
Abstract
Study Design
Systematic Review
Objectives
To conduct a meta-analysis on the survivorship of commonly performed cervical spine procedures to develop survival function curves for (i) second surgery at any cervical level, and (ii) adjacent level surgery.
Methods
A systematic review of was conducted following PRISMA guidelines. Articles with cohorts of greater than 20 patients followed for a minimum of 36 months and with available survival data were included. Procedures included were anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty (ADR), laminoplasty (LAMP), and posterior laminectomy and fusion (PDIF). Reconstructed individual patient data were pooled across studies using parametric Bayesian survival meta-regression.
Results
Of 1829 initial titles, 16 citations were included for analysis. 73 811 patients were included in the second surgery analysis and 2858 patients in the adjacent level surgery analysis. We fit a Log normal accelerated failure time model to the second surgery data and a Gompertz proportional hazards model to the adjacent level surgery data. Relative to ACDF, the risk of second surgery was higher with ADR and PDIF with acceleration factors 1.73 (95% CrI: 1.04, 2.80) and 1.35 (95% CrI: 1.25, 1.46) respectively. Relative to ACDF, the risk of second surgery was lower with LAMP with deceleration factor .06 (95% CrI: .05, .07). ADR decreased the risk of adjacent level surgery with hazard ratio .43 (95% CrI: .33, .55).
Conclusions
In cases of clinical equipoise between fusion procedures, our analysis suggests superior survivorship with anterior procedures. For all procedures, laminoplasty demonstrated superior survivorship.
Keywords
Introduction
Approximately 150 000 American adults undergo cervical spine surgery each year.1,2 This represents a significant financial burden, with direct hospital costs ranging between $5000 and $30 000 depending on procedure and jurisdiction. 3 As cervical spine surgery utilization has increased 206% between 1992 and 2005,4,5 these procedures represent a prime target to optimize value in spine care. 6
An estimated 30-50% of adults will experience neck pain in any given year, 7 and 50-80% of these individuals will go on to develop chronic symptoms. 8 Though conservative care is the mainstay of treatment, 9 surgery does have a role in the treatment of cervical radiculopathy, 10 cervical myelopathy, 11 and cervical deformity. 11 However, there is significant variability in surgical approaches to the cervical spine, particularly in cervical myelopathy, where in approximately 50% of cases surgeons feel that there is equipoise in the surgical approach (anterior, posterior, vs both), number of levels to decompress, need for fusion, and need for fixation. 12
Given that surgeons regard a variety of surgeries as equivalent in many cases, other factors should be considered in decision-making. Durability of the chosen procedure is 1 such consideration. It is important to note that while the rate of primary cervical surgeries is increasing, rates of revision procedures are accelerating at a faster rate. 13 Revision procedures are more expensive, 14 carry a greater risk of complications, 15 and are less durable than primary procedures. 16 Granular data on future probabilities of revision surgery in treatment discussions could enhance patient counselling by surgeons. 17 Previously published systematic reviews and meta-analysis have been limited to risk factors for revision rather than actual probabilities of revision.18,19
In this paper we conduct the first meta-analysis of survival probabilities for commonly performed cervical spine procedures. We compute summary survival curves for (i) second surgery at the index level, and (ii) adjacent level surgery, which will allow surgeons to calculate the probability of revision surgery at any time-point of interest.
Methods
A systematic review was conducted in accordance with the Cochrane Prognosis Methods Group as well as the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 20 An electronic librarian-assisted search of Ovid MEDLINE, Ovid EMBASE, and CENTRAL from inception to February 22 2021 (Appendix 1) was performed. A validated DCM search filter with 100% sensitivity in MEDLINE was utilized and adapted for EMBASE.21,22 The highly sensitive Irvin filter, modified for occurrence of an event rather than death, was combined with the DCM filter to restrict results to DCM prognostic studies in MEDLINE and EMBASE.23,24 CENTRAL was searched using the strategy used in the Cochrane review for DCM treatment without the requirement for surgical treatment. 25 Reference lists of included papers were screened for additional manuscripts to ensure search completion.
Eligibility Criteria and Screening
Eligible studies included those written in English language with record of survivorship analysis for adult patients with degenerative cervical pathology treated with primary (not revision) surgery. We considered second surgery (at any cervical level, Analysis 1) and adjacent level surgery (Analysis 2) as survival endpoints. Both randomized controlled and cohort studies were eligible for inclusion. We required that a cohort of at least 20 patients be followed for at least 36 months. We required that survival be reported for at least 2 homogenous treatment group: (i) anterior cervical discectomy and fusion (ACDF), (ii) artificial disc replacement (ADR), (iii) laminoplasty (LAMP), or (iv) laminectomy and fusion, ie posterior decompression and instrumented fusion (PDIF). We required that studies report at least 2 groups to avoid bias introduced by single-arm studies. 26 We excluded cohorts focusing on a special population alone (eg smokers, patients on dialysis, or concomitant deformity) or cohorts undergoing a combination of procedures.
All titles and abstracts were independently screened for eligibility by 2 reviewers using the online platform Covidence (Melbourne, Australia). All discrepancies were resolved by consensus amongst authors. Duplicate articles were manually excluded. Two reviewers independently reviewed the full text of all studies identified by title and abstract screening to determine final eligibility.
Data Extraction and Quality Assessment
Two reviewers independently extracted study data using the CHARMS checklist and assessed the risk of bias using the QUIPS tool modified for overall prognosis studies. 27 All discrepancies were resolved by consensus amongst authors. A standardized electronic data collection form was used. Our primary outcome was probability of treatment failure reported with a survival curve.
