
Abstract
Study design
Retrospective cohort study.
Objectives
Despite several recognized risk factors, PJK remains a common postoperative occurrence in adult spinal deformity surgery. This study aims to identify a significant preoperative sagittal alignment parameter that is associated with vertebral loading at the proximal junction and can predict the likelihood of proximal junctional kyphosis (PJK).
Methods
Fifty-five consecutive patients who underwent fusion surgery from lower thoracic (T9-T11) to the pelvis were included in this retrospective study. Based on the preoperative slope of the level above the upper-instrumented vertebrae (UIV+1), patients were stratified into two groups: posterior and anterior UIV+1 slope. Patient-specific musculoskeletal (MSK) models were created from pre and immediate postoperative EOS images. Pre and postoperative radiographic parameters, and normalized vertebral loading at UIV and UIV+1 were compared.
Results
6/21 (28.6%) patients with posterior UIV+1 slope developed PJK, while the incidence of PJK for anterior UIV+1 slope was 24/34 (70.6%). Average normalized shear difference of UIV+1 in PJK and non-PJK patients was 0.19 and 0.1 for posterior slope patients, whereas for anterior slope patients, they were 0.3 and 0.18 respectively. Statistically significant associations were revealed between UIV+1 slope, shear force and risk of PJK development.
Conclusion
Utilizing mathematical and musculoskeletal analyses with clinical correlation, we were able to demonstrate UIV+1 slope as a local sagittal alignment risk factor that affects shear force at UIV/UIV+1, influencing PJK risk. Considering UIV+1 slope as a local alignment risk factor for PJK development may provide insight regarding UIV selection and alignment goals during preoperative planning.
Keywords
Introduction
Proximal junctional kyphosis (PJK) is a well-recognized postoperative complication following adult spinal deformity (ASD) correction surgery with reported prevalence of 20%-40%.1,2 Multiple factors have been reported in the development of PJK which makes it difficult to define the etiology and predict its development. More than twenty risk factors have been identified that predispose patients to PJK,3,4 which can be categorized into surgical, patient and alignment variables. Long posterior spinal fusion with extension to the pelvis increases the risk of PJK development, as well as a UIV located in the lower thoracic spine.5,6 Older age, higher body mass index, and lower bone mineral density are recognized patient risk factors.4,7 Controversy exists regarding planned surgical correction and resultant sagittal alignment parameters illustrating a gap in our understanding of PJK. Investigation into the dominant radiographic risk factors is ongoing.8-11
Although the effect of sagittal alignment on the development of PJK has been investigated widely, reciprocal changes following corrective surgery and the impact of local sagittal parameters may make it difficult to identify a specific parameter as a dominant alignment risk factor. Currently, different realignment criteria offer distinctly divergent recommendations based upon targeted global sagittal parameters. The concept of the UIV orientation as a dominant driver of PJK rather than the impact of the global alignment has been proposed.12-15 Regardless of a UIV location in the upper or lower thoracic spine, posterior slope and location of the UIV postoperatively have been identified as important risk factors for PJK.
While other studies have focused on post-operative UIV orientation, this study investigates the impact of both pre- and postoperative UIV and UIV+1 orientation. We hypothesized that UIV+1 slope has an impact on shear loading, and based on previous research, is associated with increased risk of PJK development. The aim of this study is to identify the local alignment parameters associated with PJK development using mathematical, musculoskeletal, and clinical assessments, and identify patient risk of PJK based on the pre and postoperative sagittal alignment.
Materials and Methods
Patients
Fifty-five consecutive adult spinal deformity patients from a single center [average age 64.9 (SD 10.5 yrs), 69.6% females] operated on with a posterior fusion from lower thoracic (T9-T11) to the pelvis were reviewed. The mean follow-up was 75 months. The minimum and maximum follow-up durations of 1.5 and 14 years. This study was conducted retrospectively using data obtained for clinical purposes. The requirement for informed consent was waived by the Institutional Review Board (No. 21-5873), as the research involved no direct patient interaction and posed minimal risk to participants. All data were anonymized prior to analysis to ensure patient confidentiality. Exclusion criteria consisted of patients with spinal deformities derived from ankylosing spondylitis, neuromuscular diseases, fracture, infections, or Scheuermann kyphosis. The images of the thoracolumbar spine were acquired in coronal and sagittal planes using EOS imaging system (EOS Imaging, Paris, France) pre-, immediate and final postoperatively or upon the occurrence of PJK.
The pre and postoperative sagittal spinopelvic radiographic parameters were studied. These parameters included pelvic incidence (PI), pelvic tilt (PT), pelvic incidence-lumbar lordosis mismatch (PI-LL), global tilt (GT), T1-pelvic angle (TPA), distal and total lumbar lordosis (ie, L4-S1 and L1-S1), lumbar pelvic angle (LPA), non-instrumented segment pelvic angle (C2-UIV+1PA) measured the angle between two lines connecting C2 to femoral head (FH) and UIV+1 to FH.
We stratified the patients based on their preoperative slope of UIV+1 into two groups: posterior and anterior UIV+1 slope (also including zero slope). The vertebral slope angle was quantified by measuring the angle between a line perpendicular to the superior endplate of the vertebra and a vertical reference line on a standing lateral radiograph. An anterior slope identifies where the anterior vertebral body is more caudal to the posterior vertebral body and the slope of the UIV is directed caudally, while a posterior slope relative to the vertical axis indicates where the posterior vertebral body is more caudal to the anterior vertebral body and the slope of the UIV is directed cranially. The incidence of PJK development and adjacent forces at UIV and UIV+1 were studied in both groups. PJK was defined as a change of 10° or more from pre to last follow-up postoperative image from UIV to UIV+2. 16 Two independent reviewers performed the radiographic assessments. Both reviewers were non-clinicians blinded to the clinical outcomes and group assignments during the evaluation process to minimize bias.
