
Abstract
Study Design
Cross-sectional survey.
Objective
Although literature does not recommend routine wound drain utilization, there is a disconnect between the evidence and clinical practice. This study aims to explore into this controversy and analyze the surgeon preferences related to drain utilization, and the factors influencing drain use and criterion for removal.
Methods
A survey was distributed to AO Spine members worldwide. Surgeon demographics and factors related to peri-operative drain use in 1 or 2-level open fusion surgery for lumbar degenerative pathologies were collected. Multivariate analyses by drain utilization, and criterion of removal were conducted.
Results
231 surgeons participated, including 220 males (95.2%), orthopedics (178, 77.1%), and academic/university-affiliated (114, 49.4%). Most surgeons preferred drain use (186, 80.5%) and subfascial drains (169, 73.2%). Drains were removed based on duration by 52.87% of the surgeons, but 27.7% removed drains based on outputs. On multivariable analysis, significant predictors of drain use were surgeon’s aged 35-44 (OR = 11.9, 95% CI = 1.2-117.2, P = .034), 45-54 (29.1, 3.1-269.6, P = .003), 55-64 (8.9, 1.4-56.5, .019), and wound closure using coaptive films (6.0, 1.2-29.0, P = .025). Additionally, surgeons from Asia Pacific (OR = 5.19, 95% CI = 1.65-16.38, P = .005), Europe (3.55, 1.22-10.31, P = .020), and Latin America (4.40, 1.09-17.83, .038) were more likely to remove drain based on time duration, but surgeons <5 years of experience (10.23, 1.75-59.71, P = .010) were more likely to remove drains based on outputs.
Conclusions
Most spine surgeons worldwide prefer to place a subfascial wound drain for degenerative open lumbar surgery. The choice for drain placement is associated with the surgeon’s age and use of coaptive films for wound closure, while the criterion for drain removal is associated with the surgeons’ region of practice and experience.
Introduction
Avoiding postoperative complications in open spine surgery for degenerative lumbar and other conditions is of significant interest to surgeons due to concerns with readmissions, reoperations, and higher costs. 1 Today, there is significant variability in lumbar wound closure across surgeons around the world as well as with peri-operative wound management. 2 The variations in the incidence of wound-related complications may be due to the variability in the wound management practices by surgeons, including the use of drains. 3
Currently, postoperative drain utilization is highly dependent on surgeon preferences. Oftentimes, the drain is placed post-operatively empirically due to concerns of post-operative hematomas or compressive seromas. Post-operative drain placement may reduce the incidence of seroma, and postoperative hematoma that can lead to pain or neurological deficits and improve wound healing by decreasing wound tension.4,5 However, drains may also be associated with a higher incidence of postoperative infections by allowing a conduit for microbial access and colonization into the wound.6,7 In addition, drain placement can increase hospital stay and lead to patient discomforts.
While many surgeons prefer post-operative drains as a result of its perceived benefits over the potential infection risks, the current literature has its own limitations from its inconsistent results among various studies with conflicting results upon the routine usage of wound drains in spine surgery.8,9 In their systematic review on drain utilization, Muthu et al., 9 showed that routine drain use in spine surgery did not reduce surgical site infection, and the risk of post-operative hematoma did not increase without drain placement. Therefore, this current study aims to analyze surgeon preferences related to drain utilization. Additionally, we also aim to learn about factors that influence drain use and its management in open 1- or 2- level fusion surgery for lumbar degenerative pathologies.
Methods
Study Design
A survey designed to investigate the perioperative management of degenerative lumbar surgery was distributed to spine surgeons through the AO Knowledge Forum. Questions ranged from topics such as peri-operative antibiotic use, wound closure techniques, materials used and its management, along with the demographic information were included in the survey. Surgeons performing at least 10 cases of open 1 or 2-level fusion for adult lumbar degenerative pathologies annually were eligible for the study. Informed consent was not required since no specific patient data has been included in the study. Being a survey sent to the clinicians ethical committee approval was not obtained for the study.
Data Collection
The survey was distributed to over 6000 AO Spine members internationally and was conducted electronically in March 2022. Surgeon demographic information was collected including geographic region (Asia Pacific, North America, Latin America, Europe and Southern Africa, and Middle East and Northern Africa), gender, age, years of practice, specialty, and practice setting. The practicing age of the surgeons and their years of practice were categorized into predefined range clusters for the ease of analysis. In the drain domain of the study survey, surgeons were specifically asked regarding the placement of peri-operative wound drains in lumbar open fusion surgery, and specific questions on drain utilization includes the following: • Drain use (yes or no) • Placement of drain (deep or superficial to the fascia) • Days of post-operative drain utilization • Criteria for drain removal
Definitions
- Wound closure: Every participant surgeon could choose different alternatives to perform wound closure based on their preference from the muscular layer to the skin with the possibility to select multiple alternatives. - Unrestricted Range of Motion (ROM): The surgeons were asked about their preferred patient movement limitations postoperatively. If they did not restrict patients from the immediate postoperative stage to the final stage of recovery, they were considered unrestricted ROM. - Drain vs non-Drain groups: Surgeons that use peri-operative wound drain independent of any other preference were categorized as drain group (DG), while surgeons that do not use drains as a non-drain group (NDG). - Criterion of Removal: The drain group was analyzed according to the criteria by Shi et al
10
for the wound drain removal where the duration of the drain placement determines drain discontinuity for which the postoperative day is impacted. Alternatively, the drain may also be discontinued based on the drain output measured daily.
