
Abstract
Study Design:
Narrative review.
Objective:
The aim of this narrative review is to examine trends in malpractice litigation arising from spine surgery. We also hope to detail mitigation strategies that surgeons can employ to decrease their risk of a claim.
Methods:
A review of the relevant literature examining the prevalence, risks, and outcomes of malpractice litigation following spine surgery was conducted using the MEDLINE and Embase databases.
Results:
Combined queries identified 1140 potentially relevant articles. After eliminating duplicate articles and screening by title and abstract, 38 articles underwent full-text review. Of these, 22 were deemed relevant to the research questions posed. Evaluation of references identified 1 additional relevant article. Spine surgery represents one of the most litigious specialties in the United States health care system. The available literature points to a consistent pattern of common allegations leading to litigation following spine surgery. While a majority of filed lawsuits end in the surgeon’s favor, these cases carry high monetary and time expenditures regardless of outcome. Furthermore, the threat of a malpractice lawsuit motivates many surgeons to practice defensive medicine by utilizing unnecessary or unindicated tests and studies.
Conclusion:
Through the examination of trends in malpractice claims and case outcomes, surgeons may be able to adapt practices to minimize their risk of litigation. These changes can include, but are not limited to, identification of those procedures that are most litigious and a more thorough discussion of the informed consent process to include operative and nonoperative treatments prior to all procedures. More important, however, spine surgeons can potentially serve as advocates for change.
Introduction
With an estimated cost of $55.6 billion dollars annually, the medical malpractice system accounts for approximately 2.4% of health care spending in the United States. 1 (For the purposes of this article, the term claims consists of allegations of medical malpractice following spine surgery. The term lawsuit represents all claims filed within the legal system. The term malpractice system represents all claims filed or unfiled.) Within the current medicolegal system, spine surgery represents one of the most litigious medical subspecialties. 2,3 This is despite data showing that there are fewer postoperative adverse events in spine surgery compared to other commonly performed orthopedic procedures such as total joint arthroplasty and procedures addressing hip fracture. 4 In response, a growing body of spine literature attempts to quantify the incidence and costs of litigation as well as its most common causes. 3,5 -11 In this comprehensive narrative review, we detail the current incidence, common case characteristics, and economic burden of medical litigation in spine surgeries occurring within the US health care system. Further through examination of available literature, we hope to define reasonable strategies that the practicing spine surgeon can employ to reduce the risk of claims and subsequent litigation. Gaining improved understanding of this complex system may help physicians better navigate it and advocate for needed reforms.
Methods
Specific questions posed in this review included the following: What is the incidence of malpractice litigation after spine surgeries performed in the United States? Does spinal region, geography, or urgency status effect litigation rates? What are the most common allegations specified in suits filed after spine surgery? What are the outcomes of cases filed after spine surgery in the United States? What are the direct and indirect costs of the malpractice system in spine surgery? Is the current legal system equitable to both surgeons and patients? Does existing literature suggest reasonable steps spine surgeons can employ to minimize individual risk of claims and lawsuits?
To answer these questions, a review of the MEDLINE and Embase databases was performed to evaluate all published literature between September 1, 1989 through August 31, 2019. Terms searched in each database were, “medical litigation or medical malpractice or indemnity and spine surgery” (Figure 1). Two investigators, KJ and JR, independently reviewed all retrieved titles and abstracts for relevance. Studies reporting the incidence, case characteristics, outcomes, or indemnity payments following suits were identified for full text review. Articles focusing on non-US, pediatric, or exclusively nonsurgical populations were excluded. Studies that were purely editorial or had not been subjected to peer review were also excluded. Each reviewer independently performed full text evaluation of all potentially relevant articles to reach an inclusion determination. Duplicate articles were removed at this step. Articles meeting inclusion criteria and answering one of the posed questions were included in this review. Discrepancies on inclusion determination at this point were settled through independent review by the senior investigator (JD). Relevant studies were cross referenced to identify articles that may have not been captured in the initial database queries. Because included studies consisted entirely of surgeon responses to widely disseminated surveys, large closed case series reviews or retrospective cohort analysis, a bias review was deemed unnecessary.
