
Abstract
Study Design
Systematic Literature Review.
Objective
The aim of this literature review is to examine the results of total disc arthroplasty in the setting of cervical myelopathy.
Methods
A systematic review of the relevant literature examining the efficacy of cervical disc arthroplasty (CDA) in patients with cervical myelopathy was conducted using the Medline database.
Results
Our query identified 288 potentially relevant articles. After eliminating duplicate articles and screening by title and abstract 115 articles underwent full-text review. Of these, 15 were deemed relevant to the research questions posed. Evaluation of references identified 2 additional relevant articles.
Conclusion
Evaluation of outcomes measures, radiographic analysis, and failure due to implant related complications is equivalent in comparing CDA to Anterior Cervical Discectomy and Fusion (ACDF). From the literature available, the outcomes in patients undergoing cervical disc arthroplasty are at least equal to those of ACDF. The concern for persistent symptoms in patients treated with CDA due to the dynamic component on myelopathy is theoretic and not supported by the available literature.
Keywords
Introduction
Cervical myelopathy is a debilitating condition with an incidence of myelopathy-related hospitalizations estimated at 4.04/100 000 person-years, with surgical rates on the rise. 1 With increasing numbers of surgical interventions, predicting persistent myelopathy remains a critical concern. Varying patient populations, surgical techniques, and specific devices for cervical myelopathy have been utilized. Anterior cervical discectomy and fusion has been the gold standard for the anterior based treatment of myelopathy in patients with disc level pathology. Over the past 20 years, cervical disc arthroplasty has been widely accepted as an alternative to ACDF, gaining popularity in the treatment of cervical disc level pathology in appropriately selected patients. Numerous Investigational Device Exemption (IDE) studies have demonstrated the efficacy of cervical disc arthroplasty as compared to ACDF. Despite this, actual outcomes of patients undergoing CDA for the treatment of myelopathy specifically has rarely been addressed. Cervical myelopathy is a disease process that includes both static and dynamic factors. From the latter, concern exists regarding persistence of myelopathic symptoms in patients who undergo cervical disc arthroplasty. We therefore sought to determine the incidence and predictors of persistent myelopathy symptoms after CDA, as well as to assess whether these outcomes differed between CDA and ACDF.
Methods
A systematic review of the Medline database was performed to evaluate all published literature between September 1, 1989 through August 31, 2024. Search terms included: “(Total disc arthroplasty or cervical disc arthroplasty) and (cervical myelopathy or cervical spondylitis myelopathy or cervical spondylosis myelopathy).” (Chart 3) Two investigators, AB and IL, independently reviewed all retrieved titles and abstracts for relevance. Studies reporting the outcomes and complication rates of patients undergoing cervical disc arthroplasty in the setting of myelopathy were included. Studies that did not specify myelopathy vs treatment for radiculopathy were excluded. Additionally, studies comparing patients with myelopathy who had undergone cervical disc arthroplasty or anterior cervical discectomy and fusion were included. Studies that were purely editorial, not available in English or had not been subjected to peer review were also excluded. Each reviewer independently performed full text evaluation of all potentially relevant. Duplicate articles were removed at this step. Articles meeting inclusion criteria and answering one of the posed questions were included in this review. Discrepancies on inclusion determination at this point were settled through independent review by the senior author, UA. Relevant studies were cross referenced to identify articles that may have not been captured in the initial database queries.
