
Abstract
Study Design:
Retrospective Cohort.
Objective:
To compare the short-term outcomes for Laminoplasty, Laminectomy/fusion, and ACDF.
Methods:
We utilized a prospectively-collected, multi-center national database with a propensity score matching algorithm to compare the short-term outcomes for laminoplasty, laminectomy/fusion, and multi-level (
Results:
546 patients remained after propensity score matching, with 182 patients in each cohort. ACDF required the longest operative time 188 ± 79 versus laminectomy/fusion (169 ± 75, p = 0.017), and laminoplasty (167 ± 66, p = 0.004). ACDF required the shortest hospital stay (LOS ≥ 2: ACDF 56.6%, laminoplasty 89.6%, laminectomy/fusion 93.4%, p < 0.05). ACDF had lower overall complications (ACDF 3.9%, laminoplasty 7.7%, laminectomy/fusion 11.5%, p < 0.05), mortality (ACDF 0%, laminoplasty 0.55%, laminectomy/fusion 2.2%, p < 0.05), and unplanned readmissions (ACDF 4.4%, laminoplasty 4.4%, laminectomy/fusion 9.9%, p < 0.05). No significant differences were seen in the other outcomes including DVT/PT, acute renal failure, UTI, stroke, cardiac complications, or sepsis. In the multivariate analysis, laminectomy/fusion (OR 17, reference: ACDF) and laminoplasty (OR10, reference: ACDF) were strong independent risk factors for LOS ≥ 2 days. Laminectomy/fusion (OR 3.2, reference: ACDF) was an independent predictor for any adverse events 30-days after surgery.
Conclusions:
Laminectomy/fusion carries the highest risk for morbidity, mortality, and unplanned readmissions in the short-term postoperative period. Laminoplasty and ACDF cases carry similar short-term complications risks. ACDF is significantly associated with the longest operative duration and shortest LOS without an increase in individual or overall complications, readmissions, or reoperations
Keywords
Introduction
With the growing and aging population in the United States, there has been an increasing prevalence of degenerative cervical spine disease.1-4 Among these include degenerative cervical myelopathy (DCM), which often requires early surgical intervention to prevent disease progression.5-10 In recent decades, this has resulted in a dramatic increase in cervical fusions to treat cervical spondylotic myelopathy. 11 Various surgical options exist and continue to evolve; however, a direct comparative analysis on the outcomes of these surgeries is limited in current literature.
Surgical treatment for DCM includes both anterior (Anterior Cervical Discectomy and Fusion, ACDF) and posterior approaches (laminectomy and fusion, and laminoplasty). In a recent national database study on DCM surgery, the 10-year trends for mortality and morbidity significantly decreased and increased, respectively. 12 Unfortunately, this study did not provide direct comparisons between the individual surgical techniques. A number of studies suggest that laminectomy/fusion is associated with higher rates of readmissions and adverse events than other approaches. However, these studies are limited due to factors such as selection bias (e.g. did not isolate their population to a DCM diagnosis), a lack of an anterior approach for comparisons, inclusions of only inpatient outcomes, or limited to single-institutional analyses.13-19
The current study utilizes a prospectively-collected, multi-centered national database in conjunction with a propensity score matching algorithm to compare the short-term outcomes for DCM patients who require multi-level laminoplasty, laminectomy/fusion, and ACDF (with or without corpectomy). In comparison to prior literature, this study provides more recent data from a national sample, a more accurate procedural comparison than other public databases, and an assessment of unplanned readmissions.
Materials and Methods
The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) collects nearly 300 clinical variables, including preoperative demographics, intraoperative factors, and 30-day postoperative morbidity and mortality outcomes for patients in both the inpatient and outpatient setting. These are Health Insurance Portability and Accountability Act (HIPAA) compliant, de-identified data from over 700 sites participating in NSQIP. Current 2017 NSQIP contains more than 1 million patient encounters.
To ensure data of the highest quality, the NSQIP data is collected by highly trained surgical clinical reviewers (SCR), undergoes a systematic sampling process to control any selection bias, and is thoroughly audited, with exclusion of any participating site with an inter-rater reliability disagreement rate >5% (file:///D:/Research/NSQIP_PUF_UserGuide_2017.pdf). This study was qualified as exempt by the Center Institutional Review Board.
Data Collection
In this study, the NSQIP was queried from 2016 to 2017 to remain consistent with the 10th revision of the International Statistical Classification of Disease and Related Health Problems (ICD-10) coding. Initial inclusion criteria were adult (≥18 years) patients with a primary diagnosis of DCM (ICD10-M47.12). In our preliminary analysis, nearly 90% of patients who underwent a single-level ACDF were discharged on the same day of surgery. To ensure our study focuses on multilevel disease and to remain consistent between procedures, outpatient cases were excluded from the analyses. These patients were then further queried into the following 3 cohorts for comparative purposes. Laminoplasty: either 63050 (Laminoplasty, cervical, with decompression of the spinal cord, 2 or more vertebral segments) or 63051 (Laminoplasty, cervical, with decompression of the spinal cord, 2 or more vertebral segments; with reconstruction of the posterior bony elements [including the application of bridging bone graft and non-segmental fixation devices]). Laminectomy and Fusion: either 63015 (Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy [eg, spinal stenosis], more than 2 vertebral segments; cervical) or 63045 (Laminectomy, facetectomy, and foraminotomy [unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root(s)), (eg, spinal or lateral recess stenosis)], single vertebral segment; cervical). Both codes had a concomitant CPT code of 22842 (Posterior segmental instrumentation [eg, pedicle fixation, dual rods with multiple hooks and sublaminar wires]; 3 to 6 vertebral segments) to ensure multi-level fusion was performed in addition to the decompression. ACDF: 22551 (arthrodesis anterior interbody decompression cervical below C2) with a concomitant code of 22552 (for each additional interspace, cervical below C2). Corpectomy was coded by 63081 and/or 63082. These codes were used to ensure at least a 3-level ACDF with or without corpectomy was included in the study.
