
Abstract
Study Design
Retrospective legal case review.
Objective
The aim of this study is to assess recent trends and risk factors for litigation against U.S. spine surgeons to better understand the current medico-legal landscape and inform future care in spine surgery.
Methods
The LexisNexis legal database was queried for case summaries from January 1, 2020, to October 6, 2024, yielding 432 results. Recent medical malpractice reports involving alleged spine surgeon error causing patient injury were included.
Results
Thirty-three cases met inclusion criteria. Most occurred in the South (52%) and Midwest (27%) U.S. All defendants were male spine surgeons (52% orthopedic, 48% neurosurgeons). Plaintiffs were 55% male. Most defendants were in private practice (66%); 30% worked in hospital systems. Surgeries occurred in hospitals in 61% of cases. Pain was the most common alleged surgical indication (42%), with lumbar fusions being the most frequent procedure (61%, lumbar 42%). Alleged injuries included persistent pain or radiculopathy (52%) and paraplegia (24%). The most-cited surgeon errors were failure to inform/obtain consent (21%) and cord damage (18%). Verdicts favored plaintiffs in 55% of cases. No variables were significantly associated with case outcomes (P > 0.05). When plaintiffs prevailed, the median payout was $1.62 million USD (IQR $600,000-$4.5 million USD).
Conclusions
These findings offer a limited snapshot of malpractice litigation themes in U.S. spine surgery, highlighting persistent issues with informed consent and communication. While not necessarily representative of all malpractice claims, these results may offer useful insights into potential areas for clinical and legal risk mitigation.
Introduction
Spine surgery is a highly complex surgical field spanning the domains of both orthopedic surgery and neurosurgery. Each year, over 900 000 Americans undergo spine surgery annually, 1 which spans procedures from minimally-invasive decompression and spinal cord stimulator placements to highly-complex spinal deformity correction and spinal cord tumor resection.2–5 Due to the complexity of spine pathophysiology and surrounding neurovascular structures, in addition to its critical role in the human body, spine surgeons must navigate a multitude of potential complications.6,7 Common cervical spine surgery complications include dysphagia and C5 nerve root palsy while the most common thoracolumbar complications include pseudoarthrosis and hardware failure.6,7 These complications not only pose a major health and financial burden, but often lead to high-stakes litigation against spine surgeons and their institutions.8–10
A review of the literature in 2021 demonstrated spine surgery remains one of the most litigious specialties in the United States healthcare system. 9 In addition, the authors reported a wide range of outcomes reported in the literature, with 54 to 75% of cases endly favorably for the surgeon. Unfortunately, such malpractice cases led to high monetary and time expenditures, and often motivated surgeons to defensively pursue unnecessary or unindicated tests and studies which further add to the financial burden and detract time away from medically necessary practices. 9 As such, it is critical to characterize prior spine surgery malpractice cases to inform future policies at improving healthcare efficiency and patient wellbeing. Makhni et al. conducted a Westlaw (Toronto, Canada) database study of 103 spine surgery malpractice cases from 2010 to 2014 and demonstrated 34% of cases involved complaints of lack of consent, and these cases averaged a compensation of approximately $2 million USD, while cases involving intraoperative complaints averaged a compensation of over $3.6 million USD. 10
Evidently, spine surgeons are at high-risk of litigation relative to other medical specialties, and these litigations have the potential to pose an enormous financial and time-related burden on surgeons, patients, and the healthcare system.8–10 However, there is a paucity in the literature on the recent spine surgery medicolegal landscape since 2020 in the United States. As such, the present study examined malpractice claims against spine surgeons from January 1, 2020, to October 5, 2024. This analysis aims to provide an updated understanding of the current state and trajectory of malpractice litigation in spine surgery in the United States, enabling spine surgeons and healthcare institutions to understand recent causes and characteristics of litigations to optimize medical care and institutional policies accordingly.
