
Abstract
Study Design
Prospective multicenter cohort study.
Objectives
Although surgery for degenerative cervical myelopathy (DCM) often improves neurological function, predicting clinically meaningful recovery remains challenging. To identify preoperative predictors of achieving the minimum clinically important difference (MCID) in the Japanese Orthopaedic Association (JOA) score and to evaluate its association with patient-reported outcomes.
Methods
We prospectively analyzed 762 patients with moderate to severe DCM (defined by preoperative JOA score <15) who underwent surgery at 10 high-volume centers in Japan, with a 2-year follow-up. MCID was defined as a ≥2.5-point improvement in JOA score. Logistic regression identified independent predictors. Outcomes included JOA score, Visual Analog Scale (VAS), the JOA Cervical Myelopathy Evaluation Questionnaire (JOACMEQ), and the 36-Item Short Form Health Survey (SF-36).
Results
MCID was achieved in 63.0% of patients. Independent predictors included younger age (Odds ratio = 0.973 [95% confidence interval: 0.956-0.990]; P = 0.002), absence of cerebrovascular (0.466 [0.224-0.960]; P = 0.039) and cardiac disease (0.510 [0.285-0.912]; P = 0.023), greater cervical lordosis (1.021 [1.004-1.037]; P = 0.013), lower baseline JOA score (0.547 [0.485-0.617]; P < 0.001), and higher JOACMEQ scores for upper extremity function (1.011 [1.000-1.022]; P = 0.044) and QOL (1.021 [1.009-1.033]; P < 0.001). MCID achievement was associated with significantly greater improvements in VAS, most JOACMEQ domains, and all SF-36 subscales.
Conclusions
Younger age, absence of cerebrovascular and cardiac disease, greater cervical lordosis, lower baseline JOA score, and higher preoperative JOACMEQ scores for upper extremity function and QOL were associated with achieving MCID in JOA score.
Keywords
Introduction
Degenerative cervical myelopathy (DCM), encompassing cervical spondylotic myelopathy (CSM) and ossification of the posterior longitudinal ligament (OPLL), is the most common cause of spinal cord dysfunction in adults. It is characterized by progressive neurological decline, reduced physical function, and diminished quality of life (QOL).1,2 Surgical decompression remains the standard treatment for symptomatic DCM and has been shown to prevent further neurological deterioration and improve functional outcomes.3,4
The Japanese Orthopaedic Association (JOA) score is a widely used clinical instrument for assessing neurological function in patients with DCM.5,6 While postoperative improvements in JOA scores are frequently observed, such changes may not always reflect benefits that are clinically meaningful. 7 To address this limitation, the concept of the minimum clinically important difference (MCID) has gained increasing relevance. MCID is defined as the smallest change in an outcome measure that is perceived as beneficial or meaningful by the patient, clinician, or both, and that may warrant a change in clinical management.8,9 In the context of DCM, the MCID of the JOA score has been estimated at approximately 2.5 points. 10
Recent studies have identified several factors associated with achieving the MCID after surgery for CSM, including younger age, absence of comorbidities, and shorter symptom duration.11-15 In patients with OPLL, prolonged symptom duration has been associated with reduced rates of MCID achievement and limited improvement in patient-reported outcome measures (PROMs), such as upper and lower limb function, bladder function, and quality of life. 11 Despite these findings, few studies have evaluated MCID achievement in a broader DCM population that includes both CSM and OPLL, while also incorporating PROMs to more comprehensively capture the patient perspective.11,12
The present multi-center prospective study aimed to identify independent predictors of achieving the MCID in JOA score following surgery for DCM. To ensure a focus on clinically meaningful improvement, we included only patients with moderate to severe DCM, excluding those with preoperative JOA scores ≥15 based on the rationale that such patients are unlikely to achieve a ≥2.5-point improvement. In addition, we examined the association between MCID achievement and improvements in PROMs, including the Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ) and the Short Form-36 (SF-36), thereby providing a multidimensional evaluation of postoperative recovery.
Materials and Methods
Study Design, Patient Demographics, and Characteristics
A prospective, multi-center investigation of cervical spine surgery was carried out across 10 high-volume institutions in Japan. From 2018 to 2022, 1482 individuals with various cervical spinal disorders were enrolled. Following the exclusion of those with atlantoaxial instability, cervical disc herniation, cervical radiculopathy, or cervical spondylotic amyotrophy, 1105 patients diagnosed with DCM remained eligible. A total of 935 patients had complete 2-year follow-up data after excluding those who did not complete the observation period. Of this group, 864 patients completed the JOA scoring evaluations and were included in the preliminary analysis. Subsequently, 102 patients with mild DCM (defined as a preoperative JOA score ≥15) were excluded, as a meaningful postoperative improvement (≥2.5 points) was considered unlikely. The final cohort analyzed thus comprised 762 patients.
Decisions regarding surgical indication, approach, and extent of decompression were made collaboratively by each institution’s spine team. Prospectively collected data included demographics, medical history, clinical symptoms, imaging findings, operative details, and postoperative outcomes. Comorbidities, including cardiac and cerebrovascular disease, were identified based on physician diagnosis and confirmed through review of medical records at each institution. The study protocol was approved by the Institutional Review Board (approval number: 20180045), and written informed consent was obtained from all participants prior to surgery.
Radiographs and MRI Findings
In this study, radiological assessments of the cervical spine were performed by measuring the C2-7 angle on plain lateral radiographs taken in neutral, flexion, and extension positions at 2 time points: preoperatively and at 2 years following surgery. The C2-7 angle was measured using the Cobb method, which quantifies the angle between the lower endplates of the C2 and C7 vertebrae. Cervical range of motion (ROM) was calculated by subtracting the flexion C2-7 angle from the extension C2-7 angle. Preoperative MRI was used to evaluate the levels of stenosis and to detect areas of high intramedullary signal intensity on T2-weighted images.
