
Abstract
Study Design:
Retrospective cohort study.
Objective:
Investigate risk factors for PJK including theoretical kyphosis, mechanical loading at the UIV and age adjusted offset alignment.
Methods:
373 ASD patients (62.7 yrs ± 9.9; 81%F) with 2-year follow up and UIV of at least L1 and LIV of sacrum were included. Images of patients without PJK, with PJK and with PJF were compared using standard spinopelvic parameters before and after the application of the validated virtual alignment method which corrects for the compensatory mechanisms of PJK. Age-adjusted offset, theoretical thoracic kyphosis and mechanical loading at the UIV were then calculated and compared between groups. A subanalysis was performed based on the location of the UIV (upper thoracic (UT) vs. Lower thoracic (LT)).
Results:
At 2-years 172 (46.1%) had PJK, and 21 (5.6%) developed PJF. As PJK severity increased, the post-operative global alignment became more posterior secondary to increased over-correction of PT, PI-LL, and SVA (all P < 0.005). Also, a larger under correction of the theoretical TK (flattening) and a smaller bending moment at the UIV (underloading of UIV) was found. Multivariate analysis demonstrated that PI-LL and bending moment offsets from normative values were independent predictors of PJK/PJF in UT group; PT and bending moment difference were independent predictors for LT group.
Conclusions:
Spinopelvic over correction, under correction of TK (flattening), and under loading of the UIV (decreased bending moment) were associated with PJK and PJF. These differences are often missed when compensation for PJK is not accounted for in post-operative radiographs.
Keywords
Introduction
The prevalence of adult scoliosis and sagittal malalignment is high in populations older than 60 years of age. 1 Correction of sagittal deformity measured by parameters such as pelvic tilt (PT), T1 pelvic angle (TPA), pelvic incidence minus lumbar lordosis (PI-LL) and sagittal vertical axis (SVA) have been shown to improve patient health and quality of life.2-5 Unfortunately, proximal junctional kyphosis (PJK), a complication of deformity surgery,6,7 occurs in anywhere from 17-39% of adult deformity cases.8-10 PJK is radiographically defined as kyphosis at the proximal end of a construct > 10˚ and has been shown to lead to worse clinical outcomes, neurological decline and even the need for revision surgery when progressing to proximal junctional failure (PJF) defined as PJK requiring revision (i.e. secondary to fracture, hardware pullout or posterior osteoligamentous disruption).11-13 Yagi et al describe the rate of proximal junctional failure as 1.4% but the true rate may be higher.13,14 Our current understanding of the pathogenesis of PJK and PJF is incomplete and it is critical that this knowledge gap be filled in order to further optimize surgical outcomes.
Several non-modifiable risk factors for PJK have been described including patient age, larger preoperative SVA values, high body mass index (BMI > 25kg/m2) and poor bone mineral density.10,14-16 While these parameters are useful for selecting appropriate surgical candidates, they do not help the surgeon plan better operations and avoid complications. Multiple modifiable risk factors have also been described including an upper instrumented vertebrae (UIV) at T1-3, a construct incorporating fusion to the sacrum, anterior-posterior surgery, a greater correction of PI-LL mismatch, and correction beyond age adjusted alignment goals.15,17-19 In biomechanical models, the use of transverse process hooks at the UIV, proximal rod contouring in the sagittal plane, as well as tapered rods mitigated PJK rates. 20 Recently, Lafage et al showed that a posteriorly inclined upper instrumented level is more likely to cause PJK. 21 In this study, PJK patients also had significantly less spinopelvic mismatch and greater thoracic kyphosis compared to non-PJK patients.
However, not all modifiable risk factors reported in the literature agree. For example greater correction of SVA has been reported to be a risk factor for PJK.17,22 In contradiction, Mendoza-Lattes reported that under-correction of the lumbar lordosis and residual kyphosis is a risk factor for PJK. 23 A potential explanation for this is the reciprocal changes which occur in the face of changes to global alignment.
The assessment of PJK is likely complicated by the fact that the spine compensates to counteract SVA malalignment to keep the head centered over the feet. 24 For example, Protopsaltis et al showed that the presence of preoperative thoracic compensation (thoracic hypokyphosis) can be used to determine which patients will develop reciprocal thoracic kyphosis and PKJ post operatively. 25 This creates a problem in the analysis of PJK, as it may be masked by compensatory mechanisms such as pelvic tilt. In addition, PJK itself may be considered a form of compensation for alignment overcorrection to maintain global alignment. As PJK can occur in the early postoperative period, x-ray analysis can prove difficult as the global alignment is already affected.6,26 In an attempt to isolate the post-operative alignment prior to the development of PJK, Lafage et al developed a virtual correction method which accounts for the compensatory mechanisms of PJK. By combining the preoperative unfused segment to the postoperative fused segment on a lateral x-ray and removing the effects of pelvic tilt they were able to model a spine unaffected by PJK. Furthermore, using this model, they were able to show a strong correlation with smaller post-operative sagittal parameters (i.e. stricter deformity correction) in PJK patients compared to no-PJK patients. In essence, PJK seems to result from over correction of sagittal deformity beyond what is mechanically harmonious for a patient26,18 As PJK occurs, the mechanical loading due to gravity also increases potentially leading to further breakdown if load is increased beyond mechanical resistance. 27 To date there has been no study examining the combined effects of age adjusted offset, mechanical loading and sagittal parameters in concert.
The purpose of this study was to compare post-operative sagittal alignment parameters in patients without PJK, with PJK or with PJF, using combined analytic methods including virtual alignment free from PJK influence, theoretical kyphosis, age-adjusted offset, and mechanical loading on the UIV. Using these models, we hope to help predict when PJK will occur and describe an ideal spine shape which will reduce the incidence of PJK. To our knowledge there has been no study using these analytic models to determine the risk factors for PJK.
Materials and Method
Study Sample
A retrospective review of a prospectively collected multicenter database of adult spinal deformity patients was performed. Patients were enrolled into the ongoing database through an institutional review board approved protocol across all centers. The ethical approval was obtained from the Institutional Review Board of Hospital for Special Surgery prior to conducting the study (IRB No. 2014-357). Informed consent was obtained from all participating patients. The inclusion criteria included: (1) patients >18 yrs. age; (2) at least one of the following radiographic signs of spinal deformity: Cobb angle ≥ 20˚, SVA ≥5 cm, PT ≥ 25˚, and TK ≥ 60˚; (3) UIV of at least L1 and LIV of sacrum.