Images of survival curves were saved from included studies and survival probabilities were extracted from survival curves using the computer program WebPlotDigitizer. 28
Statistical Analysis
We used the Guyot algorithm to simulate the individual patient data from published survival curves using the statistical programming language R.29,30 With the simulated individual patient data, we pooled survival curves across studies using a fixed effects approach of individual patient data meta-analysis. A parametric survival curve was fit to the pooled data using the framework outlined by Ishak et al. 31 We considered exponential, Weibull, Gompertz, Log-logistic, and Log-normal probability density functions in the model building exercise. Poorly fitting probability density functions were excluded using graphical exploratory analysis. Next, the probability density function with the lowest Akaike information criterion (AIC) and adequate fit of the pooled survival curve was used for further analysis.
Data from survival curves were used in a Bayesian meta-analysis using the statistical programming language R and the Bayesian modelling language Stan using the best fitting probability density function.30,32 Non-informative prior distributions were used. 33 Bayesian analysis was implemented using previously described techniques for meta-analysis. 34 We included treatment group as a categorical variable, and therefore only considered treatment group for which at least 2 survival curves were available. We assessed for heterogeneity through visual inspection of the published survival curves in relation to each other.
Results
1829 studies were identified, and after excluding duplicates, 1456 remained. Through title and abstract screening, 1303 citations were excluded, resulting in 153 full-text citations for review. 137 citations were excluded yielding 16 citations that were included in our analysis (Figure 1).35‐40 For second surgery, 2 citations reported on the same dataset, therefore we considered 8 unique studies. 41‐49 For adjacent level surgery, 2 sets of citations reported on the same dataset, therefore we considered 5 unique studies.50‐56 Study flow diagram.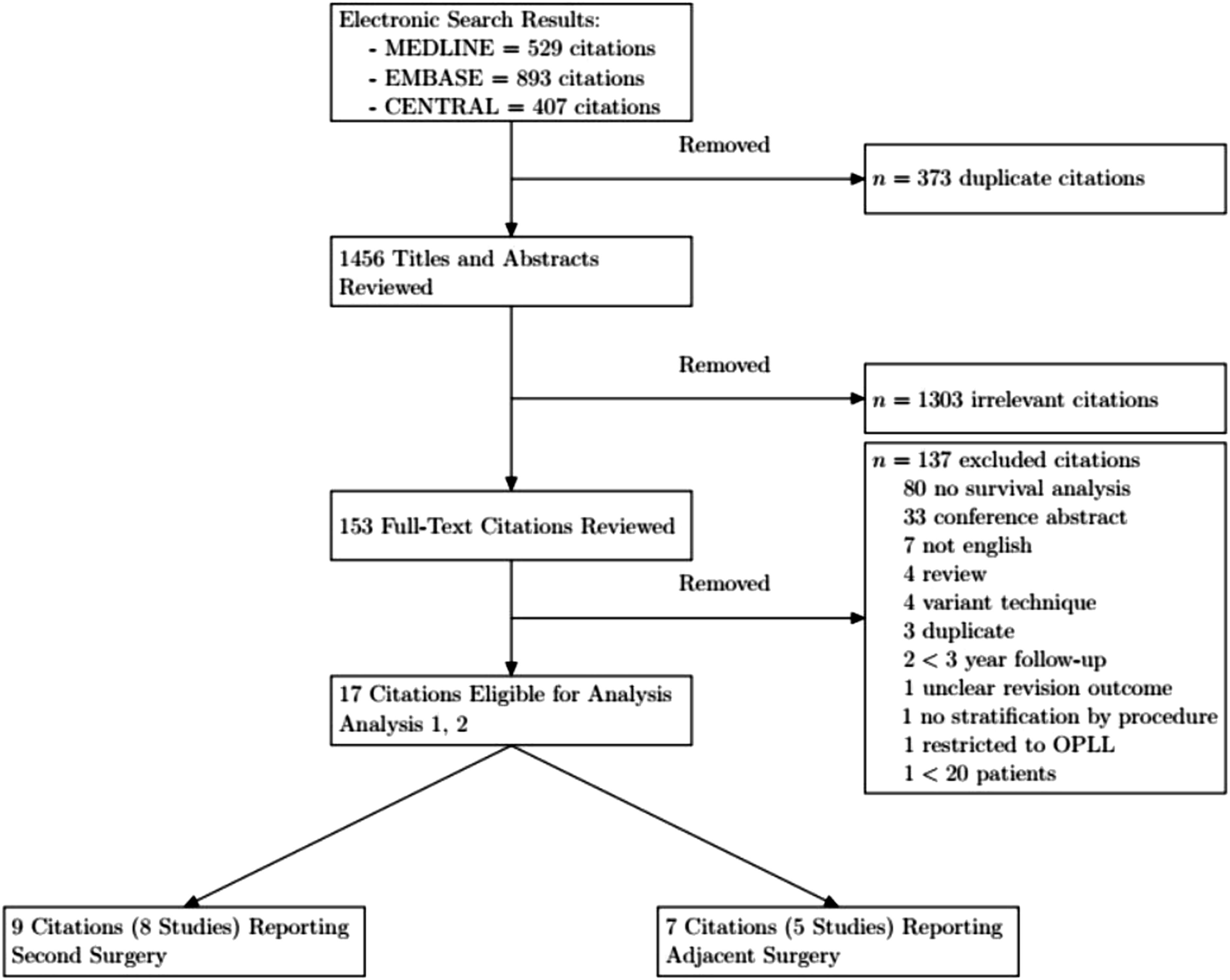
Characteristics of Studies Included in Second Surgery Analysis.
