (respectively), and the mean volumes of removed nucleus pulposus were .65 and 1.03 g, respectively. These differences were significant (P < .001). Six dural tears and one postoperative hematoma were observed in the MED group; none were observed in the FED group. During the follow-up period, 16 MED and 7 FED patients required re-operation due to recurrence (P = 1.00). Although the ODI and EQ-5D scores significantly improved at 1 and 2 years postsurgery in both groups, the differences were not statistically significant.
Conclusions
Operative outcomes were almost identical in both groups. We did not observe any operative or postoperative complications in FED. We, therefore, recommend FED as the first option for the treatment of L4/5 LDH since it has a better safety profile and is minimally invasive.
Keywords
Introduction
Several strategies are available for the treatment of lumbar disc herniation (LDH). Among these, microendoscopic discectomy (MED) and full-endoscopic discectomy (FED) are widely used in Japan, and the use of FED has been gradually increasing. The most recent annual report from the Japanese Orthopedic Society shows that the number of FEDs performed annually has reached approximately half that of MED [FED = 3499 cases, MED = 6884 cases]. 1 FED is an operative approach for uniportal full-endoscopic spine surgery (FESS). 2 In contrast, MED is a combination of endoscopy and tubular surgery. 3 The latter belongs to the group of “endoscopy-assisted surgeries,” together with unilateral biportal endoscopic (UBE) surgery, as seen in the recent classification proposed by AOSpine. 4
FED seems to be more minimally invasive than MED; not only does it use a smaller skin incision, it also causes less damage to muscle and requires the removal of a smaller quantity of bone tissue. Most recently, 1- and 2-year postoperative results of MED and FED were reported in a prospective randomized controlled study by Chen et al5,6; therein, the superiority of FED regarding clinical outcomes and safety was not shown. Furthermore, FED showed inferior results regarding median disc herniation. These findings are completely contradictory to what we have noted in our personal experience. Specifically, FED via the transforaminal approach (TELD, transforaminal endoscopic lumbar discectomy) seems to be suitable for large central LDH. 7 Previous studies regarding the operative outcomes for the treatment of LDH did not distinguish the different types of LDH. Therefore, in this study, we compared operative outcomes between FED and MED only for L4/5 LDH, the most frequent site of LDH. In addition, we excluded intra- and extraforaminal LDHs because of the distinct superiority of FED over MED in these forms of LDH. 8 To the best of our knowledge, this is the first comparative study on the treatment of L4/5 intracanal LDH between MED and FED.
Material and Methods
Patient Selection
A total of 900 consecutive patients with L4/5 LDH who underwent discectomy using the METRx endoscopic system (Medtronic Sofamor Danek, Memphis, TN, USA) or using a 4.1-mm working channel endoscope (RIWOspine GmbH, Knittlingen, Germany), between January 2016 and March 2020, were recruited. All patients had an apparent L5 radiculopathy resistant to medical treatment, epidural steroids, and/or nerve blocks. All patients underwent discectomy only at the L4/5 vertebral level. Foraminal and extraforaminal LDH were excluded because FED has a distinct advantage over other posterior approaches (open, microscopic, and microendoscopic) in these types of LDH. We also excluded patients in whom we could not distinguish whether the radiculopathy was caused by combined L4/5 lumbar spinal canal stenosis (LSCS) or other diseases (infection, discal cyst, and progressive supranuclear palsy). Two hundred thirty-six patients in the MED group and 132 patients in the FED group were excluded because of difficulties in obtaining follow-up data (Figure 1). Flow diagram of the study design. Abbreviations: MED, microendoscope discectomy; FED, full-endoscopic discectomy.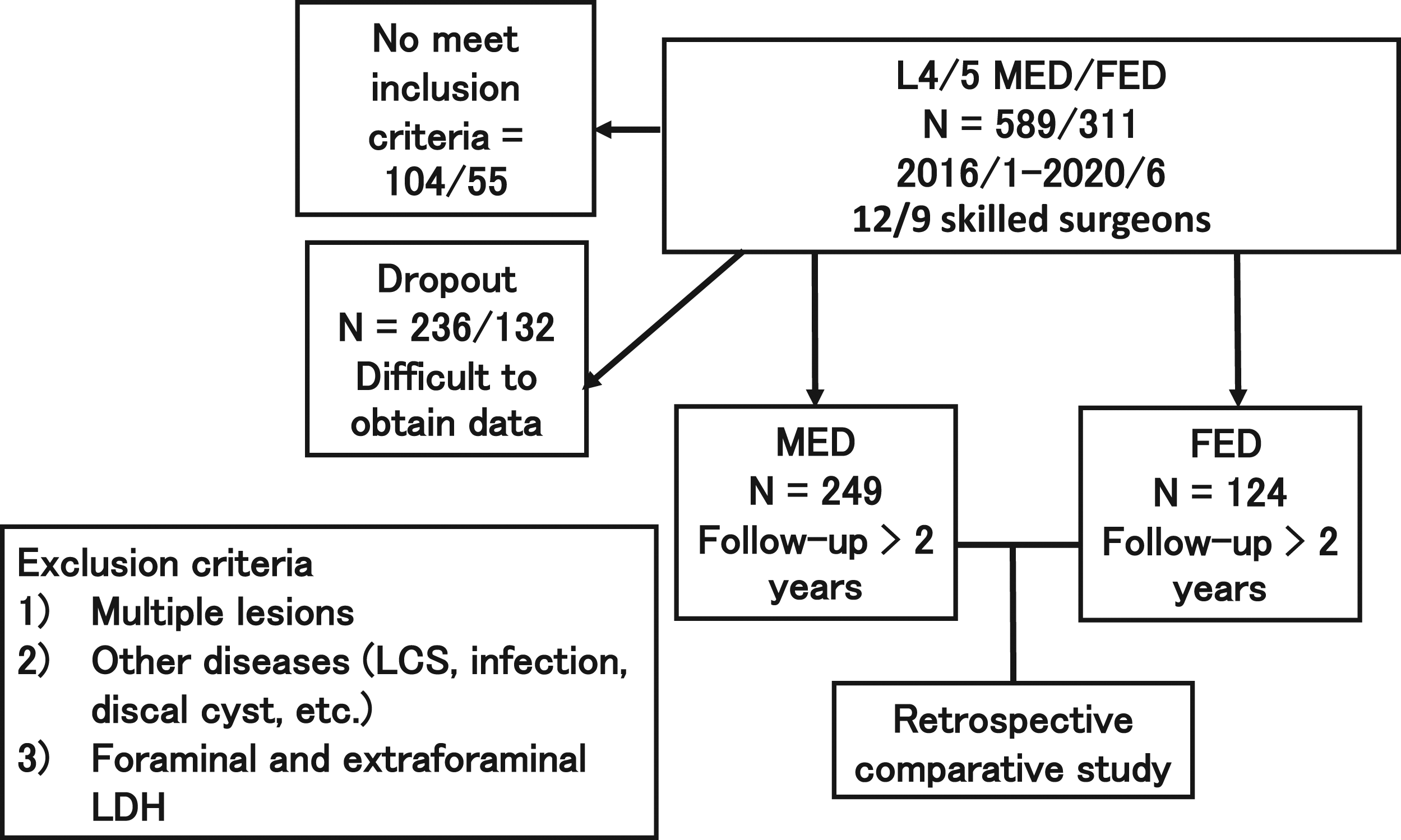
All procedures involving human participants were in accordance with the ethical standards of the research committee of the Iwai Medical Foundation (IRB approval No. 20200507) and with the 1964 Helsinki Declaration. Informed consent was obtained from the disclaimer documents of the surgical procedure handed over to the patients.
Data Collection
Demographic Data and Magnetic Resonance Imaging Findings of 373 Patients.
