
Abstract
Study Design
Retrospective cohort study.
Objectives
To assess whether preoperative vitamin D deficiency is associated with increased postoperative complications after single-level lumbar fusion.
Methods
We queried a national EHR network for adults undergoing posterior/posterolateral single-level lumbar fusion. Vitamin D deficiency was defined by the most recent preoperative 25-hydroxyvitamin D <20 ng/mL. Patients with multilevel fusion, <2-year follow-up, scoliosis, or spinal cord neoplasm were excluded. Propensity-score matching (1:1) on demographics, Charlson Comorbidity Index, obesity, osteoporosis, nicotine dependence, vitamin D supplementation, celiac disease, inflammatory bowel disease, chronic pancreatitis, and cystic fibrosis yielded 1365 patients per cohort (from 1372 deficient and 89,165 non-deficient). Outcomes included 90-day incidence of readmission, emergency department (ED) utilization, deep vein thrombosis (DVT), pulmonary embolism (PE), pneumonia, sepsis, acute kidney injury (AKI), urinary tract infection (UTI), surgical site infection (SSI), and death. Instrumentation failure, pseudoarthrosis, and revision were assessed at 90 days, 1 year, and 2 years. Risk differences and relative risks (RR) were calculated; statistical significance was set to P < 0.05.
Results
Vitamin D deficiency was associated with higher 90-day risk of readmission (RR = 1.19), ED use (RR = 1.32), AKI (RR = 1.77), SSI (RR = 2.06), death (RR = 2.40), and pseudoarthrosis (RR = 1.47). Pseudoarthrosis risk remained higher at 1 year (RR = 1.43) and 2 years (RR = 1.40), and revision surgery was higher at 2 years (RR = 1.69).
Conclusion
Preoperative vitamin D deficiency was associated with increased short-term medical complications and higher long-term risks of pseudoarthrosis and revision after single-level lumbar fusion. These findings support assessing vitamin D status preoperatively to identify patients at greater risk.
Keywords
Introduction
Vitamin D is an essential fat-soluble nutrient that plays a key role in calcium and phosphate homeostasis, muscle function, and immune regulation. Deficiency has been linked to increased risks of autoimmune conditions, infections, cardiovascular disease, and metabolic disorders.1-4 Among its many functions, Vitamin D is best recognized for its critical role in bone health. In the context of orthopedic surgery, adequate Vitamin D levels are necessary for bone healing and recovery, making its impact on postoperative outcomes an area of increasing clinical interest. 5 The most reliable marker of vitamin D status is the circulating metabolite 25-hydroxyvitamin D [25(OH)D, or calcidiol], which reflects both dietary intake and cutaneous synthesis. 4
Lumbar spinal fusion is a common procedure performed to address degenerative disc disease, instability, and other structural pathologies of the spine. 6 Several studies have evaluated outcomes in vitamin D deficient patients undergoing spinal fusion, but results have been mixed. Kerezoudis et al, reported that patients with preoperative vitamin D deficiency undergoing spine fusion had lower fusion rates and higher rates of recurrent or persistent low back pain compared to those with normal preoperative vitamin D levels. 7 In contrast, a meta-analysis by Khalooeifard et al. found no consistent differences in postoperative pain outcomes between deficient and replete patients. 8 Bajaj et al. further emphasized that vitamin D deficiency contributes to reduced bone mineral density, predisposing patients to complications such as vertebral fractures, instrumentation failure, and pseudarthrosis. 9 Interestingly, this study also investigated the role of preoperative vitamin D supplementation, but results were inconsistent: some studies reported higher fusion rates in patients who received supplementation, but others demonstrated no significant improvement in functional outcomes or disability scores. 9
Importantly, most prior work has focused on fusion success and pain scores, with less attention to broader postoperative medical and surgical complications. Given vitamin D’s established role in bone metabolism and its influence on multiple physiological systems, our large-scale retrospective study aims to evaluate the association between preoperative vitamin D deficiency and the risk of multiple medical and surgical postoperative complications after single-level lumbar fusion. We hypothesized that vitamin D deficiency would be associated with increased risks of both short-term and long-term complications. The results of this study aim to inform clinicians about the potential effects of preoperative vitamin D deficiency on lumbar fusion outcomes.