Statistical Analysis
Continuous variables were provided and analyzed as categories. For inter-group comparisons of categorical variables, Pearson χ2 analysis and Fisher’s exact test were employed as appropriate. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for each variable, in terms of its impact on the surgeon’s preference for drain utilization.
All possible independent variables collected through survey that might play a role in the drain usage were analyzed using univariate regression by forward entry and retained in the final model when P < .1. Multivariable analyses were performed to identify baseline and operative factors associated with drain utilization between the two groups, by binary logistic regression analysis. Data was exported for analysis into the statistical software program SPSS version 25 for Mac (IBM, Armonk, NY). A two-tailed P-value of <.05 was considered statistically significant.
Results
Two hundred thirty-one surgeons responded to the drain domain of the survey study on peri-operative management, including 220 males (95.2%) and 11 females (4.8%). Surgeons’ age ranged from 25 to over 65, with 7.4% between 25 and 34, 43.4% between 35 and 44, 28.1% between 45 and 54, 16.9% between 55 and 64, and 4.3% over the age of 65. Responses were obtained from an international community, with the largest group of respondents from Europe and Southern Africa (35.9%), followed by Asia Pacific (21.6%), North America (19.5%), Latin America (14.3%), and Middle East and Northern Africa (8.7%). Most respondents were orthopedic surgeons (77.1%) and academic/university hospital affiliated (49.4%). On the other hand, 27.7% of surgeons were affiliated with public/military hospitals, and 22.9% were in private practice. Finally, surgeon experiences among the respondents varied widely, and they were equally distributed across five age groups ranging from <5 years of experience to >20 years of experience.
Drain vs Non-Drain Utilization
Characteristics of Surgeons Preferring Drain versus Non-Drain Utilization.
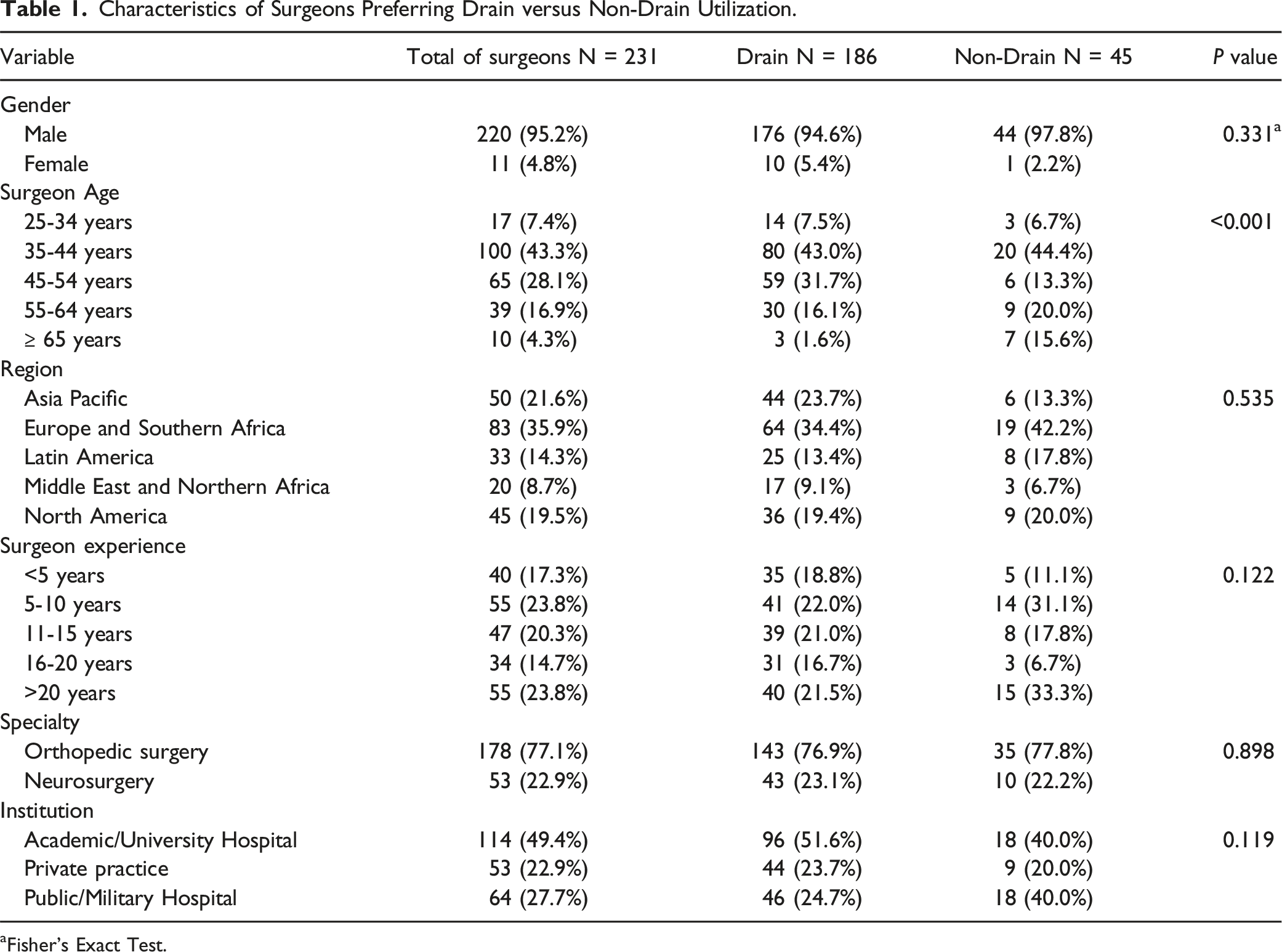
aFisher’s Exact Test.