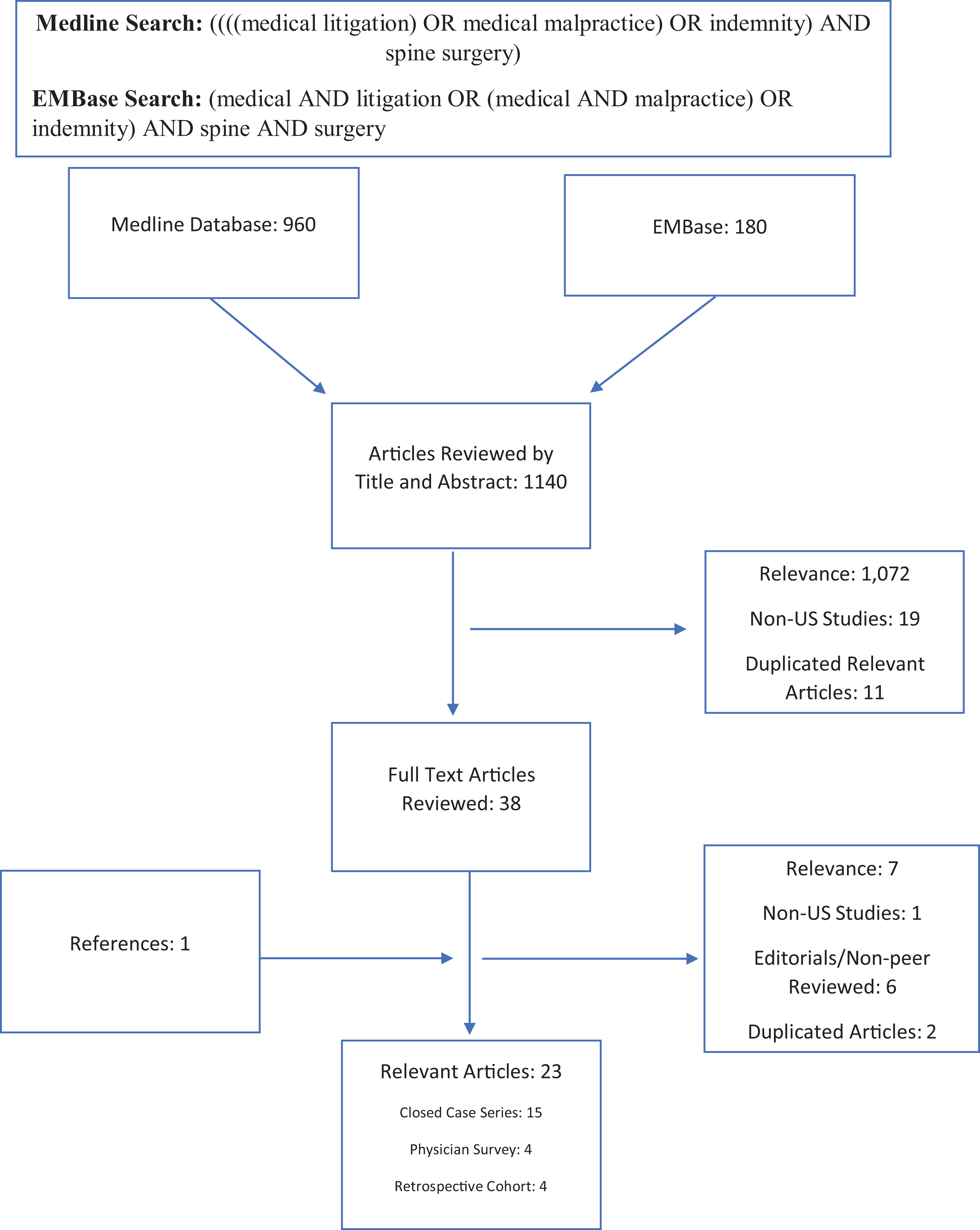
Flow chart of narrative review.
Results
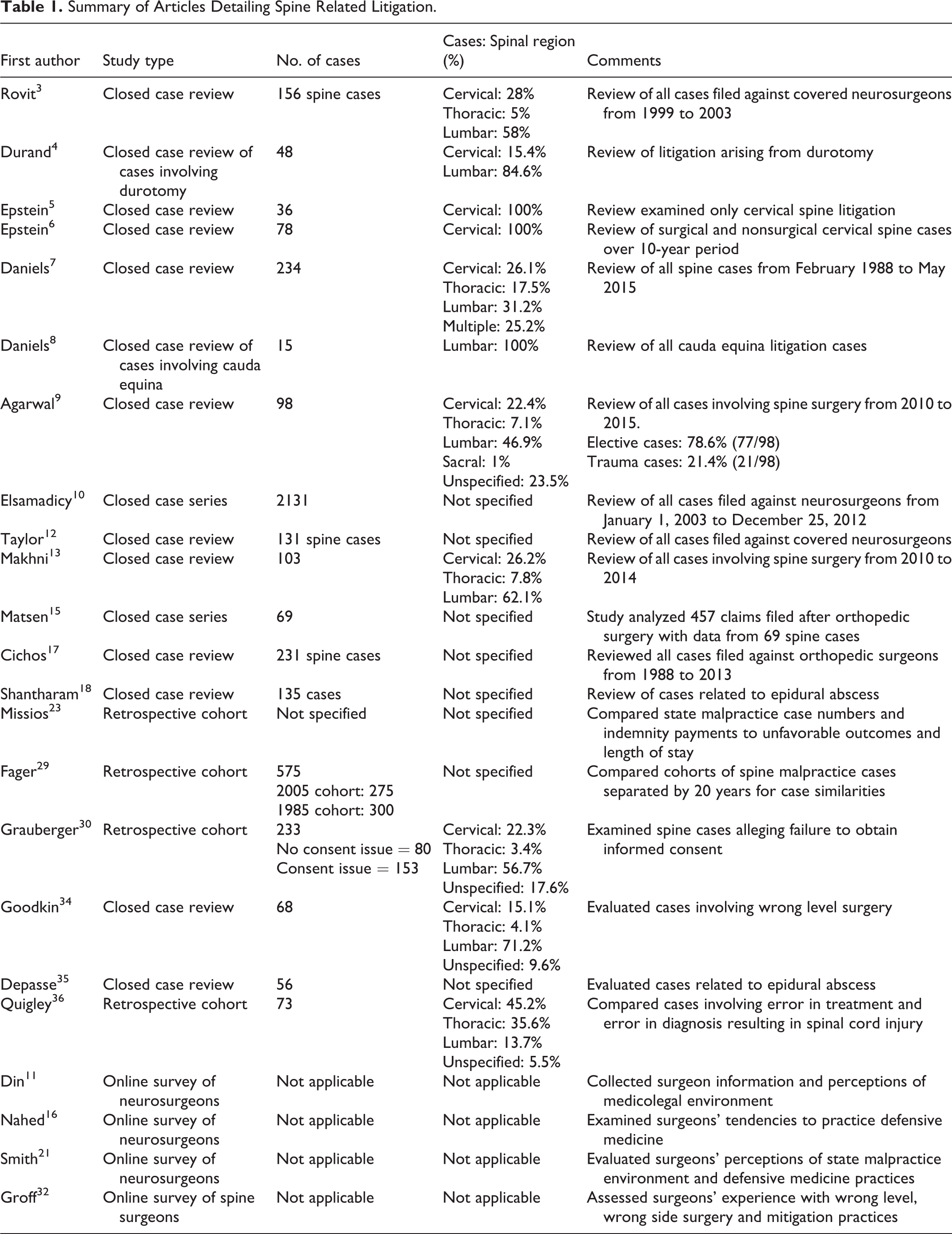
Figure 1 demonstrates the results for each phase of this review. Cumulatively, the database queries identified 1140 articles. Screening by title and abstract for relevance yielded 49 articles for review. Eleven relevant studies appeared in both queries, leaving a total of 38 articles for full text review. Of these, 22 were deemed relevant to the research questions posed after full-text assessment. Cross-referencing each included study yielded an additional article that was deemed germane to the posed questions after full text review. As a result, 23 articles were considered relevant to the questions posed in this study (Table 1).
Summary of Articles Detailing Spine Related Litigation.
Incidence of Malpractice Claims
Most spine surgeons will face one or more malpractice claims within their career. In a review of litigation involving policy holders of a large professional liability insurer, Jena et al 2 reported that 19.1% of neurosurgeons faced medical claims annually. This rate of annual claims was higher than any of the other 24 medical specialties evaluated. 2 In a review of a database maintained by a malpractice carrier in New York, Rovit et al 3 reported that 48.5% (51/105) of neurosurgeons faced 1 claim within a 5-year period and that an additional 23% faced 2 claims. While the breadth of potentially litigious neurosurgical practice extends well beyond the spine, the majority of claims neurosurgeons face stem from elective spine surgery. 3,11 -13 In a retrospective review of the Physician Insurers Association of America Data Sharing Project, Taylor 13 noted that spine cases were significantly more likely to result in claims than cranial surgeries (P < .0001, relative risk [RR] 0.45). Orthopedic spine surgeons face a similar malpractice environment. In separate reviews of medicolegal databases, Agarwal et al 10 (23.8% vs 17.3%) and Daniels et al 8 (58.1% vs 33.8%) noted that orthopedic spine surgeons were named as defendants in a higher percentage of cases than neurosurgeons. These studies highlight the elevated risk of litigation both orthopedic surgeons and neurosurgeons face when performing spine procedures.