Methods
Data Source
This retrospective study utilized data from the Research Network within the TriNetX database (TriNetX LLC, Cambridge, MA). This globally federated network is a compilation of deidentified patient electronic health record data from 106 participating healthcare organizations from across the United States. Patient information was queried using Current Procedural Terminology (CPT) codes for procedures, International Classification of Diseases, Ninth and 10th Revision (ICD-9, ICD-10-CM) codes for diagnoses, RxNorm codes for medications, and TriNetX-curated codes for lab values. TriNetX provides curated laboratory values that are standardized across institutions, and RxNorm codes provide a standardized nomenclature for clinical drugs as established by the National Library of Medicine. TriNetX is compliant with the Health Insurance Portability and Accountability Act (HIPAA) since it contains only aggregated counts and statistical summaries of de-identified information as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. Therefore, this study was not subject to IRB review.
Inclusion and Exclusion Criteria
All adult subjects (age 18+) who underwent a primary single-level lumbar spinal fusion via a posterior or posterolateral approach were identified using CPT codes (22630, 22612, 22633). Patients were further divided into 2 cohorts: those with a most recent serum level of vitamin D3 [25(OH)D3] below 20 ng/mL that was measured between 1 year and the same day of single-level lumbar fusion surgery, and patients without a vitamin D deficiency diagnosis or without a 25(OH)D3 level below 20 ng/mL 1 year before their surgery. Patients were excluded if they had a previous diagnosis of scoliosis, spinal cord or vertebral neoplasm, had multi-level lumbar fusion, and if they did not have a minimum of 2-year follow-up after single-level lumbar fusion. Rather than using a previous vitamin D deficiency diagnosis code, the most recent TriNetX-curated lab value of 25(OH)D3 before surgery was used to define vitamin D deficiency to increase specificity for inadequate vitamin D levels. A value below 20 ng/mL was used as this is generally considered insufficient by several current practice guidelines.10,11
Demographics, Comorbidities, and Outcome Variables
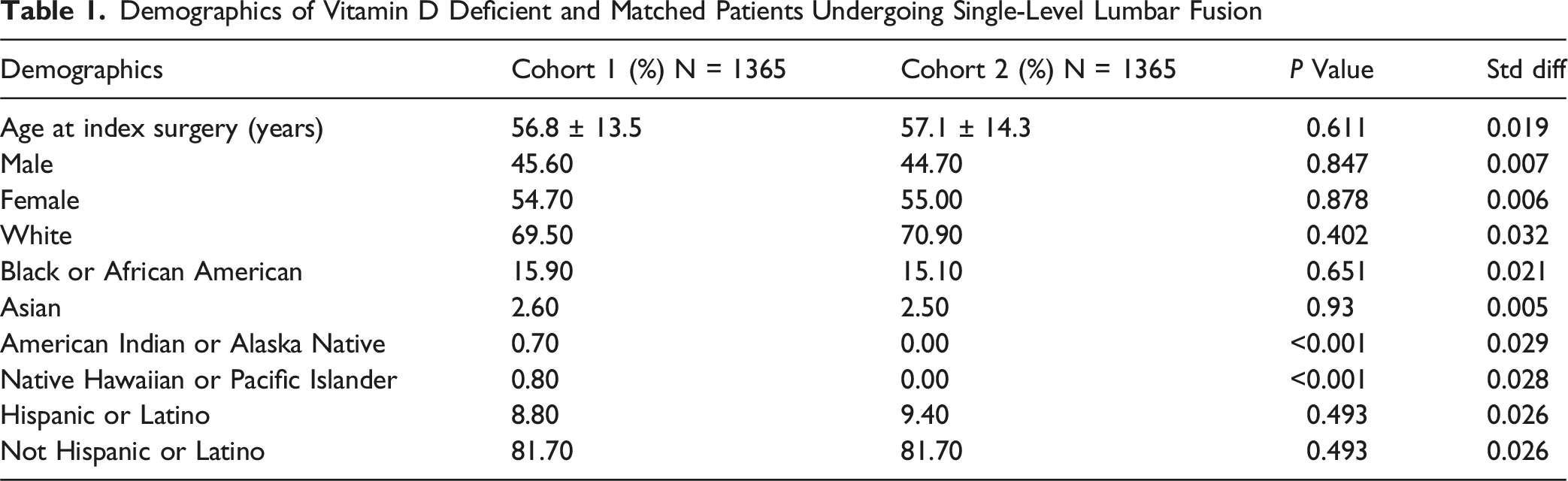
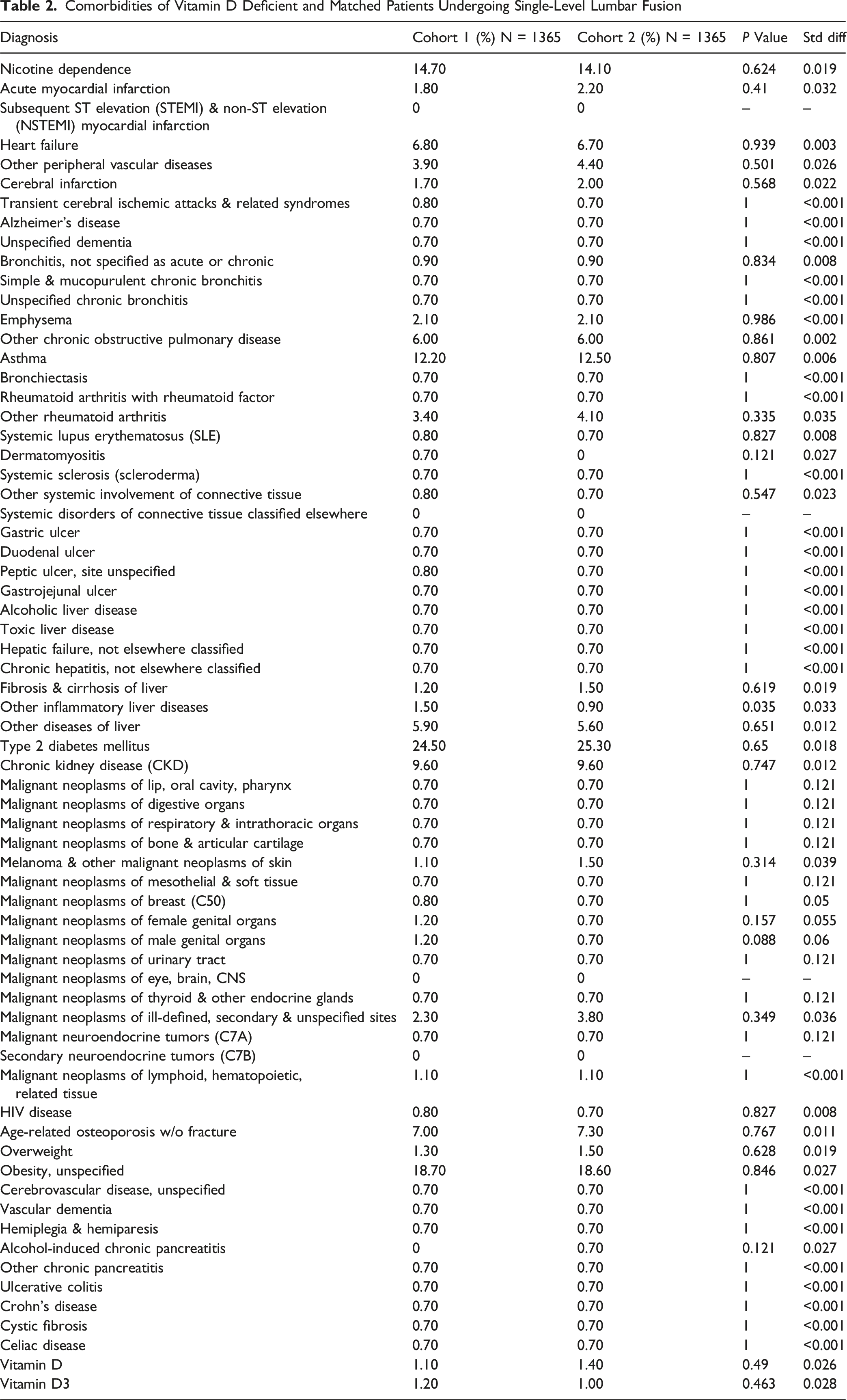
The vitamin D deficient cohort and non-vitamin D deficient cohort were propensity score matched (1:1) based on age at time of surgery, sex, race, ethnicity, Charlson Comorbidity Index (CCI), age-related osteoporosis, overweight, obesity, vitamin D supplementation, nicotine dependance, celiac disease, inflammatory bowel disease, cystic fibrosis, and chronic pancreatitis (Appendix A). Vitamin D supplementation was matched to control for patients in the vitamin D replete group who may be taking over the counter supplements. Balancing of covariates in the matched cohorts was completed using standardized difference (S-Diff), where values greater than 0.1 indicate imbalance.