Clinical Outcomes
The primary outcome of this study was the achievement of the MCID in cervical JOA score, defined as an improvement of ≥2.5 points at 2-year follow-up. Secondary outcomes included changes in PROMs (JOACMEQ and SF-36), Visual Analog Scale (VAS) pain scores, and the incidence of perioperative complications. The JOA score, with a maximum of 17 points, was used as the primary measure of neurological function. The JOA score recovery rate (%) was calculated using the following formula: (JOA score at 2 years postoperatively – preoperative JOA score) / (17 – preoperative JOA score) × 100, reflecting the percentage improvement relative to baseline. 16 In addition, the change in JOA score (postoperative JOA score – preoperative JOA score) was evaluated. As the MCID for the JOA score in DCM has been reported to be approximately 2.5 points, a gain of ≥2.5 points was considered clinically meaningful. 11 Based on this threshold, patients were divided into 2 groups in the present study: the Not-achieved group (JOA score improvement <2.5, indicating failure to achieve MCID) and the Achieved group (JOA score improvement >2.5, indicating MCID attainment).
Symptoms such as neck or shoulder pain and stiffness, chest tightness, and pain or numbness in the arms, hands, or lower body (chest to toes) were evaluated using the VAS, with scores ranging from 0 to 100 mm. Lower scores indicated less pain and greater patient comfort. The JOACMEQ evaluates health-related quality of life and functional status across key domains, including the cervical spine, upper and lower extremities, and bladder function. 17 The SF-36 assesses 8 health subdomains, physical functioning (PF), role-physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role-emotional (RE), and mental health (MH), and generates 2 summary scores: the physical component summary (PCS) and the mental component summary (MCS). 18 All adverse events related to surgery that occurred within 30 days postoperatively were classified as perioperative complications.
Predictive Factors for Achieving the MCID in Cervical JOA Score
Patient Baseline Demographic Information on 762 Patients With DCM Enrolled in this Study
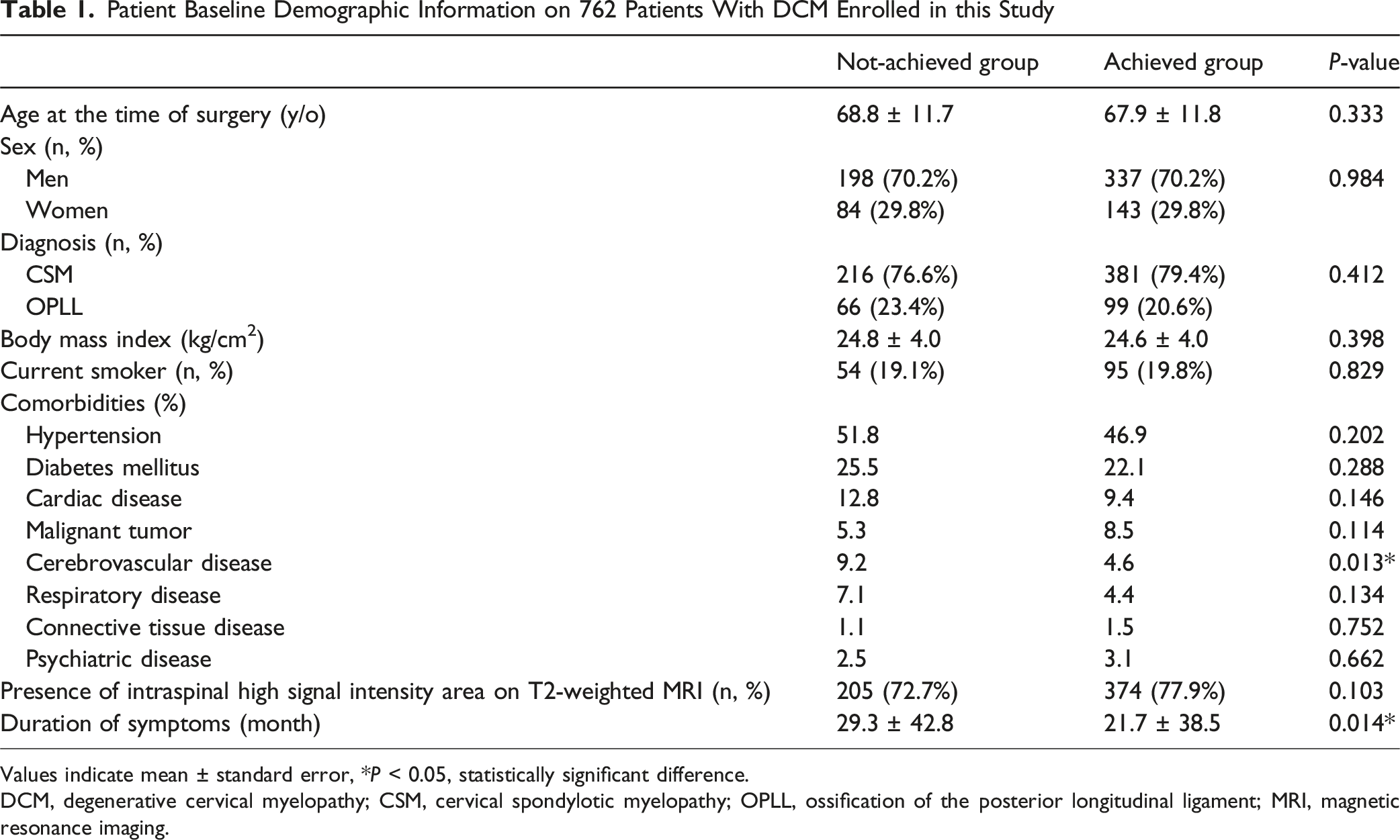
Values indicate mean ± standard error, *P < 0.05, statistically significant difference.
DCM, degenerative cervical myelopathy; CSM, cervical spondylotic myelopathy; OPLL, ossification of the posterior longitudinal ligament; MRI, magnetic resonance imaging.
