
Abstract
Study Design:
Systematic review and meta-analysis.
Objective:
To compare clinical outcomes of all available adjacent segment disease (ASD) cohorts being treated by either anterior cervical discectomy and fusion (ACDF) or total disc replacement (TDR).
Methods:
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews. Searches of electronic databases from inception to August 2017 identified 349 articles for screening. Data was extracted and analyzed using meta-analysis of proportions.
Results:
The search identified 1 double-armed study and 8 single-armed studies from which data of 5 TDR and 5 ACDF cohorts treating ASD were extracted. Between the 2 pooled TDR (n = 103) and ACDF (n = 258) groups, baseline characteristics were predominantly similar. Compared with ACDF, TDR demonstrated superior operation duration (107 vs 188 minutes, P = .011) and range of motion of C2-C7 at final follow-up at least 1 year after surgery (40.2° vs 35.1°, P = .001). Other surgical and performance parameters including estimated blood loss, complications, and Japanese Orthopedic Association score, Neck Disability Index, Visual Analog Scale neck, and Visual Analog Scale upper limb measures were comparable between cohorts.
Conclusion:
TDR confers similar surgical and postoperative outcomes to the treatment of ASD as ACDF. Both procedures lead to improvement in all performance outcomes. Larger, prospective, randomized studies will validate the findings of this meta-analysis. Longer term studies are required to ascertain the recurrence rates of ASD following either surgical treatment of primary ASD.
Keywords
Introduction
Adjacent segment pathology (ASP) involves degenerative changes to the adjacent segments of spinal fusion. When ASP presents with clinical symptoms, it is often termed adjacent segment disease (ASD). 1 These symptoms include radiculopathy, myelopathy, motor weakness, and sensory deficits. 2 The incidence of ASD following anterior cervical discectomy and fusion (ACDF) was extensively studied by Hilibrand et al 3 over a period of 10 years after surgery. They observed that ASD occurred at a relatively constant incidence of 2.9% per year. The consequence of this is that after 10 years, up to one third of fusion patients will present with symptomatic degenerative segments adjacent to the initial site of fusion.
Treatment of ASD requires a decompression component, and this has traditionally been achieved with fusion by ACDF. 1 ACDF has been viewed as a long-standing and effective intervention in managing degenerative changes within the cervical spine. However, the concern here is that while the fusion itself stabilizes spinal segments at risk due to the degeneration, it also alters the biomechanical natural distribution of forces, increasing the stress on adjacent segments. 4 Contributors to this include increased shear strains, higher intradiscal pressures, and increased adjacent segment motion. 5 Theoretically, while the exact pathology of ASD is unclear, ACDF treatment of ASD may contribute to further degenerative changes more adjacent segment in the future. 6
Total disc replacement (TDR) is an effective alternative procedure for the treatment of ASD. 1 The primary biomechanical advantage of TDR is that it is able to better preserve motion at the symptomatic levels adjacent to the initial surgery. 5 This theoretically retains a more natural distribution of forces across the cervical spine, which would then be less likely to further degenerate. Clinically, these principles implicate greater joint function preservation, and reduction in adjacent joint degeneration, making it an attractive alternative to the management of ASD. To date, there is limited evidence in the literature regarding the clinical outcomes of ASD treated by either ACDF or TDR. The aim of this meta-analysis was to pool all relevant data, and then assess and compare surgical and performance outcomes following both procedures to treat ASD. Comparable outcomes would favor larger, human studies of TDR in ASD management.
Methods
Search strategy
The strategy was designed around the PICO question format: Do patients with ASD in the cervical spine (Population) from a prior ACDF surgically treated by TDR (Intervention) compared to those treated by ACDF (Comparator) differ in clinical and radiographic outcomes (Outcome)? The present review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and recommendations. 7,8 Electronic searches were performed using Ovid Embase, PubMed, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, American College of Physicians Journal Club, and Database of Abstracts of Review of Effectiveness from their dates of inception to August 2017. The literature involving all comparative studies were searched by using the following MeSH terms in all logical permutations: “adjacent segment disease/ASD,” “anterior,” “fusion,” “disc replacement,” and “surgery.” The reference lists of all retrieved articles were reviewed independently by 2 investigators (VML and KP) for further identification of potentially relevant studies. All identified articles were then systematically assessed against the inclusion and exclusion criteria.