Methods
This study utilized LexisNexis, a comprehensive electronic database of legal records that includes case summaries, jury verdicts, settlements, and judicial opinions from trial and appellate courts across various jurisdictions in the United States. While the level of detail in these records varies, they typically provide party names, a factual summary of the alleged malpractice, and key dates such as when the malpractice occurred and when the case was resolved. LexisNexis was chosen as the primary data source for its recognized utility in scholarly analyses of medical malpractice litigation and its critical role in healthcare institutions’ recruitment and risk management practices. Since the study analyzed publicly available data from LexisNexis, Institutional Review Board (IRB) approval was not required.
Search and Selection Strategy
The LexisNexis database was searched for malpractice cases involving spine surgeons between January 1, 2020, and October 5, 2024. Spine surgeon involvement was defined as cases where an orthopedic- or neurosurgery-trained spine surgeon or institution representing a spine surgeon was listed as a defendant. Cases involving surgeries performed by non-spine surgeons or where spine surgeons served only as consultants were excluded. In effort to capture as many cases related to spine surgery, a comprehensive list of search terms was developed, which included: “spin* surg*” OR “spin* procedure” OR “back surg*” OR “spin* fusion” OR “lami*” OR “discect*” OR “diskect*” OR “microdiscect*” OR “microdiskect*” OR “kyphoplast*” OR “corpectom*” OR “spin* decompress*” OR “nucleoplast*” OR “foramin*” OR “spin* tumor” OR “spin* fracture” OR “dis* replacement”) AND (“orthopedic” OR “orthopaedic” OR “neurosurg*” OR “spin* surgeon”). This search initially identified 432 cases.
Relevant cases were organized in Microsoft Excel (Redmond, WA), and cases categorized under Social Security Disability Insurance, Workers’ Compensation, Healthcare Law, or Criminal Law were excluded as they were not relevant to medical malpractice. Additional exclusions included cases unrelated to spine surgery, those lacking identifiable malpractice claims, duplicates, or cases where the defendant was not clearly a spine surgeon or institution representing a spine surgeon who is alleged to have committed a perioperative or postoperative error. Two independent reviewers screened the remaining cases, resolving disagreements by consensus, yielding 33 recent spine surgery malpractice cases for analysis.
Data Extraction
Data pertaining to the following variables were extracted from cases meeting the inclusion criteria: state, geographic region, defendant’s name, defendant’s sex, defendant’s medical specialty (orthopedic surgery or neurosurgery), defendant’s clinical practice type (private individual or group practice vs hospital system), surgery setting (surgery center hospital), legal cause of action (negligence or procedural error), listed reason for surgery, type of spine surgery (eg, fusion, decompression, spinal cord stimulator placement), level of spine surgery (eg, cervical, thoracic, lumbar), type of harm (physical injury or death), nature of patient injury (eg, paraplegia, infection), alleged surgeon error (eg, wrong-level procedure, spinal cord or nerve root injury), litigation outcome, and compensatory figures (verdict or settlement amounts). State, federal, and municipal court dockets were consulted to fill information gaps if possible. In an effort to characterize the defendant physicians, an exploration of accessible physician directories, including Doximity (San Francisco, CA) and Healthgrades (Charlotte, NC), was conducted to ascertain the following variables: the defendant’s sex, defendant’s speciality training (orthopedic surgery or neurosurgery), and clinical setting. In instances involving multiple defendants, the primary spine surgeon named was selected for data extraction. The primary study endpoint was the legal disposition in favor of either the plaintiff or the defendant. Case outcomes were cataloged as plaintiff prevailing if the legal proceedings concluded with any nonzero verdict payment or settlement agreement. Conversely, outcomes were designated as the defendant prevailing if the verdict payment was null or the case was resolved through discontinuance.
Statistical Analysis
All statistical analyses were performed using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). Case characteristics were compared between the “plaintiff prevailed” and “defendant prevailed” cohorts, and between orthopedic surgery and neurosurgery specialty cohorts. Categorical variables were analyzed using Chi-square or Fisher’s test, as appropriate. Continuous variables were analyzed with the Wilcoxon rank sum test.
