
Abstract
Study Design:
Cadaver study.
Objectives:
To investigate the risk of the L5 nerve injury following sacral ala decortication performed during lumbosacral posterolateral fusion surgery.
Methods:
Fourteen fresh cadaver pelvises were dissected through an anterior approach and the L5 nerves on both sides were explored and macroscopically examined by direct observation. Then, the corticotomy of the sacral ala was performed at 0°, 20°, and 30° angles to the sagittal plane through the posterior approach. The site of sacral ala decortication was checked on each side and its distance to the L5 nerve root was measured.
Results:
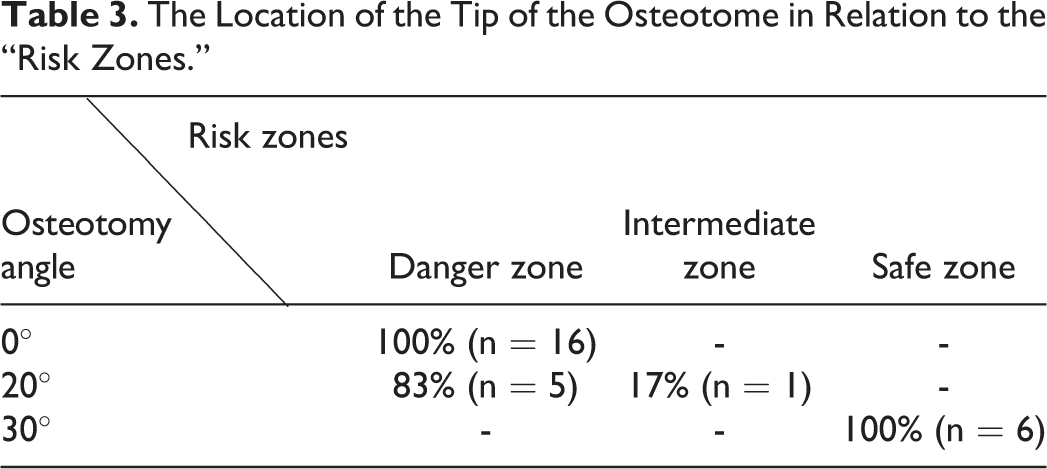
The tip of the osteotome was in the danger zone (5 mm medial to 5 mm lateral to the L5 nerve) in all cases (100%) where the osteotome had 0° angle to the sagittal plane. For those with a 20° angle, the osteotome tip laid in the danger zone in 83% and intermediate zone (between 6 to 15 mm lateral to the nerve) in 17% of cases. For those with a 30° angle, the tip was in the safe zone (>15 mm lateral to the nerve) in all cases (100%).
Conclusion:
Osteotomy of the sacral ala with <30° angle to the sagittal plane risks injury to the L5 nerve; whereas osteotomy angle >30° would not cause any injury to the nerve. It should be considered as a possible cause of iatrogenic L5 nerve injury in patients undergoing posterolateral lumbosacral fusion.
Introduction
Spinal fusion has been used for many years to treat several spinal pathologies including traumatic injuries, degenerative disorders, and deformities. Spinal fusion reduces the pain associated with spinal motion segments, counteracts the mechanical stresses experienced by the nerve roots, and partially corrects spine deformity, all of which results in reduced pain and improved function.
Among the most common techniques of spinal fusion are posterolateral fusion and interbody fusion; the latter of which is performed through anterior, posterior, retroperitoneal, and trans-peritoneal approaches. Lumbar spinal fusion is more frequent than cervical and thoracic fusions because these levels bear more motion and stress and consequently most spinal pathologies affect this area. 1 Each method of lumbar spinal fusion has advantages, disadvantages, and complications, according to which the surgeons adopt the proper approach. Posterolateral fusion can be performed in conjunction with other fusion methods; however, one of its serious complications is nerve root injury.2,3
Depending on the time of occurrence, surgical complications are categorized as intraoperative complications (bleeding, incidental durotomy, nerve root, and vascular injury), early postoperative complications (infection, hematoma, deep vein thrombosis, and transient or persistent radicular pain or dysfunction), and late postoperative complications (hardware failure, bone resorption, pseudarthrosis, and adjacent segment disease).2,3
Nerve root injury can occur due to inappropriate positioning, hematoma, improper hardware placement, or a direct injury. 2 Inoue et a1 4 reported 2 cases of iatrogenic L5 nerve injury due to perforation of the anterior cortex of sacral ala by S1 pedicular screws. In both cases, S1 pedicle screws were inserted outwardly and induced radicular pain by impinging on an L5 root. CT scan followed by selective rootgraphy of the injured nerve showed the nerve compressed laterally by screw threads in case 1 and crushed between the screw threads and the sacral body in case 2.