Selection Criteria
The inclusion criteria used were (1) confirmed clinical diagnosis of ASD in the cervical spine with a history of ACDF surgery, (2) treated with curative intent either by ACDF or TDR, (3) in patients over the age of 18 years, and (4) with at least either pain or functional parameter reported: pain via the Visual Analog Scale (VAS) and function via the Neck Disability Index (NDI). ASD was defined by a minimum of 6 months of new clinical symptoms, including radiculopathy and myelopathy, since the index surgery with confirmatory radiologic evidence of new degenerative changes to the adjacent segments on magnetic resonance imaging. The exclusion criteria applied to all identified articles were (1) other surgical treatments of ASD, including non-anterior approaches, and (2) cohorts where the ASD cohort is indiscernible. When institutions published duplicate studies with accumulating numbers of patients or increased lengths of follow-up, and when studies reported multiple time courses of the same treated cohort, only the most complete reports were included for quantitative assessment at each time interval. All publications were limited to those involving human subjects and in the English language. Abstracts, case reports, conference presentations, editorials, and expert opinions were excluded. Review articles were omitted because of potential publication bias and duplication of results.
Data Extraction and Critical Appraisal
All data was extracted from article texts, tables, and figures with any estimates made based on the presented data and figures. This includes variance estimations based on established statistical methodologies when appropriate. 9,10 Variables collected included patient demographics; perioperative outcomes including operative parameters such as blood loss, operation duration, and complications; as well as pain and functional measures such as VAS of the neck and upper limb, NDI, and range of motion (ROM). Two investigators (VML and KP) independently reviewed each included article with any discrepancy resolved by discussion to reach consensus. All attempts were made to contact study authors for any clarification of data if needed. Articles were then assessed for their respective level of evidence as per the Oxford Centre for Evidence-Based Medicine Levels of Evidence criteria, with a minimum level of 4 required for inclusion in this meta-analysis due to the rare nature of the interventions in question. 11 Because quality scoring is controversial in meta-analyses of observational studies, each article included in our analysis was appraised according to the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) criteria. 12