Factors for Drain Utilization
Univariate and Multivariate Logistic Regression Analysis for Drain Utilization.
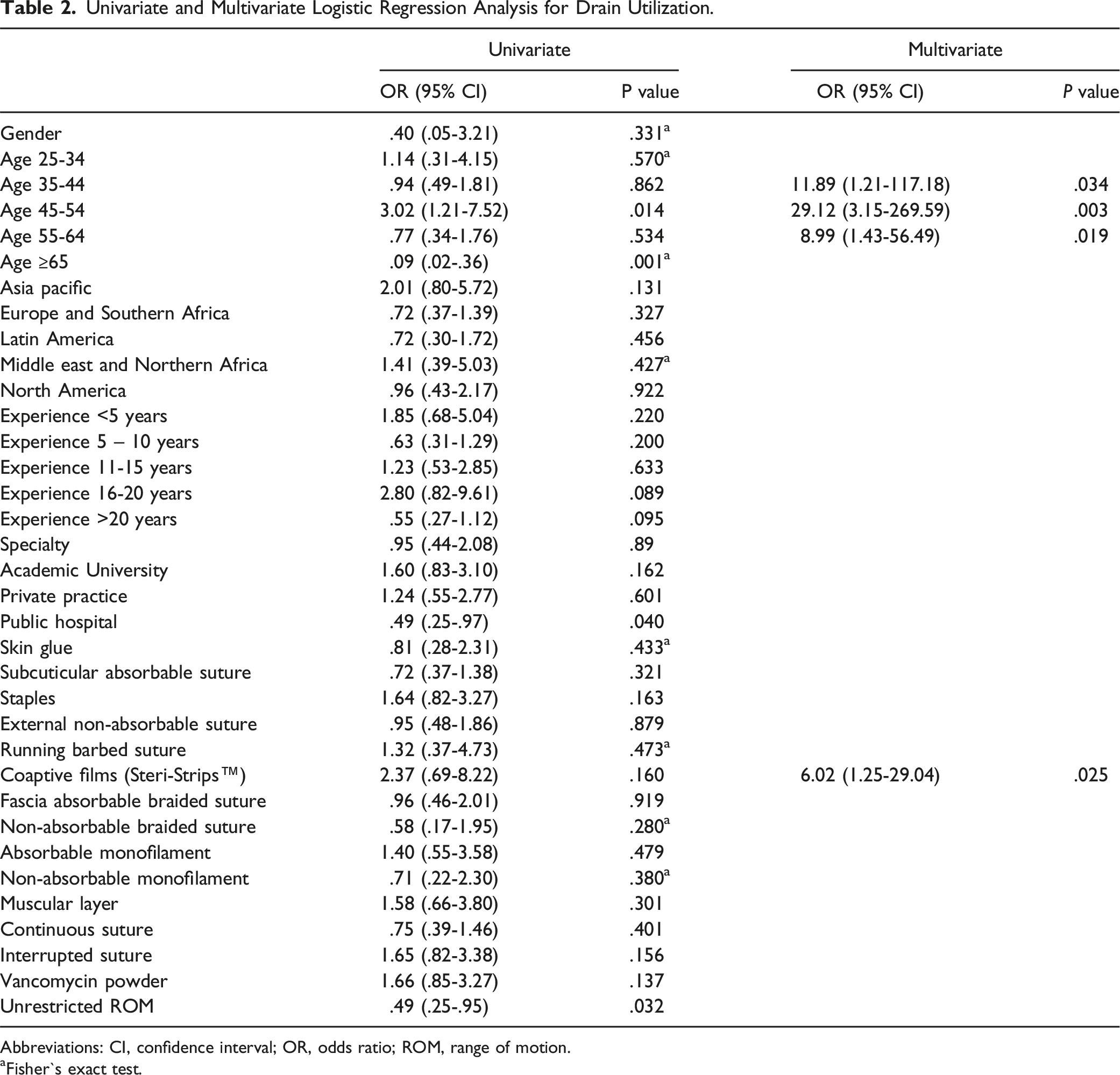
Abbreviations: CI, confidence interval; OR, odds ratio; ROM, range of motion.
aFisher`s exact test.