Musculoskeletal Model
An OpenSim musculoskeletal model that encompasses a fully articulated thoracolumbar spine was utilized.17-19 Patient-specific models were generated using standing EOS images taken before and immediately after surgery to estimate vertebral forces. Individualized musculoskeletal models were developed in OpenSim by scaling a generic spine according to each subject’s height, weight, sex, and spinal alignment captured from biplanar EOS images. An upright static posture was simulated by applying gravitational and muscle forces reflective of the subject’s body mass and sagittal spinal alignment. Muscle forces were estimated using inverse dynamics. A Hill-type muscle model was used, and muscle recruitment followed an optimization criterion minimizing the sum of muscle activations squared, which is a common and physiologically plausible assumption in MSK modeling. Simulations using OpenSim software were conducted for an upright standing static posture. Joint reaction analysis calculated for intervertebral joint loading which included compressive and shear forces at UIV and UIV+1 and were normalized relative to the patient’s weight. Shear forces were normalized, and defined as high vs low based on a threshold of 0.2. More detailed information on the modeling methodology and validation can be found in reference 20.
Statistical Analysis
Demographic and spinopelvic parameters were compared between PJK and non-PJK patients. A 2-sided independent t-test was utilized to obtain the difference between anterior and posterior slope groups with the level of significance set to 0.05. Continuous variables were expressed as mean ± standard deviation. Pearson Chi-square was utilized to test association of categorical variables ie, UIV+1 slope (posterior vs anterior) with PJK status and shear values (high vs low).
Results
Sagittal Radiographic Parameters
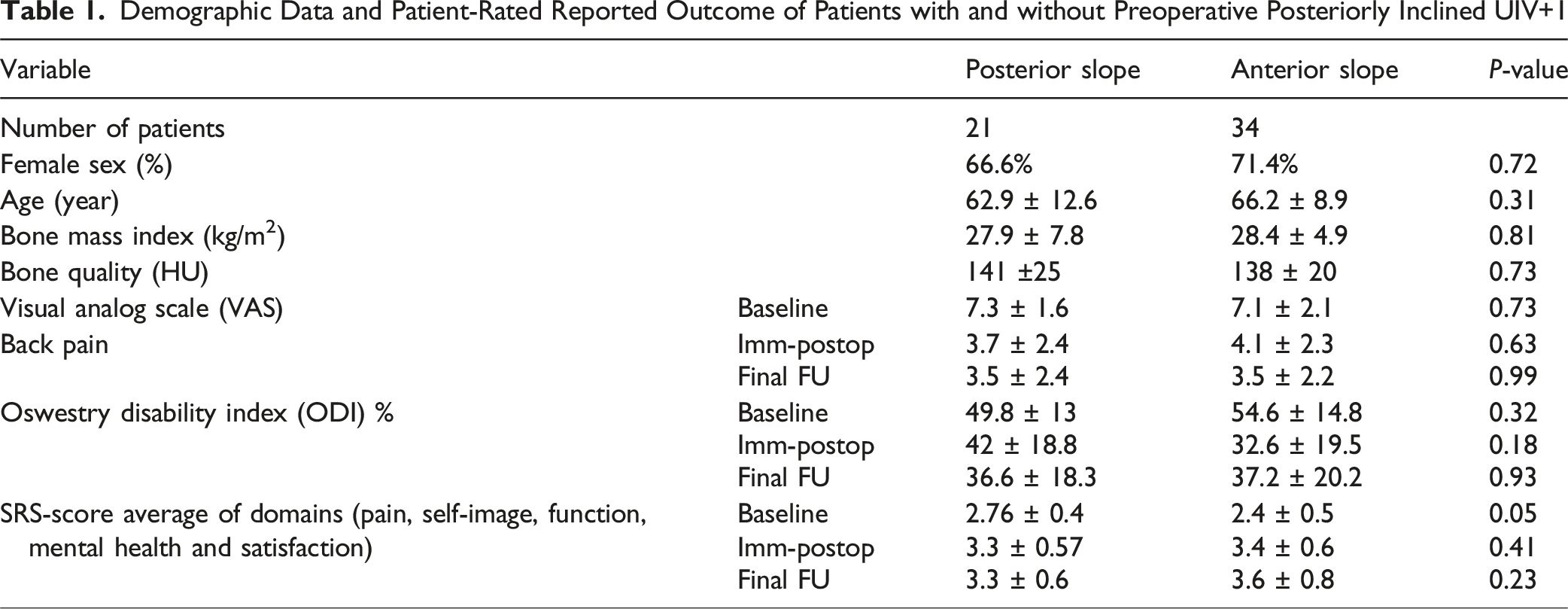
Demographic Data and Patient-Rated Reported Outcome of Patients with and without Preoperative Posteriorly Inclined UIV+1
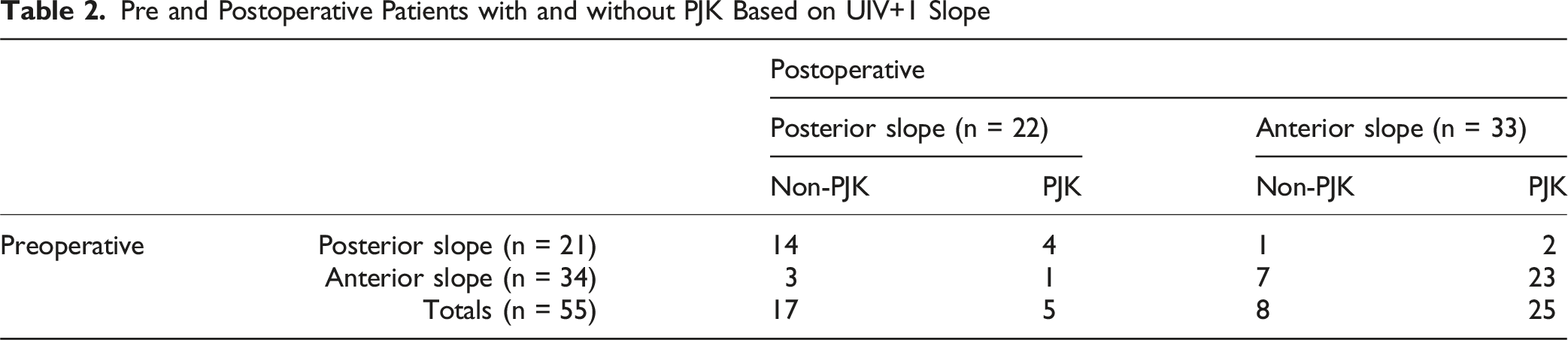
Pre and Postoperative Patients with and without PJK Based on UIV+1 Slope
Comparison of Pre and Postoperative Sagittal Radiographic Parameters Between Patients Based on Preoperative UIV+1 Slope
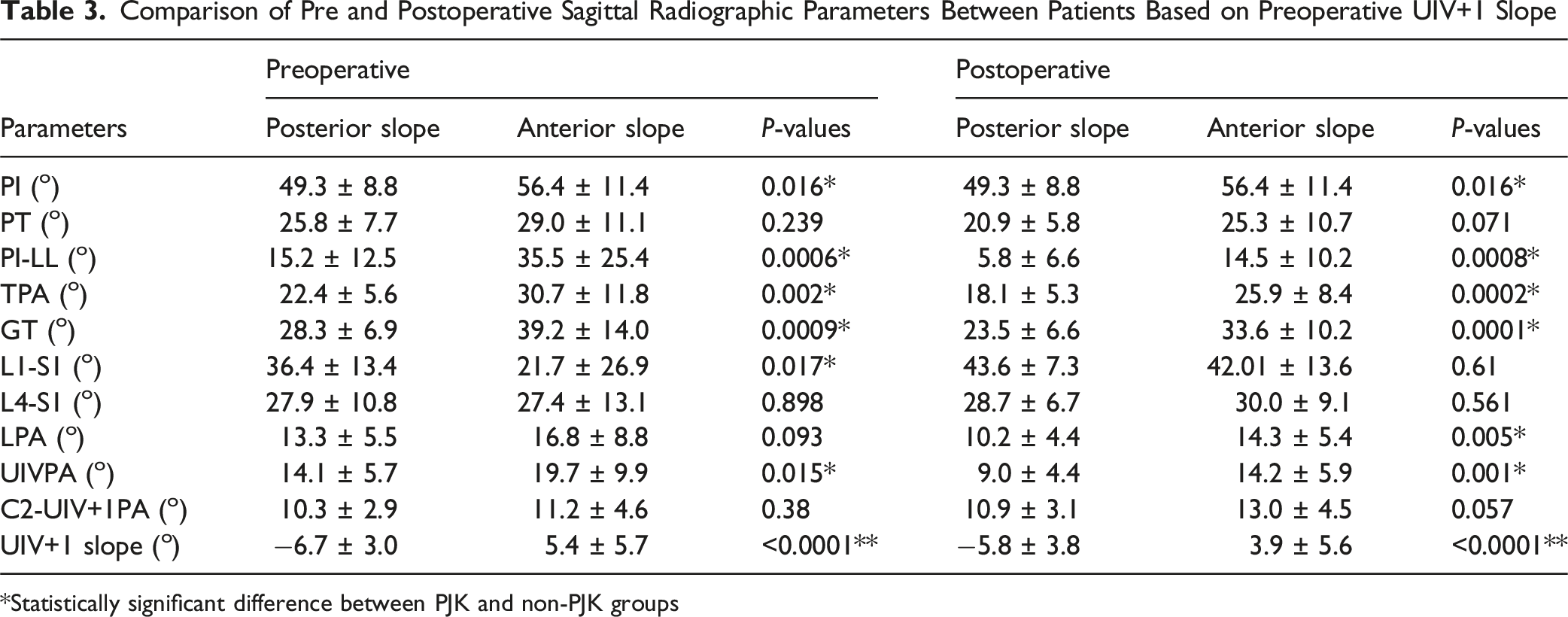
*Statistically significant difference between PJK and non-PJK groups
Analytical Correlation Between UIV+1 Slope and Location on Adjacent Forces