Another cadaveric anatomical study investigated the location of aortic bifurcation, inferior vena cava, and lumbosacral nerves in relation to the lumbosacroiliac triangle, emphasizing that it is crucial to have adequate anatomic knowledge of the lumbosacroiliac triangle in order to prevent vessel and nerve root injuries during surgery in this region. 5
L5-S1 fusion usually requires sacral ala decortication to remove the cortical bone and prepare a fusion bed for bone grafts. However, being done through the posterior approach, this method does not allow direct observation and protection of L5 nerves. Thus, the accidental direct blow of the osteotome is likely to injure the nerve root which is anatomically very close to the anterior cortex of the sacral ala. (deleted sentence)
Despite the increasing popularity of these surgeries among spine surgeons, limited information is available about the possibility of L5 nerve injury during sacral decortication. We designed this study to identify the risk of L5 injury by measuring its distance from the site of sacral ala osteotomy and define a safe zone to minimize the potential risk of iatrogenic injury to the nerve.
Material and Methods
This study was conducted on 14 randomly selected cadavers (28 samples in total). The inclusion criteria were having 20 to 70 years of age, and no history of previous tumor, infection, and surgery in the pelvis and lumbosacral region. Those who did not meet the inclusion criteria were excluded from the study. The study was ethically approved by the Ethics Committee of Shiraz University of Medical Sciences.
All dissections were performed by the first and second authors together. To find the L5 nerve through the anterior approach, the cadavers were placed in a supine position. A skin incision was made from the anterior superior iliac spine (ASIS) posteriorly along the iliac crest. The exposed fascia was longitudinally cut with a scalpel and the iliacus muscle was elevated off the iliac fossa as needed, exposing the L5 nerve lying over the anterior part of the ala of the sacrum entering the greater sciatic notch.
The same procedure was repeated on the opposite side. Then the cadavers were placed in the prone position and the spine was exposed through the standard posterior approach. A midline incision was made longitudinally over the lumbosacral region and paravertebral muscles were dissected subperiosteally and a self-retaining retractor was placed to give adequate exposure. Then the sacral alae were exposed bilaterally and decortication of the “alar dome” was performed by a 10 mm osteotome with 3 different angulations (measured by a divider) in the axial plane—0° (8 cases = 16 samples), 20° (3 cases = 6 samples) and 30° (3 cases = 6 samples) to the sagittal plane (Figure 1). Then, the cadavers were positioned laterally and the shortest distance from the osteotomy region (tip of the osteotome) to the L5 nerve was measured on both sides by using a ruler. The distances of 5 mm medial to 5 mm lateral to the L5 nerve were considered as the danger zone, 6-15 mm lateral to the L5 nerve as the intermediate zone, and distances of >15 mm lateral to the L5 nerve were considered as the safe zone.
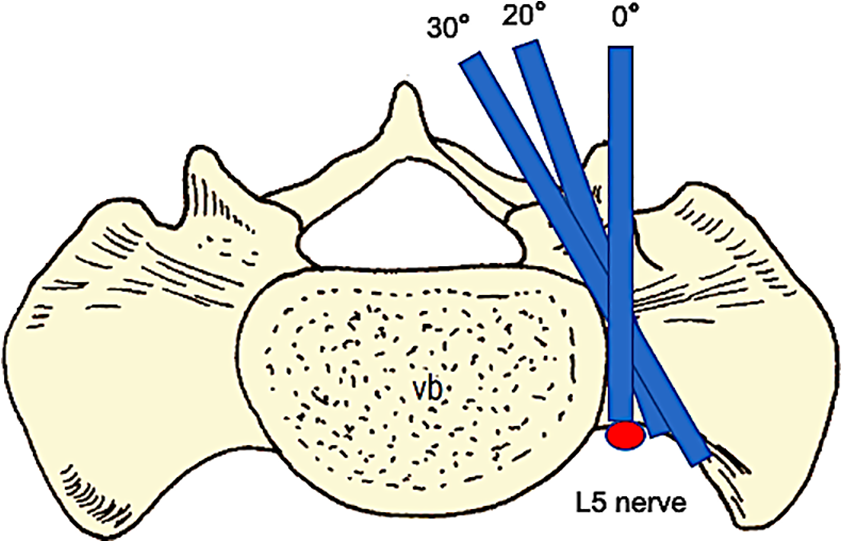
Schematic drawing of sacral anatomy and relation of the osteotomy angles to the L5 nerve location.