Results
Overall Case Characteristics
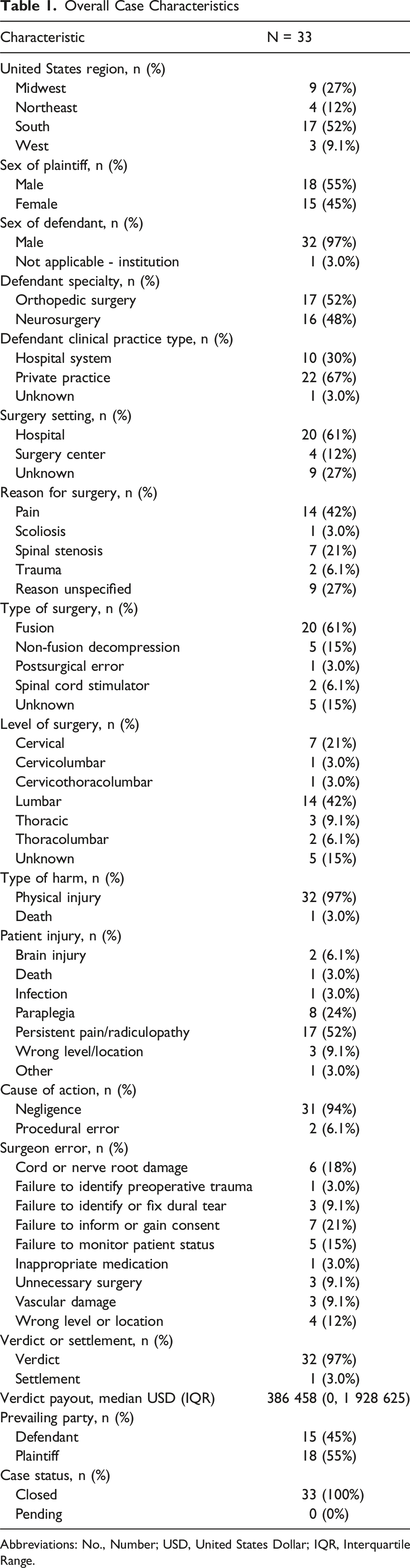
Abbreviations: No., Number; USD, United States Dollar; IQR, Interquartile Range.
In terms of adverse outcomes, nearly all cases (97%, N = 32) involved physical injury, while one case (3%) resulted in death (Table 1). The most frequently cited patient injury was persistent pain or radiculopathy (52%, N = 17), followed by paraplegia (24%, N = 8), wrong-level or wrong-side surgery (9.1%, N = 3), and brain injury (6.1%, N = 2). Infection (3%, N = 1) and postoperative death (3%, N = 1) were rare occurrences. The types of alleged surgeon errors resulting in litigation varied, with failure to inform or obtain proper consent being the most common (21%, N = 7), followed by spinal cord or nerve root damage (18%, N = 6) and failure to monitor patient status (15%, N = 5). Other cited errors included failure to recognize or effectively repair a dural tear (9.1%, N = 3), wrong-level surgery (12%, N = 4), and unnecessary surgery (9.1%, N = 3). The vast majority of cases were brought under claims of negligence (94%, N = 31), while procedural errors were identified in 6.1% (N = 2) of cases.