The following data points were collected and compiled: age, gender and BMI (Body Mass Index). At each time point (preoperative, post-operative, and 2 years post-operative for patients without revision PJK and the pre-revision time point for PJF patients) anteroposterior and lateral full length 36-inch films were obtained. Radiographic parameters were measured using a dedicated and validated software 28 (Spineview®, ENSAM Laboratory of Biomechanics, Paris, France), followed by a post-treatment using MATLAB (Version R2015b; The MathWorks, Inc., Natick, Massachusetts) and included: pelvic incidence (PI), Pelvic Tilt (PT), spino-pelvic mismatch (PI-LL), thoracic kyphosis between T4 and T12 (T4-T12), T1-pelvic-angle (TPA), and sagittal vertical axis (SVA). The PJK angle was measured between the inferior endplate of the UIV and the superior endplate of the UIV+2 using the Cobb method. This analysis was performed on the actual post-operative alignment radiographs, prior to the virtual treatment (see below) and designated the REAL alignment.
Following this, the virtual alignment method was applied using a validated technique described previously 26 according to the following framework (Figure 1):
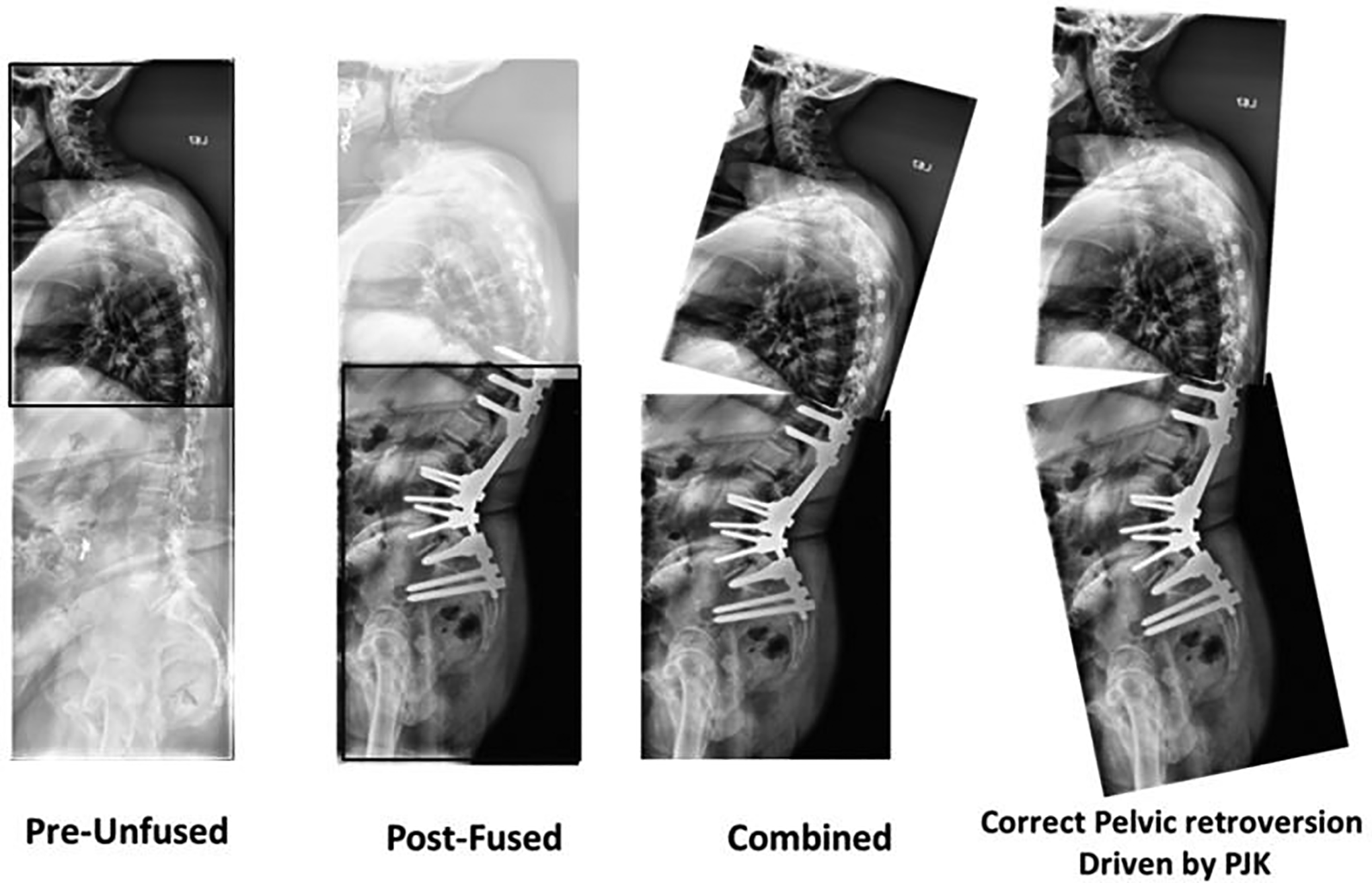
Framework for virtual alignment creation.
Fused segment: based on the 2-year post-operative alignment; incorporating the pelvis to the vertebra below UIV (UIV-1)
Unfused segment: based on the pre-operative alignment; incorporating C2 through the UIV
Combination of the fused (pelvis to UIV-1; post-operative) and unfused (C2-UIV; pre-operative) segments
Correction of Pelvic Tilt (PT): PT adjusted for the combined alignment based on validated published formulas using PI, LL, and TK 29
The analysis performed on these radiographs aimed to remove the compensatory influence of PJK and was designated as the VITRUAL alignment.
Mechanical Loading
Bending moment at the UIV was calculated using a validated model 30 combining literature data on the mass distribution/location of individual body segments.31,32 After finding the location of the centers of mass of individual segments the coordinates of the center of mass above the UIV was calculated using the formula:
with M representing the sum of all masses above the UIV, m the masses of individual segments, and r the coordinates of the individual center of masses.