Primary outcomes were incidence of medical complications 90 days after surgery and incidence of surgical complications 90 days, 1 and 2 years after surgery. Medical complications consisted of hospital readmission, emergency department (ED) utilization, deep vein thrombosis (DVT), pulmonary embolism (PE), pneumonia, sepsis, acute kidney injury (AKI), urinary tract infection (UTI), surgical site infection (SSI), and death. Surgical complications included instrumentation failure, pseudoarthrosis, and revision lumbar surgery (Appendix B).
Statistical Analysis
Statistical analysis was completed using the built-in analysis tool package within TriNetX. This consisted of risk ratios with corresponding 95% confidence intervals and chi-squared test for categorical variables to assess differences in outcomes. Statistical significance was set to P < 0.05.
Time-to-event analyses for revision were performed using Kaplan-Meier estimates with log-rank tests to compare survival curves. Cox proportional hazards models were used to calculate hazard ratios (HRs) with 95% confidence intervals. Time zero was the index surgery date, and patients were followed until the last encounter at 730 days postoperatively. In accordance with the TriNetX output, individuals with a documented revision prior to the analysis window were excluded from the Kaplan-Meier/Cox analyses.
Results
Demographics and Characteristics
Demographics of Vitamin D Deficient and Matched Patients Undergoing Single-Level Lumbar Fusion
Comorbidities of Vitamin D Deficient and Matched Patients Undergoing Single-Level Lumbar Fusion
Postoperative Outcomes
90-Day Outcomes
90-Day Outcomes of Vitamin D Deficient and Matched Patients after Single-Level Lumbar Fusion
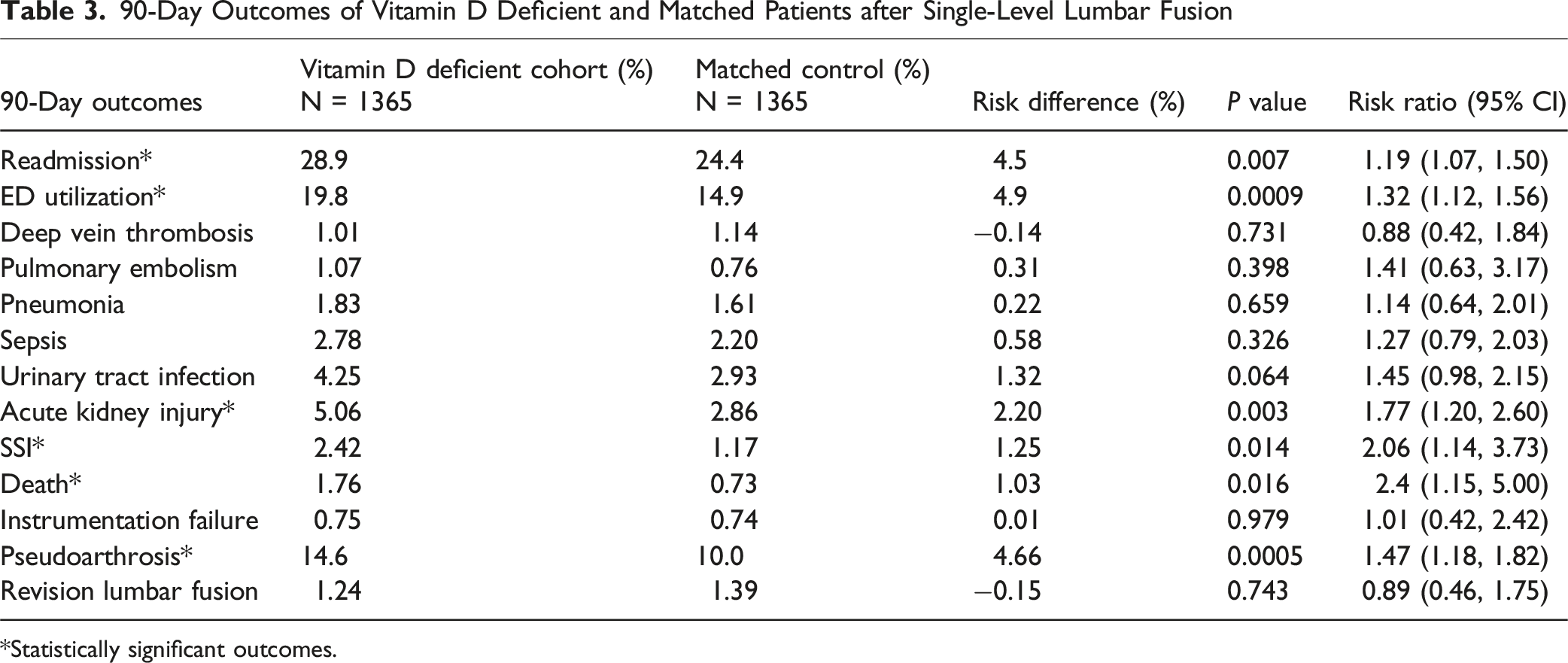
*Statistically significant outcomes.
1-Year Outcomes
1-Year Outcomes of Vitamin D Deficient and Matched Patients after Single-Level Lumbar Fusion