Comparison of Surgical Information and Perioperative Complications
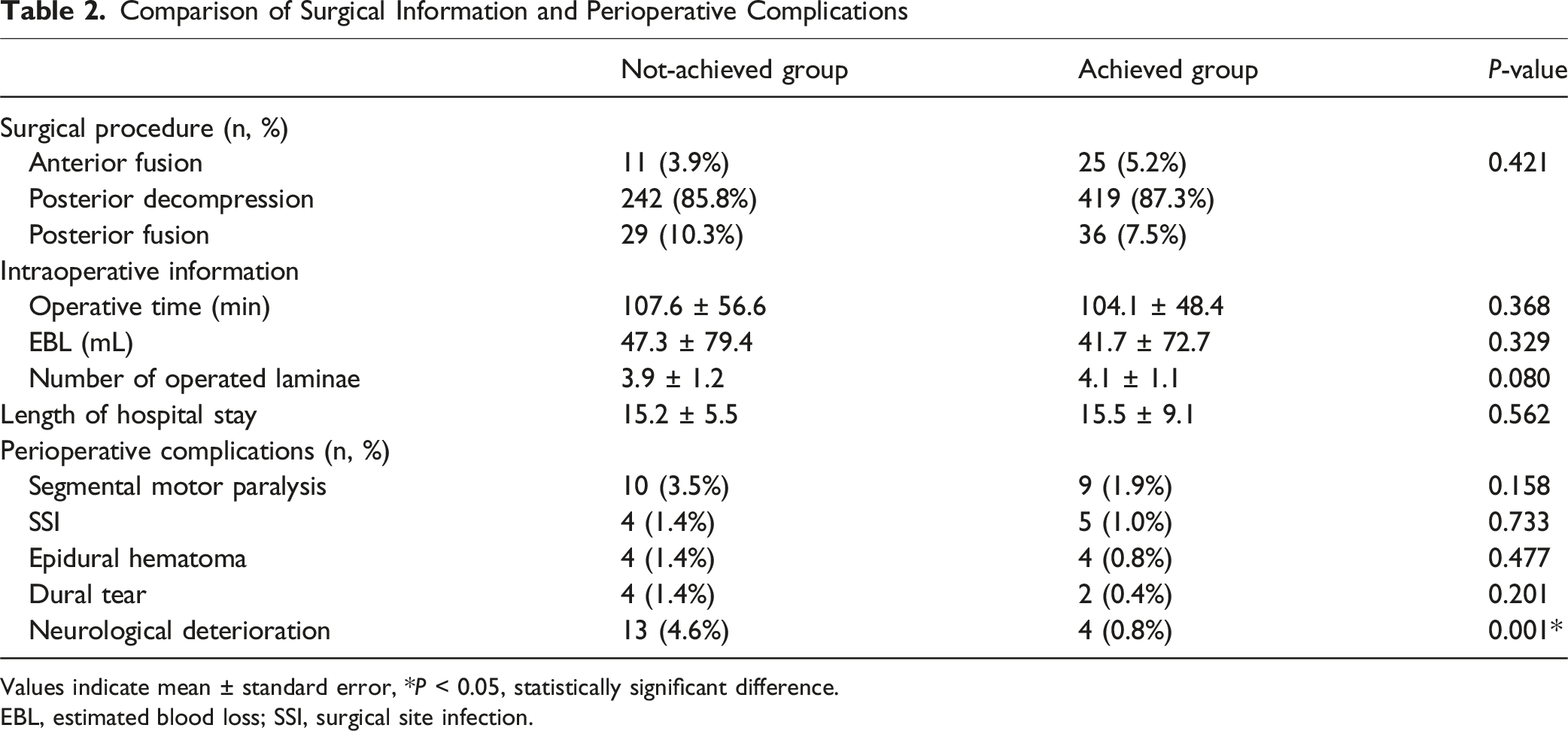
Values indicate mean ± standard error, *P < 0.05, statistically significant difference.
EBL, estimated blood loss; SSI, surgical site infection.
Comparison of Preoperative and 2-Year Following Surgery Each Cervical Sagittal Parameter
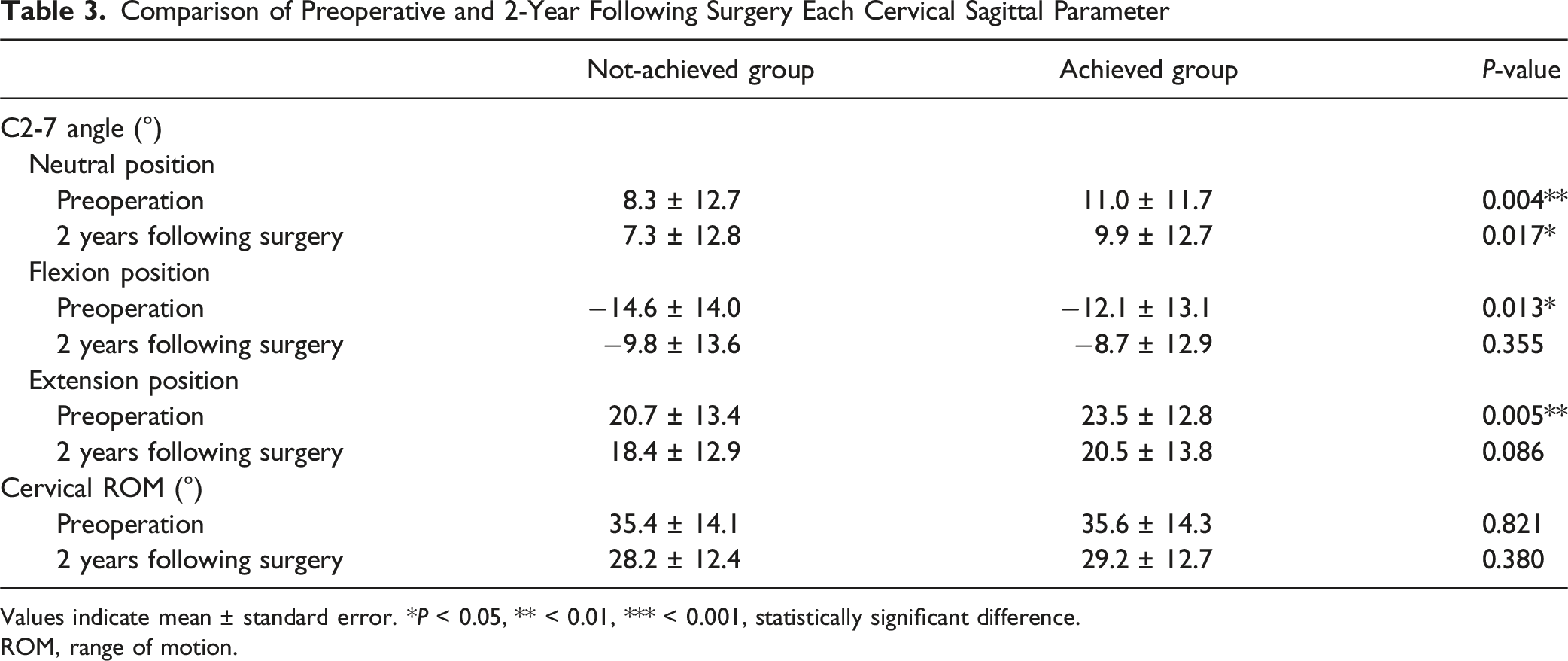
Values indicate mean ± standard error. * P < 0.05, ** < 0.01, *** < 0.001, statistically significant difference.