Using the same approach, bending moment due to gravity was calculated at each individual vertebra on a group of asymptomatic volunteers. The value of the bending moment at the UIV was then compared between reference values found on asymptomatic volunteers and alignment free of PJK influence (VIRTUAL). All calculations were performed based on a theoretical weight of 1 kg.
The criteria for radiographic PJK was defined according to that set forth by Glattes et al 8 as a kyphotic angle between the UIV and UIV+2 greater than 10° and a kyphotic change greater than 10° between pre and post-operative. Proximal junction failure (PJF) was defined according to the criteria described by Yagi et al as any patient with a symptomatic PJK requiring revision surgery. 13 These 3 groups, no PJK, PJK and PJF, were exclusive.
Statistical Analysis
Pre-operative information, including demographic, sagittal alignment and SRS-Schwab classification for the entire cohort were expressed using mean, standard deviation and frequency. The rate of radiographic PJK and PJF were reported for the entire cohort.
Pre-operative and post-operative alignment parameters were compared between no-PJK, PJK and PJF patients using an ANOVA. Comparisons were conducted using overall alignment but also the difference between current alignment and targets adjusted by age 33 and PI 25 calculated using the real and virtual alignment (e.g. alignment free of PJK influence). Multilinear logistical regression was conducted to identify independent predictors of PJK and/or PJF. Sub-stratification was performed according to the position of the UIV (Upper thoracic: UIV was above T7 and lower thoracic: UIV below T7) and the analysis was repeated for both groups.
Results
Cohort Demographics
Three hundred and seventy-eight patients were included in the analysis. The mean age was 62.7 ± 9.9 years and the population was 81% female. The average BMI was 28.0 ± 5.6kg/m2. Revision cases accounted for 30.4% of cases.
Pre-operative SRS-Schwab classification demonstrated a moderate to severe sagittal deformity with 26.2% of the cohort with a PI-LL modifier at + and 46.6% of the cohort with a PI-LL modifier at ++. Similarly, 30.2% and 38.1% had an SVA modifier at + and ++, 41.8% and 32.8% had a PT modifier at + and ++.
Radiographic PJK was present in 45.2% (n = 171) of patients. The PJF rate was 7.1% (n = 27 patients). The total rate for either PJK or PJF was 52.4% (n = 198).
Preoperative Data
Regarding demographics, there was a significant difference in the age of patients between the 3 PJK groups (no PJK = 60.7 ± 10.5 vs PJK = 64.4 ± 9.1 vs PJF = 66.0 ± 9.9 P = 0.001) but no significant difference in sex or BMI.
Comparison of pre-operative alignment demonstrated no significant difference regarding preoperative alignment parameters between PJK groups in terms of PI (56.1 vs 54.2 vs 52.5 P = 0.204), PT (25.6 vs 26.7 vs 27.8 P = 0.402), PI-LL (19.5 vs 22.4 vs 21.5 P = 0.354), TK (−31.8 vs −30.0 vs −33.4 P = 0.466), TPA
(25.3 vs 26.5 vs 27.3 P = 0.570) and SVA (79 vs 83 vs 88 P = 0.786). Additionally, no significant difference was found in terms of pre-operative SRS-Classification between no-PJK, PJK and PJF (all P > 0.3) (Table 1).
Comparison of Pre-Operative SRS-Schwab Classification Between No-PJK, PJK and PJF.

Post-Operative Data (REAL)
When comparing post-operative images (REAL) there was significantly smaller PI-LL values as PJK severity increased (No PJK = 5.7˚ ± 16.1˚ vs PJK = 2.3˚ ± 14.2˚ vs PJF = −2.7˚ ± 10.4˚ P = 0.009). In addition, the thoracic kyphosis was significantly different between PJK groups and increased as PJK severity increased (No PJK −41.8˚ ± 15.3˚ vs PJK −47.4˚ ± 16.1˚ vs PJF −55.8˚ ± 14.3˚ P < 0.001). There was no significant difference in PT, TPA or SVA between all PJK groups (all P > 0.5) (Table 2).
Comparison of Post-Operative and Change Pre-to-Post Between No-PJK, PJK and PJF.
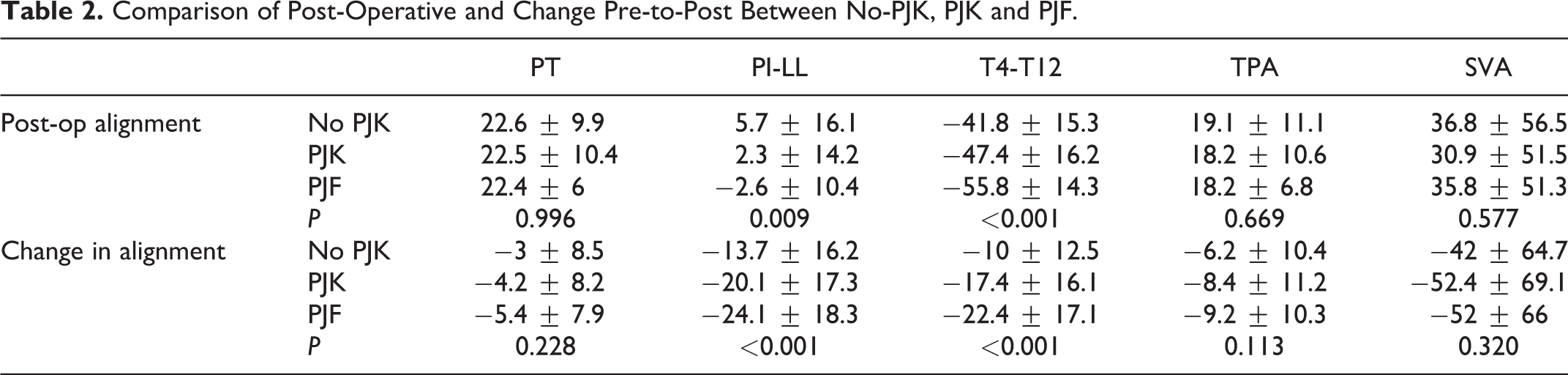
As PJK severity increased there was an increase in lumbar correction across groups (Change in PI-LL: No PJK −13.7˚ ± 16.2˚ vs PKJ −20.1˚ ± 17.3˚ vs PJF −24.1˚ ± 18.3˚ P < 0.001). There was also a larger change in the magnitude of thoracic kyphosis correction with increasing PJK severity (No PJK −10.0˚ ± 12.5˚ vs PJK −17.4˚ ± 16.1˚ vs PJF −22.4˚ ± 17.1˚ P < 0.001). There was no significant difference in the change in PT, TPA or SVA between groups (Table 2).