Though surgeons represent the most common group named in cases stemming from spine procedures, other subspecialties and numerous governing bodies also face litigation from these cases. 8,10 Agarwal noted that physicians from 8 nonsurgical specialties and various governing entities were named as defendants in litigation following spine surgery. 10 In this review emergency medicine providers (4.8%), radiologists (4.2%), and neurologists (3.6%) represented the most common nonsurgical subspecialties involved in spinal litigation. 10 Spine-related malpractice claims also frequently targeted private practices (19.6%) and hospitals(16.7%). 10 Similarly in their closed case review, Daniels et al 8 noted that hospitals and nonsurgical providers were named in 40.6% and 8% of cases, respectively. The inclusion of nonsurgical providers and institutions, such as hospitals and private practices, reflects a system where surgeons are not the only entities incurring financial risk during litigation. 10
Types of Spine Cases Resulting in Claims
Despite a common perception that surgeons incur higher risks of litigation by performing more complex procedures or caring for traumatic injury, a large majority of malpractice claims result from routine elective procedures. 3,10 By spinal region, cases involving the lumbar spine constitute 45% to 65% of claims, while thoracic and cervical spine cases account for approximately 10% to 20% and 20% to 35%, respectively (Table 1). 8,10,14 Many cases progressing to litigation involve routine rather than complex procedures. In her review of cases following cervical spine surgery, Epstein 6 reported that 42% of suits arose from 1- or 2-level anterior cervical discectomy and fusions. In Agarwal’s cases series, one-third of claims with a specified procedure arose from isolated lumbar decompression. 10 The high percentage of claims filed after relatively straightforward procedures highlights the fact that cases progressing to litigation appear more representative of a typical spine surgeon’s practice than most might expect.