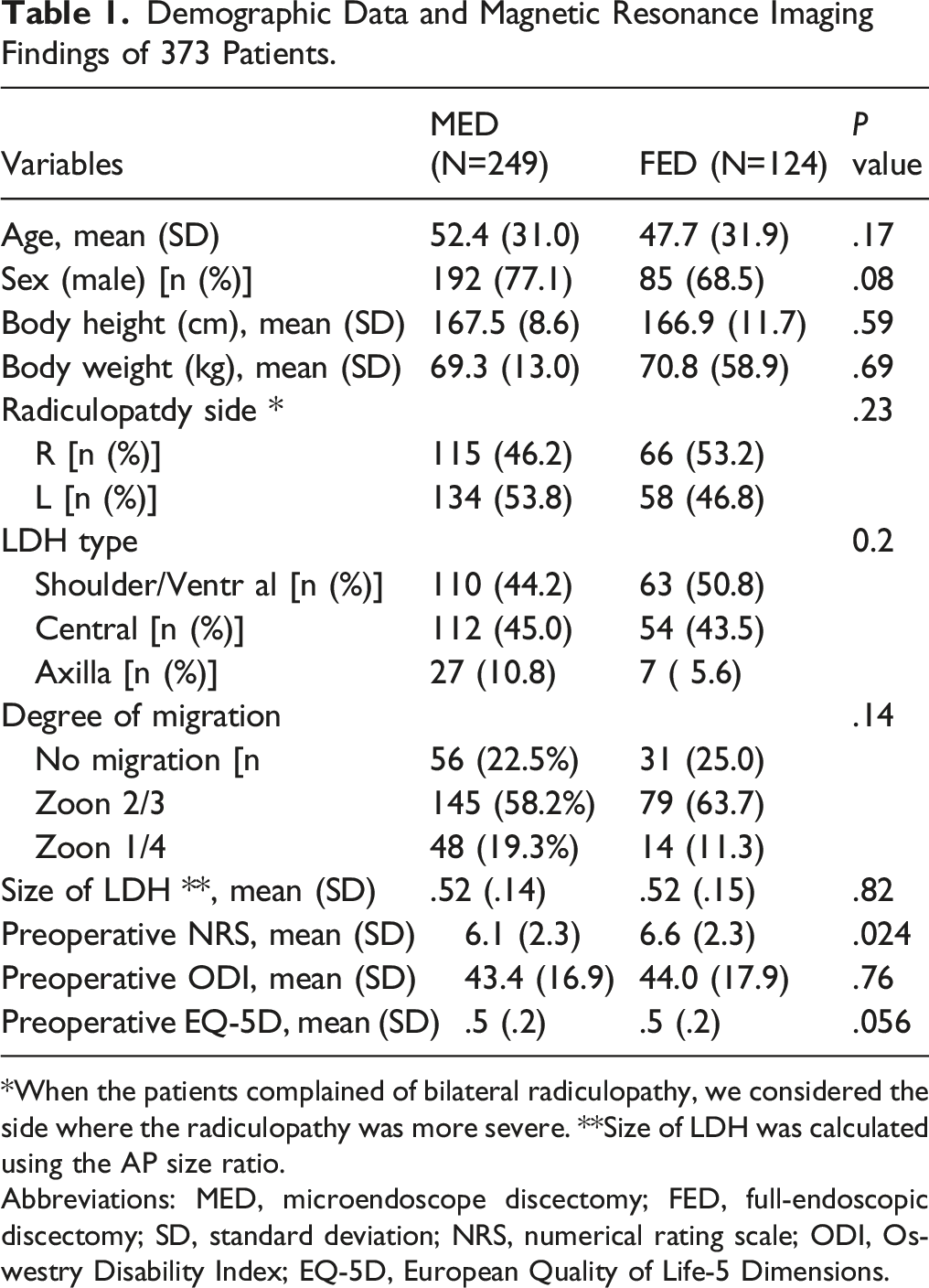
*When the patients complained of bilateral radiculopathy, we considered the side where the radiculopathy was more severe. **Size of LDH was calculated using the AP size ratio.
Abbreviations: MED, microendoscope discectomy; FED, full-endoscopic discectomy; SD, standard deviation; NRS, numerical rating scale; ODI, Oswestry Disability Index; EQ-5D, European Quality of Life-5 Dimensions.