Drain Removal
Drain duration after placement was quite variable based on several factors. In this study, 52.8% of respondents determined drain removal by the duration of the placement, and most surgeons removed the drain on day 2 (30.7%). On the other hand, 27.7% of the surgeons based their decision for drain removal on the drain outputs, and the criteria of <50 mL daily output was most prevalent among surgeons in DG (14.7%), followed by daily output between 50 to 100 cc (10%) (Figure 1). Distribution of the surgeons according to drain preference and the criterion employed for drain removal by time or output (N = 231).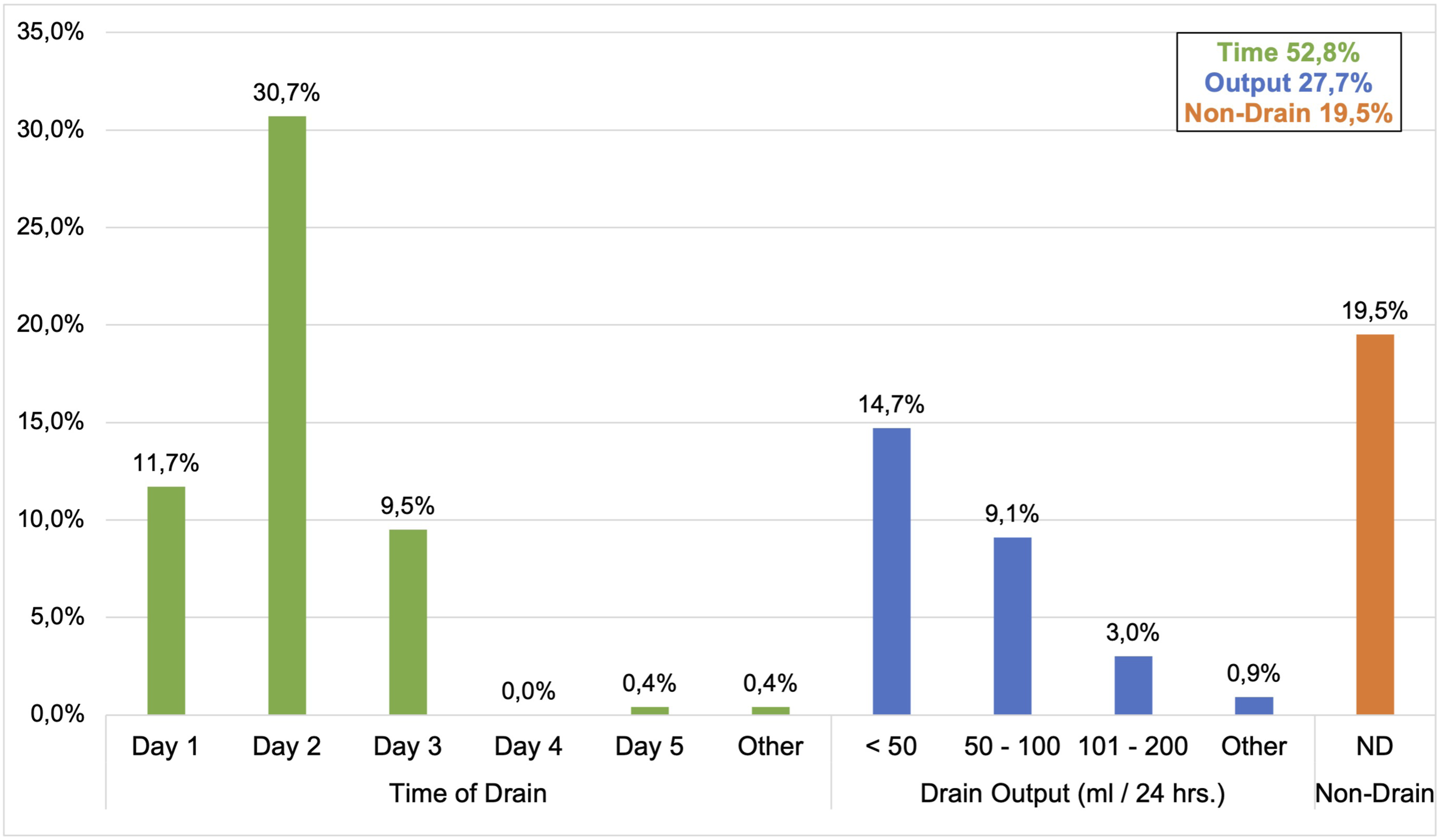
Characteristics of the Drain Group by Criterion of Drain Removal (N = 186).