The evidence examining a relationship between trauma cases and an elevated risk of malpractice claims appears conflicting. In a review of three prospectively maintained databases comparing elective, urgent, and emergent cases in a general surgery practice, Stewart noted similar rates of claims filed per procedure performed for each surgical classification. 15 In a review of cases filed against one physician owned malpractice carrier in New York, Rovit et al 3 found that only 5% of spine cases arose from traumatic injuries. However, Agarwal et al 10 noted that claims arising after trauma represented 31.4% of cases in his review. Similarly, Epstein 7 noted that 32% of cases arose from traumatic causes in her review of cervical cases contained within a national databank. Though data on the typical trauma to elective case mix does not exist, trauma cases likely constitute much less than 30% of the national case load. As a result, trauma may be overrepresented in the pool of cases proceeding to litigation in spine surgery. In comparing malpractice claims after elective and emergency procedures, Agarwal et al 10 noted that emergency cases had substantially higher indemnity payments and were significantly more likely to end in a plaintiffs’ verdicts at trial. Future studies should explore the relationship between trauma procedures and litigation in spine care.
Reasons for Litigation
Consistently, the most common plaintiff allegations in spine litigation involve procedural complications, lack of informed consent, and failure to diagnose or treat in a timely manner (Table 2). 6,7,10,14,16 Agarwal et al 10 reported varying trends in allegations between trauma and elective cases. In claims following elective cases procedural error (71.4%), lack of informed consent (29.9%), failure to treat (20.8%), and failure to diagnose (19.5%) represented the 4 most common stated reasons for litigation. For emergent cases, the most common allegations were failure to diagnose (76.2%), failure to treat (76.2%), failure to order diagnostic tests (42.9%), failure to refer (28.6%), and misinterpretation of a test (28.6%). 10 The consistency of these common allegations in spinal litigation may help spine surgeons develop strategies to reduce risk or mitigate its effects in their personal practice. Specifically, making timely and accurate diagnoses, followed by a thorough discussion of the problem and treatment options to include both operative and nonoperative and operative treatment options and the risks and benefits of each can help curb some of the most common reasons for litigation.
Most Frequently Alleged Complaint and Ultimate Outcomes of Spinal Litigation.
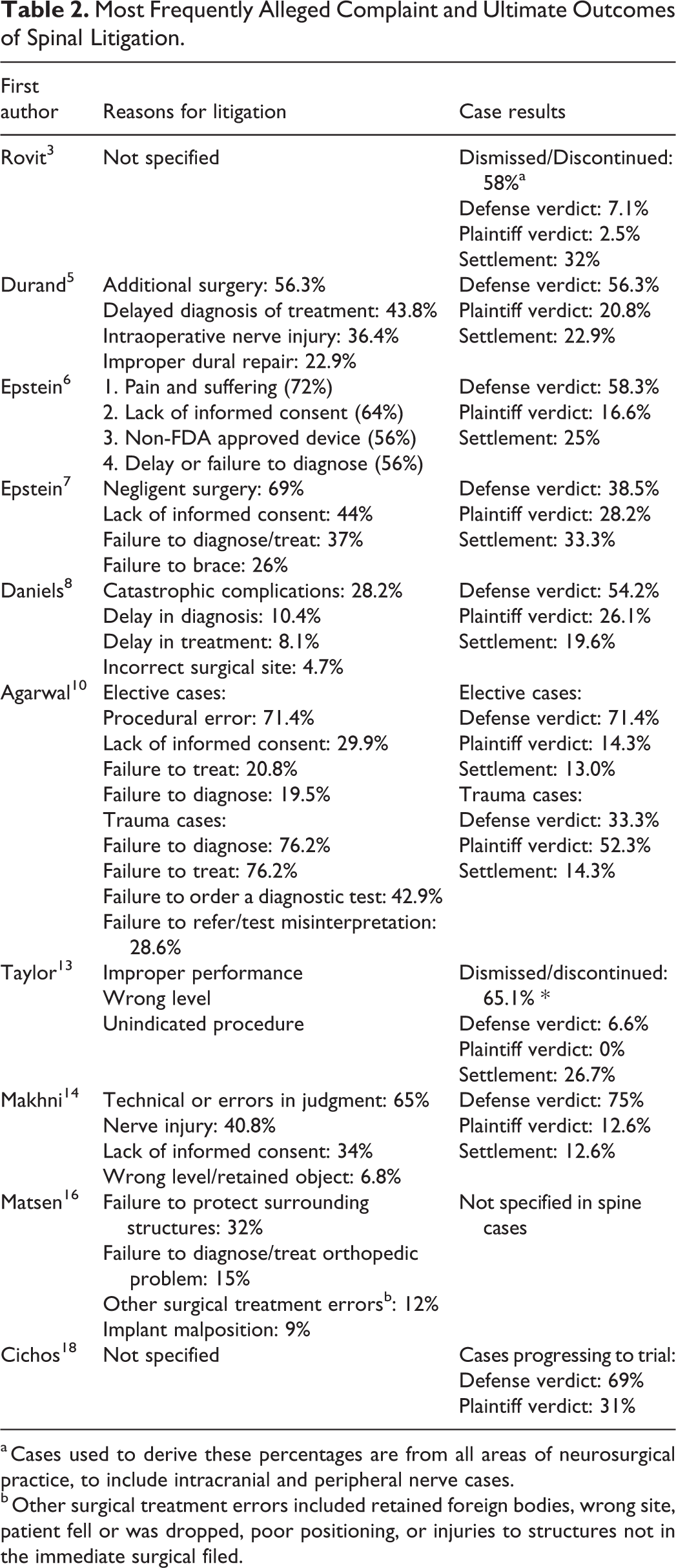
a Cases used to derive these percentages are from all areas of neurosurgical practice, to include intracranial and peripheral nerve cases.