Case Characteristics and Outcomes
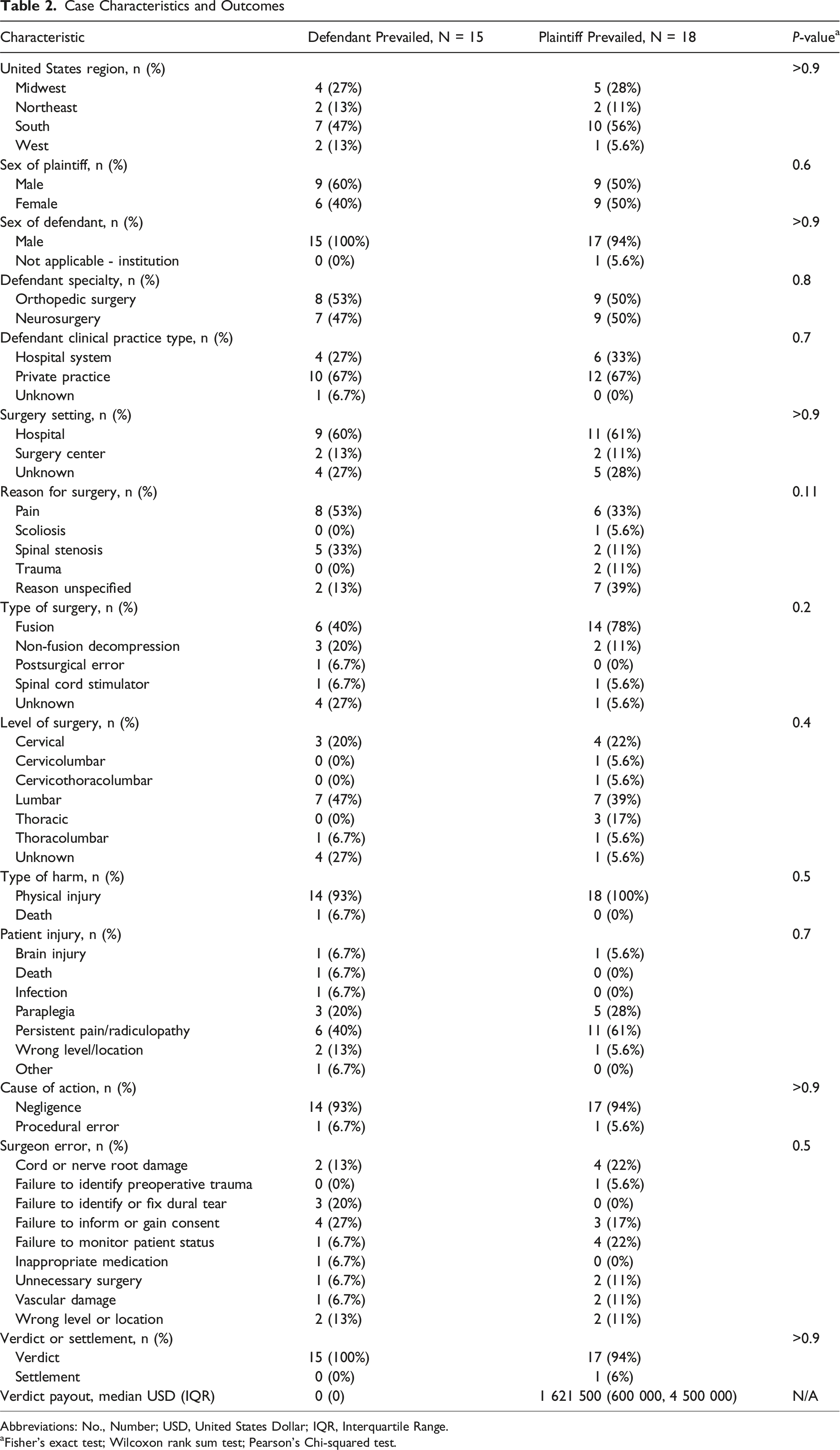
Abbreviations: No., Number; USD, United States Dollar; IQR, Interquartile Range.
aFisher’s exact test; Wilcoxon rank sum test; Pearson’s Chi-squared test.