Unrelated concomitant procedures were excluded from each cohort. For instance, any thoracic fusion, lumbar fusion and/or anterior approach surgery was excluded from the laminoplasty group. Similarly, posterior decompression, posterior fusion, lower spine surgery was excluded from the ACDF cohort. For the laminectomy/fusion cohort, any anterior approach, laminoplasty, and/or lower spine surgery was excluded. Patients were excluded from the analysis if they were non-elective or emergent surgeries or prior evidence of infection (preop sepsis, wound infection, pneumonia, cancer, emergency cases and trauma, and surgery within the last 30 days). The identification of these cohorts is similar to what has been done in prior literature.14,15,20
Independent Variables
Demographic variables included sex, race, age, and body mass index (BMI). “Other_Race” included American Indian or Alaskan Native, Native Hawaiian or Pacific Islander, or Unknown/Not Reported. BMI was organized based on the World Health Organization (WHO) classification: Underweight < 18.5kg/m^2, Normal 18.5-24.9 kg/m^2, Overweight 25.0-29.9 kg/m^2, Obese Class I 30.0-34.9 kg/m^2, Obese Class II 35.0-39.9 kg/m^2, Obese Class III ≥ 40 kg/m^2.
Comorbidities included diabetes, current smoker within 1 year prior to surgery, dyspnea, functional health status prior to surgery (independent vs. partially/totally dependent), chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF) in 30 days prior to surgery, hypertension requiring medication, renal disease (dialysis, or acute renal failure preoperatively), chronic steroid use, recent weight loss >10% in last 6 months, bleeding disorder, and American Society of Anesthesiologists (ASA).
Outcome and Complication Variables
Per NSQIP, dependent variables were collected up to 30 days after surgery. The “Any Adverse Events” variable does not include readmissions or reoperations. Instead, these included death, wound complication (superficial surgical site infection [SSI], deep SSI, wound dehiscence, organ space SSI), pulmonary complications (pneumonia, unplanned intubation, ventilator use >48 hours), deep venous thrombosis/pulmonary embolism (DVT/PE), acute renal failure, urinary tract infection (UTI), stroke/cerebrovascular accident, cardiac complications (cardiac arrest requiring CPR, myocardial infection), perioperative transfusion (intraoperative and up to 72 hours postoperative), and sepsis. Other clinical factors included operative time (minutes), length of hospital stay (days), discharge disposition (home, skilled nursing facility), unplanned readmission, and return to the operating room (OR).
Statistical Analysis
To account for the potential selection bias stemming from the risk that certain patients are more likely to undergo ACDF versus laminectomy and fusion versus laminoplasty, this study employed a propensity score match algorithm. Propensity score matching assigns each patient case a conditional probability of undergoing a procedure based on a given set of covariates (e.g. demographics and comorbidities). For example, each laminoplasty case is matched to an ACDF or LF case with the most similar propensity score. Therefore, the distribution of preoperative factors become similar between the 3 cohorts.
For descriptive and comparative purposes, the bivariate analyses were performed for both with and without propensity score matching. Chi-square or Fisher’s exact test (where appropriate) and t-tests/ANOVA were used for categorical and continuous variables, respectively. Statistical significance was defined as P-value <0.05. The outcomes that were statistically significant in the bivariate analyses were subsequently further reviewed in multivariate logistic regressions. SAS software (Version 9.3; SAS Institute Inc, Cary, NC) was used for all statistical analyses.
Results
Before Propensity Score Matching
After inclusion/exclusion criteria, a total of 925 adult patients had a primary diagnosis of DCM and belonged to 1 of the 3 cohorts (laminoplasty 182 cases, ACDF 203 cases, laminectomy/fusion 540 cases). Laminoplasty patients were more often male (69.8%) than the ACDF (60.1%) and Laminectomy/Fusion (58.5%) cohorts. No significant differences were observed with BMI between groups. Laminectomy/Fusion patients were typically older (age years ± standard deviation: laminectomy/fusion 63.3 ± 10.2, ACDF 60.4 ± 10.3, laminoplasty 62.8 ± 11.1, p = 0.003) and carried a higher comorbidity burden (ASA > 2: laminectomy/fusion 69.8%, ACDF 56.7%, laminoplasty 62.1%, p = 0.002). ACDF patients were more often prior/current smokers (ACDF 31.5%, laminectomy/fusion 24.4%, laminoplasty 19.8%, p = 0.028). No significant differences were observed in other comorbidities (Table 1).
Patient Demographics and Comorbidities *Without Propensity Matching.