b Other surgical treatment errors included retained foreign bodies, wrong site, patient fell or was dropped, poor positioning, or injuries to structures not in the immediate surgical filed.
Do High Risk States or Regions Exist?
Though physicians perceive geographical practice location as an important contributor to the risk of liability, no existing data in spine surgery definitively validates this relationship. In a national survey of 1028 neurosurgeons, 71.3% of providers reported that potential medical liability claims affect their decision on where to practice geographically. 17 While a majority of claims following spine surgery occur in the most populated states, accounting for differences in population and physician numbers creates a more convoluted picture. In their large closed case review, Daniels et al 8 reported that 67.5% of spine related claims originated in New York (24.4%), California (20.9%), Texas (11.1%), Ohio (5.5%), and Massachusetts (5.5%). However, the authors of this study did not index rates of litigation with population, procedures performed or physicians practicing in the state. In another database review, Agarwal et al 10 reported that the greatest number of cases were filed in California (17.34%), Pennsylvania (14.3%), Florida (10.2%), and Washington (10.2%). When normalized for the number of actively licensed physicians, Idaho, Washington, and Wyoming demonstrated the highest rates of litigation. 10 The varying results of these studies highlight some of the weaknesses in existing literature. Because many studies rely on information voluntarily entered into legal databases by attorneys, cases may be underreported and regional bias toward a particular database may skew specific state statistics. Given these limitations, future investigators should develop better ways to assure more complete collection of case data by state. These strategies may include querying data contained within the National Practitioner Data Bank or collected by individual states’ medical boards and insurance commissioners. This information would aid in assessing the effect of malpractice reform measures that are typically implemented at the state level.
Outcomes of Litigation
Many medical malpractice claims do not end in a trial or settlement. When cases do progress to these stages, most end in a favorable result for the defense. In a review of 10 056 claims filed against physicians from all medical specialties insured under a national malpractice carrier, Jena noted that only 55.2% of claims result in the filing and conduct of a lawsuit. 2 Of these litigated claims, 54.1% were dismissed by the court. 2 Of cases that go to court, 54-75% end favorably for the surgeon/defense (Table 2). 5 -8,10,14,18 Makhni et al 14 noted that 75% of malpractice suits filed between 2010 and 2014 ended in favor of the defendant. In a separate review of cases ending in settlement or a jury verdict, Daniels et al 9 reported that 54.2% of cases ruled in favor of the defense while 26.1% of cases resulted in plaintiffs’ verdicts and 19.6% ended in a settlement. Similarly, in 48 cases litigated cases following durotomy, Durand et al 5 noted that 56.3% resulted in defense verdicts.
While most cases that progress to a jury verdict end favorably for the defense, specific case characteristics can influence results. Agarwal et al 10 noted significant increases in plaintiffs’ verdicts in litigation that cited failure to treat (P = .025), patient death (P = .04), or cases involving emergent surgery (P = .002). Daniels et al 8 identified catastrophic complications, delay in complication diagnosis, and delay in treatment as allegations associated with higher rates of plaintiffs’ decisions. Physicians were significantly more likely to lose cases where catastrophic complications occurred (66.7% vs 37.5%, P < .001) and these case losses carried higher mean awards ($6.1 million vs $2.9 million, P = .04). 8 Cases involving a delay in diagnosis of a complication (42.9% vs 72.7%, P = .007) or delay in treatment (43.7% vs 68.4%, P = .03) also correlated with higher rates of plaintiff remuneration. 8 Similarly in a review of cases related to spinal epidural abscess, Shantharam et al 19 noted significantly higher rates of plaintiffs’ verdicts in cases with associated spinal cord injury and delays in diagnosis or treatment. In a review of 48 litigated durotomy cases, Durand et al 5 noted that delays in diagnosis or treatment resulted in significantly higher rates of plaintiffs’ rulings (61.9% vs 35.1%, P = .0253). In review of their commonalities, these studies point to catastrophic complications and delays in diagnosis or treatment as common allegations that prove difficult to defend against in litigation proceedings.