Meta-Analysis
The pooled mean values were compared for the available main perioperative and postoperative outcomes by meta-analysis of proportions, with random-effects meta-regression based on surgical technique. Each outcome was presented as a forest plot; the weighted mean value, the 95% confidence interval (CI), and the relative weightings were represented by the middle of the square, the horizontal line, and the relative size of the square, respectively. Chi-square tests were used to study heterogeneity between trials. I2 statistic was used to estimate the percentage of total variation across studies, owing to heterogeneity rather than chance, with values greater than 50% considered as substantial heterogeneity. I2 can be calculated as follows: I2 = 100% × (Q − df)/Q, with Q defined as Cochrane’s heterogeneity statistics and df defined as degree of freedom. All P values were 2-sided. All analyses were performed using the metafor package for R version 3.3.
Results
Search Strategy
A total of 349 references were identified through 6 electronic database searches. Manual search of reference lists yielded 2 additional studies. After exclusion of duplicate or irrelevant references, 287 potentially relevant articles remained for assessment (Figure 1). After applying the selection criteria, 1 two-armed study 13 and 8 single-arm studies 2,5,14 -19 were selected for analysis, yielding 5 cohorts evaluating ACDF and 5 evaluating TDR. The 2-armed study was assessed to be of Level 2b evidence, and the single-arm studies were assessed to be of Level 4 evidence. Their characteristics are summarized in Table 1.
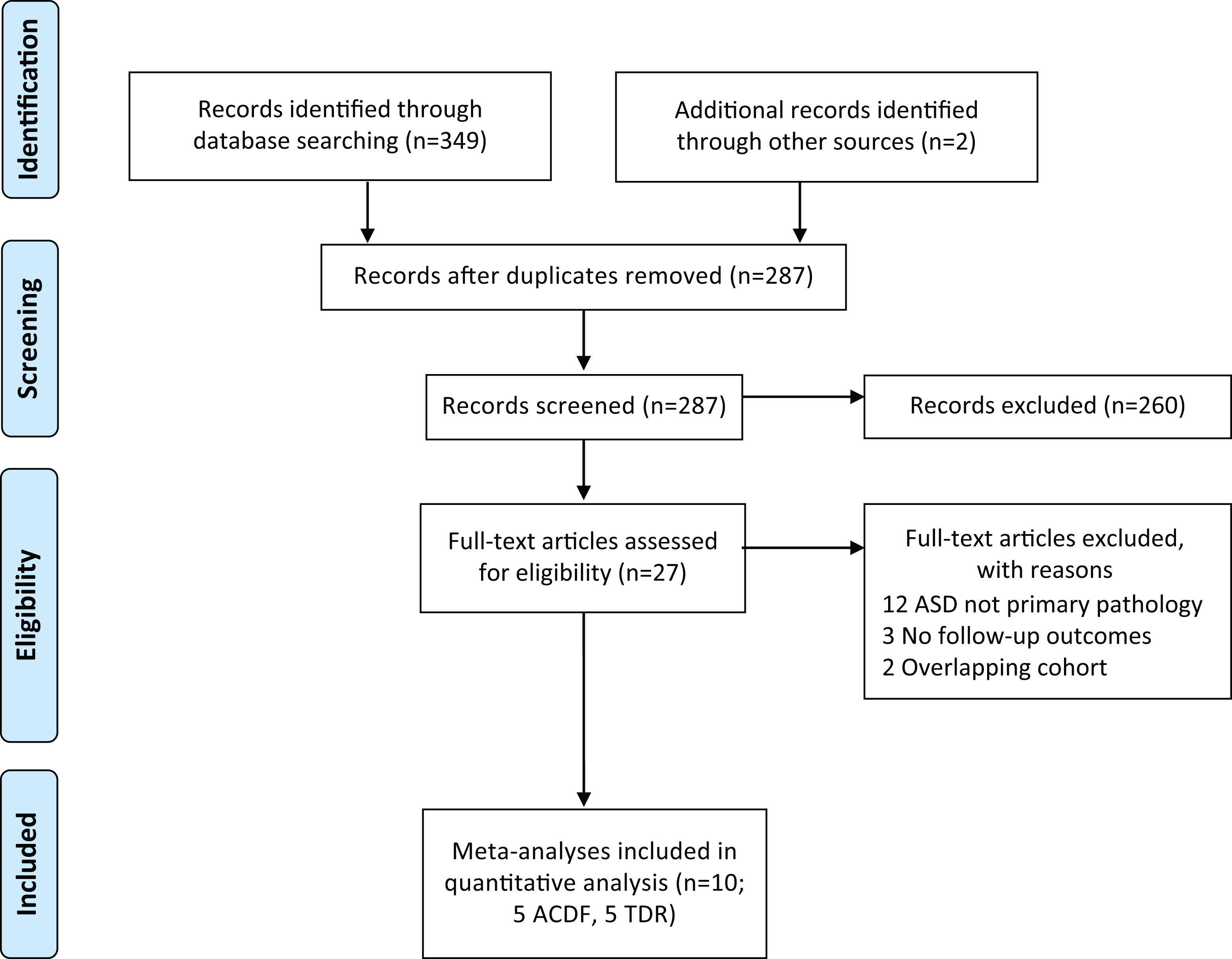
Flow diagram of search strategy results conducted per PRISMA guidelines.
Study Characteristics and Demographics of Included Studies.
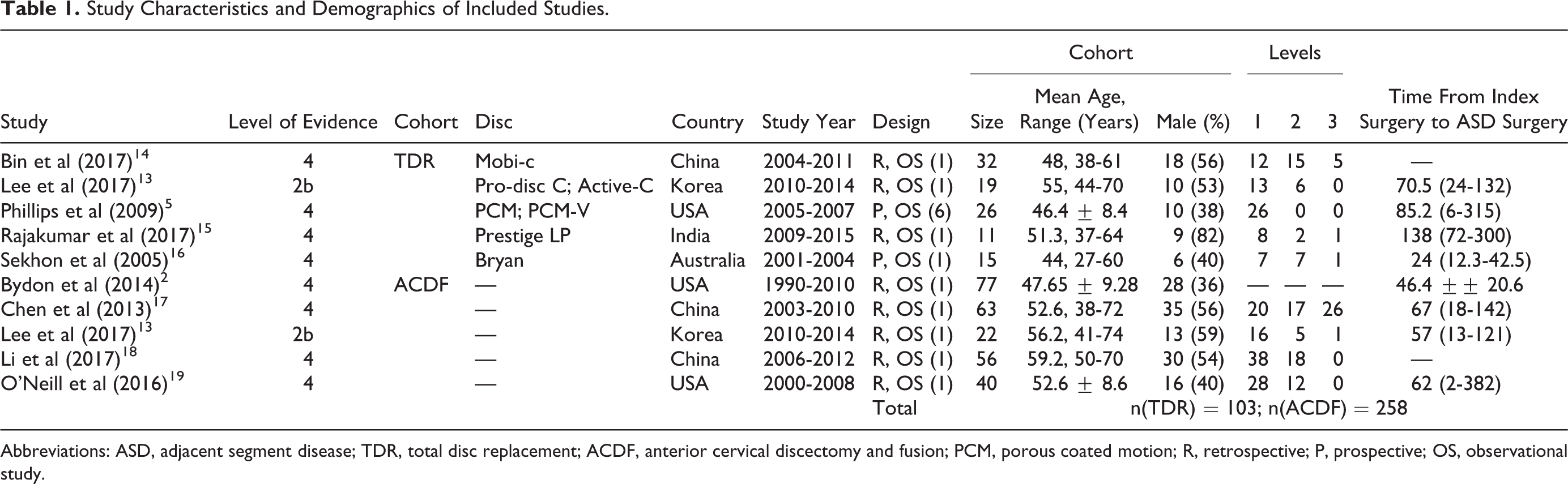
Abbreviations: ASD, adjacent segment disease; TDR, total disc replacement; ACDF, anterior cervical discectomy and fusion; PCM, porous coated motion; R, retrospective; P, prospective; OS, observational study.