Using a simplified free body diagram of the non-instrumented segment from head to UIV+1 we found three possibilities regarding UIV+1 slope and location of gravity line (vertical line passing from C2) relative to UIV+1: anterior slope and anterior gravity line (Type I); posterior slope and anterior gravity line (Type II); posterior slope and posterior gravity line (Type III) (Figure 1). Analytically, the differences in UIV+1 slope and location contributes significantly to shear force, theoretically increasing the risk of PJK development. In Type I, the horizontal components of the head, neck, and upper thoracic weight, in addition to the muscle force components on the local horizontal coordinate of UIV+1, all act in the anterior direction, increasing the posteriorly directed shear force at the junction of UIV/UIV+1. In Type II, these forces act in opposite directions, balancing each other out. Whether the resulting shear force is anteriorly or posteriorly directed depends on the upper body weight and muscle force components The Schematic of Three configurations of UIV+1 Slope and Head Position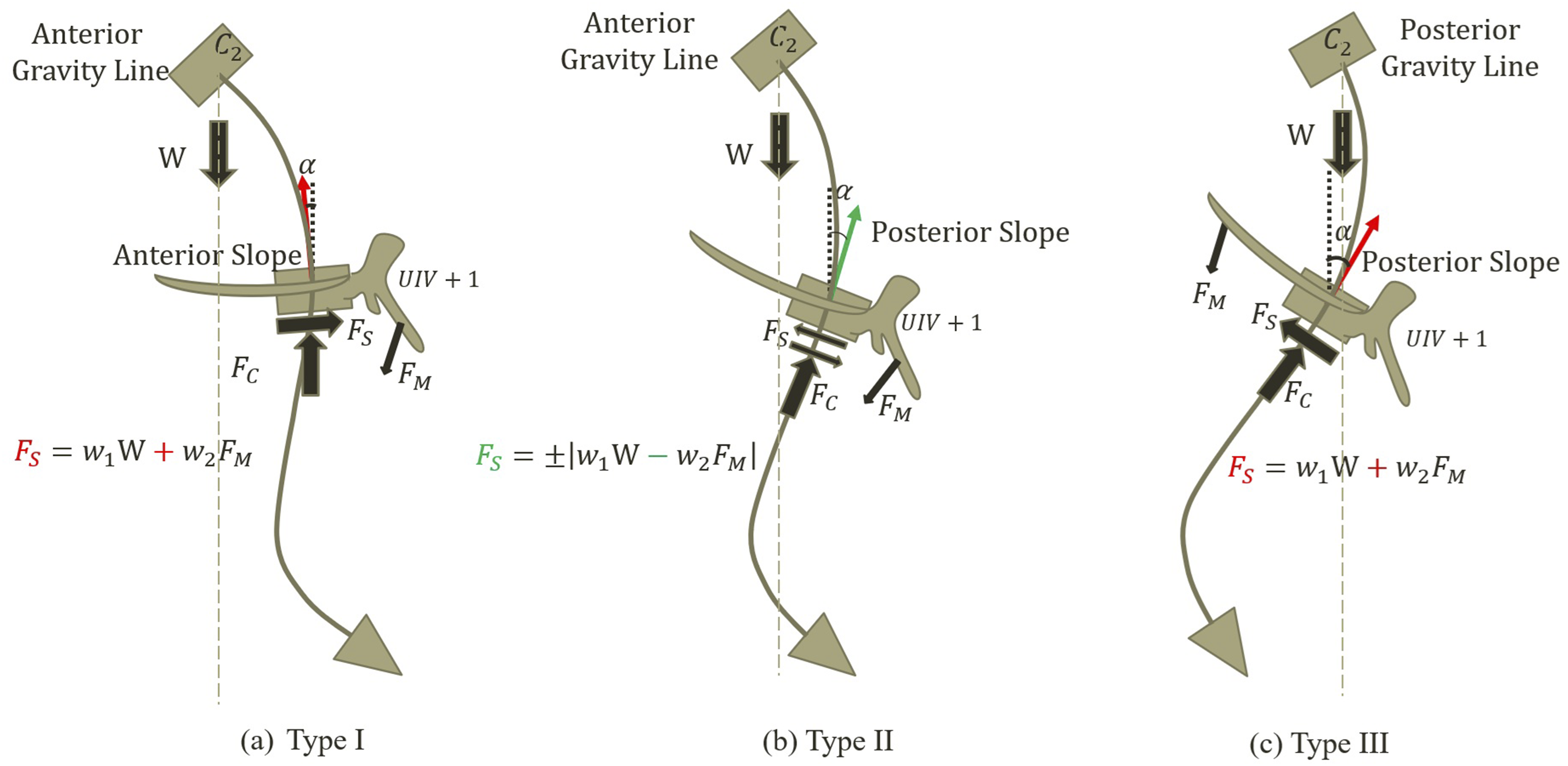