In the subanalysis of patients with an upper thoracic UIV, there was no significant difference in post-operative alignment between PJK groups (all P > 0.05). There were larger changes in PT, TPA, and SVA between pre and post-op with increasing PJK. No significant difference was found in terms of PI-LL and TK correction (P = 0.125 and P = 0.501) (Table 3).
Comparison of Post-Operative and Change Pre-to-Post Between No-PJK, PJK and PJF After Stratification by UIV Position.
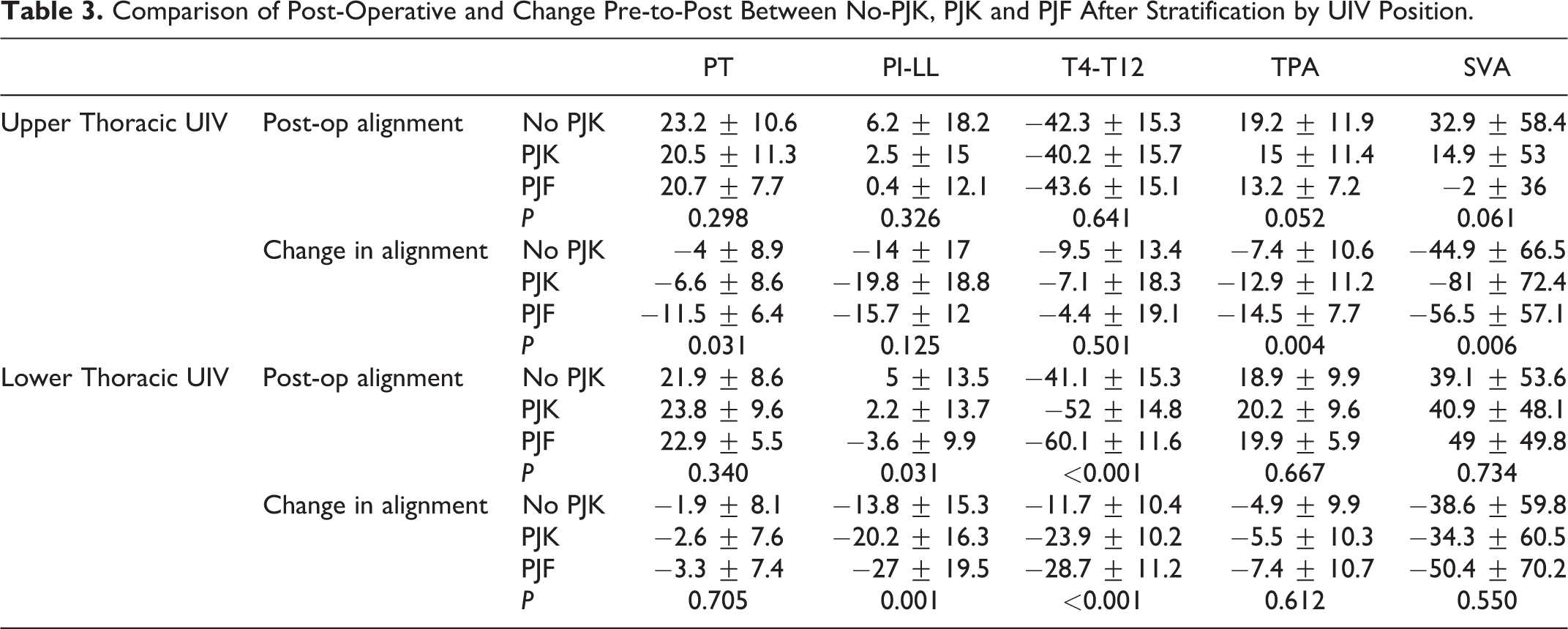
In the lower thoracic UIV group, there were significantly smaller spinopelvic mismatch (PI-LL) and a larger degree of thoracic kyphosis with increasing PJK severity, without any significant difference in PT, TPA and SVA. There was a larger change in the PI-LL value and degree of TK for PJF. There was no difference in PT, SVA or TPA correction (Table 3).
Post-operative alignment without PJK (VIRTUAL)
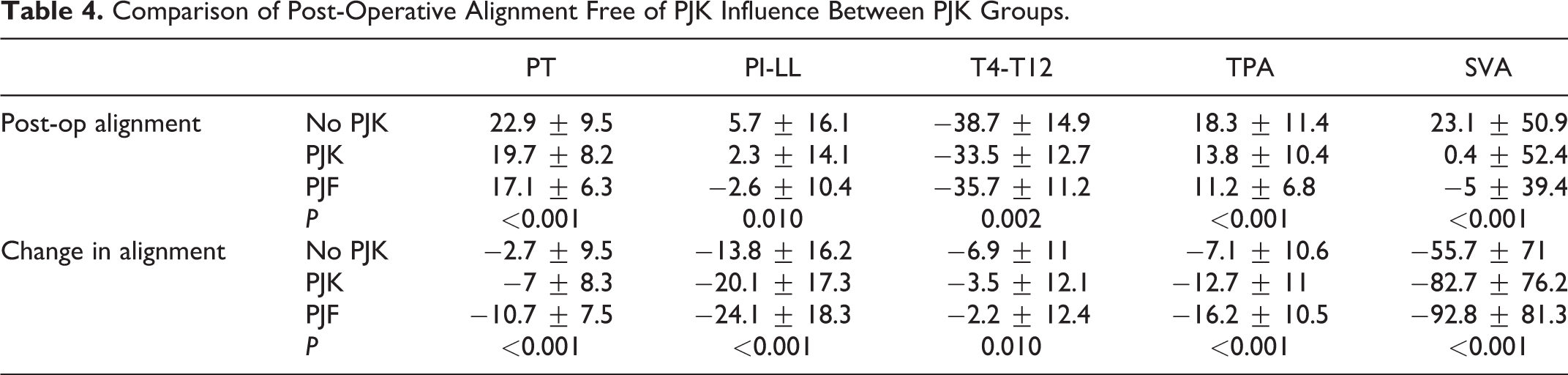
Comparison of post-operative spino-pelvic parameters free of PJK influence demonstrated significantly more posterior alignment with increasing PJK severity, associated with a larger change in all parameters (PT, PI-LL, TK, TPA and SVA) (Table 4).