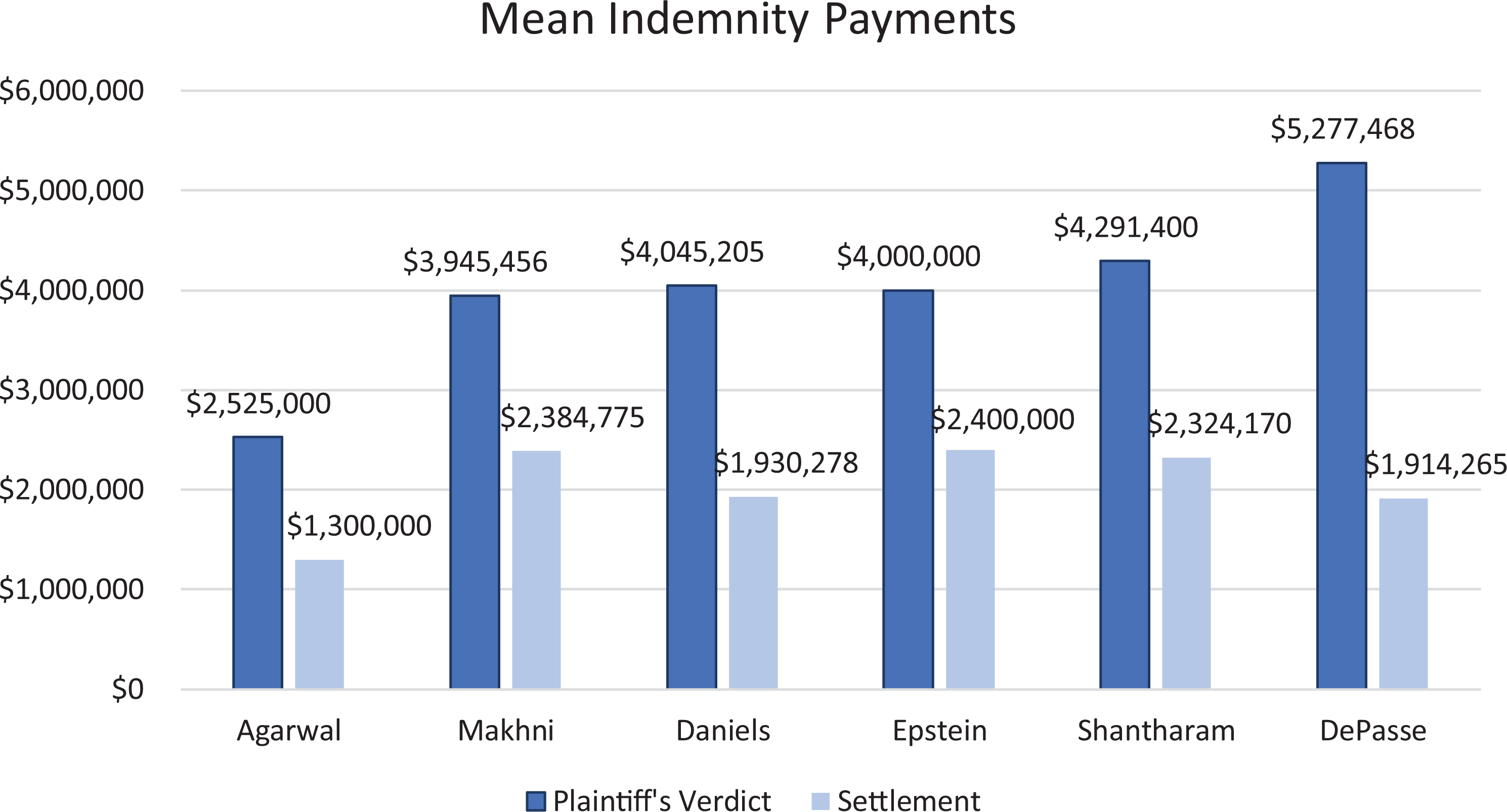
Spine cases that result in settlements or plaintiffs’ verdicts typically carry large indemnity payments (Figure 2). However, settlement amounts tend to be less than awards following verdicts. In their review of 98 cases, Agarwal et al 10 noted that the median indemnity awarded to a plaintiff in jury cases was $2 525 000 versus $1 300 000 in settlements. Interestingly, the authors also noted substantially higher median payouts following emergent cases (verdicts: $4 785 200 vs settlements: $2 800 000). 10 In a review of court proceedings arising from cervical cases, Epstein 7 reported mean awards of $4 000 000 in jury verdicts and $2 400 000 from settlements. Furthermore, the author also noted that plaintiffs’ mean indemnity through both jury verdict ($5 900 000) and settlement ($2 900 000) increased in cases with resulting quadriplegia. 7 These results demonstrate consistently lower payouts for cases ending in settlement than those decided by a jury. For these reasons, physicians nearing trial should carefully weigh the strength of their case with counsel when deciding how to proceed.