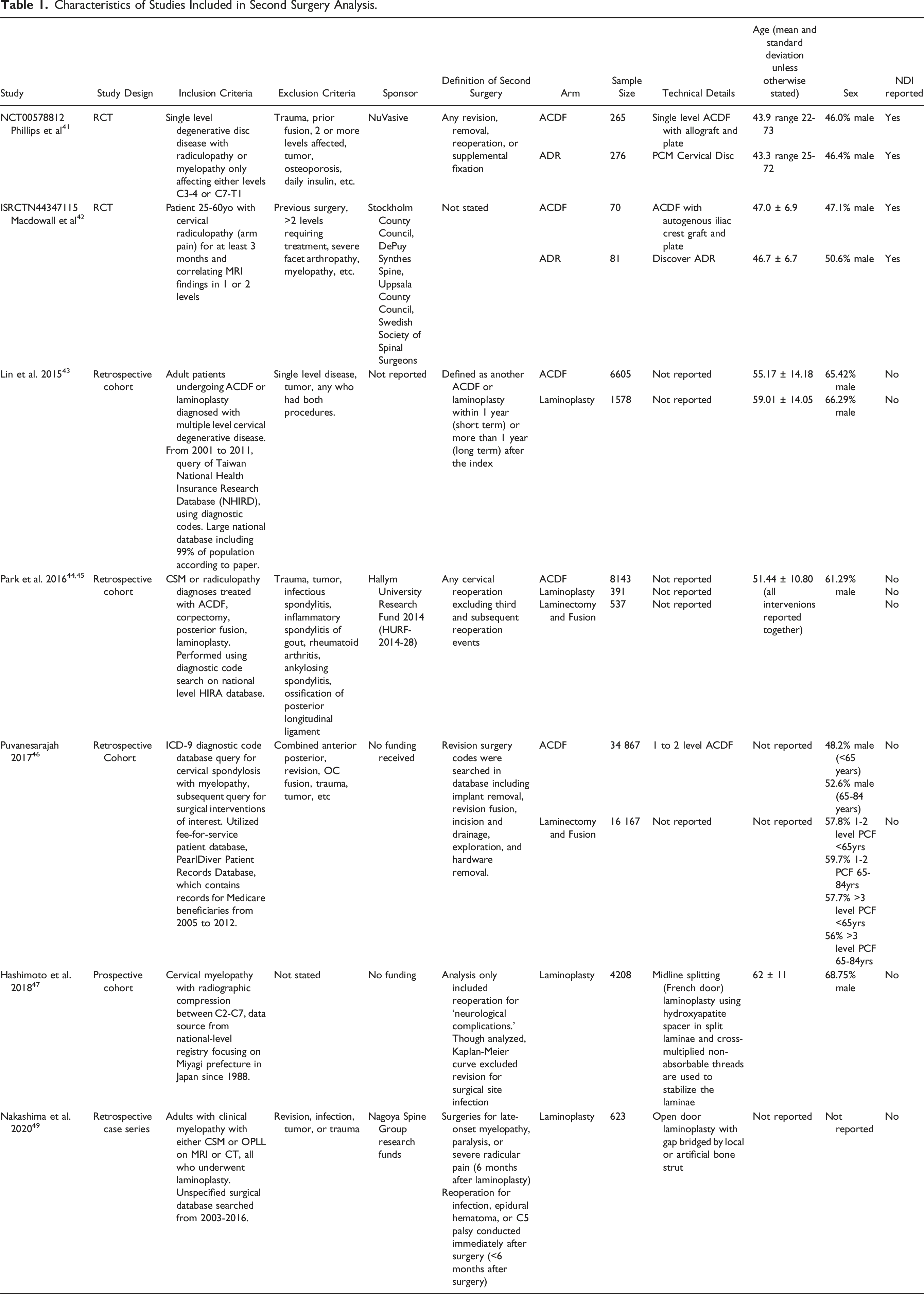
Analysis #1 considered 2 randomized controlled trials,41,42 3 large database studies,43‐46 and 2 single-center retrospective cohort studies.47‐49 At least 2 studies reported data for ACDF, ADR, LAMP, and PDIF. Overall, 49 950 patients underwent anterior cervical discectomy and fusion (ACDF), 357 underwent artificial disc replacement (ADR), 6800 laminoplasty, and 16 704 posterior laminectomy and instrumented fusion. One study limited patients to a diagnosis of radiculopathy, 42 2 included patients with either radiculopathy or myelopathy,41,44 3 included only patients with myelopathy,46,47,49 and 1 did not specify the clinical diagnosis, stating only that patients had multilevel cervical degenerative disease. 43 2 studies, both of which were RCTs comparing ACDF to ADR, included only single level disease.41,42 Two studies, both large database studies not including ADR, excluded single level disease, including only multi-level surgery.43,44 The remainder of studies in our second surgery analysis did not specify the number of operative levels.