Comparison of Post-Operative Alignment Free of PJK Influence Between PJK Groups.
When patients were stratified by UIV position, in the upper thoracic group PJK and PJF patients demonstrated a smaller thoracic kyphosis (No PJK = −40.4˚ vs PJK = −34.8˚ vs PJF = −37.2˚ P = 0.044) associated with more posterior alignment in terms of TPA and SVA (TPA: No PJK = 18.7˚ vs PJK = 14.0˚ vs PJF = 12.2˚ P = 0.025, SVA: No PJK = 27 mm vs PJK = 0 mm vs PJF = −25 mm P = 0.001) without significant difference in lumbar alignment between groups (p = 0.329). PJK and PJF patients underwent a larger global correction of spinal alignment parameters in terms of PT (−4° vs −7° vs −11.2° P = 0.042), TPA (−7.8° vs −13.9° vs −15.5° P = 0.002) and SVA (−51 mm vs −97 mm vs −80 mm P = 0.001) associated with a relative maintenance of the thoracic curvature compared to non-PJK patient (T4-T12: −7.6° vs −1.7° vs 2.0° P = 0.021).In other words, thoracic kyphosis was maintained in the no-PJK patient while it decreased in the PJK and PJF patients.
The lower thoracic UIV group had significantly smaller PI-LL mismatch as PJK severity increased (No PJK = 4.8˚ vs PJK = 2.1˚ vs PJF = −3.6˚ P = 0.035) without significant difference in thoracic alignment (P = 0.146). As a result, patients demonstrated a more posterior global alignment as PJK severity increased (TPA: 17.5˚ vs 13.7˚ vs 10.8˚ P = 0.005, SVA: 19 mm vs 1 mm vs 2 mm P = 0.041) combined with a smaller pelvic retroversion (PT: No PJK 22.3˚ vs PJK 19.4˚ vs PJF 15.7˚ P = 0.001). In terms of preoperative to postoperative change, PT, PI-LL and TPA changes were significantly larger with increasing PJK severity (PT: No PJK −1.5˚ vs PJK −7.0˚ vs PJF −10.5˚ P = 0.001; PI-LL: −13.9˚ vs −20.3˚ vs −27.0˚ P < 0.001; TPA: −6.4˚ vs −12.0˚ vs −16.5˚ P < 0.001). There was no difference in TK and SVA correction.
Offset with alignment target
Comparison of the offset between alignment targets and the virtual alignment between PJK groups demonstrated an over correction in terms of PT: No PJK = −0.9° vs PJK = 3.4° vs PJF = 6.6° P < 0.001; PI-LL: No PJK = 0.2° vs PJK = 5.4° vs PJF = 11.1° P < 0.001; TPA: No PJK = 0.6˚ vs PJK = 6.9˚ vs PJF = 10.3˚ P < 0.001; SVA: No PJK = 13 mm vs PJK = 43 mm vs PJF = 52 mm P < 0.001 and TK: No PJK = 3.7˚ vs PJK = −5.7˚ vs PJF = −11.0˚ P < 0.001 (Figure 2).
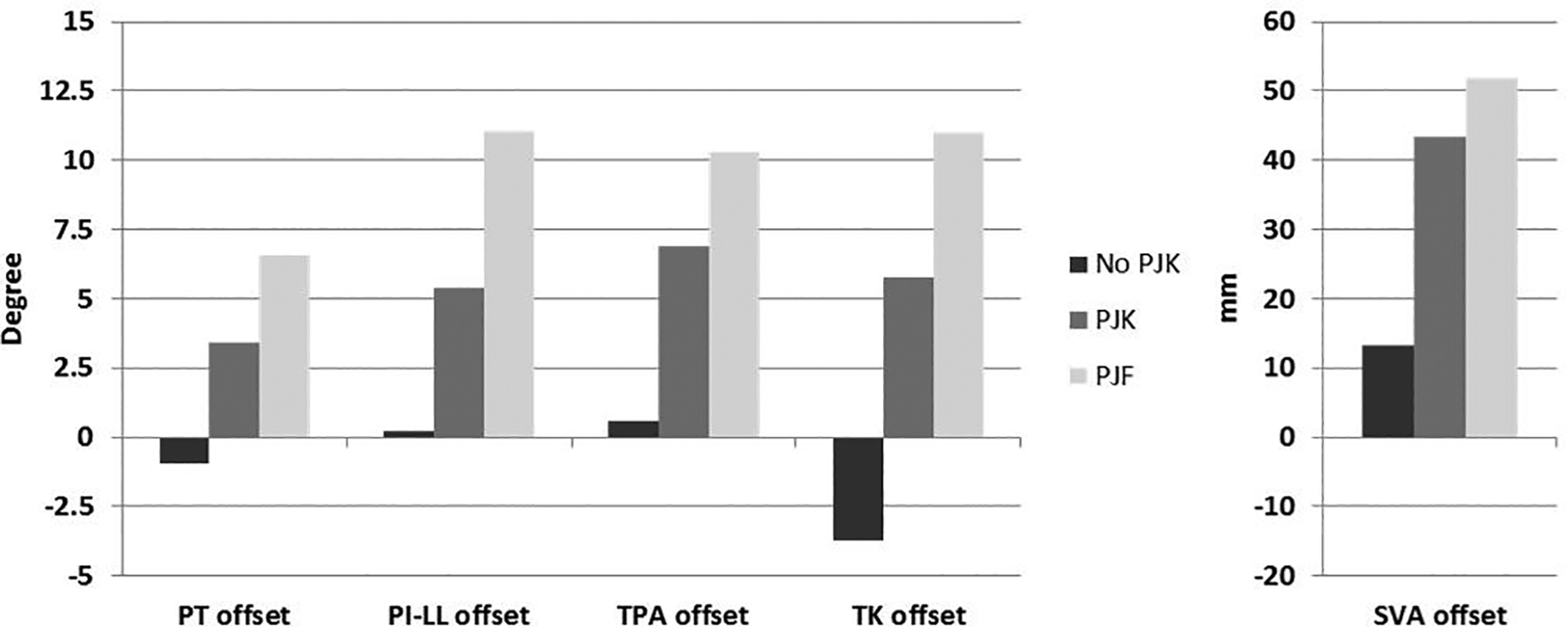
Comparison offset between alignment free of PJK influence and alignment target (age-alignment and adjusted TK) between PJK groups.