Figure 2 illustrates pre, immediate postop and follow up images of postoperative Type I and II cases. Figure 2A and 2B show Type I (anterior slope and anterior gravity line) cases with preoperative anterior and posterior UIV+1 slope who developed PJK, while Figure 2C and D include postoperative Type II (posterior slope and posterior gravity line) patients, which regardless of their preoperative slope status did not develop PJK. It is worth mentioning that we did not have Type III (posterior slope and posterior gravity line) cases in our study. Examples of Two Patient Types (I and II) Categorized by Their Preoperative and Postoperative UIV+1 Slope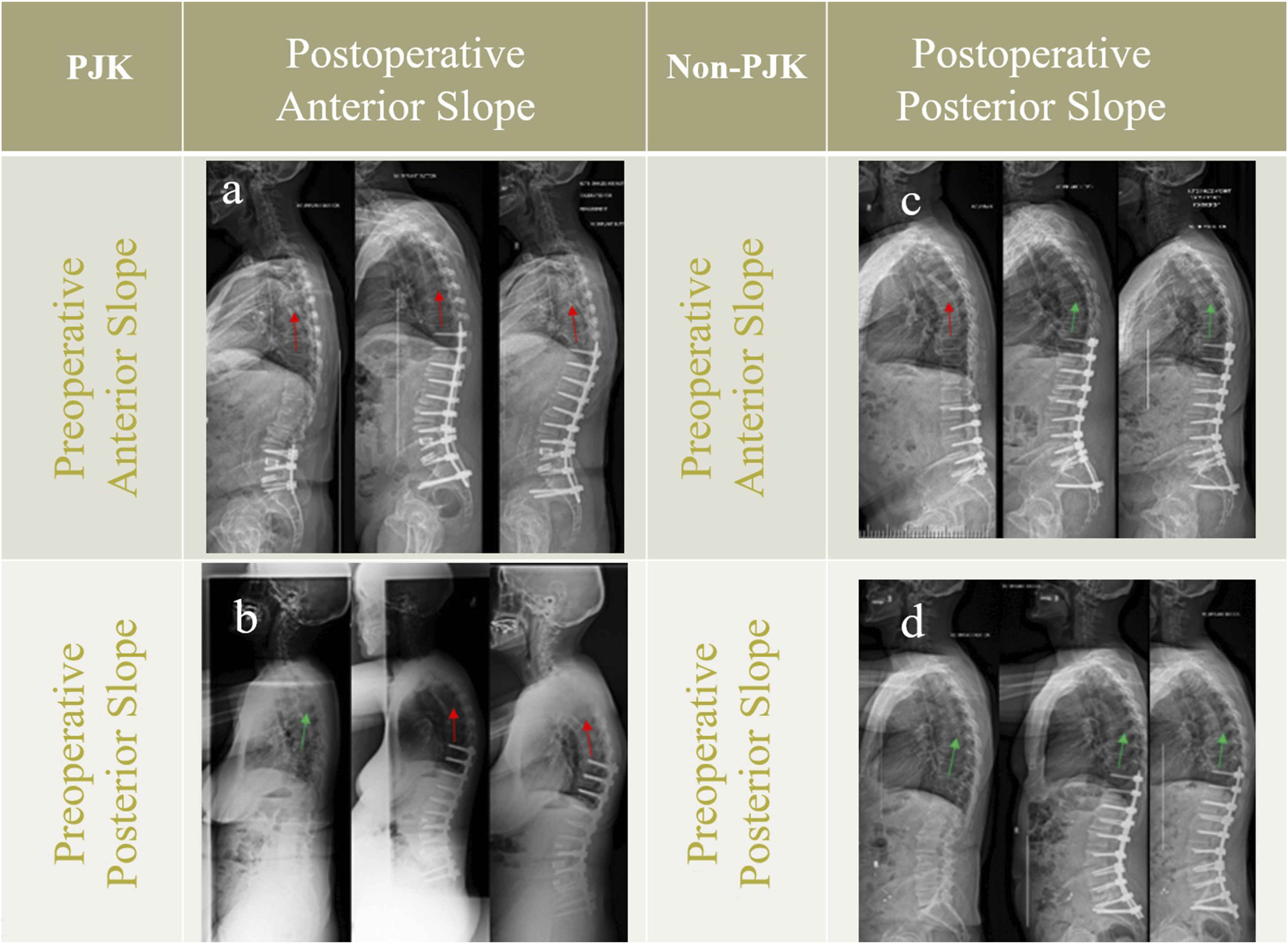
Postoperative UIV+1 Slope and Adjacent Force Association Based on Musculoskeletal Analysis
Comparison Between Vertebral Loading at UIV and UIV+1 Levels for Patients with Different Preoperative UIV+1 Inclination
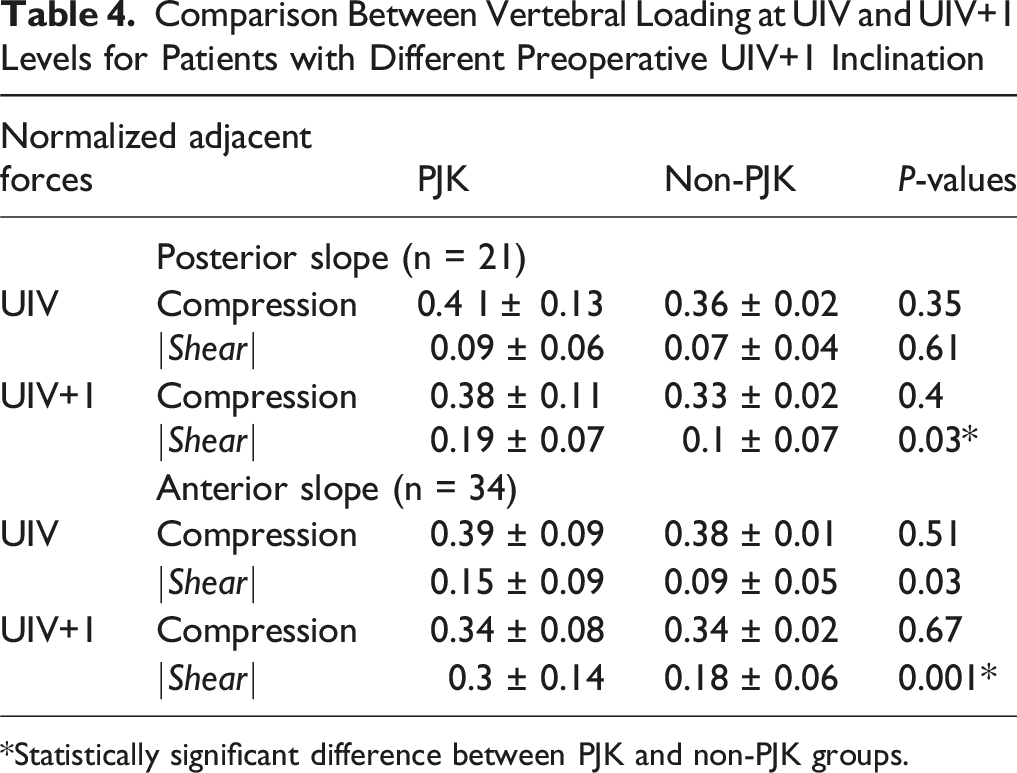
*Statistically significant difference between PJK and non-PJK groups.
Association Between Postoperative UIV+1 Slope, Shear Force and PJK Development
Figure 3 illustrates the associations between UIV+1 slope, shear force and PJK development. To investigate, shear forces were normalized, and defined as high vs low based on a threshold of 0.2.