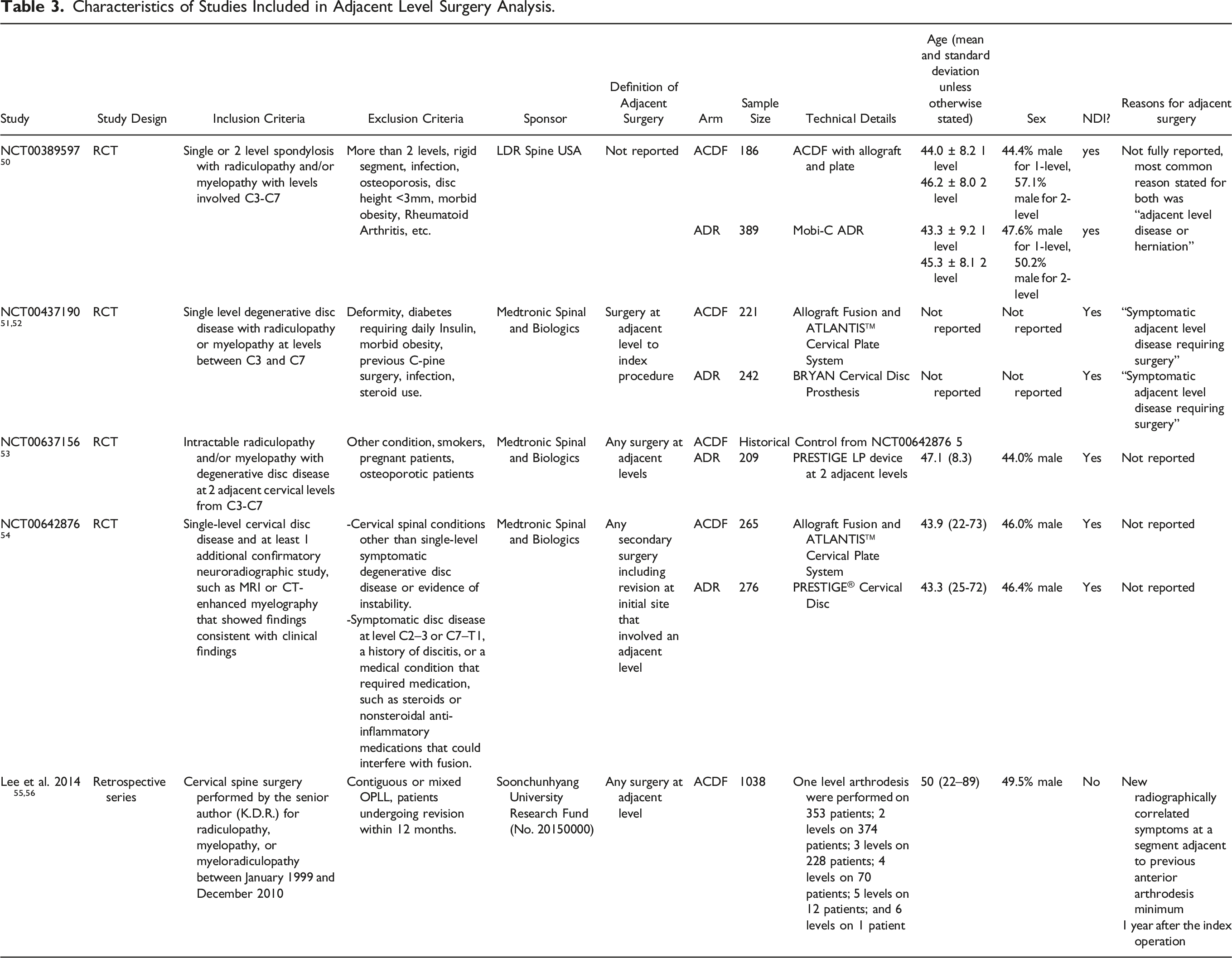
Analysis #2 considered 4 randomized controlled trials,50‐54 and 1 single-center retrospective cohort study.55,56 Only 1 study reported survival curves for LAMP and PDIF, 55 therefore Analysis #2 only considered ACDF and ADR. The ADR data from Lee et al was excluded because hybrid ACDF-ADRs were included in their data. 55 All of these studies directly compared ACDF to ADR. Overall, 1710 patients underwent ACDF and 1148 patients underwent ADR. All studies included patients with either diagnoses of radiculopathy or myelopathy with radiographic evidence of degenerative disc disease. Two studies focused on single level degenerative disease51,52,54, 1 on 2 adjacent level disease, 53 and 1 on either single or 2 level disease. 50 One study did not restrict number of levels operated in the index procedure. 56
Risk of Bias Assessment for Included Studies.