*Statistically significant outcomes.
2-Year Outcomes
2-Year Outcomes of Vitamin D Deficient and Matched Patients after Single-Level Lumbar Fusion

*Statistically significant outcomes.
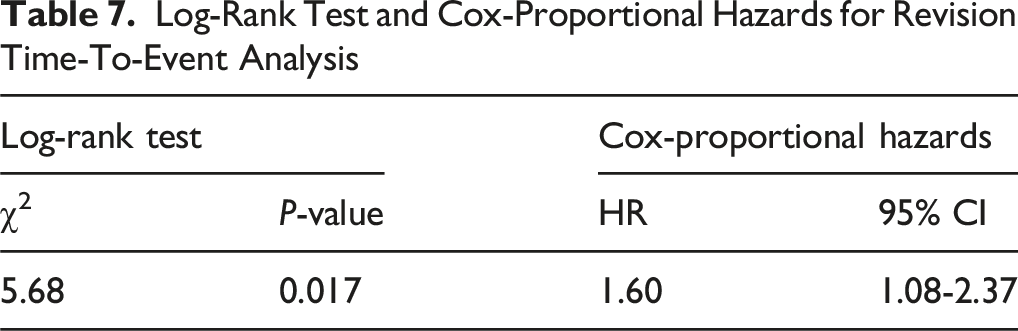
On Kaplan-Meier analysis, revision-free survival through 2 years was lower in the vitamin D-deficient cohort than in controls (93.83% vs 96.38%; log-rank χ2 = 5.684; P = 0.017) (Figure 1). Cox modeling demonstrated a higher hazard of revision in the deficient cohort (HR = 1.60; 95% CI, 1.08-2.37; P = 0.019), consistent with the higher 2-year revision proportion (5.20% vs 3.08%; RR 1.69; P = 0.007). For the Kaplan–Meier/Cox analyses, 1289 vitamin D–deficient patients (67 events) and 1297 controls (40 events) were included after excluding 76 and 68 patients, respectively, due to having outcomes prior to the time window (Tables 6 and 7). Two-Year Revision-free Survival after Single-Level Lumbar Fusion by Preoperative Vitamin D Status (Kaplan–Meier) Kaplan-Meier Summary of 2-Year Revision Outcomes by Cohort *76 patients in the vitamin D-deficient cohort and 68 patients in the matched controls were excluded because they had a revision code prior to the outcome window (signifying previous revision surgery likely in a different spinal region). Log-Rank Test and Cox-Proportional Hazards for Revision Time-To-Event Analysis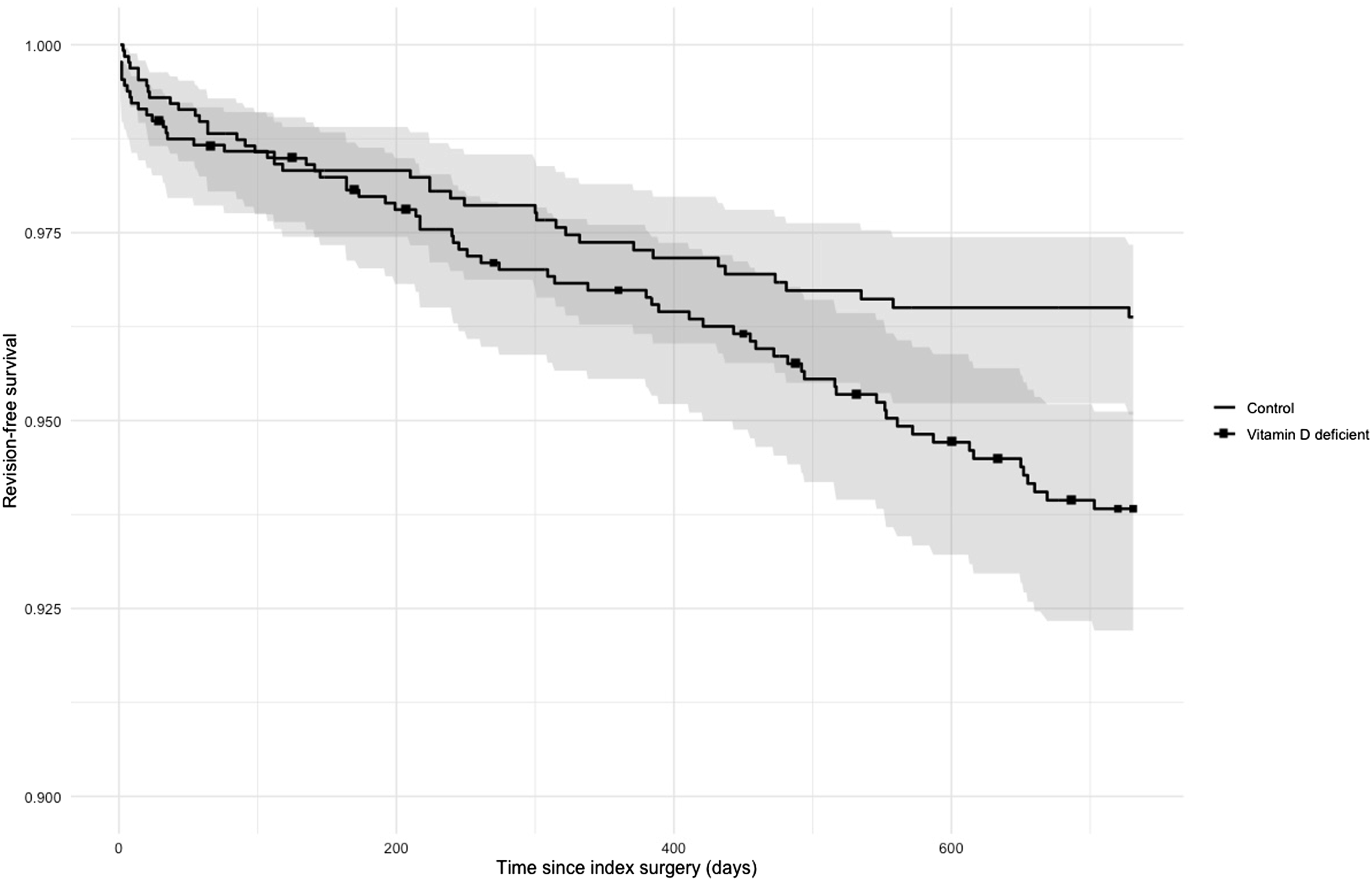

Discussion
In this large propensity-matched cohort, preoperative vitamin D deficiency in patients undergoing single-level lumbar fusion was associated with higher 90-day risks of hospital readmission, ED utilization, AKI, SSI, pseudoarthrosis, and mortality. At 1 year and 2 years postoperatively, vitamin D deficiency remained associated with an increased risk of pseudoarthrosis, and by 2 years it was also associated with a higher risk of revision