ROM, range of motion.
Comparison of Clinical Outcomes Between Not-Achieved and Achieved Group
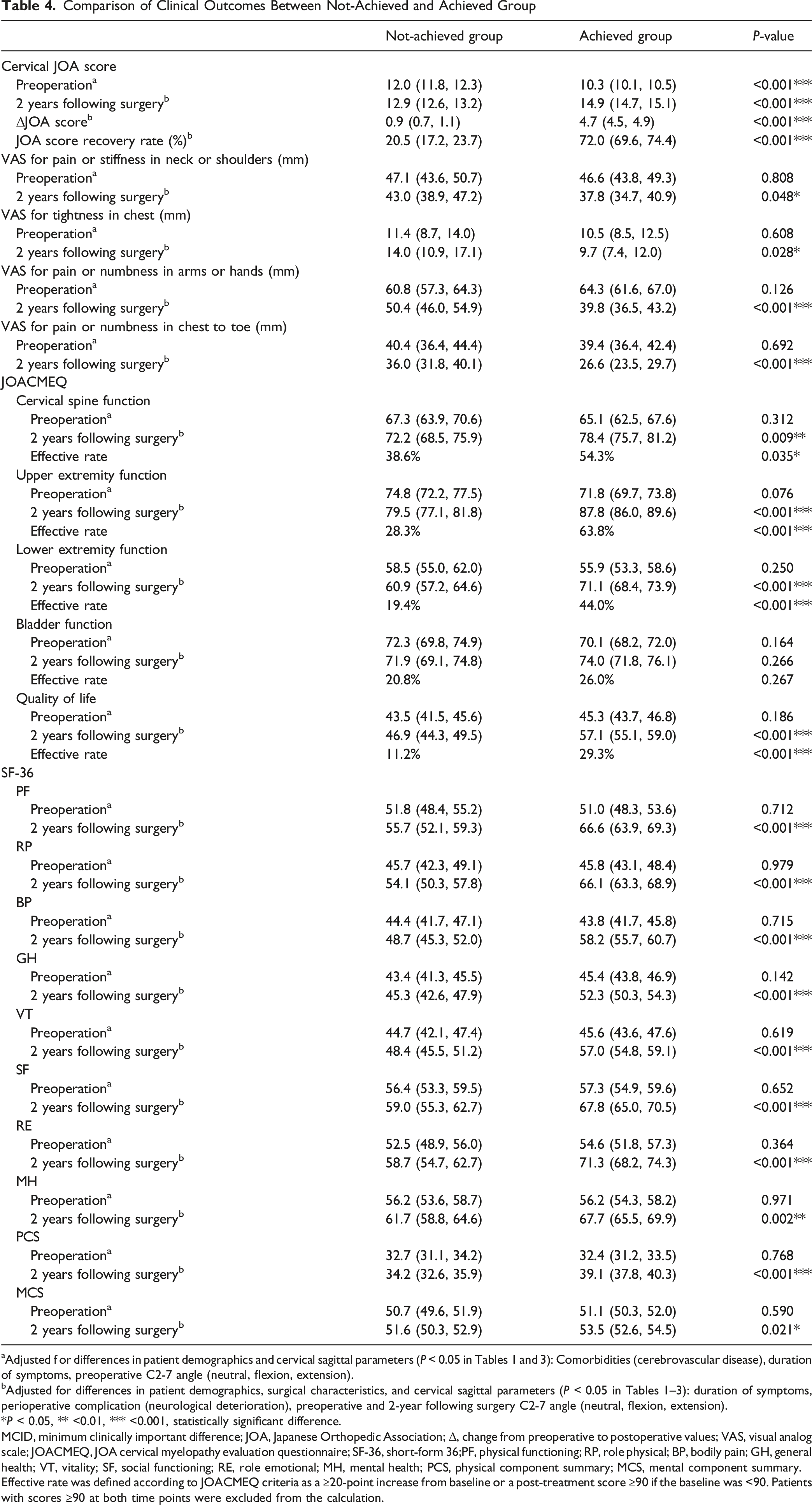
Adjusted f or differences in patient demographics and cervical sagittal parameters (P < 0.05 in Tables 1 and 3): Comorbidities (cerebrovascular disease), duration of symptoms, preoperative C2-7 angle (neutral, flexion, extension).
bAdjusted for differences in patient demographics, surgical characteristics, and cervical sagittal parameters (P < 0.05 in Tables 1–3): duration of symptoms, perioperative complication (neurological deterioration), preoperative and 2-year following surgery C2-7 angle (neutral, flexion, extension).