Baseline Characteristics
Overall, 103 and 258 ASD cases managed by TDR and ACDF, respectively, were reviewed. There were no significant differences between the cohorts for ASD based on age (49 vs 53.65 years, P = .06) and proportion of males (51% vs 48%, P = .66). Preoperative functional scores were also similar between TDR and ACDF groups in terms of NDI (41.9 vs 43.5, P = .87), Japanese Orthopaedic Association (JOA0 score (9.8 vs 9.7, P = .84), and VAS neck (6.95 vs 6.42, P = .24). However, VAS upper limb was significantly higher for the TDR group (7.1 vs 6.9, P = .02). Preoperative C2-C7 ROM was similar between TDR and ACDF cohorts (38.8 vs 40.2, P = .086). These are summarized in Table 2 and Supplemental Figures (all supplemental figures are available in the online version of the article).
Summary of All Pooled Parameters in Both TDR and ACDF Cohorts.
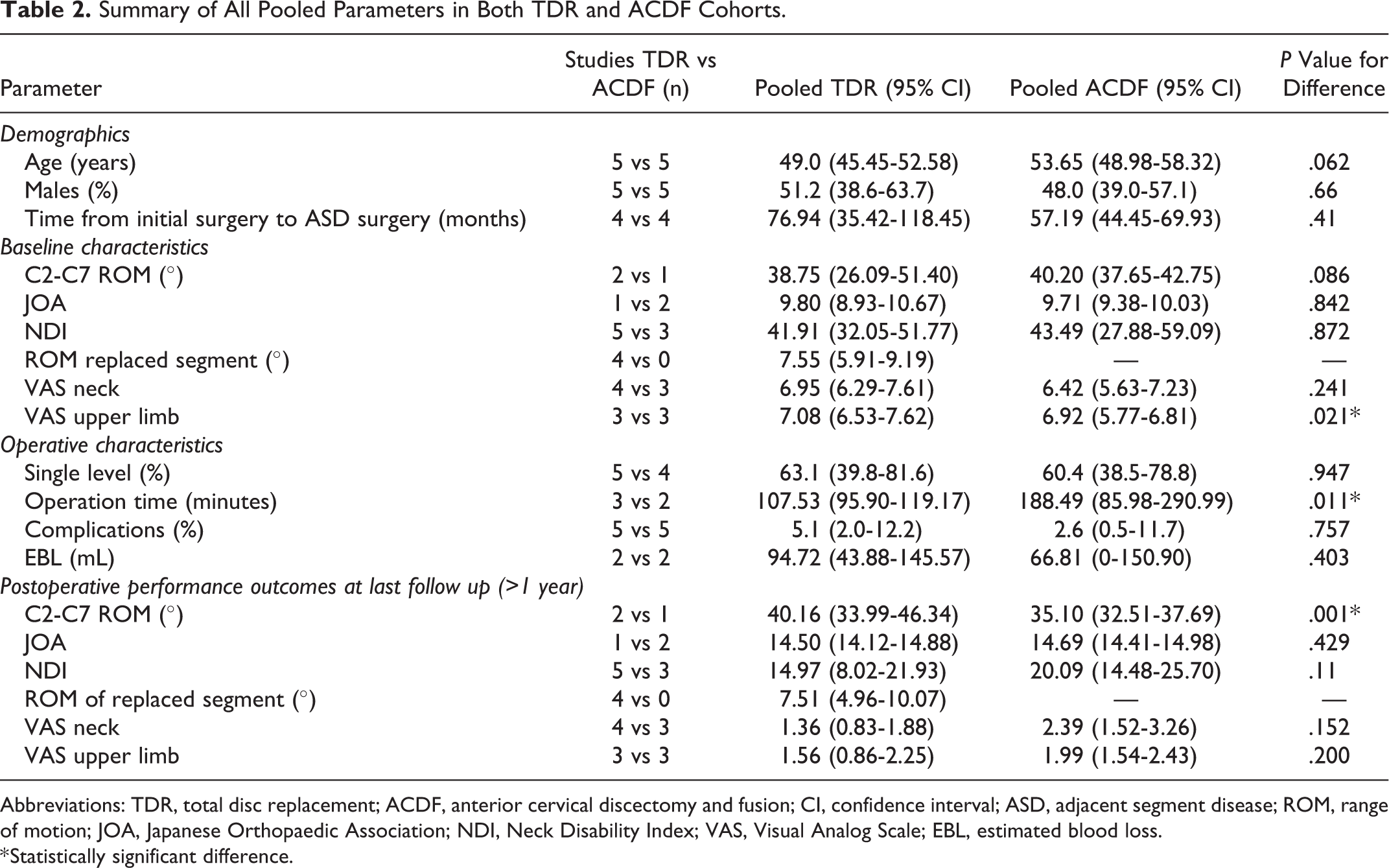
Abbreviations: TDR, total disc replacement; ACDF, anterior cervical discectomy and fusion; CI, confidence interval; ASD, adjacent segment disease; ROM, range of motion; JOA, Japanese Orthopaedic Association; NDI, Neck Disability Index; VAS, Visual Analog Scale; EBL, estimated blood loss.