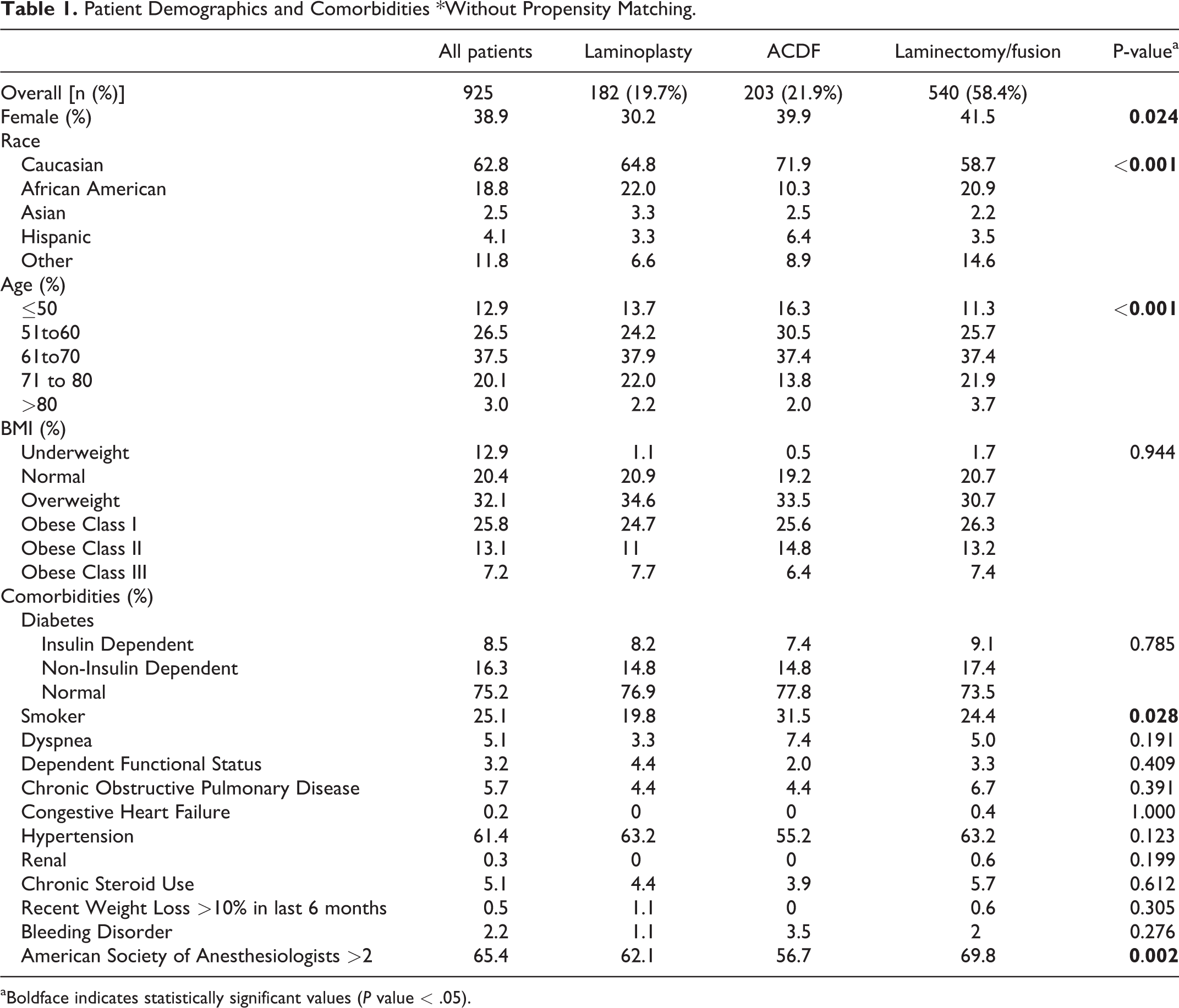
aBoldface indicates statistically significant values (P value < .05).
The mean operative time was longest for ACDF patients (189 ± 77) compared to laminoplasty (167 ± 66) and laminectomy/fusion (164 ± 68), p < 0.001. In the ACDF cohort, the majority (72.4%) underwent a 3-level surgery (versus 4-level 24.1%, and 5-level 3.4%). About 6.7% underwent a concomitant corpectomy. Most ACDF patients were discharged home (88.7%) vs. laminoplasty (75.3%) and laminectomy/fusion (67%). ACDF patients had shorter hospital stays (LOS ≥ 2 days: laminectomy/fusion 94.3%, ACDF 57.6%, laminoplasty 89.6%, p < 0.001) (Table 2).
Adverse Events *Without Propensity Matching.
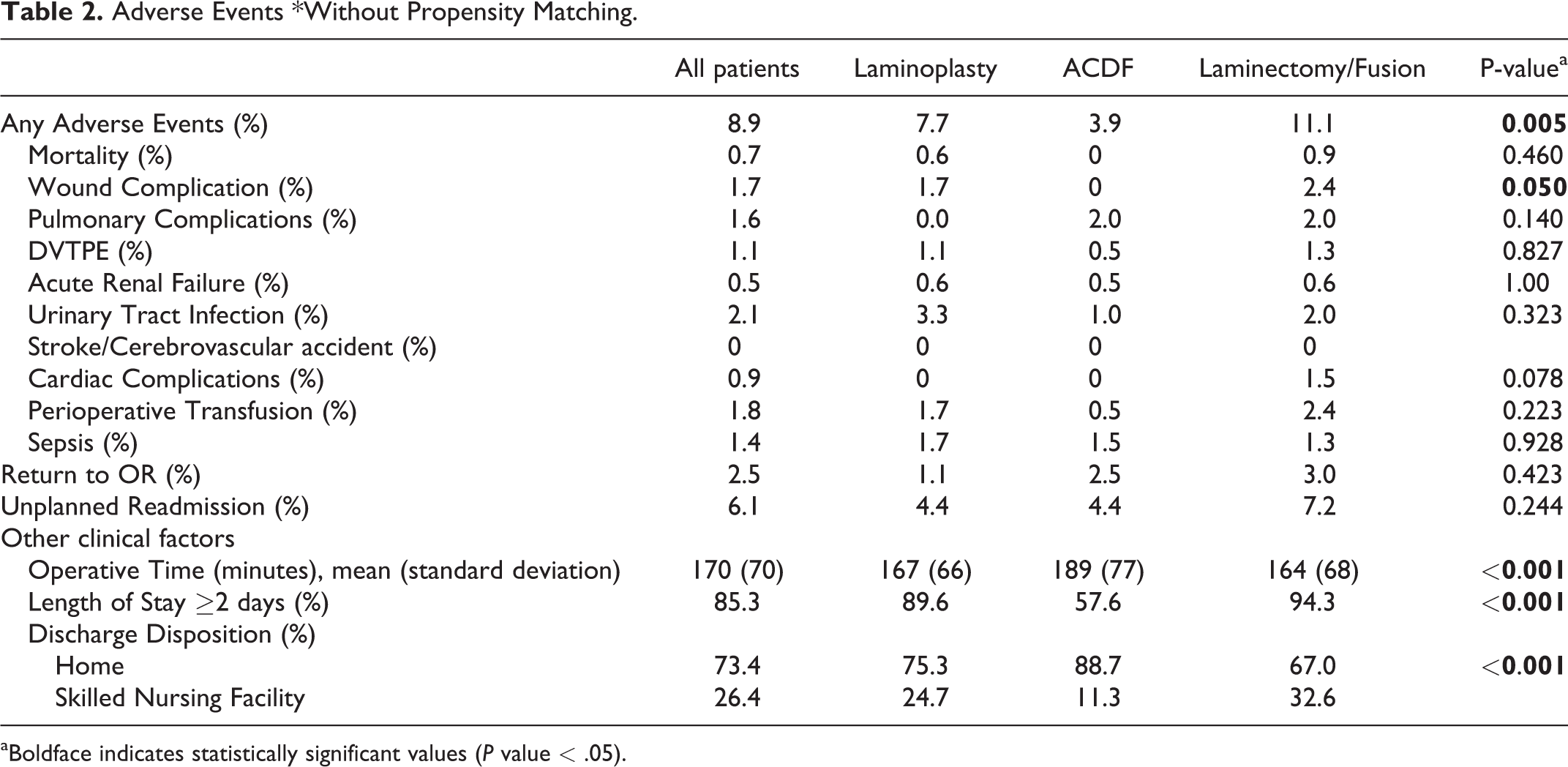
aBoldface indicates statistically significant values (P value < .05).