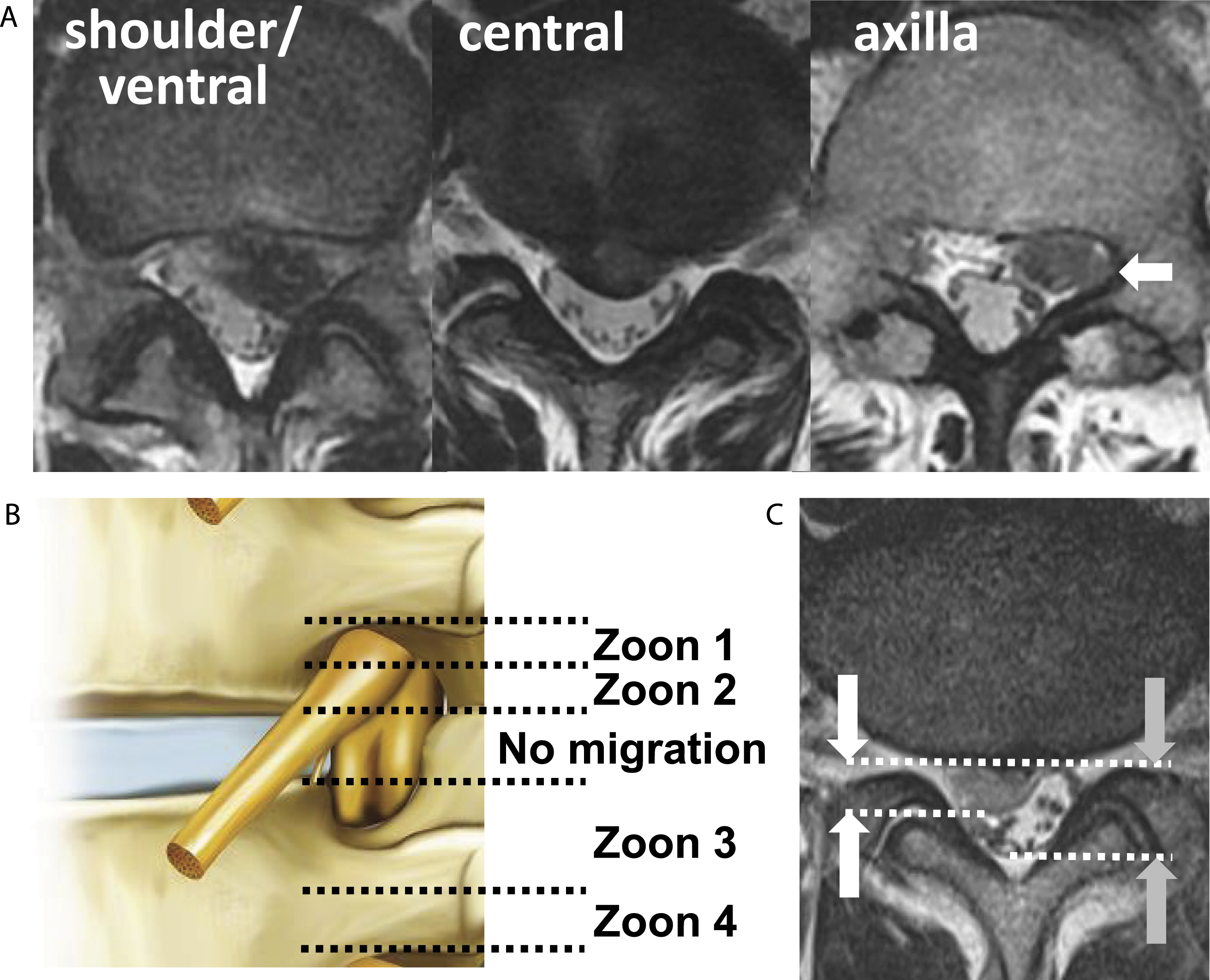
Preoperative radiographic findings on the characteristics of the LDH (LDH type, degree of migration, and size of LDH).
Univariate analysis of Operative Outcomes.
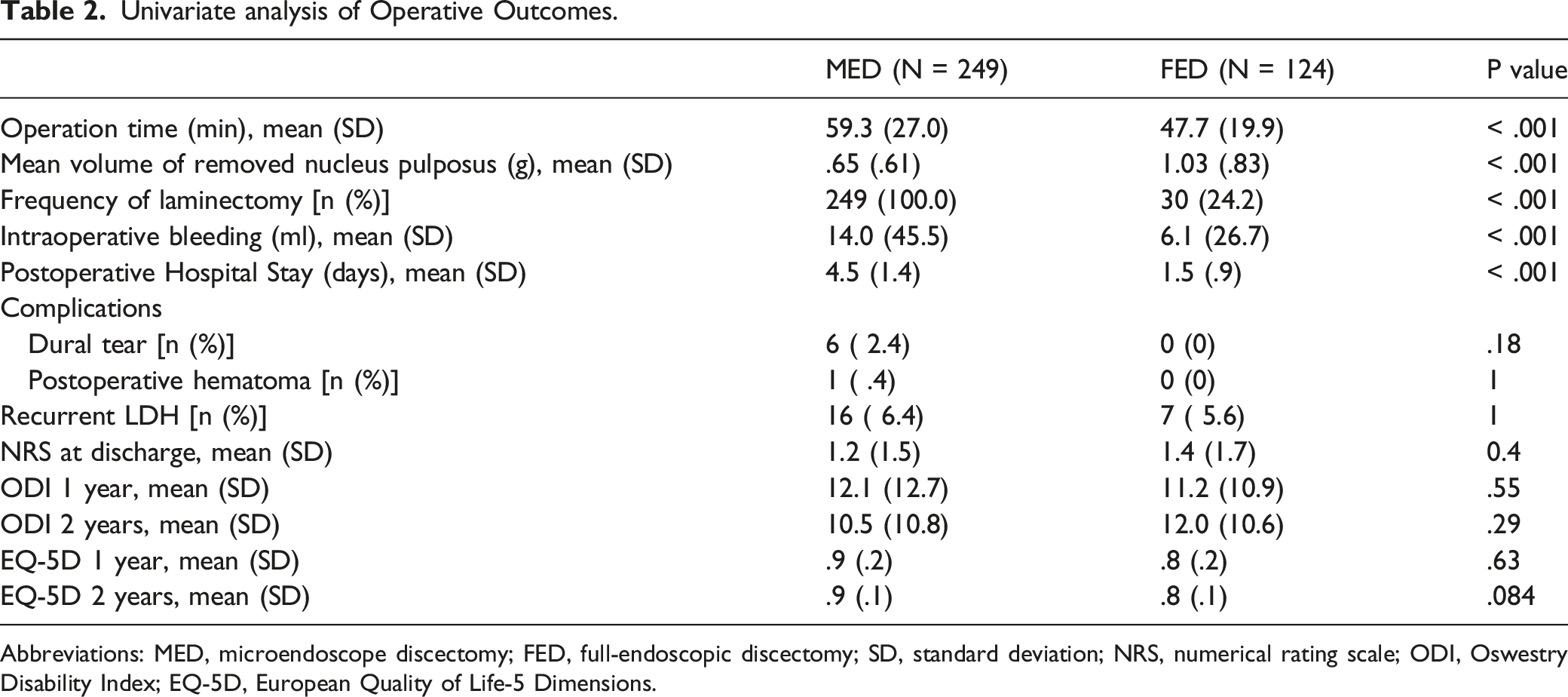
Abbreviations: MED, microendoscope discectomy; FED, full-endoscopic discectomy; SD, standard deviation; NRS, numerical rating scale; ODI, Oswestry Disability Index; EQ-5D, European Quality of Life-5 Dimensions.
Statistical Analysis
Demographic data and outcome measures were compared between the two groups using the t-test (for continuous variables) and chi-square test (for categorical variables). Following categories were used for the analysis for the intraoperative bleeding: ≦ 5ml, 5 - 10ml, 10 - 100ml, and > 100ml. Pre- and postoperative outcome measures were compared using the paired t-test. Multiple linear regression was used to determine the influence of the type of operative procedure on the postoperative ODI and EQ-5D scores. We made adjustments for potential confounding factors such as age, sex, and each preoperative measure. All analyses were performed using STATA version 16.0 (Stata Corp. LLC, College Station, TX, USA). Statistical significance was defined as a two-sided P-value < .05.
Surgical Technique
Patients were carefully logrolled to the prone position. Both MED and FED surgeries were performed under general anesthesia combined with motor-evoked potential monitoring. During the operation, a fluoroscope was placed across the center of the operating table to ensure appropriate timing.