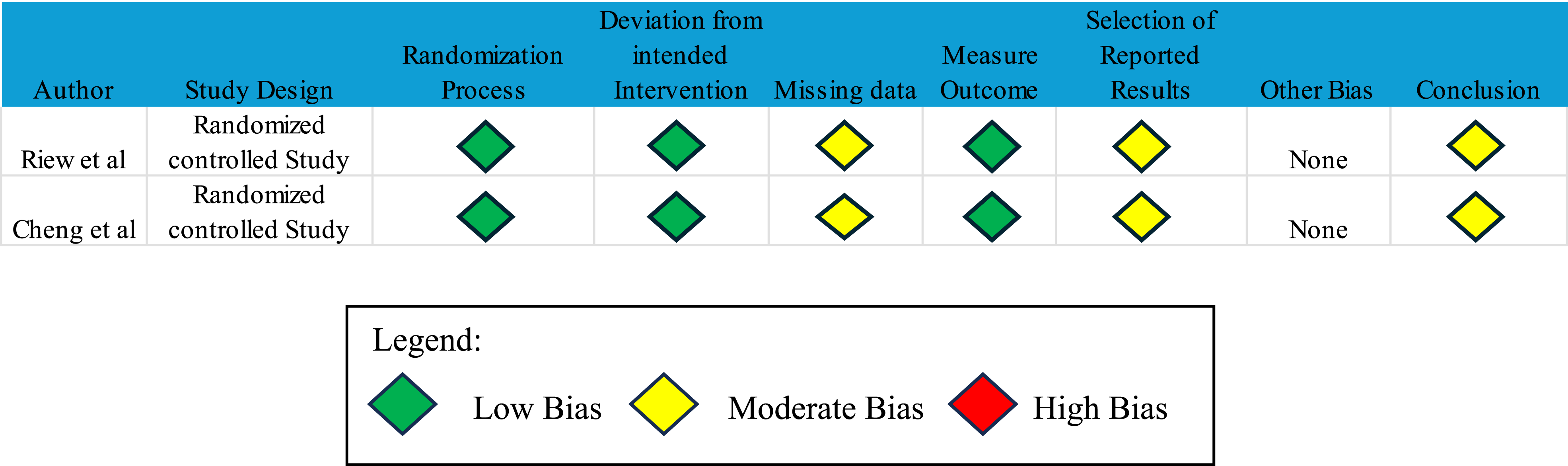
Bias Analysis
Each included study was evaluated for potential bias. Randomized trials were assessed using version 2 of the Risk of Bias tool (RoB 2) (Chart 1).