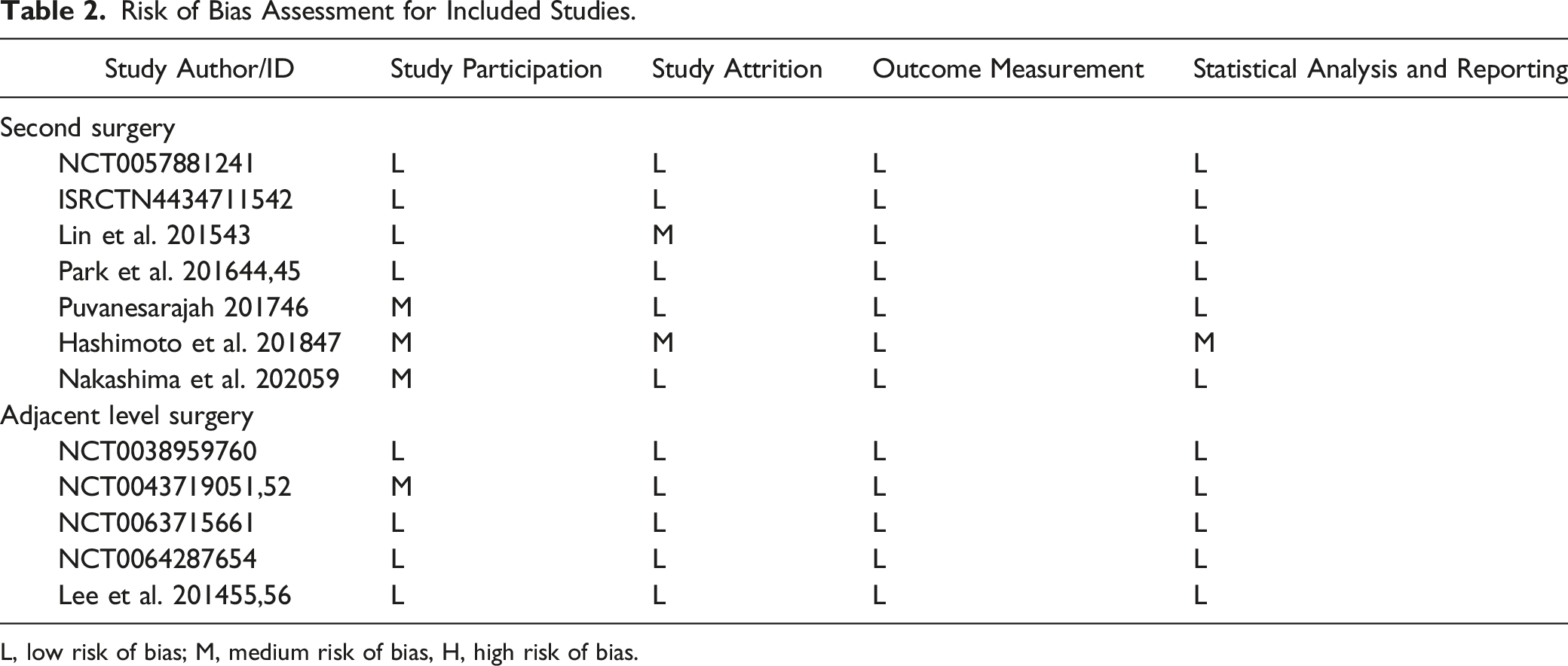
L, low risk of bias; M, medium risk of bias, H, high risk of bias.
Characteristics of Studies Included in Adjacent Level Surgery Analysis.
Individual study survival results for second surgery and adjacent level surgery are shown in Figures 2 and 3 respectively. In Analysis #1 (second surgery), we noted little heterogeneity in survival curves reported by studies on ACDF, LAMP and PDIF. There was substantial heterogeneity between the 2 studies on ADR.41,42 ISRCTN44347115
42
included patients undergoing 1 or two-level ADR, whereas NCT00578812
41
was restricted to single-level ADR. We also note ISRCTN44347115
42
recruited a smaller sample than NCT00578812
41
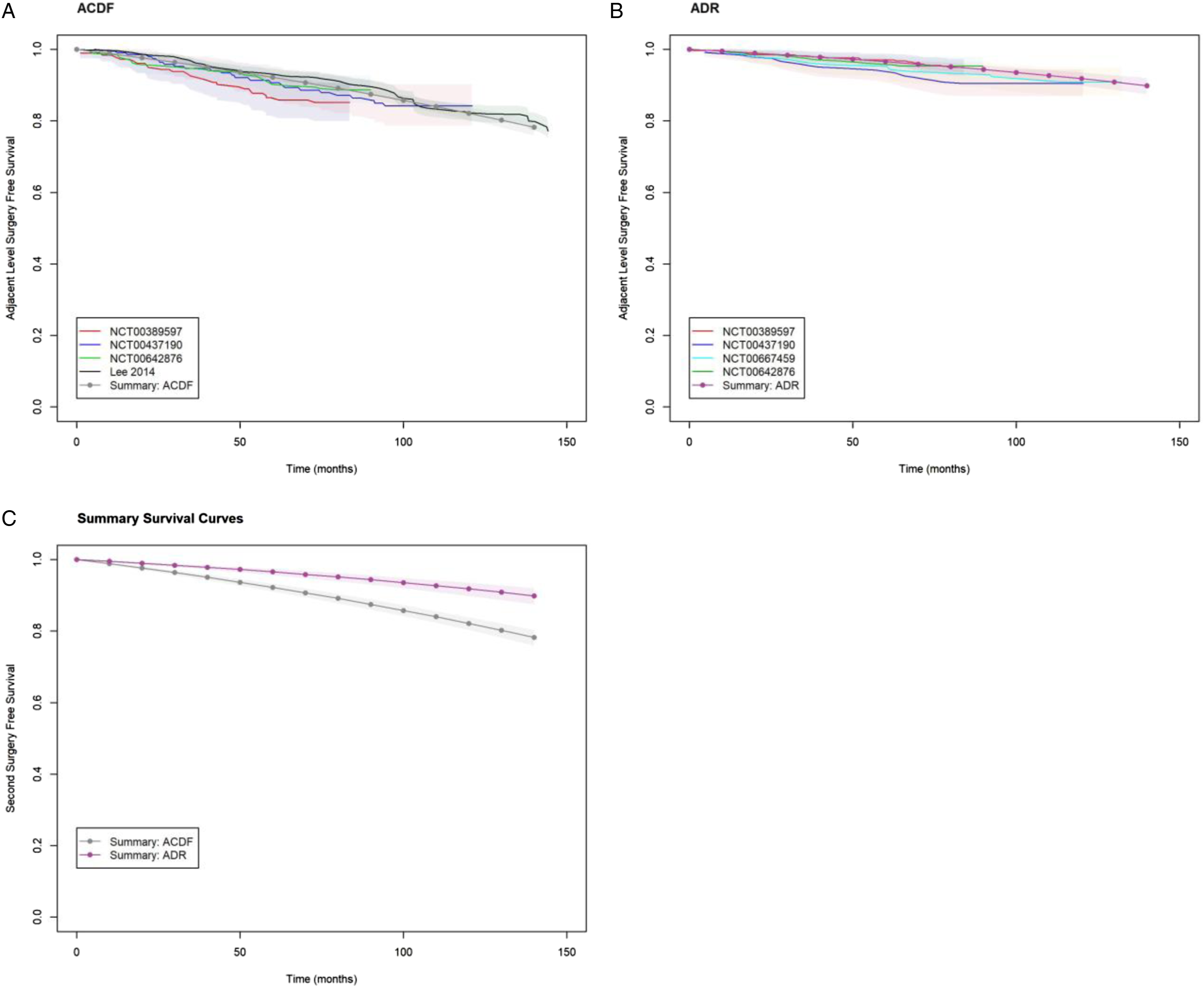