Results
Of all the studied cases, 72% were male (n = 10) and 28% were female (n = 4), with the mean age of 43.8 years (ranging from 21 to 67). In the 0° angle group, the tip of the osteotome penetrated into the danger zone in all cases (n = 16) (Figure 2); medial to the nerve in 31% (n = 5), lateral to the nerve in 50% (n = 8), and directly behind the nerve in 19% (n = 3) of cases (Table 1). In the 20° angle group, the tip of the osteotome was in the danger zone in 83% (n = 5) (Figure 3) and the intermediate zone in 17% of cases (n = 1). In the 30° angle group, all cases (n = 6) showed the tip of the osteotome lying in the safe zone (Table 2). The location of the tip of the osteotome in relation to the L5 nerve root according to the “risk zones” is depicted in Table 3.
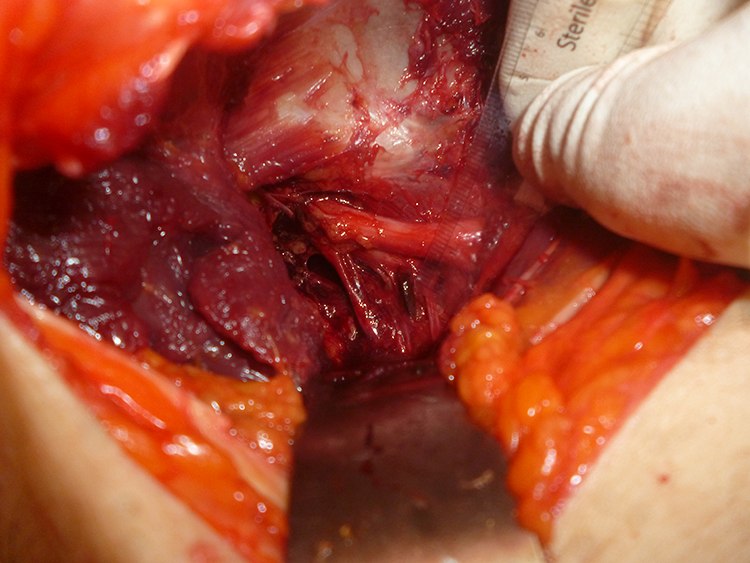
The tip of the osteotome touching the L5 nerve in a 0° corticotomy case.
Distance (in Millimeters) Between the Tip of the Osteotome and the L5 Nerve at 0° Angle of Osteotomy.
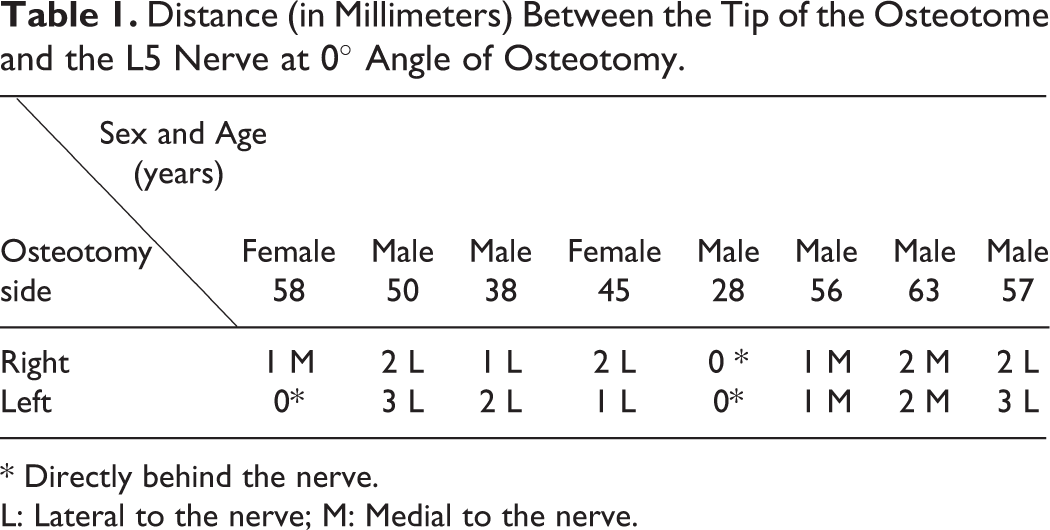
* Directly behind the nerve.