* Statistically significant difference.
Operative Characteristics
The proportion of patients with single-level procedures was similar across TDR and ACDF cohorts (63% vs 60.4%, P = .95). Operative duration was significantly shorter for the TDR group (107 vs 188 minutes, P = .011; Figure 2A); however, estimated blood loss was similar (95 vs 67 mL, P = .40; Figure 2B). Complication rates was not significant different (5.1 vs 2.6%, P = .76; Figure 2C). These are summarized in Table 2.
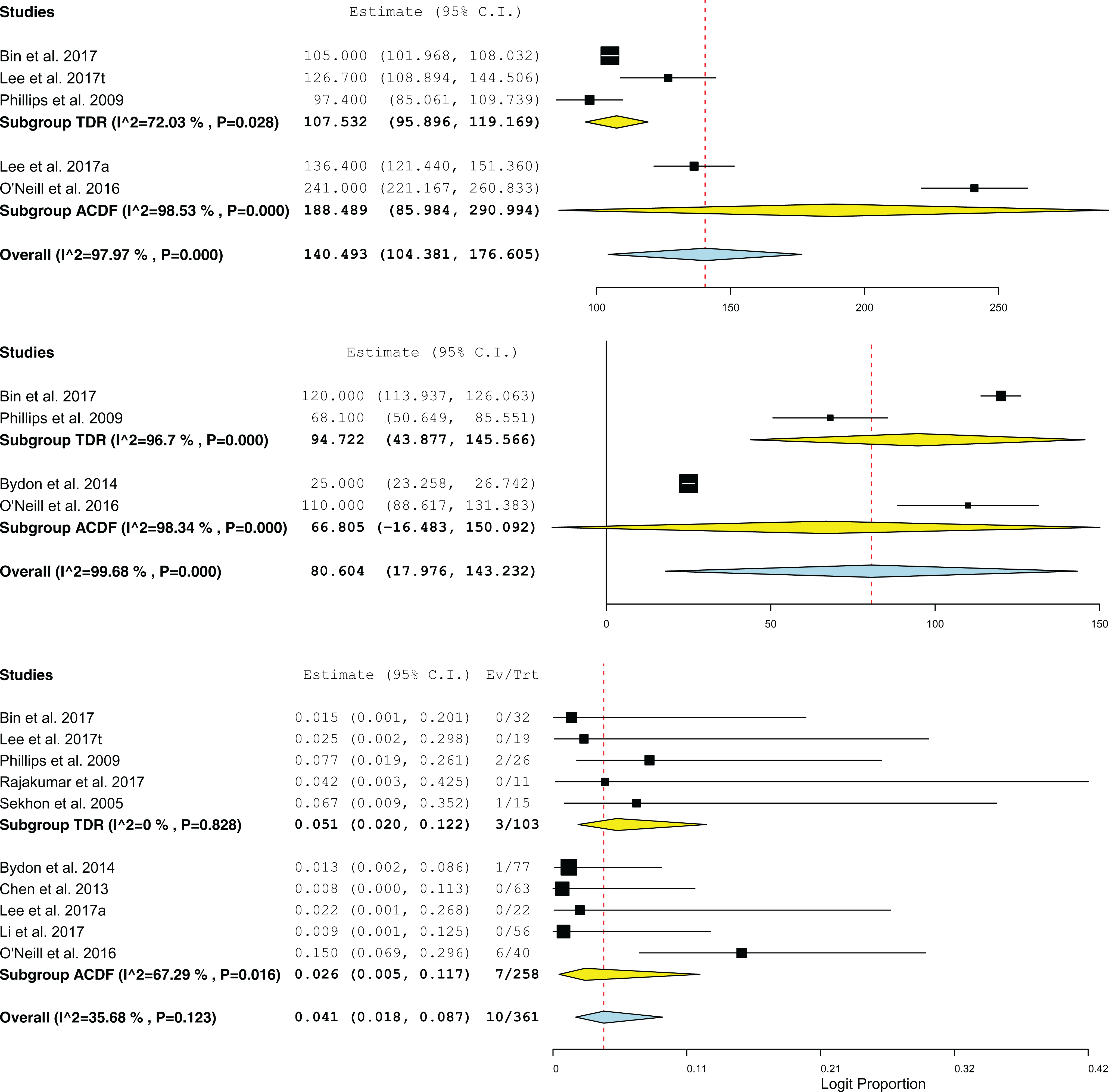
Forest plots comparing operative characteristics (A) operation duration (minutes); (B) estimated blood loss (mL); and (C) complication incidence.