Orthopedic Versus Neurosurgery Spine Surgery Case Characteristics
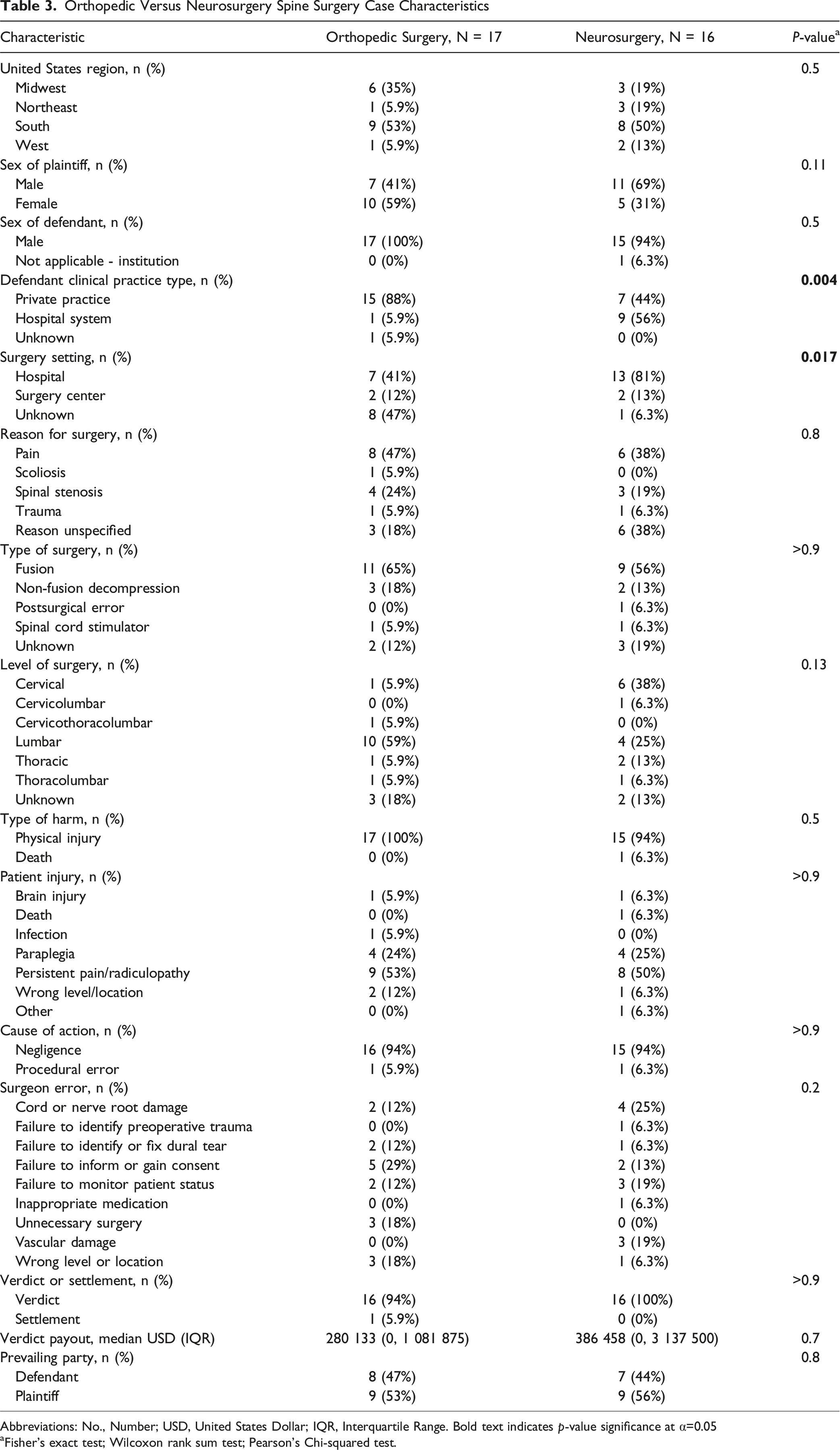
Abbreviations: No., Number; USD, United States Dollar; IQR, Interquartile Range. Bold text indicates p-value significance at α=0.05
aFisher’s exact test; Wilcoxon rank sum test; Pearson’s Chi-squared test.