resulting in wide confidence intervals for the former which overlap with the latter. In Analysis #2 (adjacent level surgery), we noted consistent results between studies for ACDF and ADR. Individual study survival curves, and parametric summary survival curve for second surgery. Individual study survival curves, and parametric summary survival curve for adjacent level surgery.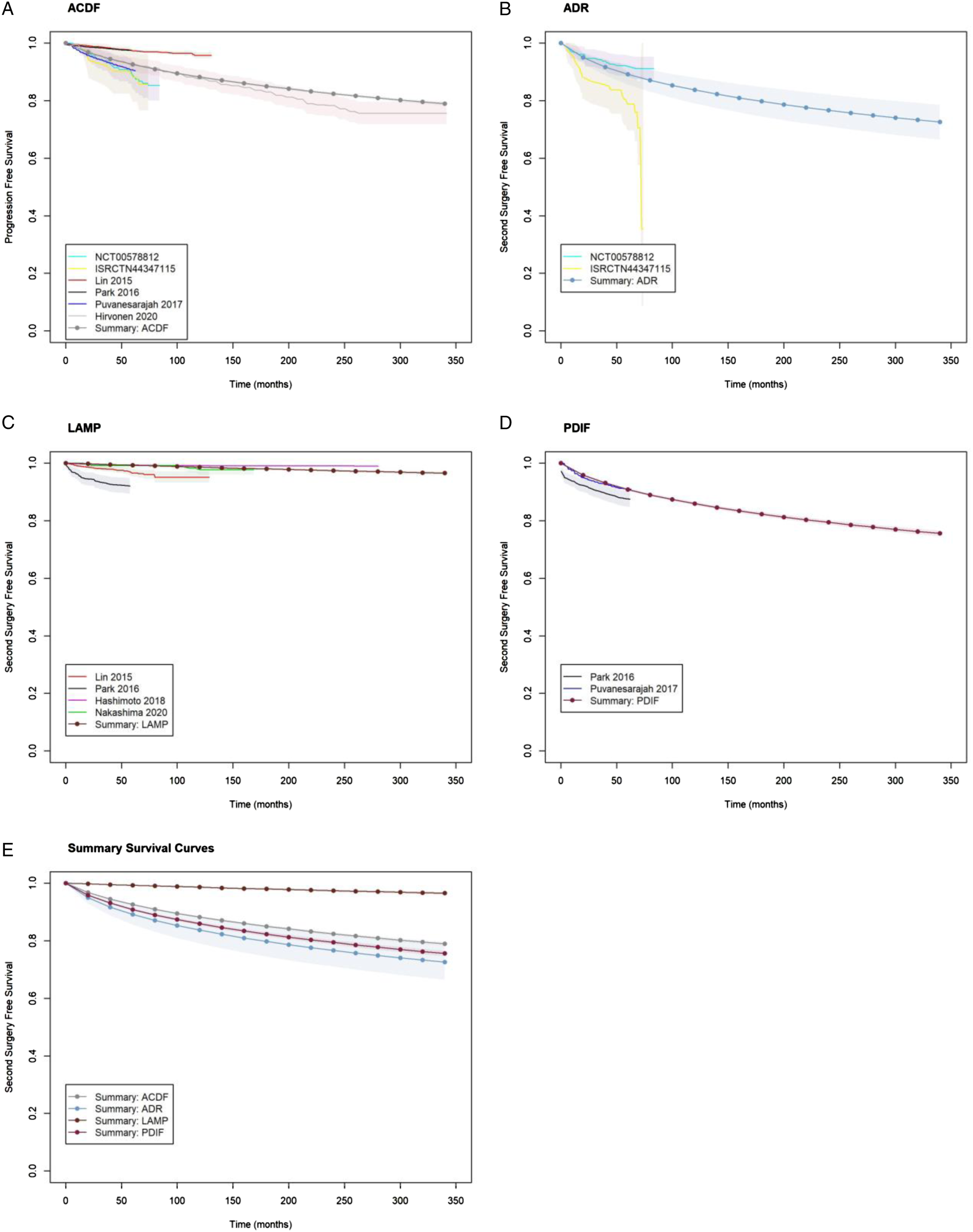
Exploratory plots for the appropriate probability density function for the pooled Kaplan-Meier data are shown in Figure A1. The exponential, Weibull and Log-logistic distributions showed a lack of linearity at early and late times and thus poor for the pooled data. Based on AIC, the Gompertz model provided the best fit, and further supported by the similarity between observed and predicted survival probabilities shown in Figure A2.
Second Surgery Free Survival Estimates from Meta-Regression.