20
From 22 patients with postoperative posterior slope, 20 patients (90.9%) had normalized shear of <0.2, whereas 24 out of 33 with anterior slope (72.7%) had normalized shear of >0.2. Comparing shear force with PJK, 21 out of 25 non-PJK patients (84%) had normalized shear <0.2 while 22 out of 30 patients (73%) with normalized shear >0.2 developed PJK. Both pre- and postoperative UIV+1 slope impacted PJK, such that 24 and 25 out of 30 patients who developed PJK had pre and postoperative anterior slope, respectively. All comparisons were statistically significant (P-values ≤ 0.002) between UIV+1 slope, shear force and PJK development. Association Between Pre and Postoperative UIV+1 Inclination, Postoperative Adjacent Shear Force, and PJK Development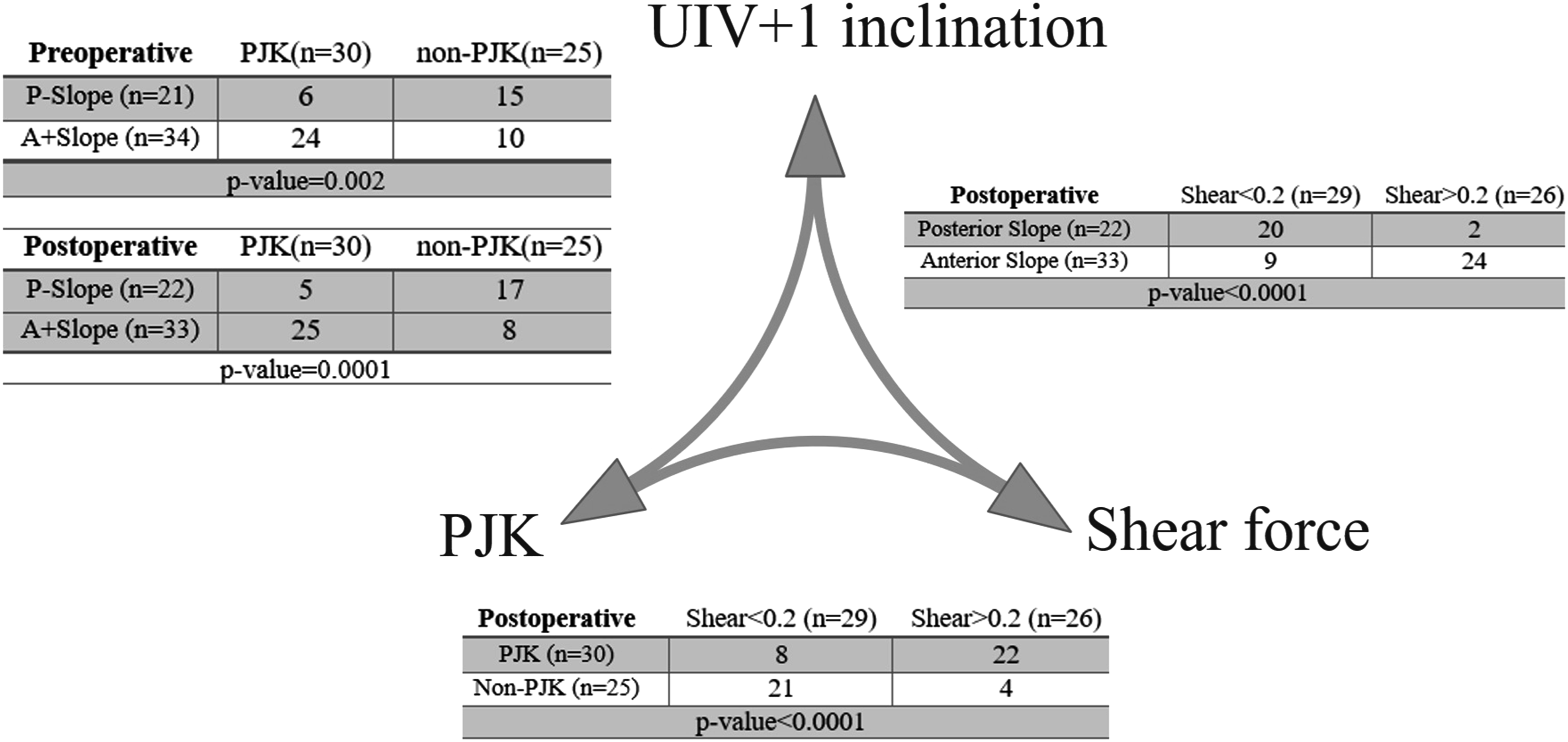
Discussion
Through mathematical analysis, we demonstrated that in Type II alignments (Figure 2B), posterior slope of UIV and UIV+1 can decrease the adjacent shear force; a finding supported by musculoskeletal analysis. Association between adjacent shear force and PJK development also was identified by musculoskeletal analysis and clinical observations. The results underscore the importance of a local sagittal alignment parameter of UIV+1 slope to reduce adjacent shear force and potential of PJK development. Preoperatively, posterior UIV+1 slope is associated with lower shear force and maintaining it following surgery can help reduce shear force postoperatively.