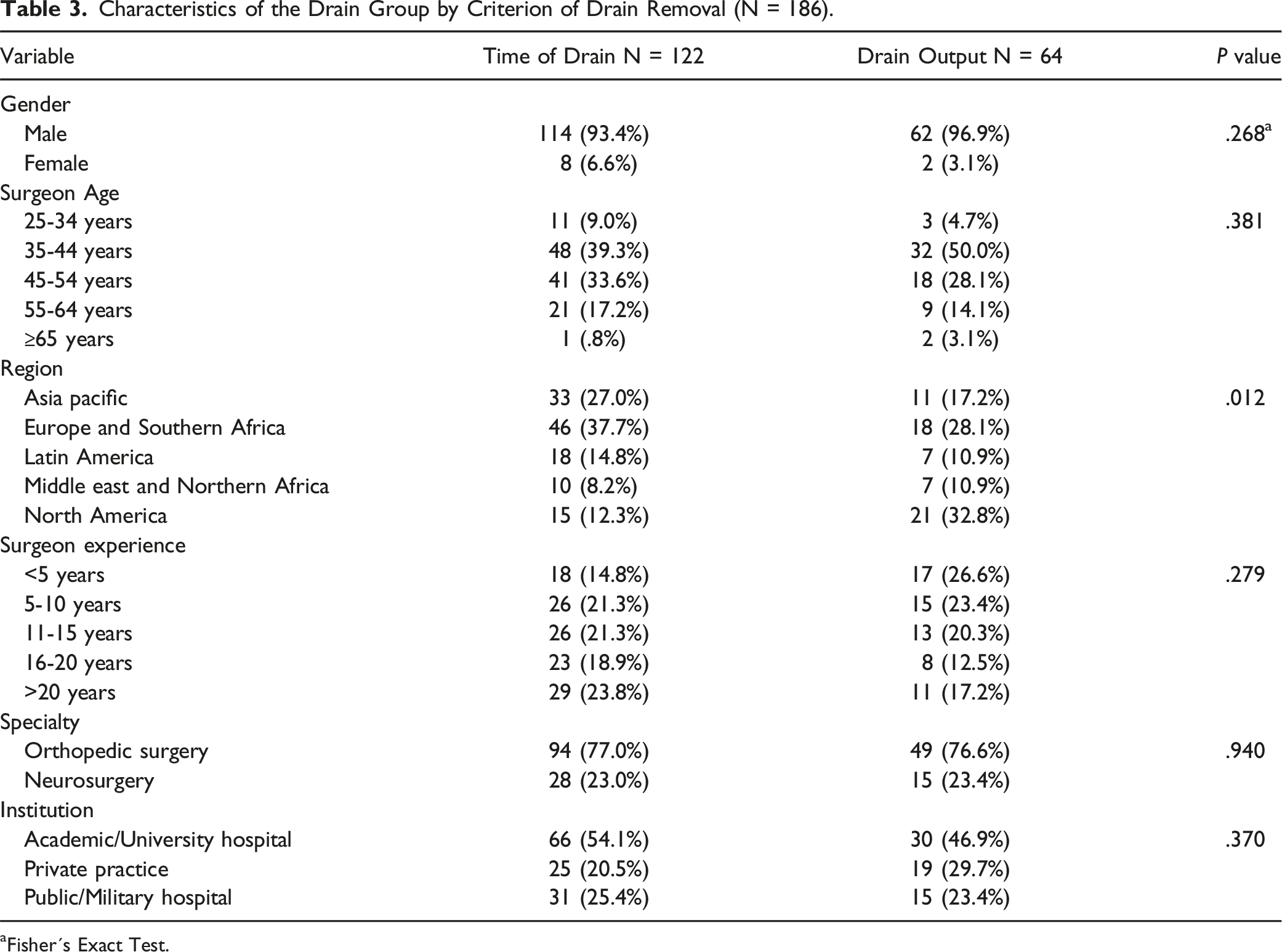
aFisher´s Exact Test.
Factors for Drain Removal
Univariate and Multivariate Logistic Regression Analysis for Drain Removal.