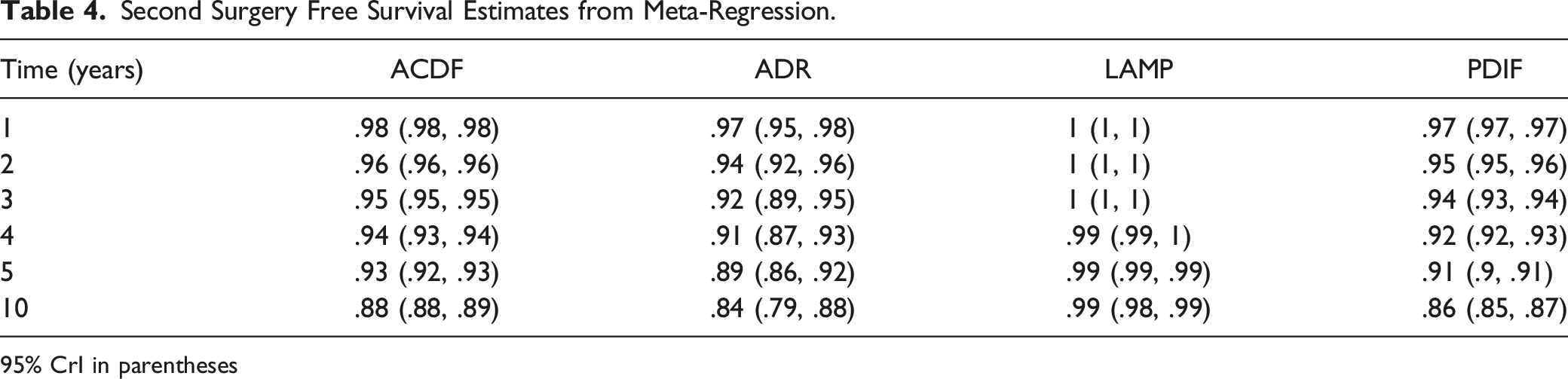
95% CrI in parentheses
Adjacent-Level Surgery Free Survival Estimates from Meta-Regression.
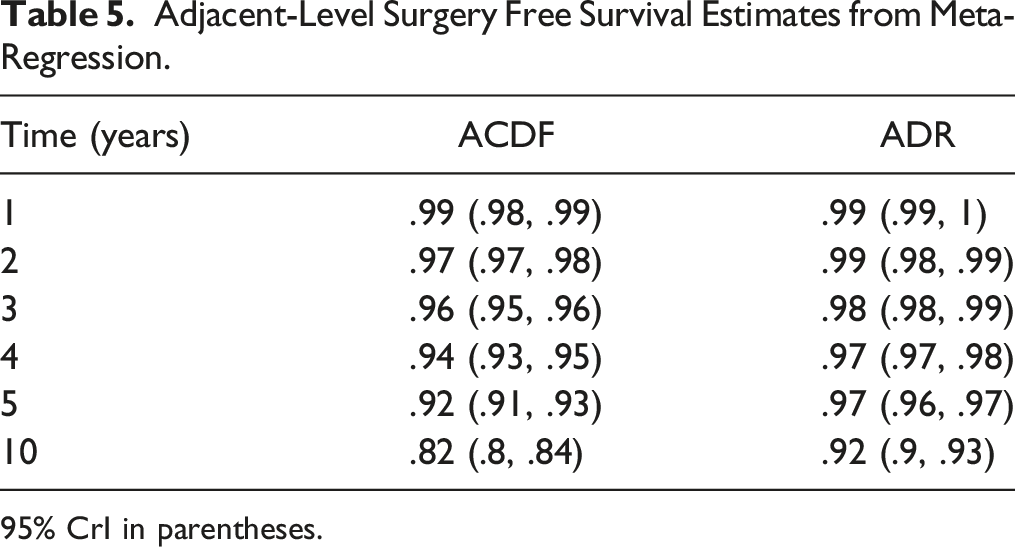
95% CrI in parentheses.
Discussion
This systematic review and meta-analysis is the first quantitative synthesis of published data on the long-term survivorship of the most commonly performed surgeries for degenerative cervical spine pathologies.
The parameteric summary survival curve for second surgery is shown in Figure 2 (log-normal) and for adjacent level surgery in Figure 3 (Gompertz). Our analysis shows a higher risk of second surgery for ADR and PDIF (acceleration factors 1.73 (95% CrI: 1.04, 2.80) and 1.35 (95% CrI: 1.25, 1.46) respectively), and a lower risk of second surgery for LAMP relative to ACDF (.06 (95% CrI: .05, .07)). The increased risk of second surgery for ADR and PDIF did not translate into significantly different survival probabilities suggesting a lack of clinical significance (Table 4). While our analysis showed that the risk of adjacent level surgery was lower for ADR relative ACDF with hazard ratio .43 (95% CrI: .33, .55).