L: Lateral to the nerve; M: Medial to the nerve.
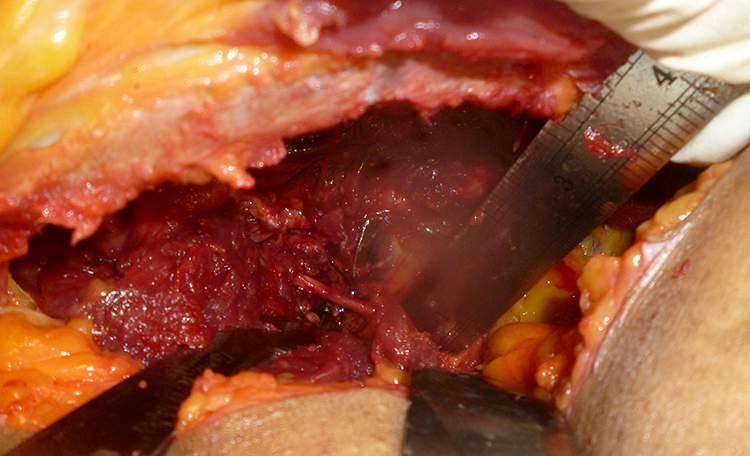
The tip of the osteotome lateral to the L5 nerve in a 20° corticotomy case.
Distance (in Millimeters) Between the Tip of the Osteotome and the L5 Nerve at 20° and 30° Angle of Osteotomy.
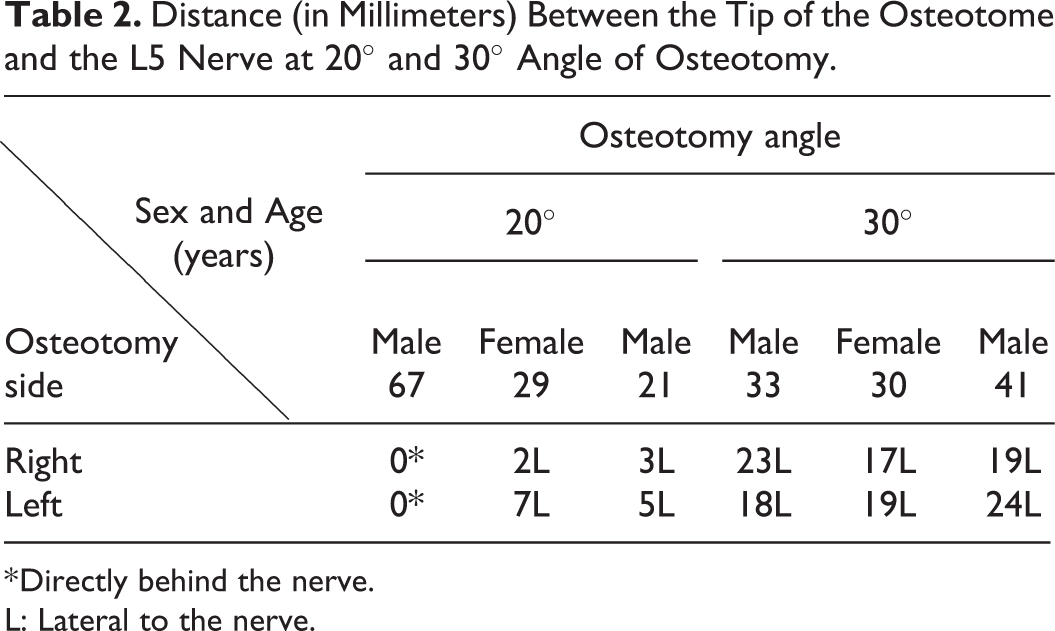
* Directly behind the nerve.