Prior studies have indicated a heightened risk of PJK associated with a high posterior slope at the UIV.12,14,15 We have demonstrated analytically that increasing posterior slope of the UIV which leads to a posteriorly shifted gravity line increases the adjacent shear forces consistent with a Type III alignment (Figure 2C). In this scenario, the non-instrumented spine lacks the ability to compensate to keep the head over the hips, and with elevated shear forces at UIV and UIV+1, compensation is through a decrease in the proximal junctional angle (PJA), which elevates the risk of PJK. Conversely, this study demonstrates that a posterior UIV and UIV+1 slope with anterior gravity line has the potential to mitigate shear forces at those levels as a Type II alignment (Figure 2B) and decrease the risk of PJK accordingly (ie, protective posterior slope). Determining the UIV slope threshold at which such inclination transitions from being beneficial to potentially problematic depends on the UIV+1’s capacity to adapt to UIV slope and amount of unfused thoracic reciprocal change which is influenced by paraspinal muscle stiffness and strength. The unfused thoracic compensation relies not only on flexibility of the unfused thoracic spine, but also on adequate paraspinal musculature to maintain a compensated posture. Too much thoracic flexibility can be problematic, but also, a rigid thoracic spine can result in inadequate compensation. While several methods have been suggested to assess the natural stiffness of unfused thoracic, currently there is no reliable technique. Some methods include the measurement of thoracic kyphosis (TK) change between supine/prone and standing postures as well as mismatch of expected thoracic kyphosis (eTK) and preoperative TK.10,21,22
While posterior slope of the UIV+1 analytically lessens shear force and appears to be protective against PJK development, 6 out of 21 patients with posterior UIV+1 slope preoperatively still developed PJK suggesting other factors that include postoperative local and global alignments, reciprocal changes such as pelvic retroversion and unfused thoracic stiffness, osteoporosis, and sarcopenia. Of these 6 patients, 2 had their local alignment of the UIV+1 converted from Type II (posterior slope) to Type I (anterior slope) postoperatively with the remaining 4 patients maintained in a Type II alignment. Despite the preferable local alignment condition addressed in this study, the global driver of PJK should not be neglected. Based on the concept of the cone of economy, the body’s main goal is to maintain the head over the feet; thus, any reciprocal changes are recruited to achieve this aim. The local parameters such as UIV and UIV+1 position and slope are directly affected by global alignment corrections. Undercorrection of lower lumbar lordosis (LLL) and overcorrection of upper lumbar lordosis (ULL) decreases and increases the UIV inclination, respectively. Moreover, pelvic retroversion and upper thoracic reciprocal changes, or lack thereof, also have contributions on local parameters. Figure 4 illustrates pre, immediate postop, and follow up images of cases that might or might not obey the correlation addressed between postop UIV+1 slope and PJK. It shows PJK cases with posterior immediate postop UIV+1 slope which alter at follow ups due to reasons such as improper distance of UIV to femoral head vertical line (4a) and pseudoarthrosis at UIV level (4b). It also demonstrates non-PJK patients that anterior immediate postop slope changes due to pelvic retroversion in the follow ups (4c) and other case that tolerates higher adjacent shear caused by anterior slope (4d). Examples of Patients With Different UIV+1 Inclination From Preoperative to Postoperative Status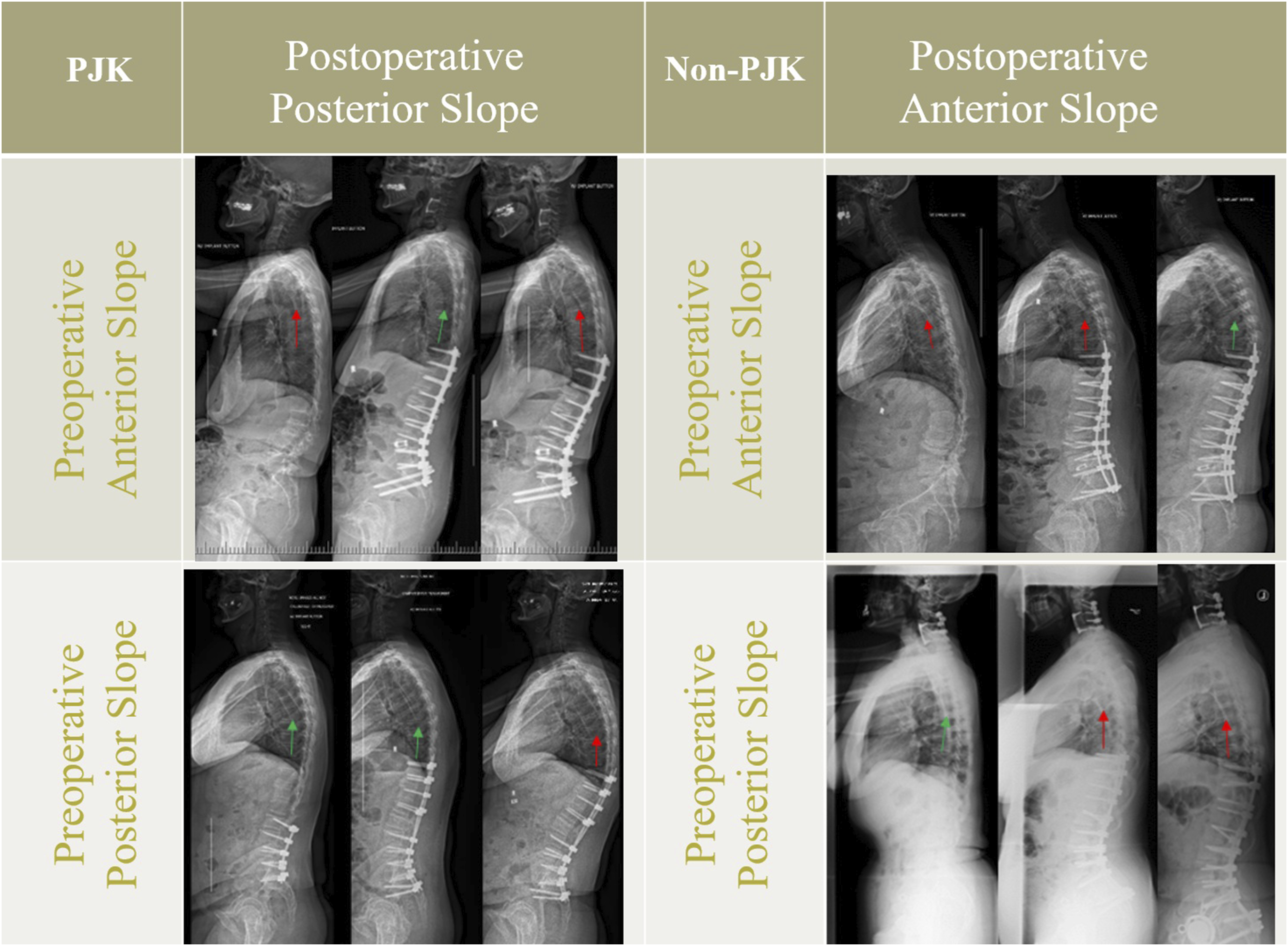
Global sagittal alignment parameters are typically targeted in realignment schemes; however, we believe that local factors such as UIV and UIV+1 position and slope are overlooked in these criteria. It is important to recognize many patients with degenerative scoliosis have a regional thoracolumbar kyphotic deformity which frequently results in anterior slope of UIV. Understanding whether the prolonged compensation impairs UIV+1 ability orient or adjust itself to UIV remains an unresolved issue that requires further investigation, particularly regarding thoracic stiffness. In addition, maintenance of the posterior soft tissue envelope at time of surgery may affect the relationship of UIV and UIV+1, and influence the proximal junction postoperatively. Integrating local factors into global realignment objectives to create optimal loading conditions at the UIV/UIV+1 to minimize shear forces may help mitigate the risk of PJK. Immediate postoperative imaging may not fully capture the long-term biomechanical behavior of the spine. However, our rationale for using immediate postoperative radiographs was to evaluate the vertebral alignment and loading conditions introduced directly by surgical correction. Several factors may change preoperative slope of UIV+1, including the degree of sagittal correction achieved, the rigidity or flexibility of the spinal segments above the UIV, patient-specific sagittal balance parameters (eg, PI–LL mismatch, sagittal vertical axis (SVA)), and compensatory mechanisms involving adjacent segments. Predicting changes in UIV+1 slope may be possible by preoperatively analyzing global sagittal alignment, assessing segmental mobility through dynamic radiographs, and simulating the expected correction using planning software. Understanding these factors can help guide surgical strategies—such as optimal selection of UIV level and extent of correction—to minimize adverse loading on adjacent segments and reduce the risk of junctional complications.