Cost of the Malpractice Litigation System
The medical malpractice system places a large economic burden on the United States’ health care system. While calculating the direct cost of this system may prove relatively straightforward, accounting for the indirect costs provides a greater challenge. Issues such as the practice of defensive medicine, physician time expenditure in litigation and the subsequent diminished availability of higher risk services may prove more costly to the health care system than direct expenditure.
Direct Costs of Malpractice
The national medical malpractice system has a high direct cost with a substantial contribution from legal fees and expenses. In a study using data from 2008, Mello et al 1 estimated direct expenses as approximately $9.8 billion dollars annually for the entire US health care system. The authors estimated defense litigation and administrative expenditures were $4.13 billion. 1 Excluding the plaintiffs’ legal costs, which are paid from indemnity payments, these figures suggest that legal fees and administrative costs associated with litigation account for 42.9% of the system’s direct costs. 1 Similarly, Kessler 20 and Studdert et al 21 reported that for every dollar spent on compensation, 54 cents went to attorney’s fees and administrative costs.
Studies investigating the direct costs of spine surgical litigation have highlighted the field’s high magnitude of indemnity payments and associated legal expenses. Rovit et al 3 reported mean indemnity payments of $457 453 for cervical spine and $485 182 for lumbar cases. Each of these indemnity averages exceeded the mean payment of all other specialties. 3 Even after achieving a successful result, defendants’ legal costs remain high. In their review of all claims filed against a single insurer, Rovit et al 3 reported average legal fee expenditures of $28 440 for cases not proceeding to trial and $73 000 for those that did. The combination of high indemnity payouts and defense expenditures manifests itself as higher malpractice premiums to providers. In a survey of the members of the American Association of Neurologic Surgeons, Nahed et al 17 reported that 70% of practicing neurosurgeons spend over 10% of their gross annual revenue on malpractice premiums. In a separate survey of neurosurgeons, Din et al 12 reported that surgeons performing mainly spine procedures spent on average $104 480.52 annually for professional liability insurance. Similarly in a 2011 survey, neurosurgeons reported $103 000 in mean annual malpractice premiums. 22 These high premium rates may affect physicians’ decisions on practice location, case mix or whether to provide high-risk services. 17
Indirect Costs of Malpractice
Though estimations of the malpractice system’s direct costs yield extremely high expenditures, indirect costs may prove even more expensive. 1 Issues such as physician time lost in legal proceedings, the practice of defensive medicine and litigation’s effect on physician psyche are more difficult to calculate but have a large impact on health care expenses and availability of services. In their estimation of the annual costs of the medical liability system, Mello et al 1 calculated $45.8 billion in indirect expenses. These expenditures represented 82.4% of the national medical malpractice system’s cost. 1
Physician time spent in litigation represents a major indirect cost of the malpractice system. Multiple authors have reported time ranges of 2.5 to 8.4 years for resolution of cases involving spine surgery. 5 -8,14 The time spent in litigation for cases depends on both the state in which the claim was filed and the ultimate case outcome. Epstein 7 noted wide variations in case adjudication times between states. For example, cases in Missouri reached a verdict in an average of 2.5 years while those in New York averaged 5.7 years. 7 Daniels et al 8 reported large differences in the average time to a decision for defense verdicts (5.1 years), plaintiffs’ verdicts (5.0 years), and settlements (3.4 years). These long periods of time in litigation exert a large toll on physicians in both opportunity costs and the psychological distress associated with legal defense. 6
Defensive Medicine
The now closed US Congress Office of Technology Assessment defined defensive medicine as, “when doctors order tests, procedures, or visits, or avoid certain high-risk patients or procedures, primarily (but not solely) because of concern about malpractice liability.” 1 Nationally, Mello et al 1 calculated the cost of defensive medicine as $45.59 billion dollars or 6.7% of annual health care spending. Rothberg et al 23 asked 42 physicians practicing within three hospitals to rate their previous day’s orders on a 5-point defensiveness scale between 0 (not at all defensive) and four (completely defensive). In this study, the authors reported that 28% of orders and 13% of costs were judged to be at least partially defensive and 2.9% of costs originated from orders which the physician graded as entirely defensive. 23
Though the previously outlined literature highlighted the burden defensive medicine has on the entire national health care system, numerous studies have focused on this practice specifically in spine surgery. In a survey of members of the American Board of Neurological Surgeons, Din et al 12 noted that providers who performed spine surgery as a majority of their case load ordered labs, medications, referrals, procedures, and imaging solely for liability concerns at significantly higher rates than those who performed fewer spine cases. These spine surgeons were roughly three times more likely to practice defensively than non-spine neurosurgeons when controlling for multiple associated variables. 12 Evidence suggests that the state litigation environment in which a spine surgeon practices may also affect medical decisions. 22 Missios and Bekelis 24 performed a retrospective cohort study combining data from the Nationwide Inpatient Sample, National Practitioner Data Bank and Area Resource File. The authors compared mortality rate, total hospital charges, and length of hospitalization for individuals undergoing spine surgery to the state’s mean dollar value of malpractice payments and the number of claims per 100 physicians practicing within the state. In this study, patients undergoing spine surgery had significantly increased hospitalization charges and lengths of stay in states within the highest quartile of claims per 100 physicians. 24 Additionally, an increase in the size of paid claims (paid claims represent both settlements and court awards captured in the National Practitioner Data Bank) reported to the National Practitioner Data Bank per physician within the state was also associated with a significant increase in length of stay and total hospital charges. 24 From this data, the authors extracted that a 1% increase in the size of paid claims per physician at the state level led to a 0.08% increase in average hospital charges after spine surgery. 24 Furthermore, 1 additional paid claim per 100 physicians in a state was associated with a 15.03% increase in average hospitalization. 24 Interestingly the authors noted that the number of claims filed in a state had no impact on the mortality rate after spine surgery. 24 This highlights the fact that as malpractice payouts increase, there is an increase in defensive medicine through comparatively longer hospital stays and additional, perhaps unnecessary ordering in the hospital.