Sub-analysis by UIV position demonstrated similar results: PJK and PJF patient showed an increase in over correction compared to alignment targets by age and PI in no-PJK patient (Figure 3).
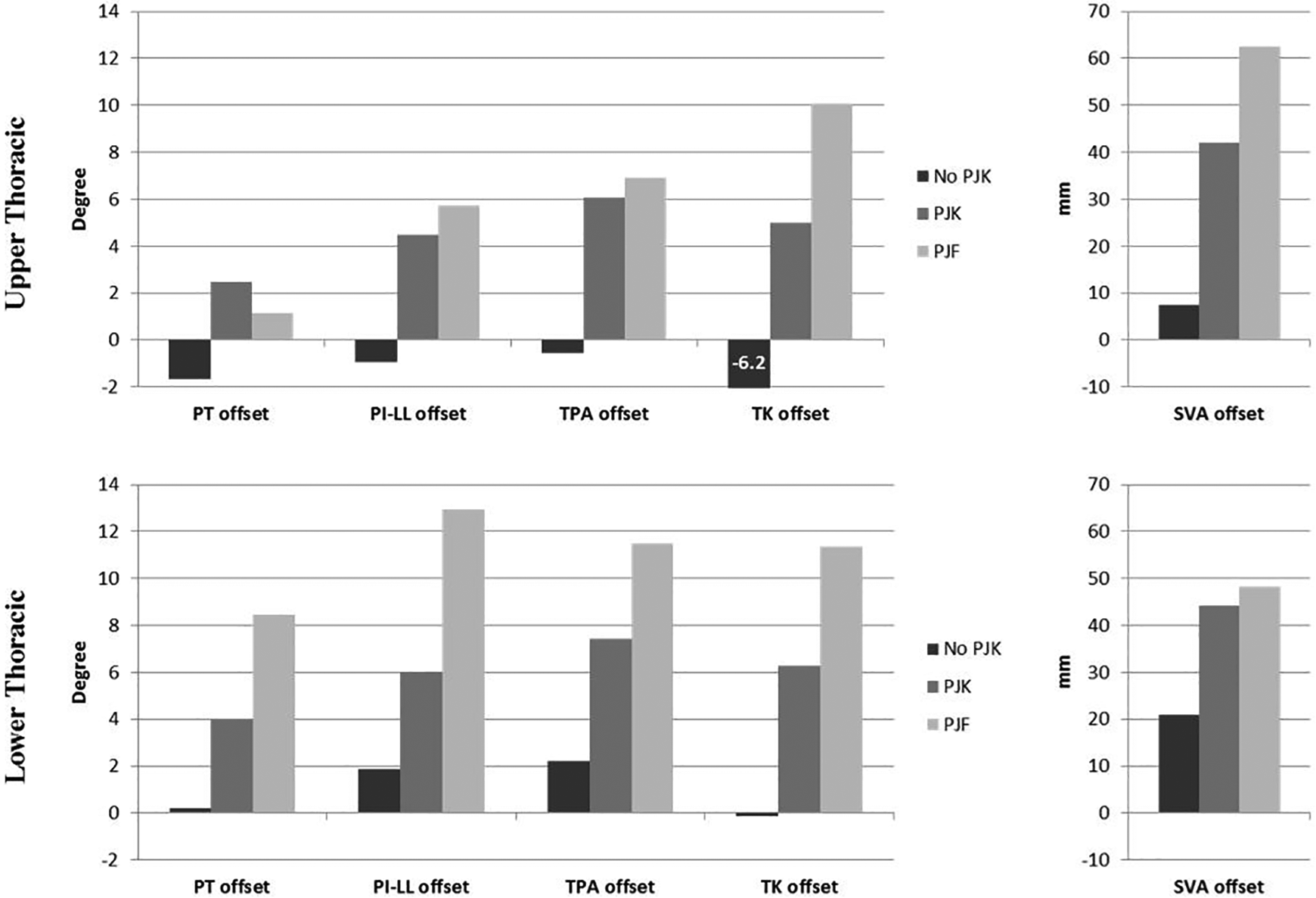
Comparison offset between alignment free of PJK influence and alignment target (age-alignment and adjusted TK) between PJK groups after stratification by UIV position (upper and Lower thoracic).
Mechanical loading
Comparison of the bending moment at the UIV using the real alignment showed increasing mechanical load across PJK severity for both Upper thoracic UIV (No PJK = 0.053 N*m ± 0.027 vs PJK = 0.068 N*m ± 0.027 vs PJF = 0.069 N*m ± 0.021 P = 0.001) and Lower thoracic (No PJK = 0.111 N*m ± 0.063 vs PJK = 0.142 N*m ± 0.054 vs PJF = 0.163 N*m ± 0.072 P < 0.001) (Figure 4). However, after removing the effect of PJK on alignment, there was a decrease in mechanical loading as PJK severity increased (Upper thoracic: 0.043 N*m ± 0.026 vs 0.028 N*m ± 0.026 vs 0.020 N*m ± 0.024 P = 0.001, Lower thoracic: 0.085 N*m ± 0.059 vs 0.058 N*m ± 0.048 vs 0.054 N*m ± 0.045 P = 0.002) (Figure 4).