The any complication rate was highest for the laminectomy/fusion cohort (laminectomy/fusion 11.1%, laminoplasty 7.7%, ACDF 3.9%, p = 0.005). No difference was observed in mortality between groups. With few exceptions, individual complications were highest in the laminectomy/fusion group and lowest in the ACDF group. Statistical differences were seen in wound complication rates (laminectomy/fusion 0.93%, laminoplasty 0.55%, ACDF 0%, p = 0.05). No differences were observed for reoperation or unplanned readmission rates (Table 2).
After Propensity Score Matching
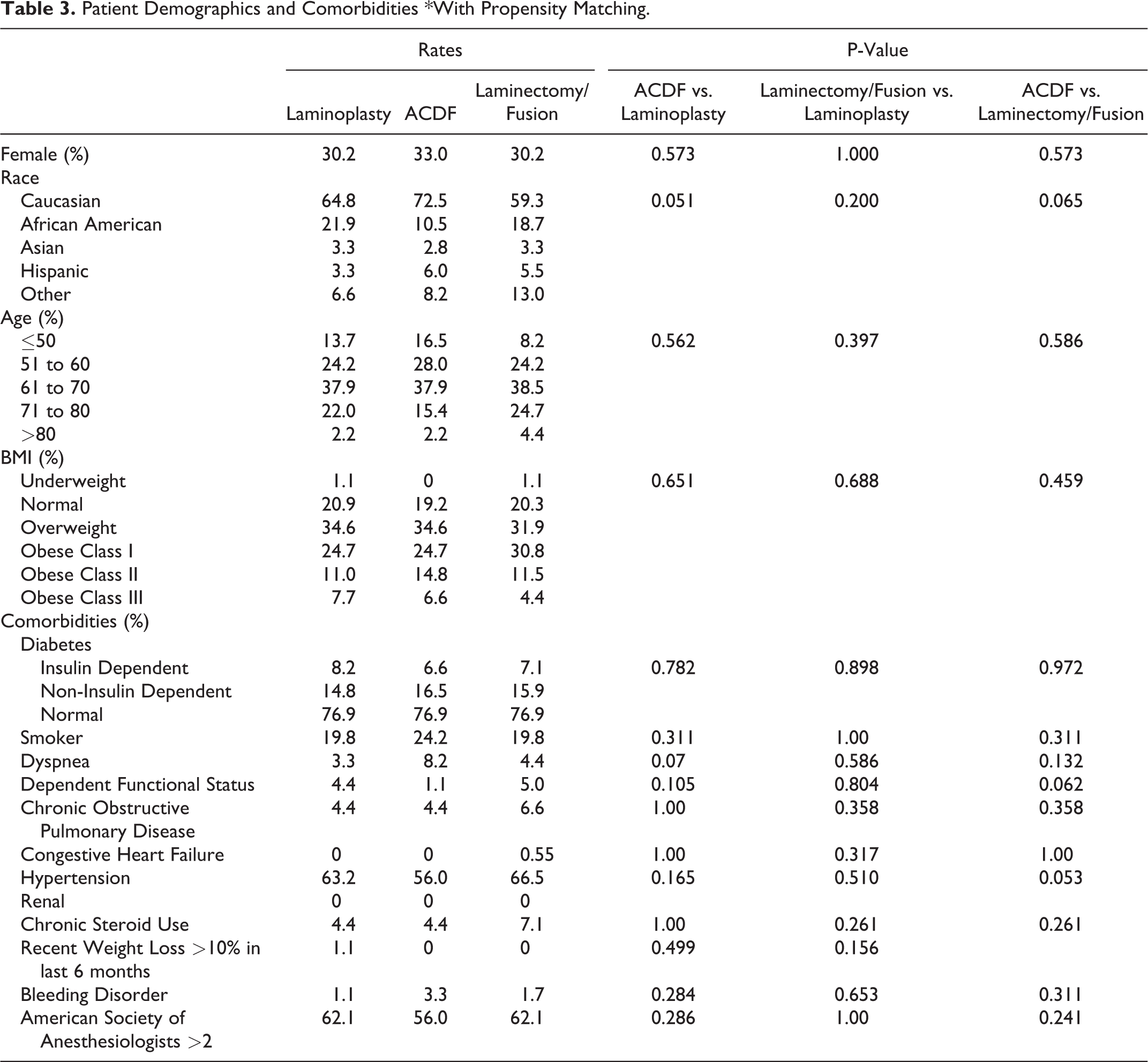
A total of 546 patients remained after propensity score matching, with 182 patients in each cohort. As seen in Table 3, the demographics and risk factors were appropriately similar between groups. In the ACDF group, 65% were 3-level, 21.7% were 4-level, and 3.0% were 5-level. About 6% of ACDF cases had concomitant corpectomy. Furthermore, ACDF cases (with or without corpectomy) required the longest operative time 188 ± 79 versus laminectomy/fusion (169 ± 75, p = 0.017), and laminoplasty (167 ± 66, p = 0.004). In contrast, ACDF required the shortest hospital stay (LOS ≥ 2: ACDF 56.6%) versus laminectomy/fusion (93.4%, <0.001), and versus laminoplasty (89.6%, p < 0.001). ACDF patients were more frequently discharged home (87.4%) versus laminectomy/fusion (73.6%, p = 0.002) and versus laminoplasty (75.3%, p = 0.005).