surgery. No association was observed with instrumentation failure at any time point. These findings align with previous studies linking vitamin D deficiency to worsened postoperative outcomes, while also adding to the existing literature by describing a broader range of short-term medical and long-term surgical complications that have been understudied.
Vitamin D deficiency has been associated with worse bone health and impaired bone remodeling and healing processes, which are critical for adequate bone fusion after lumbar fusion surgery.12,13 These processes may explain the elevated rates of pseudoarthrosis we observed at all time points. Previous studies in the literature have demonstrated this result.14-16 Specifically, Yang et al, recently performed a meta-analysis of 39 cohort studies on spinal fusion surgery and identified vitamin D deficiency as a significant risk factor for fusion failure, with an odds ratio (OR) of 2.46 (95% CI, 1.24 to 4.90). 17 Interestingly, a randomized, double-blind controlled trial by Hu et al, administered vitamin D supplementation to the treatment group and demonstrated that these patients had shorter time to fusion (Kaplan-Meier: 169 days vs 185 days; log-rank P = 0.028) and significantly lower 6-month postoperative Oswestry Disability Index and Visual Analog Scale scores compared to those without vitamin D supplementation. Our large study with careful matching strengthens the association between vitamin D deficiency and pseudoarthrosis with higher risks at 90 days, 1 year, and 2 years.
Few studies in the literature have assessed the effect of vitamin D deficiency on rates of revision lumbar surgery and have instead focused specifically on fusion rates. One retrospective chart review of 150 patients, which included 36 patients with 25(OH)D levels below 30 ng/mL, reported no increased rates of pseudoarthrosis, revision, or