1
Nonrandomized studies were evaluated using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool (Chart 2).
2
Bias analysis for non-randomized studies Bias analysis for randomized controlled studies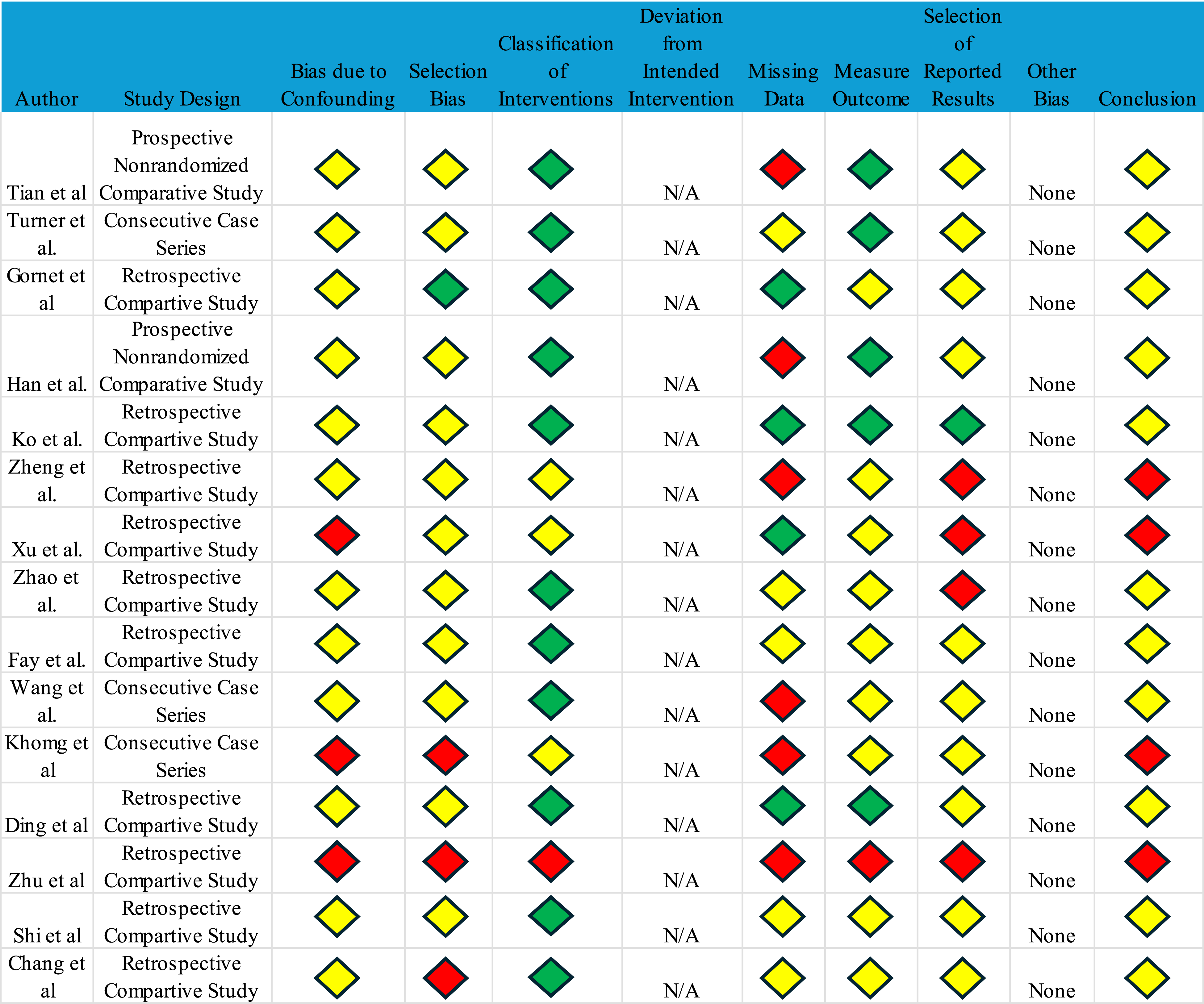
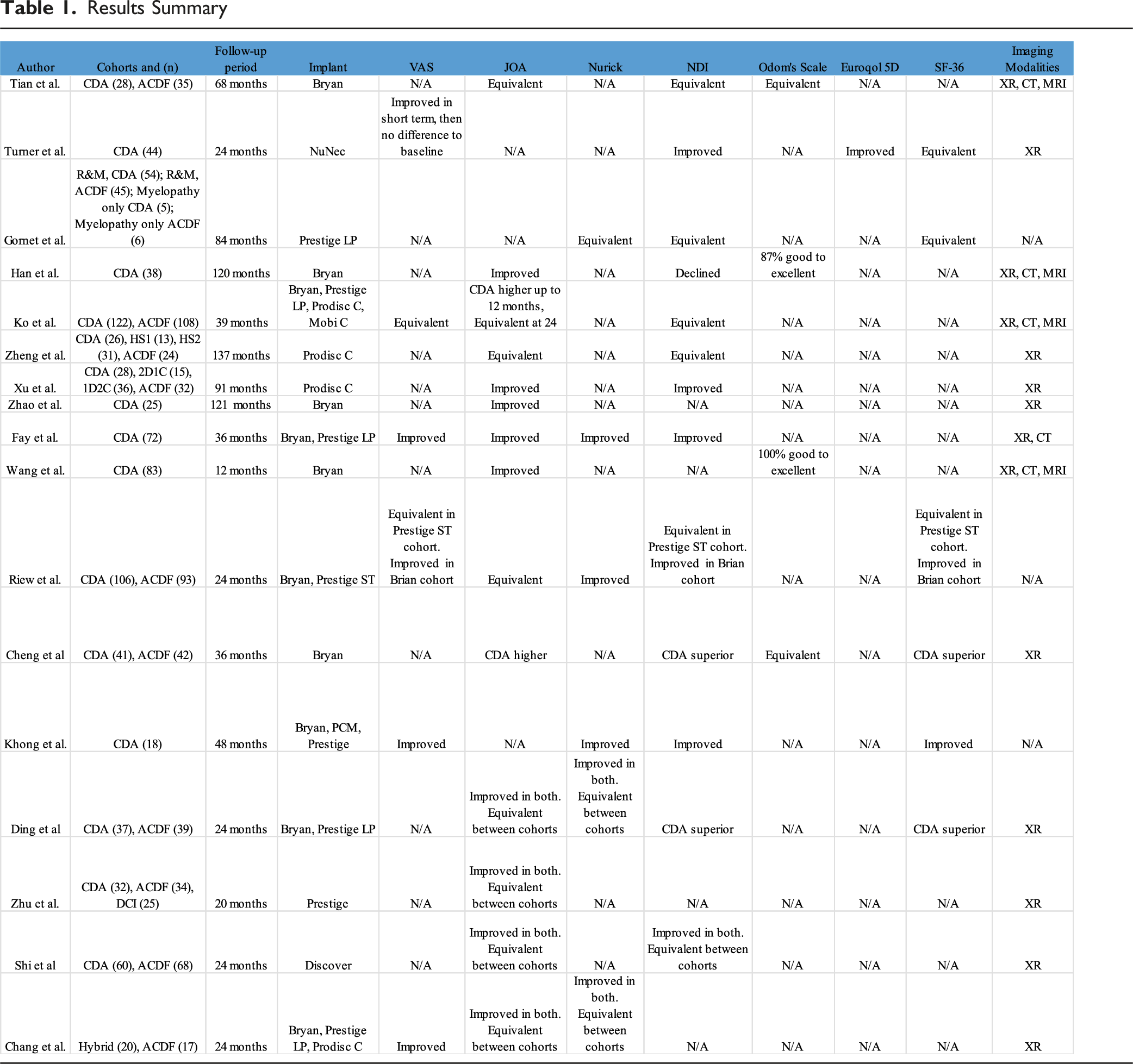
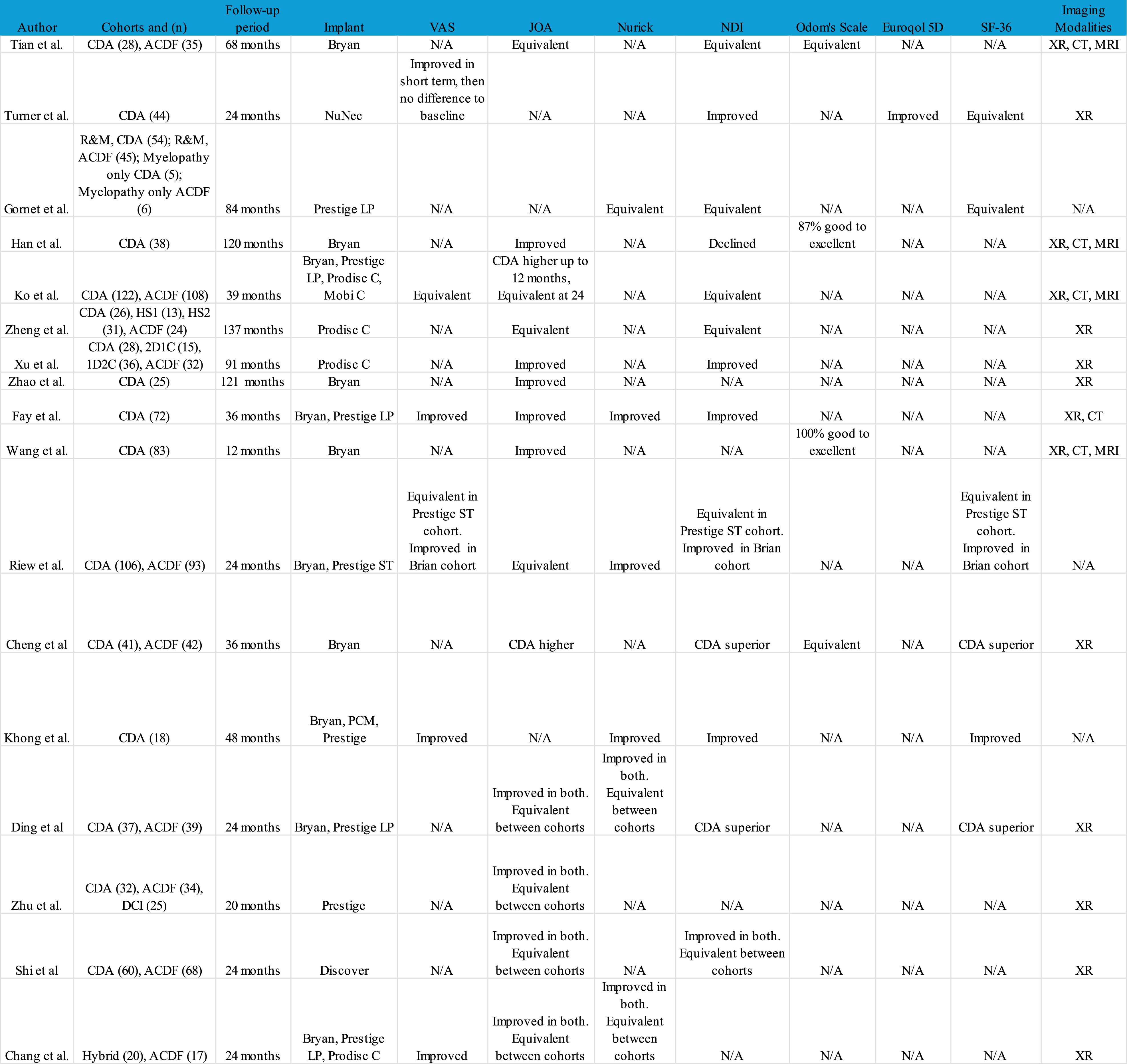
Results
Results Summary