Patient Demographics and Comorbidities *With Propensity Matching.
In regard to postoperative complications, most statistically significant comparisons were observed between ACDF and laminectomy/fusion. These included overall complications (ACDF 3.9%, laminectomy/fusion 11.5%, p = 0.006), mortality (ACDF 0%, laminectomy/fusion 2.2%, p = 0.044), wound complications (ACDF 0%, laminectomy/fusion 2.2%, p = 0.044), perioperative transfusion (ACDF 0.55%, laminectomy/fusion 3.9%, p = 0.032), and unplanned readmissions (ACDF 4.4%, laminectomy/fusion 9.9%, p = 0.042). No significant differences were seen in the other outcomes including DVT/PT, acute renal failure, UTI, stroke, cardiac complications, or sepsis (Table 3). The complication rates for laminoplasty were not significantly different to most of those seen after ACDF and laminectomy/fusion, with the exception to pulmonary complications (laminoplasty 0%, ACDF 2.2%, p = 0.044), unplanned readmissions (laminoplasty 4.4%, laminectomy/fusion 9.9%), and length of stay >2 days (laminoplasty 89.6%, ACDF 56.6%, p = 0.005) (Table 4).
Adverse Events *With Propensity Matching.
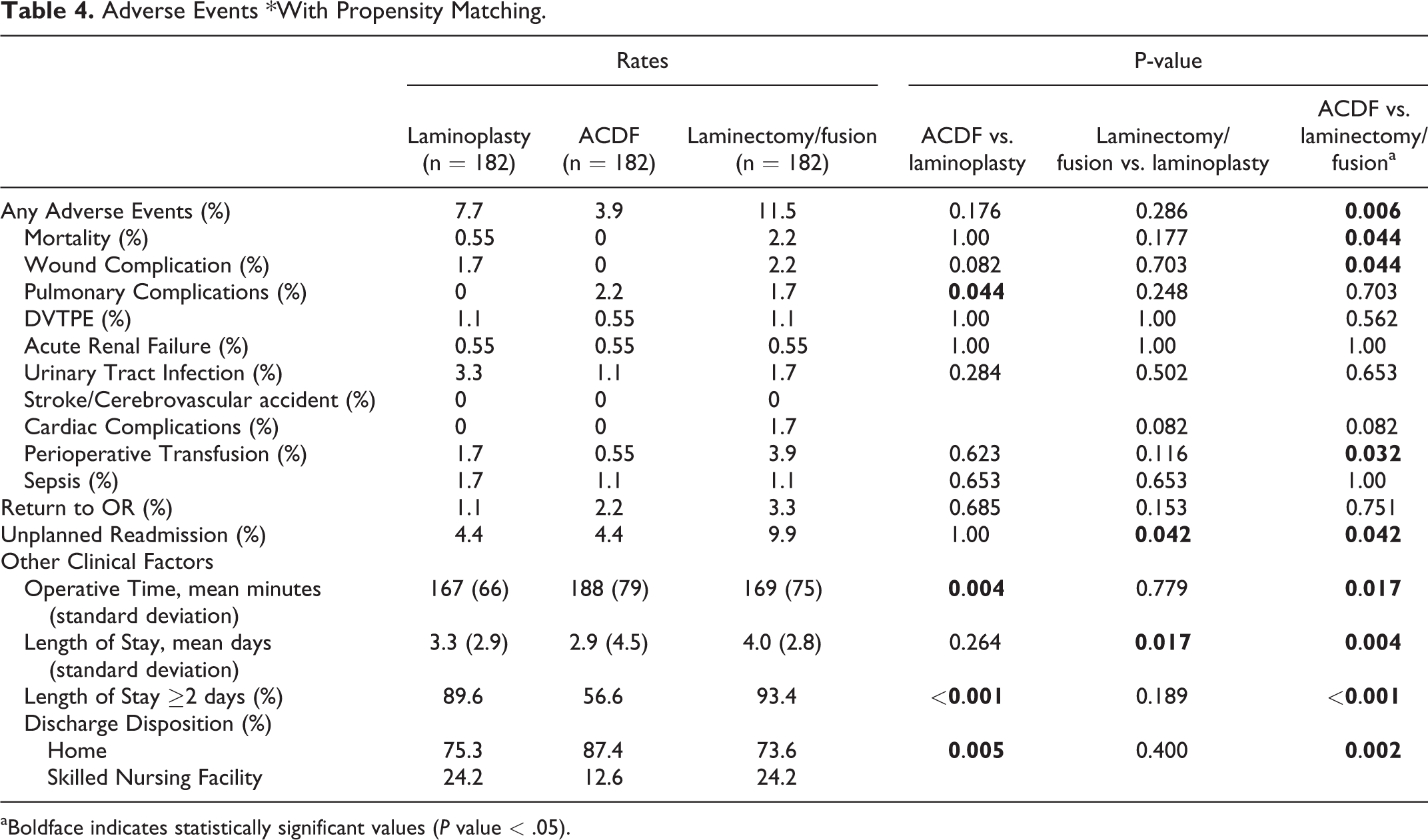
aBoldface indicates statistically significant values (P value < .05).