Discussion
A deeper understanding of medical malpractice cases involving spine surgeons is crucial for enhancing the quality of care across both orthopedics and neurosurgery. Due to the complex nature of postoperative care, orthopedic and neurosurgery spine surgeons are at a higher risk of facing medical malpractice lawsuits in the United States,11,12 with over 19% of neurosurgeons and 14% of orthopedic surgeons facing a malpractice claim each year during a study period from 1991 to 2005. 13 In neurosurgery, spine surgery faces a significantly greater likelihood of a claim than cranial surgery. 14 Previous literature has investigated medical malpractice in the spine surgery field, aiming to further the characterization of plaintiff demographics and allegations against spine surgeons.8–10,15–17 As such, our study aimed to provide an update to medical malpractice characteristics in spine surgery, although it reflects a limited sample of publicly available cases in the U.S. and thus provides descriptive insight rather than necessarily being generalizable to all broader litigation trends.
Thirty-three cases were included in the present LexisNexis database analysis from January 2020 to October 2024. There was a split among orthopedic surgeons and neurosurgeons as the defendant, of which 45% of defendants prevailed. Cases were more common in the South and Midwest, however there was no difference in outcome based on geographic region or surgeon specialty. The most common type of procedure was fusion, with the lumbar spine being the most operated spine region. Failure to inform or attain consent was the most frequent surgeon error cited in case summaries, followed by cord damage. The hospital setting was the most common location for clinical practice as well as surgery setting. There were no significant associations between any collected case summary variables and litigation outcomes.
An uneven regional distribution was observed, with more cases in the South and Midwest, and the least number of cases in the West. This is in alignment with a prior study by Zhang et al on elective lumbar spine fusion litigations, which demonstrated similar findings with the South having the greatest number of total malpractice claims, with the fewest absolute number of cases in the West. 15 When analyzed by state, prior spine surgery malpractice studies have demonstrated California to have the highest absolute number of malpractice cases.15,16 However, these findings are likely heavily influenced by the number of actively practicing orthopedic and neurosurgery spine surgeons in various regions of the United States. Future studies are necessary to determine if differences in regional resources, surgeon training, and institutional protocol contribute to malpractice case prevalence.
Overall, spine surgeon defendants were 100% male in the 33 cases included for analysis. This likely related to the underrepresentation of female surgeons in both orthopedic surgery and neurosurgery, with recent data demonstrating female surgeons comprising less than 9% of neurosurgeons and orthopedic surgeons.18,19 Interestingly, there was a relatively even number of orthopedic spine surgeons and neurosurgeons as the listed defendant in the cases, despite the greater number of orthopedic spine surgeons in the United States. 20 A prior spine surgery malpractice analysis from 2010 to 2014 reported a similar distribution, attributing 49 malpractice litigations against orthopedic surgeons and 42 litigations against neurosurgeons. 10 However, in a long-term investigation from 1988 to 2015, Daniels et al observed 58% of all cases were against orthopedic surgeons while only 34% were against neurosurgeons, 16 despite workforce trends demonstrating orthopedic spine surgeons have been outpacing neurosurgery spine surgeons in the United States. 21 Although future studies are needed to ascertain the causes of this disparity, these findings may reflect neurosurgeons taking on higher-risk spine surgeries than orthopedic surgeons, leading to higher representation in recent litigations.