*P < 0.05, ** <0.01, *** <0.001, statistically significant difference.
MCID, minimum clinically important difference; JOA, Japanese Orthopedic Association; Δ, change from preoperative to postoperative values; VAS, visual analog scale; JOACMEQ, JOA cervical myelopathy evaluation questionnaire; SF-36, short-form 36;PF, physical functioning; RP, role physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role emotional; MH, mental health; PCS, physical component summary; MCS, mental component summary.
Effective rate was defined according to JOACMEQ criteria as a ≥20-point increase from baseline or a post-treatment score ≥90 if the baseline was <90. Patients with scores ≥90 at both time points were excluded from the calculation.
Statistical Analysis
Normality of continuous variables was assessed using the Shapiro–Wilk test and visual inspection of histograms. All continuous variables included in the analysis satisfied the assumptions of normality and were summarized as means ± standard deviations. Categorical variables were summarized as percentages. Comparisons between the Not-achieved and Achieved groups in terms of baseline demographics, surgical characteristics, radiographic findings, and clinical outcomes were conducted using unpaired t-tests for continuous variables and chi-square tests for categorical variables. Binary logistic regression analyses were performed to adjust for potential confounding factors in the comparison of JOA scores, VAS, JOACMEQ, and SF-36 outcomes. The primary metric used to assess domain-specific improvement in the JOACMEQ was the “effective rate,” which reflects the proportion of patients meeting predefined criteria for treatment response in each domain. According to the JOACMEQ criteria, treatment effectiveness was defined as either (1) a post-treatment score that was at least 20 points higher than the pre-treatment score, or (2) a pre-treatment score below 90 with a post-treatment score of 90 or greater. Patients who had both pre- and post-treatment scores of 90 or higher were included in the dataset but excluded from the effectiveness analysis. The effective rate for each group was calculated as follows: (Number of patients classified as “effective”) / [(Total number of patients in the group) − (Number of patients with pre- and post-treatment scores ≥90)]. 17 Intergroup comparisons of effective rates were performed using the chi-square test. Statistical significance was determined at P-values of <0.05, <0.01, and <0.001. All statistical analyses were conducted using SPSS version 29.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline Demographics and Clinical Characteristics
Based on improvements in JOA score, 282 patients (37.0%) did not achieve the MCID and were categorized into the ‘Not-achieved’ group, while the remaining 480 patients (63.0%) met the MCID and were classified into the ‘Achieved’ group. No significant differences were observed between the 2 groups in age at the time of surgery (68.8 ± 11.7 vs 67.9 ± 11.8 years, P = 0.333), sex distribution (Men: 70.2% vs 70.2%; Women: 29.8% vs 29.8%; P = 0.984), BMI (24.8 ± 4.0 vs 24.6 ± 4.0 kg/m2, P = 0.398), current smoker (19.1% vs 19.8%, P = 0.829), or diagnosis (CSM: 76.6% vs 79.4%, OPLL: 23.4% vs 20.6%; P = 0.412). Among comorbidities, cerebrovascular disease was significantly more prevalent in the Not-achieved group (9.2% vs 4.6%, P = 0.013), whereas no significant differences were detected between the groups for other comorbid conditions. Intraspinal high signal intensity area on T2-weighted MRI was present in 72.7% of the Not-achieved group and 77.9% of the Achieved group, with no significant difference between the 2 groups (P = 0.103). The duration of symptoms was significantly longer in the Not-achieved group compared to the Achieved group (29.3 ± 42.8 vs 21.7 ± 38.5 months, P = 0.014) (Table 1).
Surgical Data and Perioperative Complications
There were no significant differences in surgical procedure between the 2 groups (P = 0.421): anterior fusion (3.9% vs 5.2%), posterior decompression (85.8% vs 87.3%), and posterior fusion (10.3% vs 7.5%). Intraoperative information, including operative time (107.6 ± 56.6 vs 104.1 ± 48.4 min, P = 0.368), EBL (47.3 ± 79.4 vs 41.7 ± 72.7 mL, P = 0.329), and number of operated laminae (3.9 ± 1.2 vs 4.1 ± 1.1, P = 0.080), showed no significant differences. Length of hospital stay was comparable (15.2 ± 5.5 vs 15.5 ± 9.1 days, P = 0.562). Among perioperative complications, the incidence of neurological deterioration was significantly higher in the Not-achieved group (4.6% vs 0.8%, P = 0.001), while other complications, including segmental motor paralysis, surgical site infection, epidural hematoma, and dural tear, did not differ significantly. (Table 2)
Postoperative Changes in Cervical Sagittal Alignments
The Achieved group demonstrated significantly greater cervical lordosis in the neutral position both preoperatively (8.3 ± 12.7° vs 11.0 ± 11.7°, P = 0.004) and at 2-year follow-up (7.3 ± 12.8° vs 9.9 ± 12.7°, P = 0.017). Preoperative C2-7 angles in both flexion (−14.6 ± 14.0° vs −12.1 ± 13.1°, P = 0.013) and extension (20.7 ± 13.4° vs 23.5 ± 12.8°, P = 0.005) were also significantly higher in the Achieved group, though no significant differences were found postoperatively in these positions. Cervical ROM did not differ significantly between groups at either time point (Table 3). Furthermore, postoperative evaluations showed no evidence of new-onset spondylolisthesis, scoliosis progression, recurrent stenosis, or advancement of OPLL at the site of posterior cervical decompression.