hardware complications 1 year after lumbar fusion surgery compared to those with higher levels of vitamin D. 18 However, this study was likely underpowered, and while patients with lower levels of vitamin D were compared to those with higher levels, a 25(OH)D level of 30 ng/mL is not typically considered deficient. In our study, revision risk was similar through 1 year after surgery and higher in the vitamin D deficient cohort at 2 years. Time-to-event analyses further supported this pattern. Revision-free survival through 2 years was significantly lower in the vitamin D deficient cohort, and Cox modeling showed a higher hazard of revision. This difference in revision may be in part due to the cumulative impact of elevated pseudoarthrosis among follow-up, though causality cannot be established from this design.
Beyond fusion-related outcomes, vitamin D deficiency was also associated with infectious complications. Specifically, the significantly higher risk of SSI and near-significant rise in UTI among vitamin D deficient patients may reflect vitamin D’s specific role in epithelial defense and wound healing. In addition to vitamin D’s general immune modulation through its effects on innate immunity and T cells, it also increases expression of antimicrobial peptides found in keratinocytes, like cathelicidin and β-defensins, which are important for barrier protection and tissue repair. 19 In contrast, systemic infections such as pneumonia and sepsis are multifactorial and may not be strongly influenced by vitamin D status. Furthermore, because pneumonia and sepsis occur less frequently than SSI or UTI in lumbar fusion patients, the study may have been underpowered to detect subtle differences between groups. Although SSI reached statistical significance, its absolute risk difference of 1.25% is modest, and may indicate a low clinical significance.