Postoperative Performance Outcomes
At minimum 1-year follow-up, follow-up ROM of C2-C7 was significantly higher for TDR group compared to ACDF (40.2° vs 35.1°, P = .001; Figure 3). Otherwise, there was no significant differences noted between TDR and ACDF groups in terms of VAS neck, VAS upper limb, NDI, or JOA scores. These are summarized in Table 2 and Supplemental Figures.
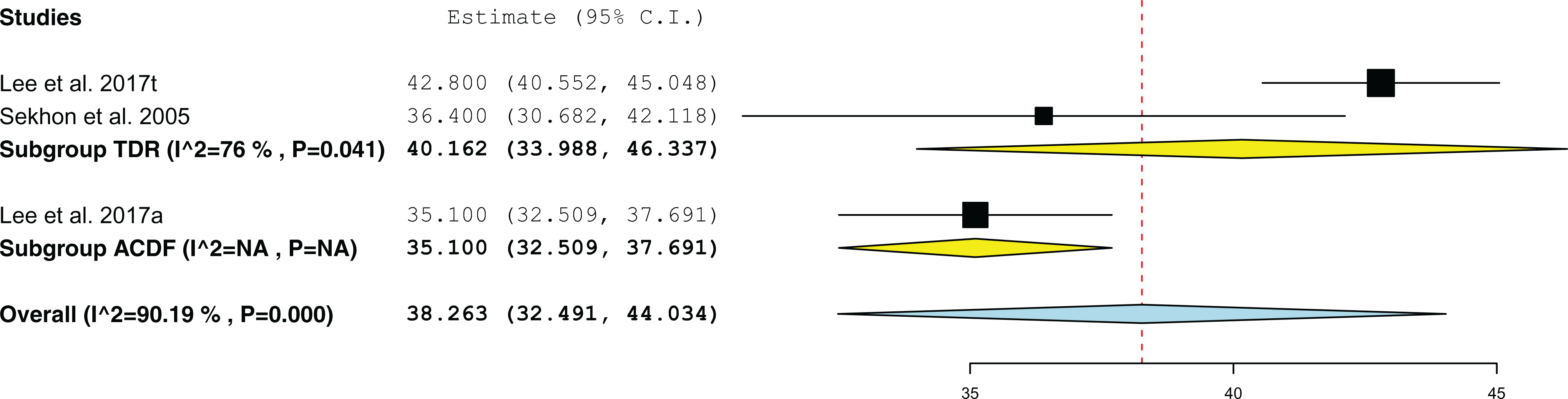
Forest plot comparing postoperative performance outcome range of motion (ROM) of C2-C7 (°).
Assessment of Risk of Bias
The assessment of bias risk by the MOOSE criteria of each included study is presented in Table 3, with no obvious overall bias risk implicated for any included study.
Results of MOOSE Assessment for Quality of Evidence for All Included Studies.
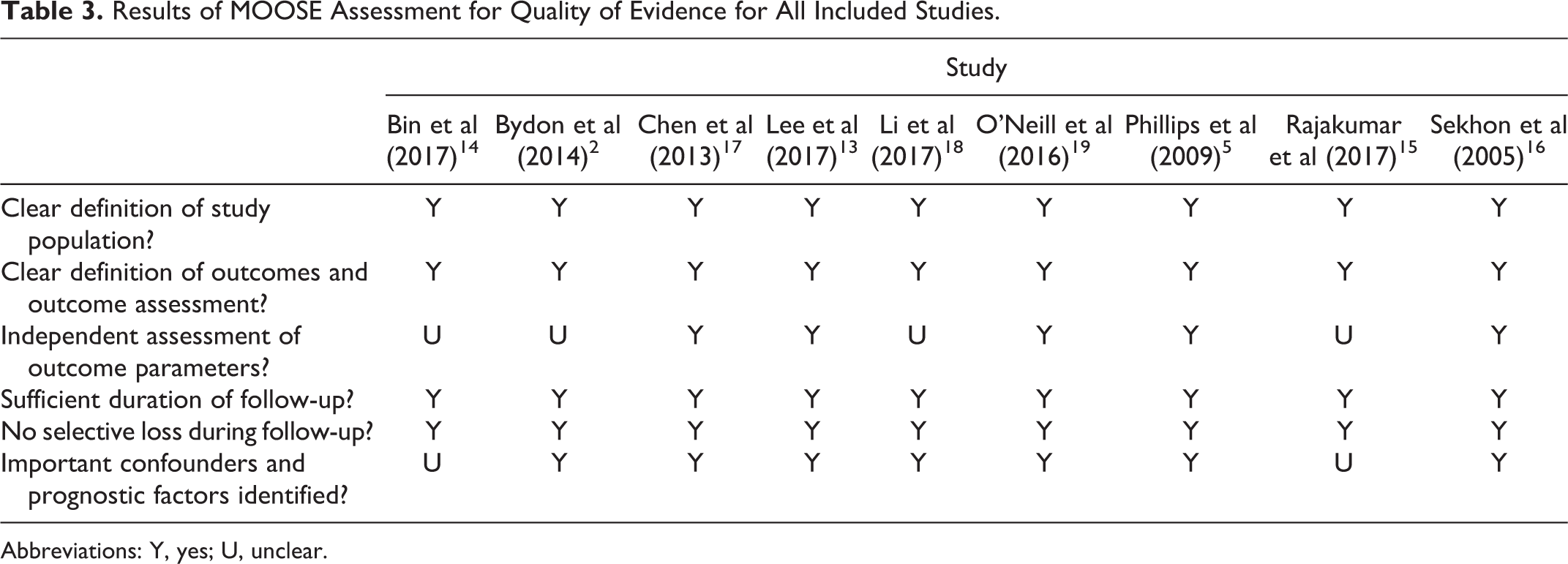
Abbreviations: Y, yes; U, unclear.