Surgical characteristic analysis demonstrated the lumbar spine was the most commonly operated level, while fusion was the most common surgery type. Similarly, prior spine surgery litigation analysis by Jackson et al. reported the lumbar spine constituted 45%-65% of claims across 23 publications on spine surgery litigation. 9 Makhni et al. noted 64 lumbar procedures relative to 27 cervical and 8 thoracic procedures in their malpractice analysis. 10 These findings are consistent with the lumbar spine being the most frequent site of spinal injury, as well as the most commonly operated site for surgical procedures.22,23 Spine fusions have also been previously documented as the among the most commonly performed spinal surgeries, potentially increasing the likelihood of litigation.24,25 In addition to our findings, Daniels et al. noted 41% of 220 spine surgery malpractice cases concerned spinal fusions, which was notably higher than decompressions (15%), discectomies (20%), or laminectomies (24%). 16
The most commonly cited alleged surgeon error in recent spine surgery lawsuits was the failure to properly inform patients or obtain patient consent, followed by direct spinal cord damage. These results on recent spine surgery malpractice claims are consistent with Agarwal et al, which analyzed litigation reports from 2010 to 2015 and found the perceived lack of informed consent as the second highest factor for lawsuits. 8 However, the main reasons for patient litigation were claimed to be procedural errors. Furthermore, Makhni et al. reported the most common complaints to be technical or judgement, nerve injury, and lack of informed consent. 10 A prior study on lack of informed consent in spine surgery malpractice cases demonstrated the most common cited failures were specifically in neglecting to explain the risks and adverse effects of surgery. 17 Unfortunately, our findings indicate a potential lack of improvement over time in surgeon-patient communication as it relates to reasons in malpractice litigations. Our findings are also consistent across surgical fields, as inadequate informed consent is a major factor cited as a cause of malpractice claims in fields from plastic and reconstructive surgery to otolaryngology.26,27 Given the median plaintiff payout exceeding $1.5 million USD, greater efforts must be made to improve clinician-patient communication in spine surgery. Our findings emphasize the increasing importance of institutional policies and individual clinician efforts to improve communication between patients and the entire healthcare team, in the context of a larger shared decision-making model that prioritizes patient autonomy. Such efforts may aid in avoiding costly and unnecessary lawsuits and improve patient satisfaction in the spine surgery setting.
Regarding patient symptomatology and injury in recent malpractice claims, persistent pain was the most common reason for surgery, as well as for litigation. A similar analysis was performed by Zhang et al. with their study on 310 lumbar fusion cases from 1970 to 2021 using the Westlaw legal database. 15 They found refractory postoperative pain as the most common injury resulting from the surgeon’s alleged negligence. Despite the highly skilled operative ability of orthopedic surgeons and neurosurgeons, spine cases have a high level of complexity and may not always yield expected results. With respect to primary institutional affiliation and surgical setting, neurosurgeons were significantly more likely to be affiliated with hospital systems and performed surgery at higher rates in the hospital setting relative to orthopedic surgeons. However, these differences had no association with verdict outcome, suggesting no clear impact of institutional affiliation or surgery setting on risk of malpractice. However, prior literature suggests continued caution and thorough risk-benefit assessment regarding patient selection for spine surgery in the ambulatory vs hospital setting are necessary to optimize outcomes.28–30
The findings that defendants prevailed in 45% of the recent cases highlights the high burden of malpractice cases in spine surgery. This rate is notably lower than as reported in prior spine surgery malpractice studies, which have collectively reported a verdict favoring the defense in 54% to 75% of cases. 9 A verdict favoring the defense in less than half of recent cases is unfavorable and may be most attributable failures in proper consenting and effective communication with patients, the highly specialized nature of the field, and the inherent risks related to spine surgery. Additionally, the COVID-19 pandemic may have indirectly contributed to this trend. The pandemic caused widespread delays in elective surgeries and strained healthcare systems, which may have hindered preoperative communication, thorough patient assessments, and exacerbated existing issues in surgical decision-making, potentially leading to the increasing likelihood of lawsuits. 31 Furthermore, the overall sense of vulnerability among patients during the pandemic may have increased dissatisfaction with surgical outcomes, contributing to a rise in legal actions. However, given the study’s small sample size and restricted data source, these results set the stage for more robust research on international trends in malpractice claims in recent years. Future research using more comprehensive datasets is necessary to confirm these trends and support generalizable conclusions.