Clinical Outcomes after Surgery
The Achieved group had significantly greater postoperative improvements. Adjusted preoperative JOA scores were lower in the Achieved group (12.0 [11.8-12.3] vs 10.3 [95% CI: 10.1-10.5], P < 0.001), while postoperative JOA scores were significantly higher (12.9 [12.6-13.2] vs 14.9 [14.7-15.1], P < 0.001). The mean improvement in JOA score (ΔJOA) was 4.7 [4.5-4.9] in the Achieved group, compared with 0.9 [0.7-1.1] in the Not-achieved group (P < 0.001). The JOA score recovery rate was also significantly higher in the Achieved group, at 72.0% [69.6-74.4] compared with 20.5% [17.2-23.7] (P < 0.001). The Achieved group also demonstrated significantly greater improvements in VAS scores for pain or stiffness in neck/shoulder (43.0 [38.9-47.2] mm vs 37.8 [34.7-40.9] mm, P = 0.048), tightness in chest (14.0 [10.9-17.1] mm vs 9.7 [7.4-12.0] mm, P = 0.028), pain or numbness in arms/hands (50.4 [46.0-54.9] mm vs 39.8 [36.5-43.2] mm, P < 0.001), and in chest to toe (36.0 [31.8-40.1] mm vs 26.6 [23.5-29.7] mm, P < 0.001). In JOACMEQ assessments, the Achieved group showed significantly better postoperative scores in cervical function (72.2 [68.5-75.9] vs 78.4 [75.7-81.2], P = 0.009), upper extremity function (79.5 [77.1-81.8] vs 87.8 [86.0-89.6], P < 0.001), lower extremity function (60.9 [57.2-64.6] vs 71.1 [68.4-73.9], P < 0.001), and QOL (46.9 [44.3-49.5] vs 57.1 [55.1-59.0], P < 0.001). The effective rate, as defined by the JOACMEQ criteria, was used to quantify clinically meaningful improvement in each domain. The Achieved group showed significantly higher effective rates in most JOACMEQ domains. Effective rates for cervical spine, upper extremity, and lower extremity function were 54.3%, 63.8%, and 44.0%, respectively, compared to 38.6%, 28.3%, and 19.4% in the Not-achieved group (P = 0.035, <0.001, and <0.001, respectively). The effective rate for QOL was also significantly higher in the Achieved group (11.2% vs 29.3%, P < 0.001). Meanwhile, no significant difference was found in bladder function (20.8% vs 26.0%, P = 0.267). Similarly, the Achieved group showed significantly greater improvements across all SF-36 subscales and both component summary scores. At 2 years following surgery, mean scores for PF, RP, BP, GH, VT, SF, RE, and MH were all significantly higher in the Achieved group (P < 0.01 for all). Both the PCS and MCS scores were also significantly better in the Achieved group (P < 0.001 and P = 0.021, respectively) (Table 4).
Predictors of MCID Achievement
Multivariate Logistic Regression Analysis of Predictors for MCID Achievement of JOA Score
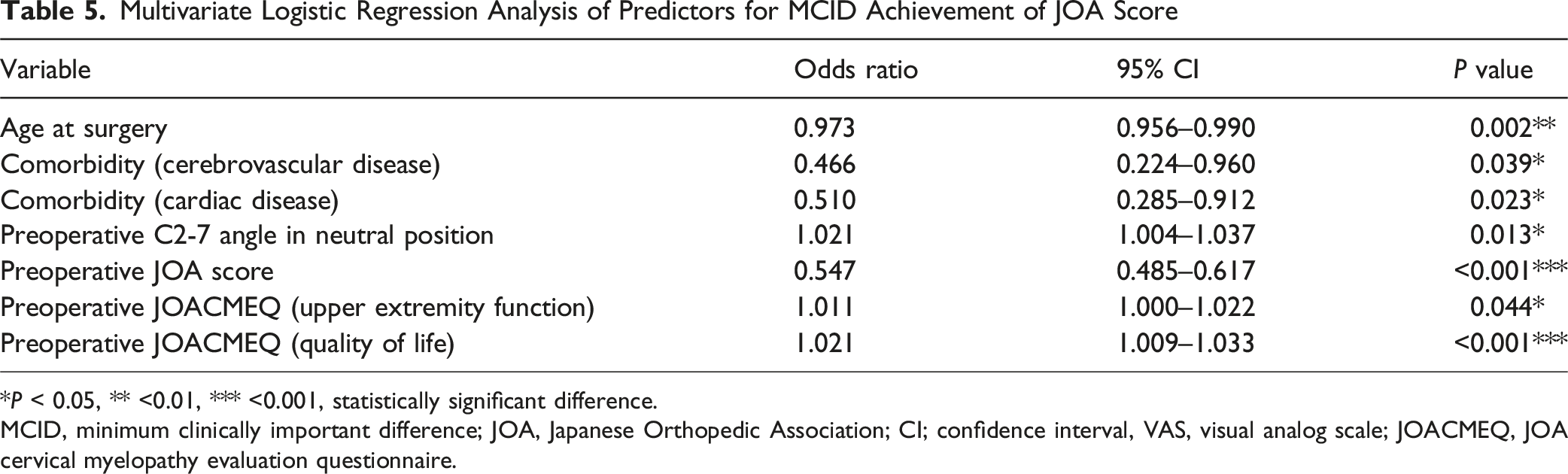
*P < 0.05, ** <0.01, *** <0.001, statistically significant difference.
MCID, minimum clinically important difference; JOA, Japanese Orthopedic Association; CI; confidence interval, VAS, visual analog scale; JOACMEQ, JOA cervical myelopathy evaluation questionnaire.