Discussion
This meta-analysis describes the clinical outcomes of patients with symptomatic ASD secondary to prior surgery treated by either ACDF or TDR. Pooled estimates from published studies to date suggest that there is no significant difference between the 2 procedures with respect to blood loss, complication rates, and performance outcomes. However, TDR appeared to confer significantly superior ROM of C2-C7 (P = .001), as well as lower operative durations (P = .011), when compared to ACDF. The merits of both procedures require further longer term comparative investigation in order to continue to develop the decision algorithm between them.
Lee et al 13 report the only direct comparative study published to date of ASD patients with ACDF history, with an ACDF cohort of 22 and a TDR cohort of 19. Their findings were complemented in our meta-analysis by the pooling of other single-armed studies. Overall, they found in their study that when compared to ACDF, TDR had statistically comparable estimated blood loss, improvements in VAS upper limb, nil complications, and superior cervical ROM. These trends mirror those observed overall in this meta-analysis. Interestingly, however, they also observed statistically superior improvement in NDI following TDR at last follow-up compared to ACDF, as well as comparable operation durations. While the statistical significance of these observations was lost in our meta-analysis, their directions of trend were still upheld. These differences are likely to be a result of the greater cohort sizes achieved via pooling of the single-armed studies.
The primary indication for the surgical treatment of ASD is symptomatic relief. With respect to the cervical spine, Bydon et al 2 observed in their series of 108 ASD cases, secondary to prior fusion, that the most common symptom was neck pain (97%), followed by cervical radiculopathy (71%) and sensory deficits in the cervical distribution (57%). The functional measures of VAS neck, VAS upper limb, and NDI are thus important measures to consider when conducting postoperative evaluation. In favor of both ACDF and TDR is that they both have been seen to provide exponential improvement in VAS and NDI immediately after surgery, with improvements continuing to progress, albeit at a slower rate, well beyond 1 year. 13 Considering that the complication rates between the 2 procedures are similar, neither ACDF nor TDR seems to possess any serious concerns in not satisfying their primary indication.
One significant finding of our meta-analysis was that following TDR, the ROM of C2-C7 at final follow-up was significantly greater to that of ACDF. This is important to consider as a smaller cervical ROM has been linked with worse general health status in patients with cervical pathology. 20 However, this finding requires further investigation for only 2 TDR 13,16 and 1 ACDF 13 cohorts were able to be pooled. Within the cohorts, it is noted that only in the ACDF cohort was the final postoperative ROM significantly lower than that of the preoperative measurement (35.1° vs 40.2°, P = .049). In both TDR cohorts, the final cervical ROMs were statistically comparable to that of the preoperative ranges. This may be an important consideration for ASD patients as it has been suggested that the maintenance of cervical ROM is associated with greater neurological improvement, as well as reduced degeneration of newly adjacent segments. 21,22
What remains an interesting avenue for future investigation is the incidence of recurrent ASD following treatment of primary ASD. Compared to ACDF, TDR may offer superior recurrent ASD control, because it has the potential to provide greater restoration of normal spinal biomechanics, which protects against degeneration in adjacent segments. 15,23 Unfortunately, long-term data comparing ACDF against TDR with respect to recurrent ASD is limited. In the only direct comparative study, Lee et al observed significantly less incidences of radiologic ASP following TDR (2/19, 11%) compared to ACDF (8/22, 36%, P = .04) after treatment of primary ASD. In the largest single-arm ASD studies available, Bin et al 14 and Xu et al 24 observed 3/32 (9%) and 27/108 (25%) cases of suggestive recurrent ASD following TDR and ACDF treatment. If one procedure can be comprehensively shown to afford greater degenerative control in ASD, then this will assist clinicians in deciding optimal management in the future.