Twelve skilled surgeons performed the MED surgeries. They had more than 5 years of experience of spinal surgery and had received advanced training in MED. An 18-mm skin incision was made 10 mm lateral to the midline for discectomy. The basic operative procedure has been described previously.3,13
Nine skilled surgeons performed FED using a 4.1-mm working channel endoscope. They had more than 5 years of experience of spinal surgery and had received advanced training in FED. The FED group comprised 19 cases (15.3%) of interlaminar approach (IELD, interlaminar endoscopic lumbar discectomy) and 105 cases (84.7%) of the TELD outside-in technique. Although we unified IELD and TELD to increase the number of FED group, we could not find much differences between IELD and TELD (under the manuscript preparing). An 8-mm skin incision was made 5-10 mm lateral to the midline (for the IELD) or 80-120 mm lateral to the midline (for the TELD). The basic operative procedure has been previously described.7-9
Results
The demographic data of the patients are summarized in Table 1. This retrospective study included 249 and 124 L4/5 LDH patients in the MED group (192 men, 57 women) and FED group (85 men, 39 women), respectively. The mean age at surgery was 52.4 years in the MED group and 47.7 years in the FED group. The mean body height and weight were 167.5 cm and 69.3 kg (in the MED group), and 166.9 cm and 70.8 kg (in the FED group), respectively. There were no statistically significant differences in patient backgrounds between the MED and FED groups. We also compared the preoperative MRI findings between the two groups and found no significant differences in terms of LDH type, degree of migration, and size (Table 1).