A Just System?
The purpose of the medical legal liability system is to compensate patients for damages due to negligence and to deter providers from practicing in a negligent manner. 20 Though the modern medicolegal system proves very costly, it may not effectively achieve its goals. The high costs of litigation may cause some patients with legitimate claims to be turned away because the potential monetary award is too small to justify the time, resources and risk of a unfavorable outcome. 3 Additionally, in some cases the results of litigation do not match the strength of the evidence presented. Multiple studies, across various fields of medicine, have asked independent physicians to grade the strength of adjudicated malpractice claims. Defendants won 80% to 90% of cases where experts deemed they provided good medical care and approximately 70% of cases where medical care was uncertain. 25 -30 In a review of 36 cervical spine cases, Epstein 6 believed only 66.6% (10/15) of patients who received indemnity had legitimate claims. Conversely, 23.8% (5/21) of patients with legitimate claims did not receive indemnity. 6 Though no system can achieve perfect accuracy, the current environment seems to do a poor job providing indemnity to patients harmed due to negligence while also punishing a number of physicians who provided good medical care.
Minimizing the Risk and Effect of Litigation
While no generalized advice can eliminate the risk of litigation, examining common causes may prove helpful. A reported 24.4% to 56.4% of malpractice cases involve allegations that the spine surgeon did not obtain proper informed consent before surgery. 7,10,14 In most instances, a lack of informed consent reflects a communication failure of the important elements of the case, its risks and alternatives to surgery rather than the absence of a physical signed document. In a review of spine cases involving informed consent, Grauberger et al 31 noted that failure to explain the risk of surgery (30.4%) or alternative treatment options (9.9%) represented the most common allegations. Bhattacharyya et al 32 examined 28 cases alleging a lack of informed consent against orthopedic surgeons. In this study, the authors noted that documentation of the informed consent process in the medical record and obtaining informed consent in the surgeon’s office significantly lowered the rate of indemnity. 32 Conversely, obtaining the informed consent on the hospital ward or preoperative holding area was associated with a significantly higher risk of indemnity. 32 This data highlights the importance of both documentation and creating an environment that promotes physician-patient communication prior to surgery.
Developing and adhering to protocols to minimize the risk of wrong-level surgery or retained foreign body represents another strategy that surgeons can employ to minimize litigation. Through an online survey, nearly 50% of responding spine surgeons reported having performed a wrong level surgery at least once and approximately 10% admitted to performing a wrong side surgery. 33 In their review of 103 cases, Makhni et al 14 reported that these issues occurred in 6.8% of all cases (7/103). Though these errors do not occur in a large number of cases, they represent complications that can be minimized by spine surgeons. Spine surgeons should develop a consistent system to label, mark and identify operative levels that uses the assistance of intraoperative imaging. 34,35 Additionally, intraoperative radiographs immediately prior to closure can help assess for retained foreign bodies particularly in cases involving multiple levels, high blood loss or where discrepancies exist in the surgical count.
Finally, surgeons should strive to provide a timely diagnosis and treatment of issues requiring urgent or emergent care. Delays in both diagnosis and treatment represent 2 of the most consistent allegations in all studies reviewing litigation following spine surgery. 6 -10,14,19,36,37 These complaints correlate with higher rates of malpractice cases ending poorly for surgeons. Reviewing litigation following cases with cauda equina syndrome, Daniels et al 9 reported that delay in surgical intervention (>48 hours) represented the only tested variable that was significantly associated with adverse jury verdicts. Similarly, Agarwal et al 10 noted a significant relationship in cases citing a failure to treat and the incidence of a plaintiff’s verdict. To minimize these issues, physicians should aggressively investigate unexplained symptom constellations, particularly in the trauma and postoperative patient populations, and promptly care for identified progressive or time sensitive pathology.
Conclusion
The US medicolegal system places many challenges on a practicing spine surgeon. From the high monetary costs associated with liability insurance to observed defensive practice patterns, this system undoubtedly influences patient care. Through gaining a thorough understanding of the common pitfalls cited and general trends in case outcomes, spine surgeons can adapt responses to potentially lower their risk of litigation and better understand the system when claims are filed. More important, surgeons can better advocate for systemic changes that increase efficiency and produce equitable results in a timely and less costly manner.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.