In order to validate the decision between ACDF and TDR to manage ASD, practical operative features of each approach may prove influential. This meta-analysis found that only operative duration (P = .011) was significantly different between the 2 approaches, with TDR being shorter in time, while estimated blood loss (P = .40) and complications rates (P = .76) were not. Whether or not operative duration alone is sufficient to advocate for TDR over ACDF remains to be seen. In the case of ACDF and TDR as original surgeries, there appears to be no difference in operative duration, meaning that the value of this metric has yet to be fully explored when there is a difference, as is the case for repeat surgery to manage ASD. 25
It is worth noting that with respect to functional outcomes, this meta-analysis found both procedures to be largely comparable, with the exception of follow-up ROM of C2-C7. Thus, in anticipating the development of a decision algorithm between these 2 approaches, consideration should appreciate that ASD patients should not be considered as naïve patients. This is because patients presenting for ASD from previous ACDF will be older, have established degeneration already by definition, and have previous surgical disruption to surrounding soft tissue, which are all proven risk factors for ASD itself. 26 -28 Thus, perhaps the significant differentiator between ACDF and TDR to manage ASD is the long-term success of each procedure in preventing further ASD. Only time will tell if such a superiority exists, as currently the literature is too young to evaluate this, and this will undoubtedly assist clinicians in determining the optimal approach for a patient.
Strengths and Limitations
This meta-analysis adhered strictly to the PRISMA guidelines in its search, and searched for all double- and single-arm studies to pool in order to answer this PICO question with limited studies published to date. The definitions of ASD secondary to prior surgery as the primary surgical indication and fusion by anterior approach only were strictly enforced. Furthermore, potential source of publication bias in overlapping cohorts were accounted for.
However, a number of limitations exist. This meta-analysis involved the pooling of multiple Level 4 single-arm studies reporting outcomes for either ACDF or TDR, with Lee et al 13 being the only double-arm study in the literature to date reporting outcomes for both interventions. Unfortunately, indirect comparisons introduce an additional degree of uncertainty to the comparability of the 2 cohort groups. To address this, we analyzed the baseline characteristics, including demographics and preoperative functional measures in order to assess the homogeneity of pooling all included studies. It is promising to note that no demographic features between the TDR and ACDF groups were significantly different, and only one preoperative functional measure was significantly different. This was preoperative VAS upper limb, where TDR and ACDF were 7.1 versus 6.9 (P = .02). Given upper limb symptoms are not as common as cervical symptoms in presenting cases of ASD, and the fact that both procedures demonstrate significant improvement in VAS upper limb after surgery to statistically similar levels, we believe this aspect remains comparable. However, it is clear that further data is necessary to validate both this trend and significance.
Another consideration is the multitude of clinical variables that can vary between ASD cases. This includes the number of levels being treated, an anterior or posterior approach, and presence of myelopathy, among others. Given this introduces methodological heterogeneity in the meta-analysis, we attempted to minimize this bias by utilizing RE modelling. Interestingly, Xu et al 24 found that none of those aforementioned features affected the recurrence rate of ASD following ACDF treated primary ASD.
Finally, typical study limitations such as limited follow-up, small cohort size, retrospective nature, and lack of randomization weaken the findings of this meta-analysis. Limited follow-up affects our ability to interpret control for ASD recurrence, as well as functional outcomes. Given Hilibrand et al 3 demonstrated the risk of ASD continues for decades after index fusion surgery, we cannot discount recurrent ASD and longer term follow-up will clarify how TDR versus ACDF provide control for this. The small cohort size and retrospective nature cannot account for the risk for selection bias in reported patient outcomes, which may have skewed the comparative results. Randomization will overcome this by minimizing this risk. Thus, future studies that involve longer term follow-up, larger cohorts, and are conducted in a prospective, randomized controlled manner are required to validate and enhance the findings of this meta-analysis.
Conclusion
Overall, ASD secondary to prior ACDF that typically presents with neck pain and disability are effectively alleviated in the short term by both TDR and ACDF procedures. TDR appears to be statistically noninferior to ACDF with respect to most surgical and performance outcomes. The only significant differences are superior operation durations and ROM of C2-C7. Longer term study is required to evaluate the recurrence of ASD following either procedure, in order to ascertain true clinical relevance. This will be best executed in larger, prospective, and randomized studies.
Supplemental Material
GSJ_Supplementary - Clinical Outcomes of Treating Cervical Adjacent Segment Disease by Anterior Cervical Discectomy and Fusion Versus Total Disc Replacement: A Systematic Review and Meta-Analysis
GSJ_Supplementary for Clinical Outcomes of Treating Cervical Adjacent Segment Disease by Anterior Cervical Discectomy and Fusion Versus Total Disc Replacement: A Systematic Review and Meta-Analysis by Victor M. Lu, Ralph J. Mobbs and Kevin Phan in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.