There was a significant difference in the mean operation time between the MED group (59.3 ± 27.0 min) and FED group (47.7 ± 19.9 min) (P < .001), as well as in the mean volume of removed nucleus pulposus (.7 ± .6 vs 1.0 ± .8 g; P < .001). Furthermore, there was a significant difference in the frequency of laminectomy between the MED and FED groups (100.0% vs 24.2%; P < .001; Table 2). There was a significant difference in the mean intraoperative bleeding between the MED group (14.0 ± 45.5 ml) and FED group (6.1 ± 26.7 min) (P < .001). Regarding complications, in the MED group, dural tears occurred in six patients, and one patient required readmission for postoperative hematoma; however, no complications were observed in the FED group. During the first 2 years postsurgery, reoperation for recurrent LDH was performed in 16 patients (6.4%) in the MED group and 7 patients (5.6%) in the FED group. However, there were no significant differences in complications or recurrence between the two groups.
The NRS score was used to evaluate early effects on the patients’ leg pain. The preoperative NRS score (6.1 ± 2.3) in the MED group improved significantly postoperatively (1.2 ± 1.5; P < .001). The preoperative NRS (6.6 ± 2.3) in the FED group also improved significantly postoperatively (1.4 ± 1.7; P < .001). However, there was no significant difference in leg pain evaluation at discharge between the MED and FED groups.
The preoperative ODI score in the MED group (43.4 ± 16.9) improved significantly after 1 year following the surgery to 12.1 ± 12.7 (P < .001) and remained approximately the same after 2 years (10.5 ± 10.8). The preoperative EQ-5D score in the MED group (.5 ± .2) also improved significantly postoperatively to .9 ± .2 (P < .001) after 1 year and remained approximately the same after 2 years (.9 ± .1). The preoperative ODI scores in the FED group (44.0 ± 17.9) improved significantly postoperatively to 11.2 ± 10.9 (P < .001) after 1 year and remained approximately the same after 2 years (12.0 ± 10.6). The preoperative EQ-5D score in the FED group (.5 ± .2) also improved significantly postoperatively to .8 ± .2 (P < .001) after 1 year and remained approximately the same after 2 years (.8 ± .1). However, the ODI and EQ-5D scores at each time point were not significantly different between the two groups.
Multivariate Analysis of Postoperative ODI after 1- and 2-Year Follow-Up.
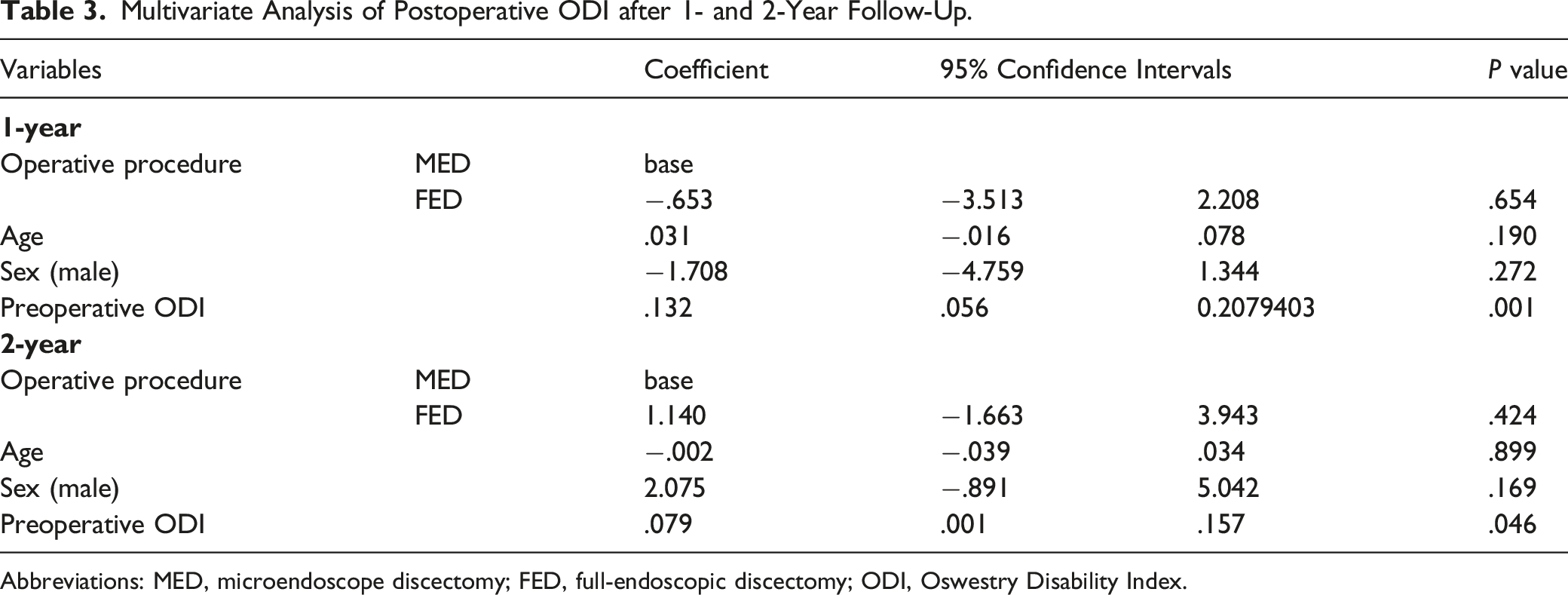
Abbreviations: MED, microendoscope discectomy; FED, full-endoscopic discectomy; ODI, Oswestry Disability Index.