In the multivariate analysis, laminectomy/fusion (OR 17, p < 0.001, reference: ACDF) and laminoplasty (OR 10, p < 0.001, reference: ACDF) were independent risk factors for LOS ≥ 2 day. In addition, laminectomy/fusion was an independent predictor (OR 3.2, p = 0.029, reference: ACDF) for any adverse event 30-days after surgery. Other multivariate regressions did not yield statistically significant predictors, such as those for unplanned readmissions (Table 5).
Multivariate Analyses.
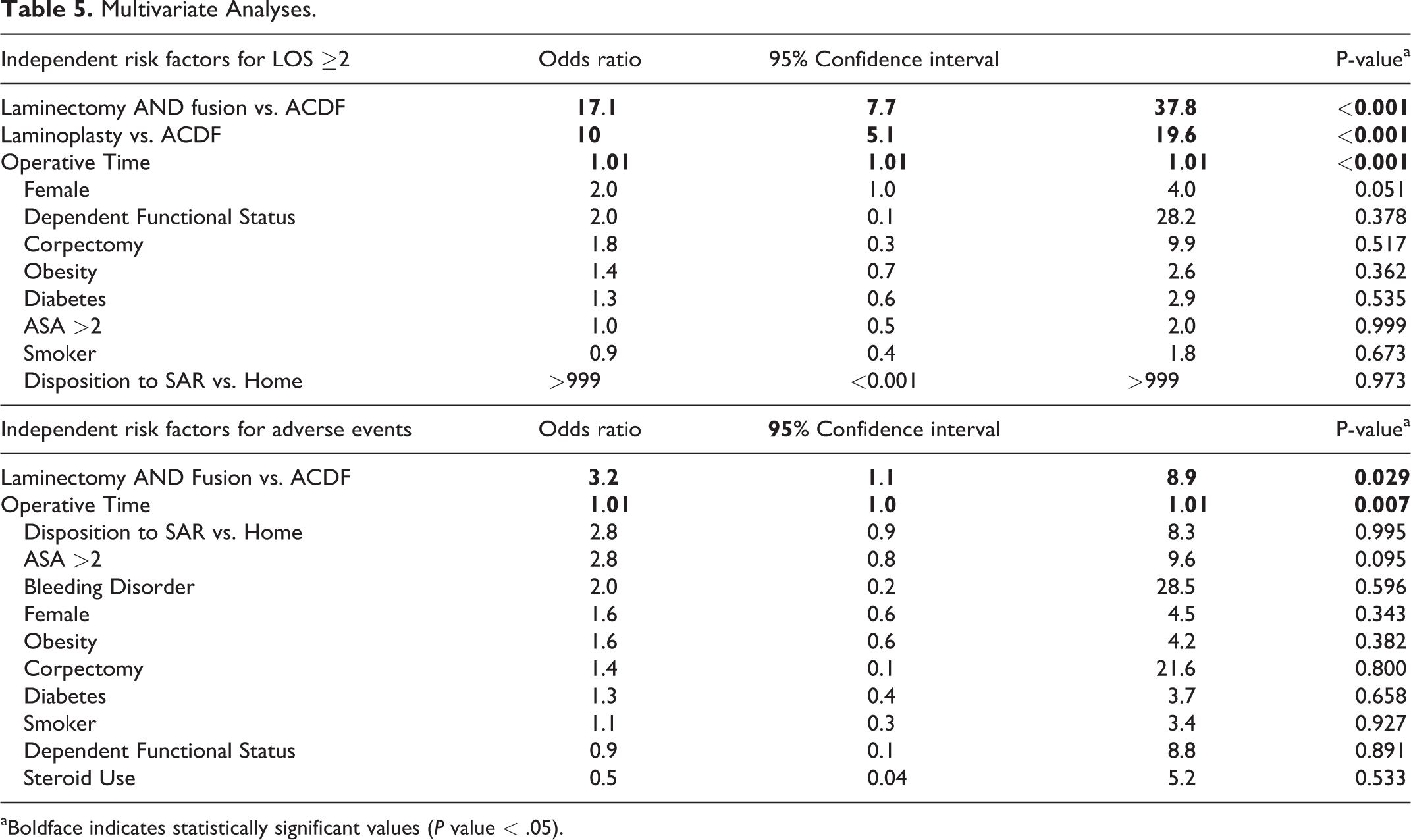
aBoldface indicates statistically significant values (P value < .05).