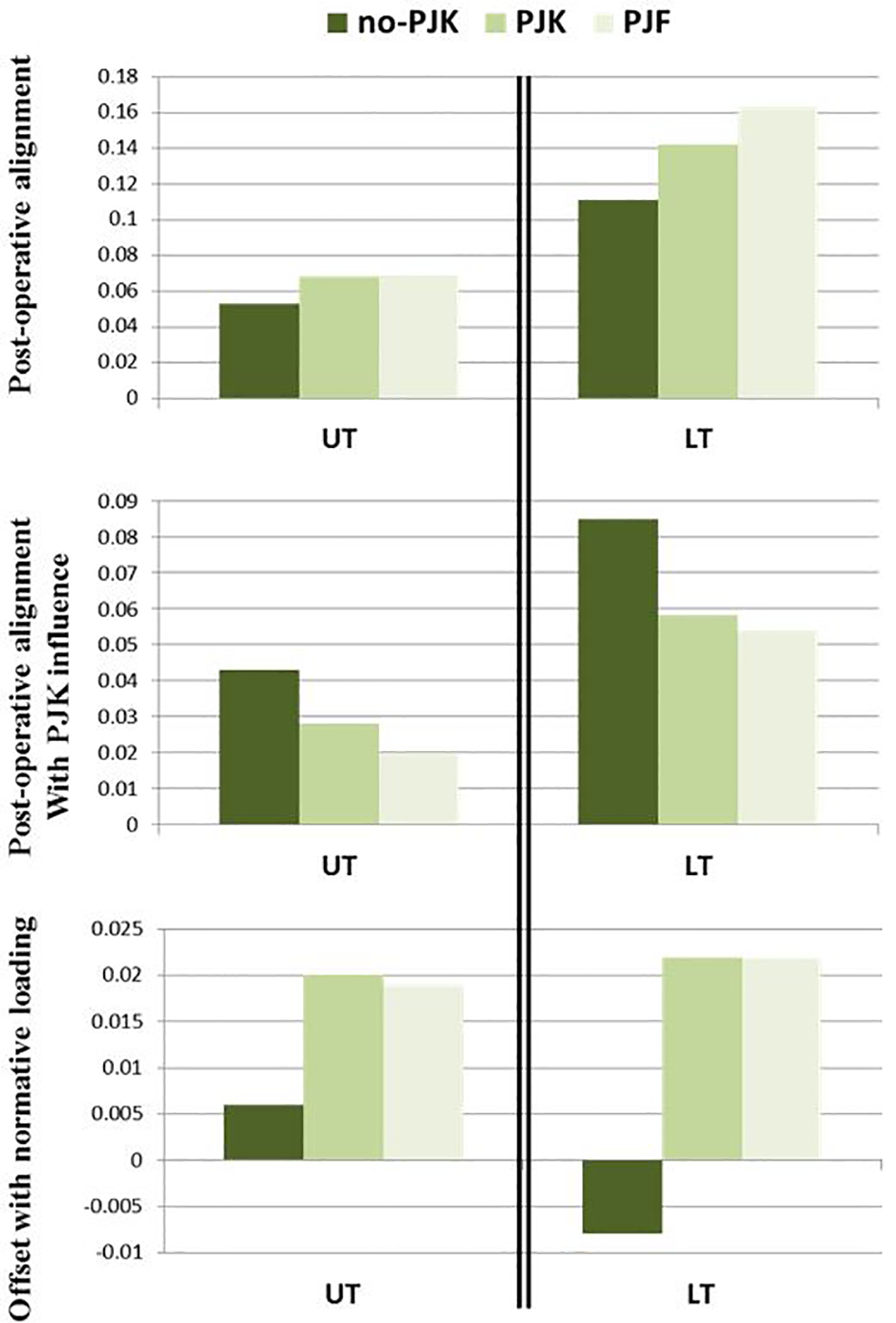
Comparison of mechanical loading between PJK groups after stratification by UIV position (UT: Upper Thoracic; LT: Lower Thoracic). All results are expressed in Nm and were calculated based in a theoretical weight of 1 kg.
Comparison of the offset between normative bending moment values obtained by applying the same model on a cohort of 119 asymptomatic volunteers and the bending moment on the alignment free of PJK influence demonstrated that the bending moments at UIV of PJK and PJK patients were larger than the sustained by the control group (Figure 4).
Multivariate logistic regression analysis
Using a multivariate stepwise logistical regression, significant independent risk factors for PJK or PJF were PI-LL alignment (P = 0.008; OR: 1.038), TPA free of PJK influence offset from age alignment (P < 0.001; OR: 1.085), bending moment on alignment free of PJK influence (P = 0.009; OR: 1.136), and the bending moment offset from normative value on alignment free of PJK influence (P < 0.001; OR: 1.259).
Examining the subgroup of upper thoracic UIV patients, significant independent predictors of PJK or PJF included SVA free of PJK influence (P = 0.008; OR: 1.027), SVA free of PJK influence using offset from age alignment (P < 0.001; OR: 1.033), and bending moment offset from normative value on alignment free of PJK influence (P < 0.001; OR: 1.367). The overall accuracy of classification using these predictors was 72.9%.
Examining the subgroup of lower thoracic UIV patients, significant independent predictors for PJK and PJF included TPA free of PJK influence (P < 0.001; OR: 1.154), Pelvic Tilt free of PJK influence offset from age alignment (P = 0.001; OR: 1.204), Bending moment offset from normative value on alignment free of PJK influence(P < 0.001; OR: 1.222). Accuracy of classification for lower thoracic patient was 67.8% using these 3 independent predictors.
Discussion/Conclusion
In this study, the overall rate of PJK was 45% and the rate of PJF was 7.1%. Comparison of preoperative alignment measures between patients without PJK and those with either PJK or PJF demonstrated no significant difference in deformity.
Post-operative alignment demonstrated no difference in global alignment (TPA and SVA) and pelvic orientation (PT) despite having a smaller spino-pelvic mismatch and a larger thoracic kyphosis in PJK and PJF patients. We believe the maintenance of global alignment was likely due to the compensatory nature of PJK in the sagittal plane. It is well known that as spinal malalignment worsens (typically anterior malalignment), patients recruit compensatory mechanisms to maintain sagittal balance. In the non-instrumented spine, these mechanisms include pelvic retroversion and thoracic hypokyphosis, followed by compensation in the lower limbs with knee flexion. 24 Following over-correction of PI-LL (ie. posterior malalignment), the opposite phenomena are observed: a decrease in pelvic tilt and an increase in thoracic kyphosis in an effort to maintain a neutral posture. 34 In the setting of ASD surgery with fusion, the compensatory increase in thoracic kyphosis in the unfused segment of the spine can take the form of PJK. In other words, PJK patients create a focal deformity to maintain neutral global alignment in the face of surgical over correction. This phenomena occurs to normalize the SVA. 26
Proximal junction kyphosis typically occurs early in the post-operative course (within 65 days) and can alter sagittal parameters, leading to difficulty with interpretation of standing long cassette films.26,35 Early post-operative films are already affected by PJK and thus the determination of its effect on other sagittal alignment parameters are difficult to conclude. The virtual model utilized in this study was designed to remove the compensatory effect of PJK on global alignment and was used previously to show that PJK patients had more posterior sagittal alignment following deformity surgery. 26 In the current study, these findings were reiterated by PJK and PJF patients having significantly more posterior sagittal alignment in spinal parameters including PT, PI-LL mismatch, TK, TPA and SVA with the virtual removal of the effects of PJK.