The global alignment targets such as PI–LL mismatch, TPA, and GT are important considerations in surgical planning. However, based on our findings, we propose that even in cases where PI–LL mismatch or TPA slightly exceeds traditional thresholds, acceptable outcomes may still be achieved if the proximal segment—particularly the UIV and UIV+1—is placed in a favorable local alignment. Specifically, maintaining the UIV and UIV+1 in a Type II alignment (ie, slightly posteriorly inclined but not excessively) appears to provide a biomechanical advantage (low junctional shear force), and can also preserve posterior tension and reduce the risk of proximal junctional complications. This suggests that optimal local alignment at the proximal junction may, to some extent, compensate for modest deviations in global alignment targets.
The posterior ligamentous disruption at the UIV/UIV+1 level may be a potential confounding factor influencing postoperative changes in UIV+1 slope and the development of junctional complications. The supraspinous-interspinous ligament complex plays a critical role in maintaining posterior tension band integrity and contributes to the biomechanical stability of the proximal junction. Preservation of this complex may help maintain a more favorable (ie, protective) posterior slope at UIV+1 by resisting anterior translation and kyphotic angulation, especially during the early postoperative period when soft tissue healing is incomplete.
This study has a reported rate of PJK at 54.5% (30/55), that although high, is in keeping with other reported rates in adult spinal deformity cohorts with fusions from low thoracic to pelvis. Lafage et al. 23 suggested a scoring system to identify high risk patients for PJK with risk factors being age >55 (1 point), lower instrumented vertebra S1 or pelvis (1 point), UIV position (upper thoracic – 1 point; lower thoracic – 2 points) and lordotic correction change >10° (1 point). Rate of PJK for patients with risk factor equal to 4 was 53% with an odds ratio of 5.3 (3.3-8.6), and 5 was 69% with an odds ratio of 11.0 (6.4-18.9). In this cohort of patients, 26/56 (46%) of patients had a score of 4 and 29/56 (52%) had a score of 5, indicating the high-risk nature of this cohort.Despite unique strengths, a few limitations can be mentioned for this study. Inclusion of small sample size and patients from two surgeons at a single institution is the major limitation. However, this study was designed primarily as a mathematical and mechanical analysis to explore the biomechanical mechanisms underlying proximal alignment and shear forces. The clinical sample, while limited, was included to provide initial validation and context for the model findings. To generalize the findings of this study, a larger number of cases are needed to confirm the results of UIV+1 slope effect. Although, there was no significant difference in BMD between groups, the lack of adjustment for soft tissue integrity and other PJK risk factors may limit the generalizability of the findings. Assuming uniform muscle strength and a static standing posture simplifies the complexity of real-world biomechanics. Other than individual variations in muscle strength, coordination, and recruitment patterns can be significantly different in individuals and influence spinal loading. Incorporating personalized muscle properties and attachment sites can significantly enhance the accuracy of musculoskeletal (MSK) analysis results. To estimate subject-specific muscle forces and improve the predictive accuracy of junctional biomechanics under dynamic conditions, EMG-informed musculoskeletal models have been developed.24,25 Significantly greater joint loads (P < .01) were estimated based on the EMG optimization method compared to the static optimization, and the produced muscle activation patterns were more closely aligned with each participant’s recorded EMG data. However, they may not be readily available in routine clinical settings. Since we exclude the patients with severe low BMD, the occurrence of proximal junctional failure (PJF) was not common in our series. Study on more severe mechanical complications like PJF needs incorporating BMD and muscle weakness using multi-variable analysis in the study. Further investigation is needed to identify whether abnormal UIV+1 alignment may contribute to these more severe complications.
Conclusion
Through mathematical and musculoskeletal analyses of patients with adult spinal deformity treated with low thoracic to pelvis fusions, we have identified the importance of UIV+1 slope as a local alignment parameter in reducing shear forces at the proximal junction. Clinical observations further support the association between UIV+1 slope, adjacent shear force, and risk for PJK development. Future research should consider UIV slope as a local alignment parameter and determine its utility regarding UIV selection in preoperative planning.
Footnotes
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Schroeder Arthritis Institutes, University Health Network and UHN foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.