Nevertheless, our findings highlight the importance of thorough documentation of patient visits and procedural notes, as well as physicians’ commitment to adhering to best practices. This is especially essential to spine surgery, as adverse surgical complications and poor outcomes can result in debilitating pain or functional limitations that severely impairs quality of life, or results in patient death. 32 This is especially important to consider given that the median payout for these cases exceeded $1.5 million USD in the present study. Such litigations in spine surgery may lead to significant financial losses, possibly equating to several years’ worth of income and reputational damage to physicians or institutions. 32 The complexity of these findings cannot be understated. With the rise of medical malpractice cases and efforts to discourage frivolous lawsuits, some states have enacted legislation that places a cap on these payouts. 33 However, these measures may infringe on patient rights by limiting the compensation for legitimate claims, underscoring the need for a balanced approach to ensure fairness to both patients and healthcare providers.
On a final note, in response to concerns highlighted by such malpractice claims, hospitals have implemented communication-and-resolution programs (CRPs), which aim to facilitate discussions about medical injuries with patients and families. 34 CRPs aim to engage patients experiencing adverse outcomes, such as those detailed in this study, by acknowledging the unfavorable events, complex emotions, and providing proactive compensation to mitigate patient harm and future incidences. 35 However, in cases involving CRPs, compensation was less frequently provided in instances of substandard care. Nonetheless, these programs were generally well received by both practitioners and patients, reflecting their potential to strengthen the patient-physician relationship in the aftermath of adverse events. 36
Limitations
While this study provides valuable insight into the recent medical malpractice landscape for spine surgery, it has certain limitations to consider. First, the LexisNexis legal database, although extensive, does not include all recent litigation cases related to spine surgery, which may skew the present findings. Specifically, the LexisNexis legal database only includes publicly available, litigated cases from U.S. trial and appellate courts. As such, it excludes most malpractice claims that are settled privately, dismissed pretrial, or resolved through arbitration. Therefore, despite its meaningful utility in prior spine surgery malpractice literature on more historic cases,8,10,15 the total number of cases identified in this study represents only a subset of all malpractice activity and underestimates the true volume of litigation involving spine surgeons. Second, this analysis reflects trends solely within the United States, and findings may not be generalizable to countries where medico-legal systems, healthcare structures, and litigation patterns may differ significantly. Third, some cases were excluded from the study due to incomplete information in the LexisNexis database, resulting in lack of extensive data on demographics, settlement amounts, clinical settings, and cases settled privately outside the court. This reduction in case counts may decrease the statistical power of our study. Fourth, the involvement of both non-testifying and testifying expert witnesses may have influenced trial outcomes. However, data on medical experts was not collected, as available information on testifying experts was non-comprehensive, and non-testifying individuals are protected from disclosure by attorney-client privilege. 37 These limitations, coupled with the small sample size of this study, may ultimately constrain the generalizability of our findings within the broader scope of spine malpractice. Nevertheless, this study is successful in providing updated insight into spine surgery malpractice trends in the United States from 2020 to 2024.
Conclusions
In this legal case series review of publicly available malpractice claims from 2020 to 2024, we identified a concentration of cases in the Southern and Midwestern U.S., with lumbar fusion procedures most involved. The most frequent allegations were related to postoperative pain and issues with informed consent. While these observations reflect only a limited number of public legal cases, they may offer preliminary insight into recurring themes in malpractice litigation. These findings underscore the need for improved documentation, communication, and consent practices in spine surgery.
Footnotes
Consent for Publication
There are no copyrighted material, images, or figures in the present manuscript. All authors consent to publication and grant the journal reproducibility rights upon acceptance.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Samuel K. Cho, MD: AAOS: Board or committee member, American Orthopaedic Association: Board or committee member, AOSpine North America: Board or committee member, Cervical Spine Research Society: Board or committee member, Globus Medical: IP royalties and Fellowship support, North American Spine Society: Board or committee member, Scoliosis Research Society: Board or committee member, Stryker: Paid consultant. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.