Multivariate Analysis of Postoperative EQ-5D after 1- and 2-year follow-up
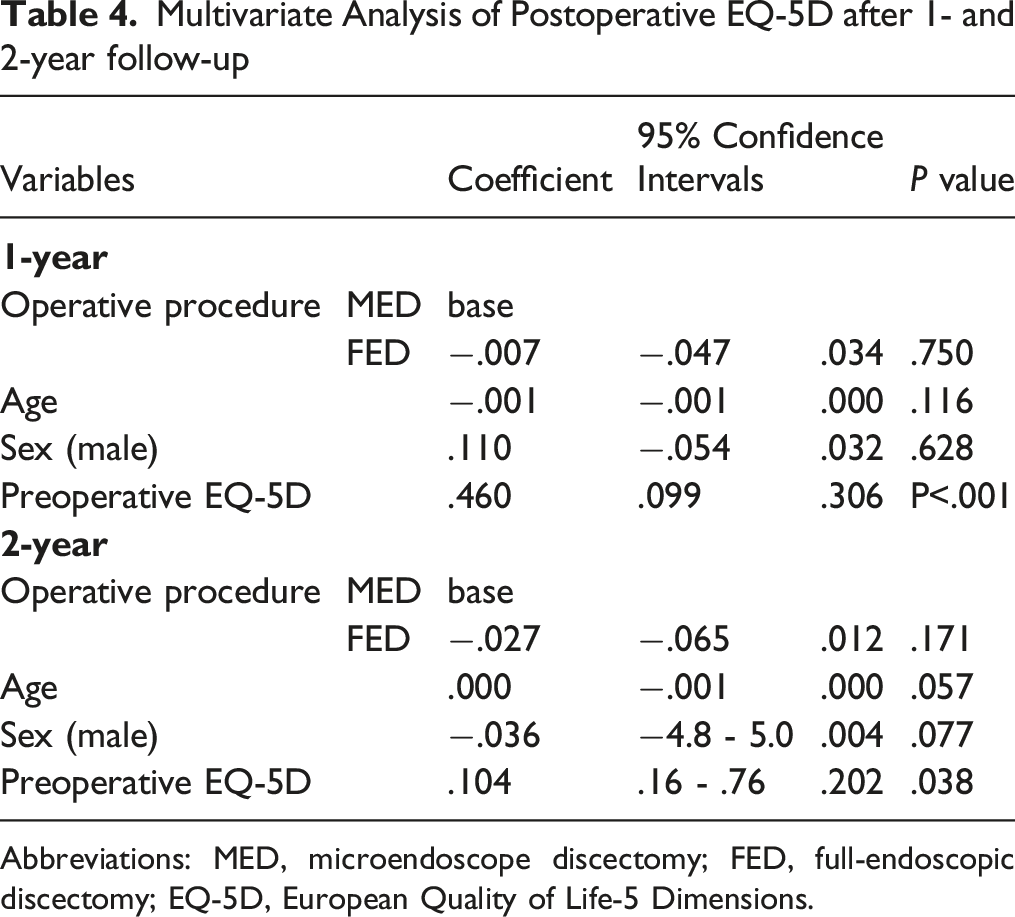
Abbreviations: MED, microendoscope discectomy; FED, full-endoscopic discectomy; EQ-5D, European Quality of Life-5 Dimensions.