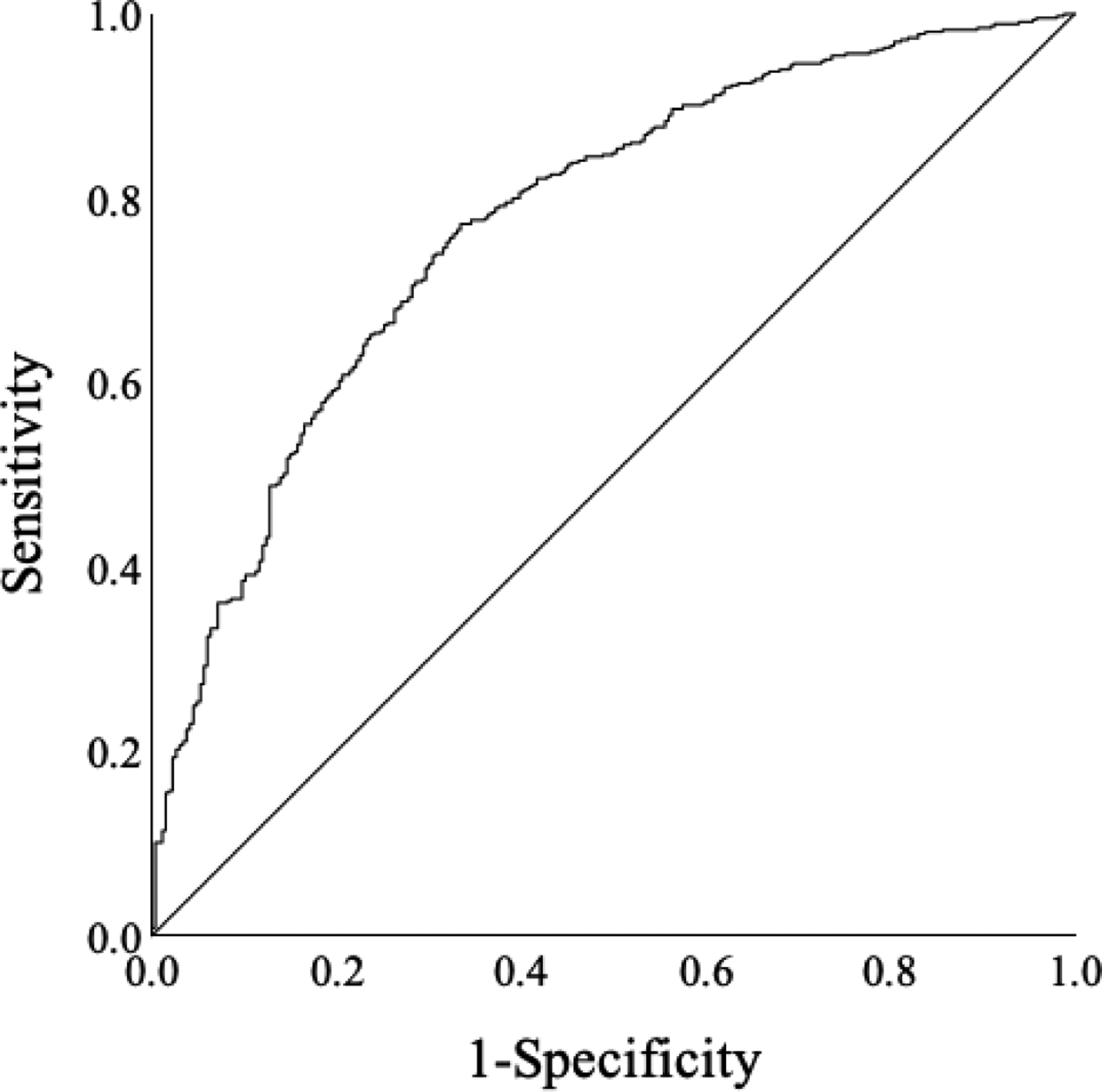
ROC Curve Evaluating the Predictive Accuracy of the Logistic Regression Model for Achieving the MCID in the JOA Score
Discussion
This large prospective study identified predictors of achieving the MCID in cervical JOA score after DCM surgery. Among 762 patients, younger age, absence of cerebrovascular or cardiac disease, greater cervical lordosis, and lower preoperative JOA scores were independent predictors. Higher baseline JOACMEQ scores for upper extremity function and QOL were also linked to better outcomes. Compared to the Not-achieved group, the Achieved group showed significantly greater improvements in clinician- and patient-reported measures, including VAS, JOACMEQ, and all SF-36 domains. The multivariate model demonstrated good predictive accuracy (AUC = 0.775). These results suggest that MCID achievement is influenced not only by surgery but also by preoperative neurological status, comorbidities, and alignment, emphasizing the value of comprehensive preoperative evaluation.
Several previous studies have suggested that younger age is associated with more favorable surgical outcomes in patients with DCM.13,19-22 Nakashima et al. reported that significantly greater postoperative recovery in younger patients based on modified JOA and Nurick scores, 20 while Tetreault et al. identified that age as an independent predictor of achieving the MCID in functional outcomes. 13 In the present study, univariate analysis did not show a significant difference in age at the time of surgery between Not-achieved and Achieved group. However, binary logistic regression analysis identified younger age as a significant independent predictor of MCID achievement in the cervical JOA score. This discrepancy between univariate and multivariate findings suggests that the influence of age may only become apparent when accounting for other confounding variables. While univariate analysis evaluates each factor in isolation, it may not fully reflect the underlying relationships between variables. Multivariate analysis, by adjusting for covariates such as comorbidities, baseline neurological function, and cervical alignment, allows for a more accurate assessment of the independent effect of age. These findings indicate that younger patients tend to experience greater improvement after surgery, likely due to more adaptable neural function, better overall physical condition, and fewer age-related degenerative changes.
Previous research has indicated a potential association between cervical spine pathology and systemic vascular conditions. Chen et al. reported a higher risk of posterior circulation infarcts in patients with cervical spondylosis, possibly due to altered vertebrobasilar flow from chronic degeneration. 23 Lin et al. similarly found increased rates of acute coronary syndrome and arrhythmias, indicating a broader vascular burden in these patients.24,25 In the present study, cerebrovascular and cardiac diseases were independently associated with reduced likelihood of achieving MCID in cervical JOA score. These comorbidities may hinder recovery by impairing spinal cord perfusion, limiting neuroregeneration, and complicating perioperative care. Reduced physiological reserve and rehabilitation potential may further limit functional gains. Taken together, these results indicate that systemic vascular comorbidities, particularly cerebrovascular and cardiac conditions, should be taken into account when evaluating surgical outcomes in patients with DCM.