Reasons for Unplanned Readmission
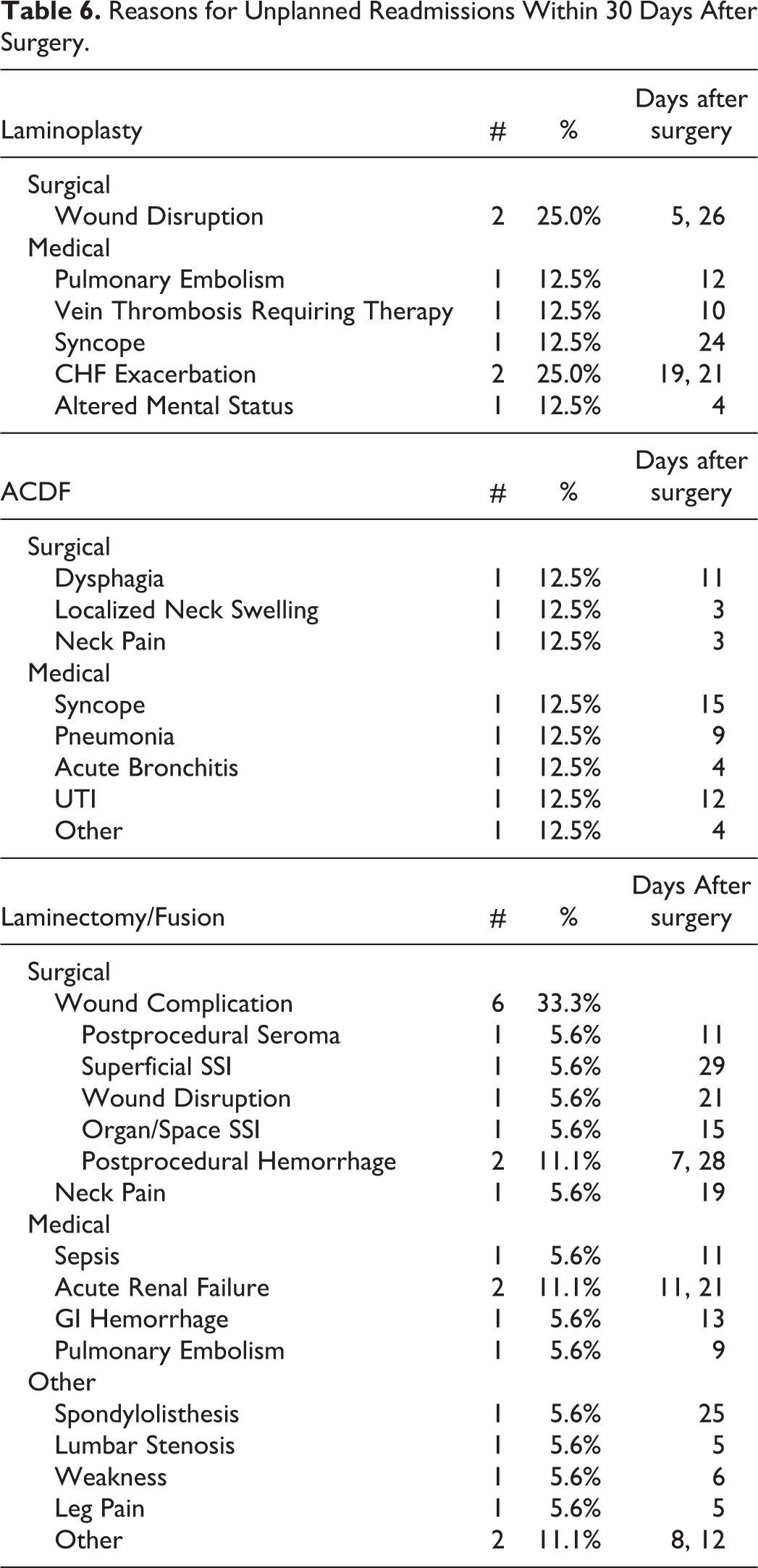
Wound complication is the most common (33.3%) reason for unplanned readmission after laminectomy/fusion. Surgery-related reasons for readmissions after ACDF included dysphagia, localized neck swelling, and neck pain. Wound complication (25%) was also a common reason for unplanned readmission for laminoplasty (Table 6).
Reasons for Unplanned Readmissions Within 30 Days After Surgery.
Discussion
Several established options for the treatment of DCM exist, but the ideal surgical technique remains elusive due to the lack of comprehensive comparative analyses on clinical outcomes and the disparate evidence supporting each approach. Furthermore, indications for each technique may vary based on a number of factors including cervical alignment, the presence of ossification of posterior longitudinal ligament (OPLL), surgeon preference, the number of levels involved, etc. With regard to the anterior approach, ACDF can achieve direct decompression of the affected cord and establish solid cervical stability, but at the cost of possible dysphagia, dysphonia, pseudoarthrosis, and adjacent segment disease, especially for multilevel DCM.21-24 As for the posterior approach, laminectomy/fusion can effectively decompress the cord but result in a significant loss of cervical range of motion. 16 In contrast, laminoplasty serves as a motion-preserving procedure that may obviate the risk of pseudoarthrosis, provide the option for future anterior procedures, and allow for effective indirect decompression, which may be safer than direct decompression. Nevertheless, there is a paucity of data confirming the superiority of one approach with respect to short-term outcomes and complications. 25
In a prior national database study, Varthi et al reviewed 779 patients who underwent cervical laminoplasty versus posterior decompression and fusion.14,15 Similar to our study, they found that laminectomy/fusion patients were more comorbid at baseline than laminoplasty patients. They found that laminectomy/fusion increased LOS, any adverse events (19.7% vs. 11.1%), and readmission risk (7.9% vs. 3.3%). Similar results were observed in a more recent, larger NSQIP review. However, these studies did not further specify the underlying diagnoses for these procedures.14,15 Heterogeneity in the indications for surgery may bias the type of surgical technique employed.
Kaye et al. reviewed 54,348 patients who underwent surgical intervention for cervical spondylotic myelopathy and found an overall morbidity and mortality rate of 9.8% and 0.43%, respectively. 26 They found that posterior-only and combined approaches were significantly associated with higher complications when compared with ACDF (OR 1.66, p < 0.001). Due to limitations inherent to database design, laminoplasty could not be directly compared to laminectomy/fusion.
In a meta-analysis of 10 studies comparing anterior versus posterior approach for the treatment of multilevel cervical spondylotic myelopathy, Luo et al found that anterior surgery group had a higher postoperative complication risk (OR 1.65, p = 0.009), reoperation rate (OR8.67, p < 0.001), intraoperative blood loss and operative time, but lower LOS. 23 It is important to note that the anterior approach was defined as ACDF with or without corpectomy in 8 of those studies. Corpectomy is known to be more technically difficult with higher rates of perioperative complications including, dural tear, graft/instrumentation-related issues, extended operative time, and blood loss.27,28 In our study, ACDF cases with corpectomy had longer operative times (243 ± 156) than those without corpectomy (185 ± 70.4, p = 0.016). However, corpectomy was not a significant risk factor for complications after ACDF surgery and no ACDF case with corpectomy required a reoperation or readmission within 30 days of surgery in this study.