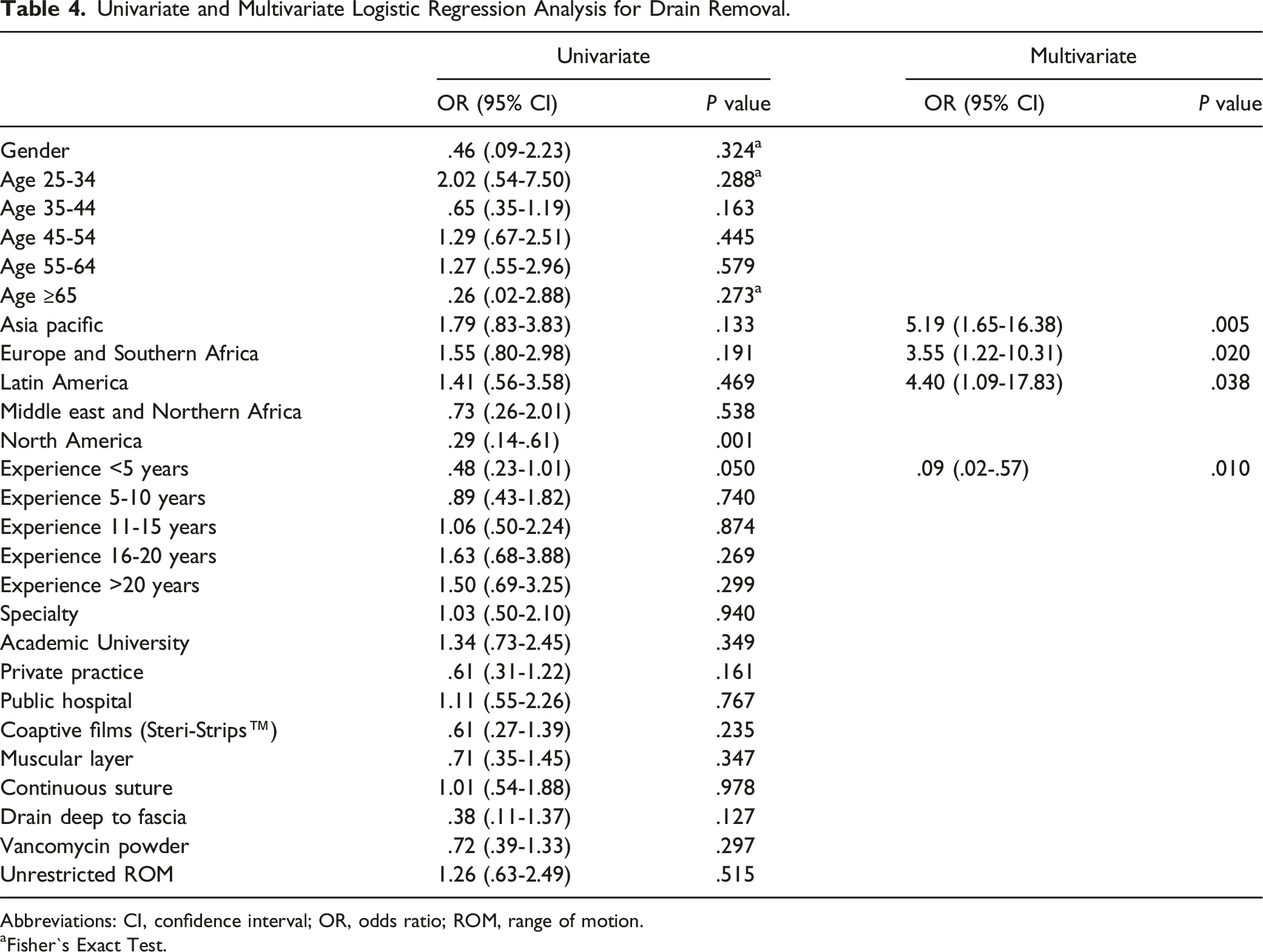
Abbreviations: CI, confidence interval; OR, odds ratio; ROM, range of motion.
aFisher`s Exact Test.
Discussion
The present study investigates the preference for peri-operative wound drain in open lumbar fusion surgery. Results of the study indicate that most spine surgeons from different regions worldwide still prefer to place a drain in their open surgery for lumbar degenerative diseases despite evidence that they may not be beneficial. 9 Notably, there is scarce literature on this specific issue in spine surgery. Our overall results indicate >80% of the respondent surgeons preferred drain utilization, and our findings correlate with previous literature reports regarding surgeon preferences for post-operative drain placement as part of wound closure. 2
In our multivariate analysis for predicting factors favoring the wound drain utilization, the surgeon's age and the employment of coaptive films (ie, Steri-Strips™) were significant factors. Coaptive film is an adhesive tape used to replace sutures in wound closure. 11 One possible explanation for more frequent drain use associated with coaptive film is that surgeons trust drains' ability to remove excess blood and create a negative pressure in the surgical wound to facilitate wound healing. 12 Therefore, coaptive films can be used with drains for time-saving in wound closure as an alternative to multi-layer closure without significant risk of wound complications. It can also be used for maintaining cosmetic purposes. 13 Further, the preference of drain use noted in the senior surgeons might be due to the controversies as identified in the literature that might prevent them from adopting their recommendations to their practise.