Zhong et al. have published the only other meta-analysis on the risk of second surgery in ACDF vs ADR incorporating data from 12 RCTs. 56 They conducted a random-effects meta-analysis of pooled second surgery rates at various follow-up times. Notably 50% of studies only followed patients to 2 years. They found that the risk of second surgery was lower with ADR compared to ACDF (Risk Ratio .54 (95%CI: .36-.80). Zhong et al.’s findings differ from ours that ADR carries a higher risk of surgery with an acceleration factor 1.35 (95% CrI: 1.25, 1.46), albeit with no difference in actual survivorship (Figure 2E). This discrepancy stems from the fact that, in the Zhong et al. meta-analysis, the pooled second surgery rate for ACDF was 11.6% which contrasts with our findings of a 4% second surgery rate at 2-years (Table 4). It is interesting that second surgery rates for ADR are similar in our and Zhong et al.’s meta-analysis (6% and 6.1% respectively). There are several potential reasons for differences in estimates of in ACDF second surgery rates. First, 75% of studies in the Zhong meta-analysis were industry funded, whereas only 50% were industry- funded in our ACDF vs ADR comparisons for second surgery. Second, the majority of studies in the Zhong et al meta-analysis reported index and adjacent level surgery separately, and second surgery was simply calculated as the sum of both event rates. This approach assumes that second and index level surgery are mutually exclusive. Such an assumption will overestimate second surgery rates if patients undergo both an index and adjacent level surgery in the same second surgery. Third, Zhong et al. were not able to account for observation time and censoring in their analyses. Our meta-analysis of actual second surgery time-to-event data addresses the methodological limitations of the Zhong et al meta-analysis.
Our findings agree with previously published meta-analyses on the risk of adjacent-level surgery. Deng et al. conducted a meta-analysis on the risk of adjacent-level surgery in ACDF vs ADR with 8 randomized controlled trials. 19 Their finding that ADR carried a lower risk of adjacent level surgery at 4-5 years, 7 years, and 9-10 years of follow-up agree with our findings. Badhiwala et al. conducted a meta-analysis on the risk of adjacent level surgery ACDF vs ADR. 57 They included 11 RCTs reporting with follow-up to 2 years, 4 years, 5 years, or 7 years. They report 5-year adjacent level surgery free survival rates of 91.9 (95% CI: 88.9-94.1) and 97.1 (95% CI: 95.2-98.2) for ACDF and ADR respectively which closely agree with our estimates shown in Table 5.
Our study incorporates an important methodological advancements over Zhong et al.’s, Deng et al.’s and Bhadiwala et al.’s meta-analyses.18,19,57 The analytical approach used in these papers was restricted to fixed follow-up times. We instead digitized published survival curves and reconstructed individual patient data using recently developed algorithms. This is a less restrictive requirement and allowed us to include the totality of longitudinal data in 1 meta-analysis. This approach allowed us to include very large sample sizes in our paper: 73 811 patients for second surgery, and 2858 patients for adjacent level surgery and therefore confidence intervals around summary survival curves are relatively precise.
Several limitations are important to consider. First, we are unaware of any sample size calculations for survival meta-regression and therefore are unable to formally evaluate the power of our analysis. A commonly cited rule-of-thumb that linear regression requires 10 to 20 subjects per variable. 58 In Analysis #1 (second surgery), we used 3 variables (surgery as a categorical variable) with a minimum of 759 observations for the LAMP variable. In Analysis #2 (adjacent level surgery), we used 1 variable (surgery as a categorical variable) with a minimum of 357 observations for the ADR variable. Therefore, we feel our analysis is statistically viable. Second, inclusion/exclusion criteria were variable across studies. Some studies included patients with myelopathy, while this was an exclusion criterion in others. In particular, trials were restricted to 1 or 2 operative levels, while observational studies considered greater levels. Despite this methodological heterogeneity, we noted a low level of heterogeneity.
Lastly, we cannot report demographic homogeneity between groups. It is critical to note that the main purpose of this study is to produce individual survival curves for each of these procedures and that this is not a direct comparative study. Although the incidence of different pathologies is not specifically reported, we suspect that the 2 papers producing the bulk of the laminoplasty patients in our study contained more patients with OPLL, as this was not an exclusion criterion for them, and rates of OPLL are known to be higher in East Asia, with both papers focussing on a Japanese population. However, to our knowledge, there is no literature to suggest that OPLL is protective against reoperation. In fact, large cohorts such as those produced by Fujiwara et al. suggest higher rates of complication and reoperation in patients with OPLL compared to Cervical Spondylotic Myelopathy (CSM) 60 . Additionally, laminoplasty is usually preferred for multi-level disease, as opposed to single level disease 61 , thereby increasing surgical time, dissection, and presumably complications. If anything, these factors would bias our results against the survivorship of laminoplasty. Nevertheless, an important caveat of this study is demographic heterogeneity.
Our survival curves can aid patients and surgeons during the shared decision-making process. Parametric survival data can be used to more concretely discuss the risk of additional surgery when planning treatment. Furthermore, in cases of clinical equipoise between cervical procedures for a specific patient, our analysis can be used to include durability as a factor in the decision-making process.
Conclusion
Herein we present survival and reoperation curves for the most performed cervical spine procedures for myelopathy and radiculopathy. We incorporated all available long-term survival data from high-quality publications. We found no significant difference in adjacent segment surgery between ACDF and ADR. We found posterior laminectomy and fusion to have a significantly higher risk of secondary surgery when compared to ventral approaches or posterior laminoplasty. This allows a pragmatic patient-centred discussion regarding expectations and outcomes of surgery. Second, in cases of clinical equipoise between fusion procedures, particularly between single or 2 level ACDF and posterior laminectomy and fusion, our analysis suggests superior survivorship with the anterior procedure.
Supplemental Material
Supplemental Material - Long-Term Survivorship of Cervical Spine Procedures; A Survivorship Meta-Analysis and Meta-Regression
Supplemental Material for Long-Term Survivorship of Cervical Spine Procedures; A Survivorship Meta-Analysis and Meta-Regression by Mohamed Sarraj, Philip Hache, Farid Foroutan, Colby Oitment, Travis E. Marion, Daipayan Guha, and Markian Pahuta in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.