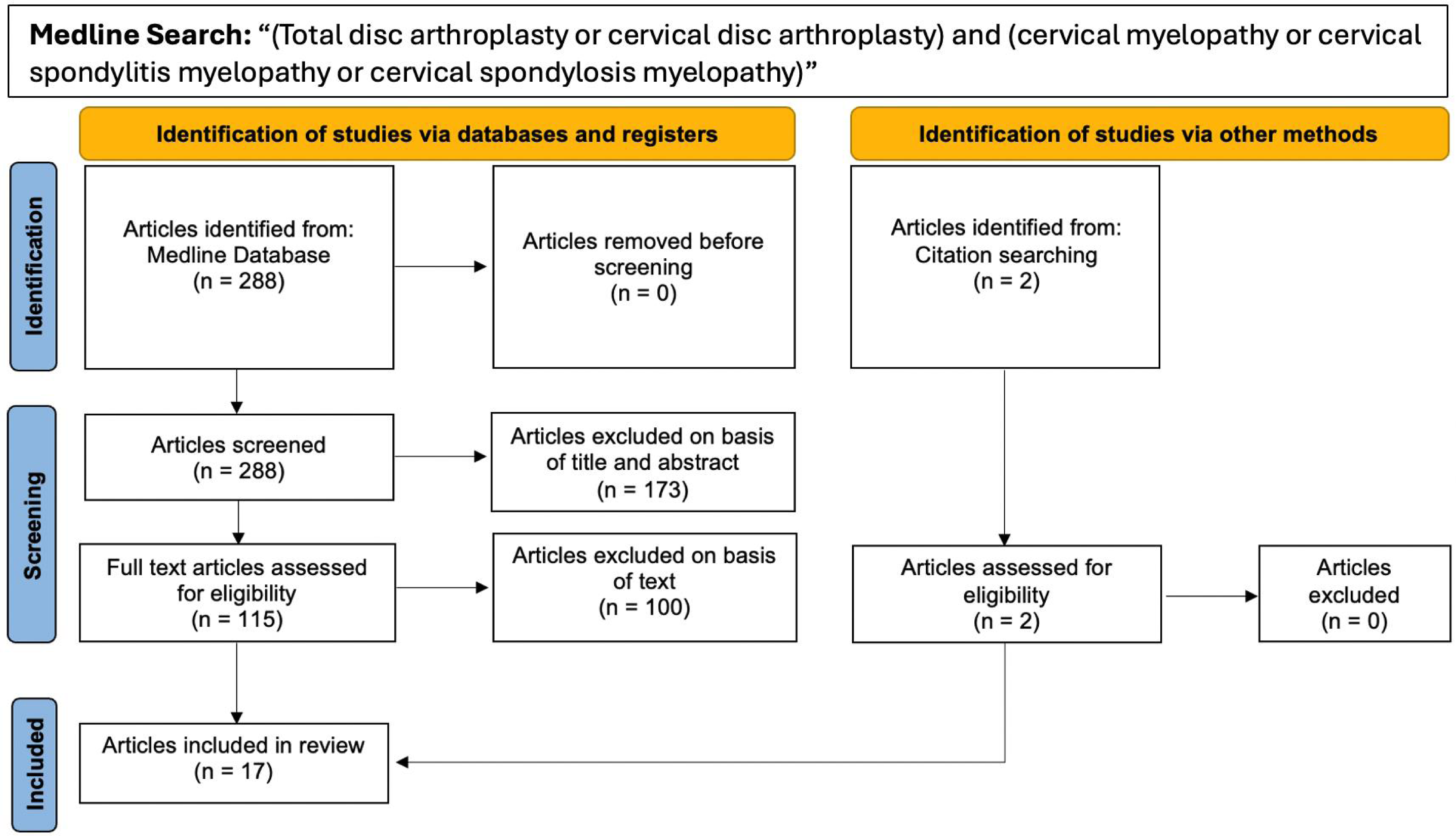
Prisma diagram
What is the Incidence and Predictors for Persistent Symptoms after Cervical Disc Arthroplasty in Patients with Myelopathy?