Systemic effects were also observed with significantly increased rates of AKI and mortality in the vitamin D deficient group. This aligns with previous research that links vitamin D deficiency to worsened kidney function and major cardiovascular events,20,21 and with prior studies that have associated vitamin D deficiency with increased rates of all-cause and cause-specific mortality.22,23 However, because we elected to match for CCI, we did not include myocardial infarction and other cardiovascular events in our outcomes, which limits our interpretation of causes of death in our cohorts. Thus, the increased rates of SSI, AKI, death, and pseudoarthrosis (often presenting as pain and instability) likely led to the increased rates of hospital readmission and ED utilization seen in the vitamin D deficient cohort. Lastly, the absolute risk difference of mortality between both cohorts was modest (1.03%), and may not represent a clinically significant difference.
These findings suggest that assessing vitamin D status preoperatively could help identify patients at elevated risk of complications. Although causality cannot be confirmed from our study, these findings suggest that vitamin D status may represent a potentially modifiable marker of risk before lumbar fusion; however, this warrants prospective evaluation.
Limitations
Despite the significant findings of our study, several limitations must be acknowledged, especially those inherent to database research. This was a retrospective analysis of electronic health record data within TriNetX and therefore relied on information not collected directly by investigators. Although we used propensity score matching to account for demographics, comorbidities, and other potential confounders, residual bias remains possible. Important variables such as surgeon experience, perioperative care, bone mineral density, and severity of vitamin D deficiency were not available and may have influenced outcomes. Outcomes such as pseudoarthrosis and instrumentation failure were identified using ICD-10 codes, which may not perfectly capture radiographic or clinical diagnoses. Operative technique (eg, minimally invasive vs open) is not uniformly available in TriNetX and could not be controlled, although approach heterogeneity was reduced by restricting the cohort to posterior/posterolateral fusions.
Vitamin D supplementation was also difficult to assess. While we matched for supplementation prior to surgery, vitamin D is often taken over the counter and not consistently documented in electronic records; thus, some patients may have been misclassified. The dose and adherence to supplementation before surgery also could not be determined. Given the limitations of study design within TriNetX, we could not control for patients who began vitamin D supplementation after their surgery. Lastly, it was not possible to stratify patients within the vitamin D deficient cohort by level of deficiency, however, 70% of patients in this cohort had levels of 10-20 ng/mL.
Conclusion
Preoperative vitamin D deficiency prior to single-level lumbar fusion is associated with higher rates of 90-day readmission, ED utilization, AKI, SSI, pseudoarthrosis, and mortality. Vitamin D deficiency was also associated with a higher risk of pseudoarthrosis at 1- and 2-year follow-up, as well as increased revision surgery at 2 years. No significant differences were observed in instrumentation failure between groups. These findings underscore the importance of adequate preoperative vitamin D levels and may help surgeons identify patients with deficiency who may be at increased risk for worsened postoperative outcomes. Future prospective and randomized studies are needed to determine whether correcting vitamin D deficiency can mitigate these risks and improve long-term spinal fusion success.
Supplemental Material
Supplemental Material - Postoperative Complications of Single-Level Lumbar Spine Fusion in Patients With Preoperative Vitamin D Deficiency: A Retrospective Cohort Study
Supplemental Material for Postoperative Complications of Single-Level Lumbar Spine Fusion in Patients With Preoperative Vitamin D Deficiency: A Retrospective Cohort Study by Diego Garcia, Jonathan Sayegh, Bryce Michael, Yazin Hindosh, Arturo Lujan, Rami Khoshaba, Isam Sami Moghamis, Peter Du, and Abduljabbar Alhammoud in Global Spine Journal
Footnotes
Ethical Considerations
Data was acquired and analyzed using TriNetX software. TriNetX contains only aggregated counts and statistical summaries of de-identified patient information. As such, ethics approval was not required for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online