L: Lateral to the nerve.
The Location of the Tip of the Osteotome in Relation to the “Risk Zones.”
Discussion
One of the most serious and important postoperative complications of spinal fusion, especially in the lumbosacral region, is nerve root injury, which has always been a major concern for spine surgeons. The etiology may be multifactorial, including hematoma, nerve traction following alignment correction, hardware placement, direct root injury by a sharp instrument, and so on.
Our hypothesis in this study was that the anatomy of the L5 nerve and its close location to the sacral ala may make it vulnerable to direct injury during alar decortication which is intended to provide a fusion bed for bone grafts in the lumbosacral posterolateral fusion surgery. Considering this close anatomical relationship, it may be one of the contributing factors to radicular pain and temporary or permanent sensory-motor impairment associated with this nerve after spinal fusion surgery however, further studies are required to confirm this association.
A retrospective study on 361 cases of spinal fusion revealed the overall incidence of lumbar nerve root injury is 2.9%, with the L5 nerve being the most commonly involved. 6 In a retrospective comparison of complications between posterior and transforaminal lumbar interbody fusion in 119 patients, Mehta et al 7 reported iatrogenic nerve injury in 7.8% of PLIF and 2% of TLIF cases. Husono et al 8 retrospectively examined 240 consecutive PLIF cases for non-isthmic spondylolisthesis and reported a 17% incidence of transient and a 7.5% incidence of permanent neurological injury.
Matejbík 9 reported an extraordinary anatomical variation in the course of lumbar nerve roots and lumbosacral plexus which may have a significant effect on the incidence and clinical presentation of iatrogenic injury to these structures. In a study on 52 cadavers, Waikakul et al 10 investigated the course of lumbosacral nerve roots and their distance from the sacral ala and sacroiliac joint. They stated that L4 and L5 nerve roots lie close to the anterior surface of the sacroiliac joint and the ala of the sacrum and dissection with a sharp instrument should be avoided at sacral ala 5 to 7 mm medial to the sacroiliac joint to prevent iatrogenic injury to the nerve roots. They also have reported that almost one-third of the L4 nerve roots join the L5 nerve roots at the level above the most anterior part of the sacroiliac joint, suggesting that any trauma at this level could injure not only L5 but also L4 nerve roots.
In this study, we tried to find a simple and quantificational method to determine the risk of L5 nerve root injury during sacral ala decortication and its relationship to the direction of the osteotome. We noticed that if the surgeon drove the osteotome at an angle of zero degrees to the midsagittal plane, the tip of the osteotome in every case, entered the danger zone. In 5 samples (3 samples in the 0º and 2 samples in the 20º groups), the location of the tip of the osteotome was exactly behind the nerve and in all other cases, it was very close to it. As the angle of corticotomy to the sagittal plane was increased to 30º, the tip of the osteotome moved laterally into the “safe zone,” minimizing the risk of injury to the L5 nerve root.
Therefore, although decortication and removal of soft tissues over the sacral ala may improve successful fusion rate, great care must be taken to avoid inadvertent slipping off the tip of the osteotome or too far penetration through the anterior sacral cortex in order to avoid the direct blow and possible injury to the L5 nerve root.
One limitation of our study is that we only considered a direct impact of the osteotome on the nerve as a possible cause of the injury. However, even indirect pressure on the nerve, that can occur due to surrounding tissue distraction, hematoma, or a displaced cortical bone fragments by the osteotome can cause nerve irritation, regardless of the exiting point of the osteotome. Other limitations of this study are the small sample size and wide variety in the age of cadaveric specimens, which were mainly due to the limited availability of fresh cadavers. Future studies may also be designed to investigate the difference between the male and female pelvis and the vulnerability of vascular structures in front of the sacrum.
Conclusion
Based on the findings of this cadaver study, sacral ala osteotomy with <30° angle to the sagittal plane increases the risk of L5 nerve injury because of the close distance between the tip of the osteotome and the L5 nerve. We suspect that this might potentially contribute to the L5 nerve injury, which is experienced by some patients after posterolateral spinal fusion surgery.
Footnotes
Authors Note
This study was carried out in
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.