Several studies in this systematic review included patient reported outcomes (PROs), specifically the Japanese Orthopaedic Association (JOA) and Nurick scores to address the severity of cervical compressive myelopathy. Each of these investigations reported improvements in PROs and decrease in myelopathic symptoms after patients underwent cervical disc arthroplasty. Moreover, these studies have heterogeneity in device selection.
In terms of recurrence of symptoms or new neurologic symptoms, 3 studies reported this complication.3-5 Turner et al reported recurrence of symptoms in 2 of 44 (4.5%) patients, these patients underwent foraminotomy at their index level beyond 18 months of their initial surgery. 3 Zhao et al. reported uncoforaminal stenosis due to severe degeneration of the uncinate process and heterotopic ossification (HO) in 2 of 25 (8%) patients, 4 The authors addressed this by removing the uncovertebral joint and HO mass with maintenance of their original CDA implant. 4 Khong et al. reported worsening of myelopathy in 2 of 18 (11.1%) patients. 5 One of the patients had ongoing cord compression at the index level which was addressed with a corpectomy. The other patient had worsening myelopathy from a posterior disc-osteophyte complex and this was addressed with revision to ACDF at the index level. 5 The etiology of the new neurological symptoms or continued preoperative symptoms are similar in all studies as the authors report continued cervical degeneration resulting in osteophytosis or HO as the cause of compression. In case reports, involving a few patients, recurrence of myelopathy has been reported due to dislocation or posterior migration of the prosthesis into the spinal canal causing cord compression.6-8
Ko et al. utilized MRI to measure the length of increased intramedullary signal intensity (IISI). 9 They found that in both the CDA cohort and the ACDF cohort that there was a decrease in the IISI (1.23 cm to 0.28 cm in CDA cohort; 1.07 cm to 0.37 cm in ACDF cohort) which correlated with improvements of JOA scores (12 to 14 in CDA cohort; 11 to 12.5 in ACDF cohort).
Do Clinical Outcomes Differ Between Patients Undergoing Cervical Disc Arthroplasty and Anterior Cervical Discectomy and Fusion in the Setting of Myelopathy?
In total, 11 articles were deemed relevant to question 2 after full-text review; ten articles were randomized controlled studies and 1 article was a prospective non-randomized comparative study.
The minimum follow-up period for each of these 11 studies ranged from 10 months to 10 years, with a mean minimum follow-up length of 54 months. Nine of the studies included procedures performed by only 1 surgeon while 2 studies included procedures performed at multiple centers. The cervical disc arthroplasty implants utilized in these studies included the Bryan (Medtronic), Prestige LP (Medtronic), prodisc C (Centinel Spine), Mobi-C (Highridge Medical), Prestige-ST (Medtronic), and DISCOVER (Depuy). Specific outcomes included range of motion (ROM), Japanese Orthopaedic Association score (JOA), Nurick Classification, Visual Analogue Scale (VAS), Neck Disability Index (NDI), Short Form-36 (SF-36), Odom Criteria, radiographic outcomes, as well as assorted complications including secondary surgeries, adjacent segment disease (ASD), heterotopic ossification (HO), CSF leak, and dysphagia.
Functional Outcomes/Pain Scores
Regarding postoperative measures of cervical myelopathy, ten studies analyzed JOA scores,9-19 while 4 studies reported Nurick scores (Table 1).14,15,17,18 Of the ten studies analyzing JOA scores, only Cheng et al 13 found that CDA patients experienced superior improvement in JOA scores compared to ACDF patients (JOA 15.2 in CDA, JOA 14.4 in ACDF, P = 0.016) , whereas the remaining 9 studies found equivalent improvements in JOA between CDA and ACDF cohorts. Of the 4 studies analyzing Nurick Classifications, each found equivalent improvements between CDA and ACDF cohorts.
Three included studies reported changes in Visual Analog Scores (VAS) in patients undergoing cervical arthroplasty or arthrodesis. Riew et al noted that patients with the Bryan CDA prosthesis demonstrated greater improvements in pain compared to patients who underwent arthrodesis 18 while Ko and Chang found equivalent improvements in pain in both cohorts.9,15 Ten studies9-14,16-19 analyzed postoperative NDI. Cheng and Ding reported better postoperative NDI improvement in patients who underwent arthroplasty as opposed to arthrodesis.13,14 The remaining studies reported equivalent improvement in postoperative NDI between CDA and ACDF patients.