In our study, we found that surgeon preference for drain removal was based on time rather than output in majority of cases. Removal of the drain on post-operative day 2 was the most common practice. The most significant predicting factor for drain removal based on duration of placement was the surgeons’ region of practice. This might reflect the standard of care that is existent in these regions upon usage of wound drains. Alternatively, the decision for drain removal based on output was significantly associated with surgeon experience <5 years of practice. This might reflect the tailored approach followed by the early career surgeons. However, non-routine usage of wound drain which is considered as the best practice recommendation was not found to be related to the surgeon experience in our study. Shi et al. 10 compared the drain removal according to time vs output. Their study found beneficial effects with time driven drain removal on post-operative day 2, including less postoperative drain output, less blood loss, less length of stay and earlier postoperative mobilization without increasing the incidence of surgical site infection and symptomatic spinal epidural hematoma. The most commonly employed criteria for removal in their series was drain output <50 mL daily with drain removal typically on day 3. In a recent single-center retrospective cohort study performed by Karamian et al, 11 they demonstrated that drain duration or drain output did not affect the readmission rates following lumbar spine surgery. Therefore, surgeons should consider prompt removal of drain to minimize overall blood loss and length of hospital stay. In another single-centre retrospective study performed by Pennington et al, 12 they found an association between the prolonged drain retention and the risk of deep wound infection after degenerative spine surgery, with a drain retention time of the infected group of 5.49 days while 3.51 days for the non-infected group. Similarly, Egenolf et al, 13 showed that the drainage volume did not significantly increase in single level degenerative lumbar surgery after the evening of postoperative day 1. Therefore, drain removal is assumed to be safe after postoperative day 1. Having known from the literature analysis that utilization of drain increases the length of hospital stay, 9 early removal may be beneficial to avoid untoward complications which might be guided by the drain output cut-off or drain duration whichever is earlier. Other factors that might contribute to the drain removal include the drain pressure and the type of drain instrument. However, the current recommendations favour negative pressure wound drains in selected high-risk cases only. 14
Although the common rationale behind the use of drain is to prevent symptomatic haematoma formation and minimize the chance of surgical site infection, literature does not support this rationale and clearly nullifies the usage of drain on these grounds. 9 Our results showed that surgeons preferring a postoperative unrestricted range of motion were more likely to not use a wound drain, and it was found to be a significant factor in our univariate analysis (P = .032). However, it was not found to be significant as predicting factor for drain utilization on multivariate analysis. Postoperative exercise has demonstrated to reduce disability and pain following lumbar fusion surgery. 15 Drain utilization could potentially interfere with the early mobilization and increase patient discomfort. Drains can lead to less mobilization which is associated with a higher rate of medical complications such as pneumonia, deep vein thrombosis, and other infections. 16
A significant finding from our study is that drain use is prevalent even when the literature is not supporting the presumptive benefits of postoperative wound drains.6,8,9 Drain use is still being preferred by most surgeons around the world according to the findings of the present study. This phenomenon should have possible explanations. First, surgeons do not believe and follow the current literature results due to their experiences and concerns. They may believe that the reported studies are biased and poorly conducted, 17 so the results are not valid and reproducible in their centers. 18 Another possible explanation may be that drain use is propagated through surgical trainings, and the practice is maintained after the transition from training to clinical practice. 19
Literature Review