In a single-surgeon retrospective matched cohort analysis, Woods et al. compared laminoplasty to laminectomy/fusion in 121 patients over a 5-year period with a minimum 6.7 month follow up period. 29 They found that subjective clinical improvements occurred in both cohorts in regards to gait and pain. Laminoplasty patients trended toward a higher overall complication rate (13% vs. 9%) and revision rate (5% vs. 2%); however, there was no statistical significance associated with these differences.
Recently, Kato et al compared the 30-day perioperative complications as well as the 2-year patient-reported outcomes (e.g. modified Japanese Orthopaedic Association, Neck Disability Index, Short Form-36, and Physical Component Summary) between those who received an anterior versus posterior surgical treatment for degenerative cervical myelopathy. 30 Similar to our study, they used a propensity-score matching algorithm; however, they were able to include preoperative mJOA scores and MRI findings (e.g. extent of disc disease, OPLL, number of diseased levels) in their matched analysis. These authors found that the 2-year postoperative patient-reported outcomes and the overall complication rates were not significantly different between groups. In the sub-analysis, they found that certain individual complications were statistically more common based on the approach (e.g. anterior—dysphagia/dysphonia; posterior—surgical site infection, C5 radiculopathy). Given the relatively small sample size in each cohort after propensity score matching, these authors report that they were not able to compare outcomes between specific surgical techniques.
To build upon prior literature, we used a large national sample to compare the outcomes between common surgical techniques to treat cervical spondylotic myelopathy. In comparison to the prior literature, our study showed that the overall complication and mortality rate was highest for laminectomy/fusion (any adverse event 11.5%, mortality 2.2%) versus ACDF (any adverse event 3.9%, mortality 0%, p = 0.006) and versus laminoplasty (any adverse event 7.7%, mortality 0.55%, p = 0.286). As a result, laminectomy/fusion patients were at highest risk for requiring an unplanned readmission (9.9%) versus laminoplasty (4.4%, p = 0.042) and versus ACDF (4.4%, p = 0.042). The most common reasons for an unplanned readmission after laminectomy/fusion was wound complication (33.3%). This was similar for the laminoplasty cohort. Interestingly, wound complications were not common for the ACDF cohort. Instead neck swelling and dysphagia were common reasons for readmission. It is possible that wound complications are inherently more common with a posterior approach given that well-known risk factors such as diabetes, obesity, and steroid use, were controlled for in the propensity score matched analysis. The higher tensile forces that pull at the midline fascia along the backside of the neck may contribute to the higher risk for wound issues. The fact that laminoplasty did not have a significantly higher risk for this compared to ACDF may be due to the relatively less soft tissue dissection required in comparison to laminectomy and fusion. ACDF patients required the longest mean operative time likely due to concomitant corpectomy, but this did not translate into worse short-term complications and readmissions for the patient. Furthermore, ACDF patients had the lowest mean length of stay (2.9 ± 4.5 days) with nearly half of ACDF patients requiring less than 3 days in the hospital. In comparison, laminoplasty (LOS ≥ 2: 89.6%, p < 0.001; mean LOS 3.3 ± 2.9) and laminectomy/fusion (LOS ≥ 2: 93.4%, p < 0.001; mean LOS 4 ± 2.8) groups required much longer hospital stays. When controlling for perioperative factors, both laminoplasty and laminectomy/fusion were significant independent risk factors for LOS ≥ 2 days. The longer LOS for these 2 cohorts is likely related to the significantly greater proportion of patients being discharged to a skilled nursing facility than home.
There are a number of limitations to consider for this study. First, patients older than 90 years were coded as 90+ to prevent patients from being identified due to unique data per the NSQIP data; therefore, the age distribution is somewhat truncated. Second, the data is limited to 30 days after surgery and limited to readmissions to hospitals within NSQIP only. It is possible that complications occur beyond this follow-up period. Third, an in-depth analysis of surgery-specific variables is limited due to the general nature of this database. For instance, there are a number of different techniques for laminoplasty (e.g. “French-door laminoplasty,” “open-door laminoplasty) that we were not able to control for in our analyses. Fourth, the specific indications for the chosen procedure is not known. For example, if a patient had kyphosis, a laminoplasty might not have been appropriate. Fifth, we were not able to fully control for the number of levels of pathology between the different procedures. Unfortunately, this is limited by CPT definitions. For example, CPT 22842 was used to include concomitant cervical fusion after decompression. However, CPT 22842 only provides the range of 3 to 6 vertebral segments. Although it is possible to count the number of times the CPT 22614 is used concomitantly for each patient undergoing a posterior cervical fusion, we found that there was significant coding error as many of these patients did not have this CPT code or was under-reported. Therefore, we cannot further elucidate the exact number of levels. We acknowledge that this can lead to selection bias as it is possible that a laminectomy/fusion may involve a higher number of levels and that a 6-level posterior cervical fusion may be at risk for a worse complication rate than a 3-level ACDF. We attempted to narrow the range of levels by including at least a 3-level ACDF and excluding unrelated procedures as explained in the methods. Finally, while short-term complications are relevant, what may be more important are long-term outcomes and complications, such as pseudarthrosis, adjacent segment disease, implant failure, and patient-reported outcomes. These questions may be better answered in future large, prospective studies.
Conclusion
Although we found that laminectomy/fusion carries the highest risk for early postoperative morbidity, mortality, and unplanned readmissions, there are instances when disease specific factors including cervical alignment, presence or absence of OPLL, number of levels involved, body habitus, short neck, may favor a posterior approach over an anterior one. In some instances, a laminectomy/fusion may be more appropriate than laminoplasty (e.g. significant axial neck pain, cervical kyphosis >10-15 degrees, negative k-line, hill-shaped OPLL).31-35 Therefore, the ideal surgical technique for treating DCM hinges on multiple factors, which should include both short- and long-term outcomes. Our study’s findings should be included in the preoperative discussion with the patient when determining the ideal surgical approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.