Gornet et al, Riew et al, Cheng et al, and Ding et al compared changes in SF-36 scores in arthroplasty and arthrodesis patients. Cheng et al and Ding et al reported improved SF-36 measures in the CDA cohort compared to the ACDF cohort.13,14 Riew et al. demonstrated equivalent improvement in postoperative SF-36 measures for patients undergoing arthroplasty with a Prestige-ST implant compared to an ACDF cohort. 18 In the same study, the authors noted improved SF-36 measures in the Bryan CDA cohort compared to the ACDF cohort. 18 Gornet et al. reported equivalent postoperative improvement in SF-36 measures between their CDA and ACDF cohorts. 17
Range of Motion/Alignment
Nine out of eleven studies compared postoperative flexion-extension ROM between CDA and ACDF through the use of preoperative and postoperative radiographs (Table 1). All 9 studies reported maintained postoperative ROM in the CDA group but decreased postoperative ROM in the ACDF group at their respective follow-up.9-16 Ding et al, Zhu et al, and Cheng et al all reported greater ROM about the global cervical and segmental cervical regions when comparing CDA to ACDF patients (P < 0.05). Shi et al, Chang et al, Ko et al, and Tian et al reported greater ROM in the CDA vs ACDF patients about the segmental cervical regions only (P < 0.05). Zheng et al and Xu et al reported statistically significantly greater ROM for CDA vs ACDF patients about the global cervical region only (P < 0.05). Two out of the 9 studies did not analyze postoperative ROM as one of their outcome measures.17,18
Radiographic outcomes were analyzed in ten studies. Zheng et al and Xu et al both reported decreased postoperative cervical lordosis and T1 slope angle (defined as the angle formed by a perpendicular line extending from the center of the T1 endplate and a second line extending from the center of the T1 endplate to the upper aspect of the sternum) in the ACDF cohort compared to the CDA cohort (Table 1).11,12 Tian et al. found that CDA patients experienced better maintenance of preoperative alignment and lower incidence of ASD compared to ACDF patients. 10 Ko et al. reported improvements in intramedullary signal intensity between the CDA and ACDF cohorts. 9 Ding et al. reported anterior prosthesis migration in 3 out of 37 CDA patients. 14 Shi et al reported anterior migration in 10/60 patients receiving the DISCOVER CDA prosthesis (compared to 0/68 patients receiving ACDF, P = 0.000), some degree of HO formation in 8/60 CDA patients (4 with grade I, 3 grade II, 1 grade III) compared to 0/68 ACDF patients (P = 0.000), and subsidence in 2/60 DISCOVER CDA prosthesis patients (compared to 1/60 in the ACDF group, P = 0.600).
Complication Profile
Included studies point to an equivalent rate of postoperative complications in patients with myelopathy undergoing disc arthroplasty or arthrodesis. Shi et al. reported similar rates of dysphagia (10.0% in CDA, 10.3% in ACDF, P = 0.956) between the CDA and ACDF groups. 19 Ko et al. reported equivalent rates of postoperative complications between the CDA and ACDF cohorts, including dysphagia (2.46% in CDA, 4.63% in ACDF, P = 0.370) and CSF leak (0.82% in CDA, 0.93% in ACDF, P = 0.931). 9 Similarly, Ding et al reported reoperation rates of 3/37 patients in the CDA cohort and 1/39 patients in the ACDF cohort (P = 0.28). On the other hand, Gornet et al reported similar rates of secondary surgery between CDA and ACDF patients, but a statistically significant decrease in a composite measure of serious postoperative adverse events at the 7 year follow-up mark in the CDA cohort compared to the ACDF cohort (54.5% in CDA, 65.9% in ACDF, P = 0.019), with the composite measure including cancer, cardiac arrest, death, dysphagia/dysphonia, gastrointestinal complications, HO, infection, neck and/or arm pain, neurologic deficits, spinal events (as defined as a “spine-related diagnosis at any level of the spine, such as spondylosis, fusion, disk herniation, disk degeneration, facet joint syndrome, cord compression, vertebral compression fracture, kyphosis, spinal hemangioma, etc.”), respiratory complications, vascular complications, and wound complications. 17 The largest differences in postoperative adverse events at the 7 year follow-up mark included neck and/or arm pain (5.6% in CDA, 21.5% in ACDF, P < 0.001) and spinal event (12.0% in CDA, 31.7% in ACDF, P < 0.001).