Discussion
Although several meta-analyses comparing the outcomes of FED with those of MED have already been reported, findings regarding the complications and recurrence rates remain controversial.14-20 The previous comparative studies between MED and FED involved different types and vertebral levels of LDH.5,6,21-24 Depending on the type and level of LDH, the treatment strategy differs. It is, therefore, necessary to analyze LDH differently according to the type of LDH and the vertebral level affected. Therefore, in the present study, we focused on L4/5 intracanal LDH (which is the most common type of LDH) and compared the operative outcomes of MED and FED. Before comparing the outcomes, we also confirmed that there were no differences between the two groups in terms of characteristics of the LDH (LDH type, degree of migration, and size of LDH) as well as patient background data (age, sex, body height, body weight, and radiculopathy side).
Our analysis showed that FED was superior in terms of operation time (shorter), safety profile (safer), and invasiveness (minimal). We could show that the intraoperative bleeding of FED was significantly reduced to that of MED in this study, FED was also superior as far as this parameter was concerned. These findings are in line with those of previous studies.23-25 Although not statistically significant, FED might prevent complications such as dural tears and hematoma. More than 100 mL of intraoperative bleeding was observed in 9 MED cases, and hemostasis was observed; however, we did experience such bleedings in only 1 FED. The fact that FED is minimally invasive to the surrounding tissues (bone, muscle, and ligament) might affect not only the operation time but also contribute to reduce the number and the severity of complications.
In terms of early operative outcomes, we evaluated NRS scores at admission and discharge. We did not find any differences in NRS scores at discharge between the MED and FED groups; however, the discharge data were average 1.5 days after the operation for FED, meanwhile the data for MED corresponded to data at average 4.5 days after the operation. Considering these differences, FED appears to have better early operative outcomes.
In terms of long-term operative outcomes, we evaluated the ODI and EQ-5D scores at 1 and 2 years postsurgery. Although the ODI and EQ-5D scores significantly improved in both groups at 1 and 2 years postsurgery, we did not find any significant differences at any point in time, regarding these scores between the two groups. Furthermore, we did not find a significant difference in the recurrence rate of LDH during the 2-year follow-up period between the two groups. The previously reported recurrence rate for LDH is 1.1-23.9 %; our results are within these previous ranges.26-28 We can, therefore, conclude that the long-term operative outcomes of FED are the same as those of MED. Chen et al conducted a prospective randomized controlled study comparing MED (n = 122) and FED (n = 119)5,6 and showed similar improvements in ODI and EQ-5D scores at 1 and 2 years postsurgery; they also found similar complication and recurrence rates in both groups. However, they concluded that FED had inferior results in median disc herniation (MDH) because 16.7% of the patients who had MDH in the FED group experienced residual or recurrent herniation. They also emphasized that incomplete removal of the LDH was more frequent in FED than in other operative procedures, based on their personal experiences (all of the six patients with residual herniation came from the FED group in their study) and data from other studies.2,29,30 Considering this point, we calculated the volume of the removed disc material and found that the volume was significantly higher in the FED group. In our study, incomplete removal of the LDH did not predominantly occur in the FED group. MED requires laminectomy and flavectomy, which have an external decompression effect on the appropriate nerve root. On the other hand, FED has lesser external decompression effect than that of MED. Our data indicate that if sufficient removal of LDH is achieved by FED, it will definitely not be inferior to MED.
Our study was neither a prospective study nor a multi-institutional study, nor completely matched comparative study. However, the patient background and LDH characteristics were matched as much as possible between the two groups, and the study focused on L4/5 intracanal LDH. Furthermore, we lost the follow-up of hundreds number of patients. These are limitations of this study. We could show the non-inferiority of FED over MED on both short- and long-term outcomes. Furthermore, we showed a potential advantage of FED regarding the reduction of operative complications such as dural tears and epidural hematomas.
Full-endoscopic spine surgery necessitates longer training for trainee surgeons to acquire the required surgical skills.31,32 However, anyone can acquire such skill; actually, all nine surgeons who performed FED in this study were trained by one skilled endoscopic spine surgeon. If the required skills are acquired, FED will be a better alternative to other conventional LDH surgeries.
Conclusions
This retrospective study with 1- and 2-year follow-up periods showed that long-term operative outcomes of MED and FED (using a 4.1-mm working channel) regarding L4/5 intracanal LDH were the same. In addition to requiring a shorter operation time, FED has potential advantages in terms of reduced operative complications (such as dural tear and epidural hematoma).
Footnotes
Acknowledgements
We thank all the operating room staff (for their technical assistance) and the medical records clerks (who helped in collecting patient data). We also thank the radiological department staff for recording the CT and MRI data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.