Summary of the Recent Literature Available Comparing Drain Utilization in Lumbar Surgery.
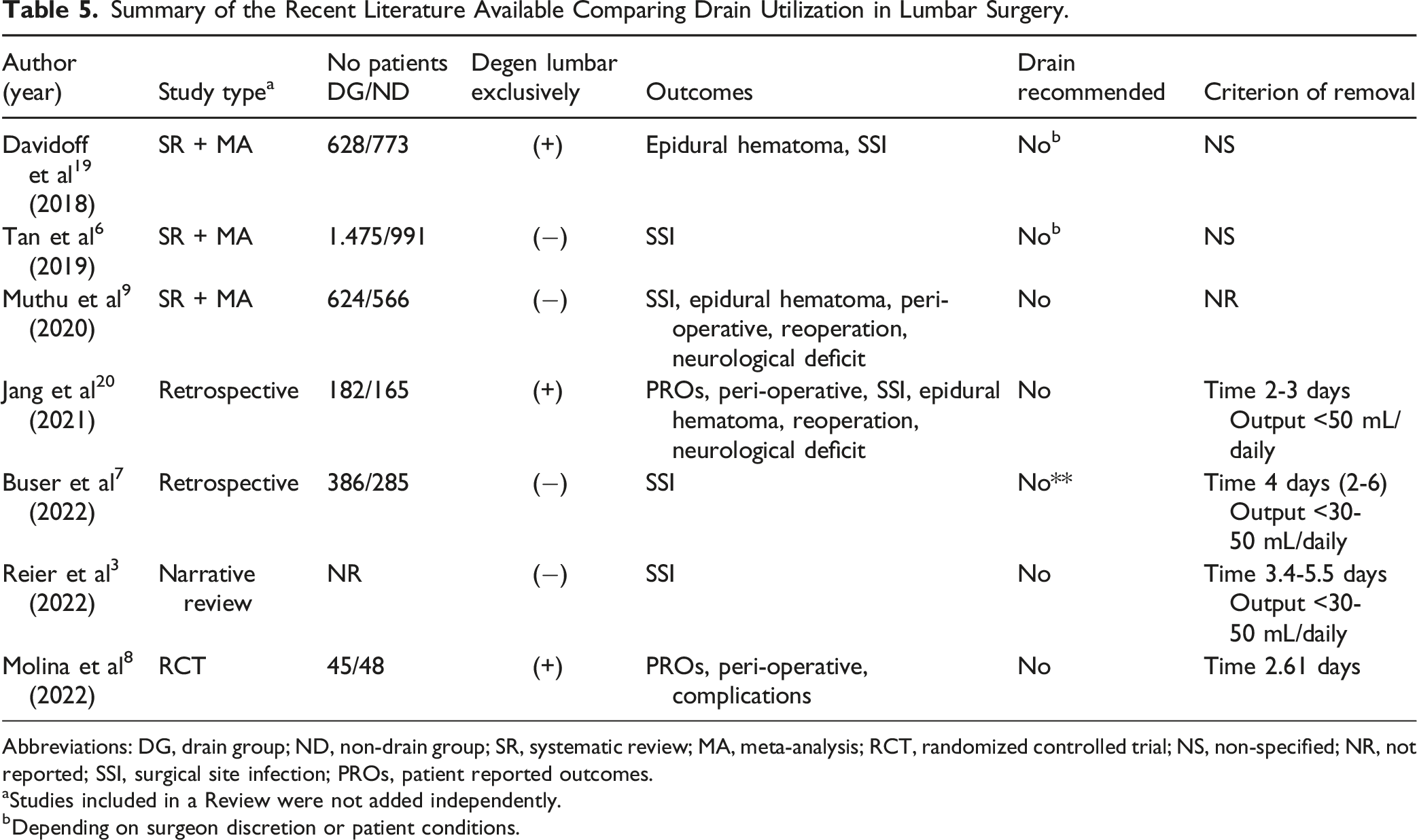
Abbreviations: DG, drain group; ND, non-drain group; SR, systematic review; MA, meta-analysis; RCT, randomized controlled trial; NS, non-specified; NR, not reported; SSI, surgical site infection; PROs, patient reported outcomes.
aStudies included in a Review were not added independently.
bDepending on surgeon discretion or patient conditions.
Another point of particular interest is the lack of a consensus recommendation regarding the criterion for draining removal after placement. In two systematic reviews with meta-analysis6,20 that included 628 and 1475 patients in the drain groups respectively, the criterion for drain removal was non-specified. However, in the most recent, high-quality, and comprehensive systematic review and meta-analysis with evidence summary using GRADE 22 methodology performed by Muthu et al, 9 the criterion for drain removal was not analysed. On the other hand, drain duration was the criterion for removal was reported in 4 of the 7 studies from 2018 to today. Drain removal was reported with 2-3 days of utilization in Jang et al 21 In the randomized controlled trial published by Molina et al, 8 the average time of drain placement was 2.61 days, between 3.4 and 5.5 days of drain duration in a narrative review done by Reier et al, 3 and 4 days (2-6 days) in the retrospective study performed by Buser et al. 7 However, there is consensus when the drain output criterion is employed for the decision-making that outputs lower than 30-50 mL daily are suitable for drain removal.3,7,21
Based on the systematic literature review and survey results, we find a disconnect between the current clinical practise and evidence-based wound drain usage recommendations. Although the evidence is compelling, we suggest future high-quality studies to explore into this issue to arrive at a definite conclusion considering all the patient and procedure factors that might play a role in the current decision to routinely use wound drains. Further, the optimal drain utilization approach in the high-risk individuals need further exploration.
Limitations
This study has several limitations. First, all the data represent the surgeon preferences related to wound drain utilization in open lumbar fusion surgery. These preferences could be influenced by local working-conditions and the availability of supplies. Secondly, though we sought to have a representative sample of spine surgeons from all the regions around the world, unfortunately the response rate was low among more than 6000 surgeons that received the survey which might introduce response bias and limited sample size potentially undermines the external validity of the study findings. Therefore, the accuracy and representation of this study to reflect the true sentiments and practices among surgeons around the world should be interpreted with caution. Further, the conclusions derived from the multiple subgroup testing has limited validity for generalization considering the number of responses analyzed in each of them. Thirdly, many other peri-operative factors were not analyzed as part of this focus study, such as blood loss, surgical duration, neurological status, patient reported outcomes, and others. Additionally, there is clinical heterogeneity in some studies of the literature review and must be analyzed carefully when compared with the results of the present study. Finally, we did not assess hypothetical clinical scenarios with different patient comorbidities and conditions that could impact the decision-making regarding drain utilization and wound management.
Conclusions
There is a disconnect between the current clinical practise and evidence-based wound drain usage recommendations. Although current recommendations do not favour routine drain usage majority of spine surgeons worldwide prefer to place a post-operative wound drain for open 1- or 2- level lumbar fusion surgery. The common practice noted is to place the drain in subfascial plane and its removal is based on the duration especially on day 2. Finally, the choice for peri-operative drain placement is significantly associated with the surgeon's age and the use of coaptive films (Steri-Strips™) for wound closure, while the criterion for drain removal varied significantly with region and surgeon’s experience.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine degeneration experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.