Discussion
This study sought to identify whether cervical disc arthroplasty performed in patients with cervical myelopathy resulted in similar results as compared to ACDF. Evaluation of outcomes measures, radiographic analysis, and failure due to implant related complications is equivalent in comparing CDA to ACDF. From the literature available, the outcomes (to include neurologic patient reported outcomes (PROs)) in patients undergoing cervical disc arthroplasty are at least equal to those of ACDF.
Anterior surgical treatment of patients with cervical myelopathy in the setting of congenital stenosis has undergone considerate debate. Even after appropriate anterior decompression, there may be residual canal stenosis due to facet hypertrophy, ligamentous hypertrophy, and a small canal. With decompression in addition to long term stabilization of the spine as treatment goals, the literature is limited on the efficacy of anterior alone treatment. There is concern that CDA in this setting may result in persistent myelopathy due to the persistence of motion. The literature is particularly sparse in relation to this entity. Chang et al addressed this entity in their study on hybrid-CDA vs ACDF. The treatment groups consisted of patients who either underwent a 3-level ACDF or a 2-level CDA plus 1-level ACDF. Evaluating their clinical assessment, both groups improved in VAS for neck and arm pain, JOA scores, and Nurick grades. At a mean follow up of 2 years, none of the patients experienced device failure or need for revision surgery related to device related complications. None of the patients in their series experienced worsening myelopathic symptoms. Their study suggests that treatment of cervical myelopathy via anterior based surgery (CDA or ACDF) in the setting of congenital stenosis can be successful. Additional studies are needed to make this recommendation.
This study has several limitations. As identified from the bias analysis, the majority of the studies which met inclusion criteria have at least moderate bias. There are very few randomized controlled trials comparing ACDF to CDA in the setting of myelopathy. Additional randomized controlled trials including only those patients with myelopathy would assist in allowing firm conclusion to be made. The heterogeneity of implants in addition makes it difficult to draw firm conclusions. Not all implants are FDA approved for 2 level pathology, suggesting that there are implant related differences that may affect outcomes. Despite these limitations, the available literature suggest that the treatment of cervical myelopathy in the absence of congenital stenosis is safe and efficacious, with similar outcomes to ACDF.
We believe performing a meta-analysis on the data obtained would have strengthened the findings of this study. A meta-analysis requires a systematic approach to data collection, ensuring that studies included are sufficiently homogeneous in terms of patient populations, interventions, outcome measures, and follow-up periods. This process involves defining strict inclusion and exclusion criteria, conducting a comprehensive literature search, extracting relevant data, and applying statistical methods to synthesize results. Consistency in outcome reporting is crucial to allow for meaningful comparisons, as is standardization in study methodologies to minimize bias. Unfortunately, based on the data we collected, we were unable to conduct a meta-analysis due to the significant heterogeneity in outcome measures and follow-up periods across the included studies. The variability in reported metrics and differing time points for assessment prevent meaningful statistical aggregation, increasing the risk of misleading conclusions.
The cause of symptoms in patients with degenerative cervical myelopathy deserves considerable attention. In many of the studies identified and evaluated, patients with ossification of the posterior longitudinal ligament were excluded. Those with evidence of cervical instability were also excluded. A minority of studies did not discuss their exclusion criteria. Due to the pathogenesis of OPLL, progression is more likely with an arthroplasty procedure, making a fusion procedure a more suitable option when considering an anterior based approach. It is also generally recommended that a fusion procedure be performed in the setting of cervical instability as opposed to an arthroplasty procedure. Additional caution based on the literature includes patients with osteoporosis, inflammatory spondyloarthropathy, or severe systemic disease.
Conclusion
Based on the available literature, we conclude that the outcomes in patients undergoing cervical disc arthroplasty appear to be equal to those of ACDF. In evaluating outcomes measures, radiographic analysis, and failure due to implant related complications, CDA is equivalent to ACDF in the treatment of DCM. From the literature available, the outcomes in patients undergoing cervical disc arthroplasty are at least equal to those of ACDF.
Footnotes
ORCID iDs
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international spine experts, and AO Spine North America. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization based in Davos, Switzerland.