Using the VIRTUAL model, PJK patients were stratified into those who had a lower thoracic UIV (below T7) vs. an upper thoracic UIV (above T7). This analysis showed that the lower thoracic UIV group had an over-correction of the lumbar lordosis as PJK severity increased (smaller PI-LL mismatch). This occurred without significant change in the thoracic kyphosis. Interestingly, patients who had UIV in the upper thoracic region instead had significantly less restoration of their thoracic kyphosis as PJK severity increased (i.e. they remained hypokyphotic). Both situations resulted in pathologic equilibration of the global alignment resulting in PJK. Moreover, the bending moment was reduced at the UIV using the VIRTUAL model which likely results in a natural equilibration to increase the load which may result in PJK. We see this in the REAL analysis which showed an increase bending moment after PJK had occurred. Thus, it is critical to take into consideration the effects of PJK when planning surgery and account for thoracic restoration. Lafage et al demonstrated this principle in an earlier study noting that posterior inclination of the UIV and thoracic hypokyphosis predisposed to PJK whether the UIV is located in the upper thoracic region or the thoracolumbar region. 21
In a previous study comparing alignment to age adjusted targets, Lafage et al showed that the PI-LL mismatch was smaller in PJK patients because of overcorrection. 18 However, in this study there was no other change noted in PT. In the current study using the VIRTUAL model no-PJK patients matched age-adjusted alignment targets whereas PJK patients had their deformities overcorrected with regard to age adjusted PT, PI-LL, SVA and TK. This was possible to delineate because we were able to correct for the compensatory mechanisms of PT and PJK.
The spine works optimally in a specific configuration to transfer load from the torso to the lower extremities. Alterations to the alignment can pathologically alter mechanical loads across discs and facets. A focal deformity first occurs in response to over correction of sagittal alignment, this change results in an abnormal loading of the discs and facets which can result in bone failure and increasing deformity creating a vicious cycle. Thus, in this study we analyzed mechanical loading across the UIV between no-PJK and PJK patients. Analyzing the post-operative radiographs demonstrated significantly increased bending moments as PJK severity increased. However, comparison of the bending moment utilizing the virtual model demonstrated significant under-loading of the UIV for the PJK and PJF patient. This is significant because the body is perhaps overcompensating for mechanical malalignment resulting in underloading of the UIV. Why these patients are not able to reach equilibrium is still poorly understood but likely related to the fact that overcompensation leads to decompensation of tissues and bone resulting in an ability to equilibrate.
Several limitations exist to the current study. Other important risk factors in the pathogenesis of PJK such as BMD, muscle quality, and patient activity were not examined in concert to alignment parameters. However, the bending moment can be thought of as the force to failure, and is different for every individual depending likely on their host factors such as ligament and bone quality, frailty etc. Moreover, the cohort of PJF patients was defined as any patient requiring revision. For this group we could not account for patients who refused / were denied surgery or lost to follow up. Thus, the real rate of PJF was likely higher than what we report. Furthermore, in this study we were unable to compare the preoperative surgical planning between patients with PJK and those without. To compensate for this, we considered the fused segment of the spine as the preoperative plan in the virtual model. Future studies should compare preoperative surgical plans to post-operative results to better outline how optimal alignment goals can help prevent PJK. Moreover, more studies are needed to examine the combined effects of modifiable and non-modifiable risk factors for PJK.
Other scoring systems exist for stratifying risk in adult spinal deformity cases. Firstly, the Schwarb-SRS score examines overall spinal alignment (SVA), pelvic tilt and pelvic incidence minus lumbar lordosis. This scoring system was developed based on patient outcomes and encourages correction of SVA < 4 cm, PT < 20˚ and PI-LL <10˚. 5 Other scoring systems include the Global Alignment and Proportion (GAP) score which examines the relative pelvic version (measured minus ideal sacral slope, relative lumbar lordosis (measured minus the ideal lumbar lordosis), relative spinopelvic alignment (measured minus the ideal global tilt), age and lordosis distribution index (the L4-S1 lordosis divided by the L1-S1 lordosis multiplied by 100). 36 While both of these scoring systems have been validated, 37 they fail to account for dynamic changes in alignment which are caused by PJK. Using the VIRTUAL model, this study was able to account for the dynamic equilibration effects of PJK to allow true analysis of alignment.
In summary, this study synthesizes many alignment factors which contribute to PJK. We show that PJK patients had sagittal overcorrection past their ideal range compared to those who did not develop PJK. Moreover, we found that PJK patients with a thoracic UIV had under correction of thoracic kyphosis and those with a lower thoracic UIV had overcorrection of the lumbar curvature. The VIRTUAL model is useful for evaluating early PJK radiographs as it removes compensatory aspects of sagittal alignment leaving a patient’s pure alignment unaffected by gravity. It is critical for surgeons to restore the thoracic kyphosis if planning on instrumenting an upper thoracic vertebra as the UIV. These findings help confirm that PJK is a pathological variant of reciprocal change to maintain equilibrium between the SVA and the gravity line.
Key Conclusions
Comparison of preoperative alignment demonstrated no difference between patients without PJK, with PJK or PJF
Comparison of post-operative alignment free of the influence of PJK demonstrated more posterior alignment (PT, TPA, SVA) for PJK and PJF patients and an over correction compared to age-alignment targets.
In the sub analysis of patients with UIV in the upper thoracic area, TK was significantly smaller and TPA/SVA significantly larger as PJK severity increased. In the lower thoracic subgroup, there were significantly smaller PT and PI-LL values and increased TPA/SVA values as PJK severity increased.
Offset from age-adjusted parameters, posterior alignment and bending moments are the independent predictors of PJK and PJF in adult spinal deformity correction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes (current), Nuvasive (current), K2 M (current), Innovasis (past), Biomet (past), and individual donations. Funding sources did not play a role in investigation.