Preoperative cervical sagittal alignment has emerged as an important factor in postoperative neurological recovery in DCM.26-29 In this study, greater cervical lordosis in the neutral position independently predicted MCID achievement in the cervical JOA score. Suda et al. reported that a segmental kyphosis over 13° was linked to poorer outcomes after laminoplasty for CSM, indicating that kyphotic deformity may impair spinal cord decompression. 26 Shamji et al. similarly found that patients with kyphotic alignment had less favorable neurological recovery than those with lordotic alignment. 27 In contrast, Lee et al. observed no clear association between sagittal alignment and outcomes after laminoplasty in OPLL, possibly due to differing pathophysiology or patient selection. 28 Considering the collective evidence, preserving or restoring cervical lordosis appears to contribute meaningfully to achieving clinically important neurological improvement following posterior decompression. Careful preoperative assessment of cervical sagittal alignment should therefore be regarded as an essential component of surgical planning in patients with DCM.
The clinical relevance of PROMs in evaluating recovery after surgery for DCM has gained increasing recognition.12,17,18,30-33 The JOACMEQ was developed as a disease-specific instrument to assess domains such as cervical spine function, upper and lower extremity function, bladder function, and QOL. 17 Nikaido et al. validated its use in surgical assessment, demonstrating its responsiveness to clinical change. 31 Similarly, the SF-36 has been widely used to evaluate health-related QOL in patients with DCM, 18 with King et al. showing its sensitivity to neurological impairment and postoperative improvement. 32 In the current study, the Achieved group demonstrated significantly greater improvements across all SF-36 domains and most JOACMEQ domains. In contrast, no significant postoperative difference was observed between the 2 groups in the bladder function domain, suggesting that autonomic recovery is less responsive to surgical intervention. Additionally, lower preoperative JOA scores were associated with higher rates of MCID achievement, likely reflecting a greater capacity for measurable improvement among patients with more severe baseline neurological impairment. These findings support the complementary use of PROMs such as the JOACMEQ and SF-36 alongside clinician-based assessments, enabling a more comprehensive and patient-centered evaluation of surgical outcomes in DCM. The JOA score reflects objective neurological deficits, while the JOACMEQ captures patient-perceived function. Some patients may report relatively high QOL or upper extremity function despite residual neurological impairment, allowing for measurable postoperative improvement. Moreover, the absence of ceiling effects and potential score mismatches between clinician- and patient-rated scales may have contributed to this association. While the JOACMEQ provides disease-specific insight into function and quality of life across domains relevant to cervical myelopathy, we acknowledge that it may not fully capture broader aspects of physical and psychosocial well-being. Therefore, the inclusion of the SF-36 in our analysis offers a more comprehensive perspective on patients’ overall health status following surgery.
The incidence of perioperative neurological deterioration was significantly higher in the Not-achieved group. This complication, defined as new or worsening motor or sensory deficits within 30 days after surgery, may indicate greater surgical vulnerability in this subgroup. Contributing factors could include longer symptom duration, more severe baseline cord compression, or chronic spinal cord changes, all of which may increase the risk of intraoperative injury. Although uncommon, such events may have adversely impacted the potential for postoperative neurological recovery in these patients.
Several limitations should be noted in the present study. First, the surgical procedures and approaches were not randomized, which may have introduced selection bias. Laminoplasty accounted for the majority of decompression procedures in this cohort and is typically selected for patients with favorable sagittal alignment. As greater cervical lordosis was identified as a predictor of MCID achievement, it is possible that preoperative alignment influenced both the surgical approach and outcomes, thereby confounding the observed associations. Second, the duration of symptoms was self-reported and thus subject to potential recall bias. Third, we applied a uniform MCID threshold of 2.5 points for the JOA score, although the optimal value may vary depending on baseline severity. In line with this definition, patients with mild DCM (preoperative JOA score ≥15) were excluded, as they were unlikely to demonstrate such improvement. As a result, the findings of this study apply primarily to patients with moderate to severe disease and may not be generalizable to those with milder forms of DCM. Finally, the follow-up period was limited to 2 years, and long-term outcomes remain to be clarified. In addition, the study cohort consisted entirely of patients treated in Japan. As such, differences in baseline characteristics, surgical preferences, and healthcare delivery systems may limit the generalizability of these findings to other populations. Despite these limitations, the present study was strengthened by its large, diverse cohort, the use of validated PROMs, and robust statistical analysis to identify clinically meaningful predictors of neurological recovery and QOL improvement.
Conclusion
In this multicenter prospective study of patients with DCM, younger age, absence of cerebrovascular and cardiac comorbidities, greater cervical lordosis, lower preoperative JOA scores, and higher JOACMEQ scores for upper extremity function and QOL were independently associated with achieving MCID. Patients who achieved MCID demonstrated significantly greater improvements in both clinician- and patient-reported outcomes. These findings suggest the multifactorial nature of surgical recovery in DCM and support the complementary use of PROMs alongside traditional outcome metrics. Comprehensive preoperative assessment may facilitate more accurate prediction of surgical benefit and contribute to improved patient-centered care.
Footnotes
Acknowledgments
We extend our sincere appreciation to all participating institutions for their collaboration and support. During the preparation of this manuscript, ChatGPT (OpenAI) and Grammarly (Grammarly Inc.) were used to refine grammar and correct typographical errors. These tools were employed solely to enhance clarity and readability, without altering the scientific content or interpretation of the results.
ORCID iDs
Ethical Consideration
The study protocol was approved by the Institutional Review Board (approval number: 20180045).
Consent to Participate
Written informed consent was obtained from all participants prior to their inclusion in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed in this study are available from the corresponding author on request.