
Abstract
Study Design
Retrospective Cohort Study.
Objective
Modic changes (MCs) have been associated with low back pain; however, their prognostic value in surgical outcomes—particularly in patients with lumbar spinal stenosis (LSS) treated with decompression alone—remains unclear. Few studies have investigated the progression and long-term clinical impact of MCs. This study aimed to evaluate the 10-year progression of MCs and their association with clinical outcomes following posterior decompression surgery for LSS.
Methods
This study included 62 patients who underwent posterior decompression for LSS and completed a 10-year follow-up with MRI and clinical assessments. MCs and disc degeneration were evaluated using standardized MRI criteria. Japanese Orthopaedic Association (JOA) scores and recovery rates were assessed preoperatively and at follow-up. Outcomes were compared between Modic-negative patients and those with preoperative Modic Type 1 or Type 2 changes. Analysis of covariance adjusted for confounding variables.
Results
The prevalence of MCs increased from 37.1% preoperatively to 74.2% at 10 years. Type 1 changes were dynamic, often progressing to Type 2 or 3. Type 2 changes were more stable and associated with significantly lower postoperative JOA scores and recovery rates compared to Modic-negative or Type 1 patients (P < 0.05), after adjustment for age, sex, sagittal alignment parameters, and disc degeneration. Type 2 MCs were also linked with minimal improvement in back pain.
Conclusion
Modic changes, particularly Type 2, are associated with inferior long-term outcomes. These findings suggest that Modic Type 2 may serve as a prognostic marker of advanced degeneration and may be associated with reduced recovery following decompression surgery.
Keywords
Introduction
Lumbar spinal canal stenosis (LSS) is a degenerative condition of the lumbar spine that commonly causes lower extremity pain or numbness, particularly during standing and walking. Its prevalence increases with age, with Japanese epidemiological data indicating a prevalence of approximately 10-11% among individuals aged 70-79 years. 1 In cases of severe LSS that do not respond to conservative treatment, posterior decompression surgery is widely performed in patients without intervertebral instability and has been shown to provide favorable outcomes. 2
Modic changes (MCs) are signal alterations in the vertebral endplates and adjacent bone marrow detected on magnetic resonance imaging (MRI), typically associated with intervertebral disc degeneration.3-5 While the association between MCs and LBP5-10 has been well documented, their clinical significance in lumbar spinal surgery remains unclear. Several studies have examined whether preoperative MCs influence clinical outcomes following decompression or instrumented fusion surgery for lumbar spine disorders.11-23 However, the majority of this research has focused on lumbar disc herniation11,15-17,20-23 or spondylosis,12,13,18 with treatment including discectomy11,15-17,20-23 or instrumented fusion.11-13
Only a few studies have addressed the impact of MCs in patients with lumbar spinal canal stenosis (LSS) treated surgically.14,24,25 These studies consistently reported that the presence of MCs did not significantly affect clinical outcomes, regardless of the surgical method employed. However, the long-term clinical significance of MCs in this patient population remains unclear, and to date, no study has investigated the progression of MCs over a 10-year postoperative period.
This study aims to investigate the 10-year progression of Modic changes and their impact on long-term clinical outcomes in patients with LSS treated with posterior decompression surgery.
Materials and Methods
Study Design and Participants
This retrospective study analyzed prospectively collected data as a subanalysis of a previous longitudinal investigation that examined the long-term postoperative progression of intervertebral disc degeneration following posterior decompression surgery for LSS, in comparison with healthy controls. 26 In this subanalysis, specific attention was given to MCs, with the aim of evaluating their long-term progression and clinical impact.
This study shares the same patient cohort as our previous 10-year MRI analysis. 26 Between 2005 and 2007, 258 consecutive patients underwent posterior lumbar decompression surgery for LSS or mild degenerative spondylolisthesis (Meyerding Grade I) at a single institution and were initially enrolled in the study. Of the 258 patients initially enrolled, 52 died, 116 were lost to follow-up, and 17 declined or were unable to undergo MRI. An additional 11 were excluded (6 due to unrelated neurological disorders affecting gait and 5 due to having undergone additional lumbar fusion surgery). Thus, 62 patients (24%) completed the 10-year follow-up and were included in the final analysis. The mean age at the time of surgery was 68.6 years (range: 41-82), and the final cohort consisted of 47 men and 15 women, with an average follow-up duration of 11.3 ± 1.2 years.
Eligible participants were required to be at least 50 years old, have MRI-confirmed LSS with neurogenic claudication, and no history of tumor, vertebral fracture, spinal infection, or significant spinal deformity. All included patients underwent posterior decompression surgery and completed at least 10 years of clinical and imaging follow-up. Patients were excluded if they were older than 75 years at the time of surgery, had undergone previous lumbar spinal surgery, presented with cervical or thoracic spinal pathology, had neurological conditions such as Parkinson’s disease, or underwent additional lumbar fusion at the index level during the follow-up period.
For clinical outcome comparisons, only Modic changes located at the decompressed (operative) spinal level(s) were considered. Patients with Modic changes exclusively at non-operative levels were excluded from the Modic-positive group. Specifically, 1 patient with Modic Type 1 changes at L2/3 and 2 patients with Modic Type 2 changes at L1/2 or L2/3 were not classified as Modic-positive for the purpose of outcome analysis.
Surgical Technique
All patients underwent posterior lumbar decompression using the spinous process-splitting laminectomy technique without instrumentation, as previously described by Watanabe et al.27,28 This technique preserves the paravertebral muscles and posterior ligamentous structures, providing adequate spinal canal decompression with minimal invasiveness.
Evaluation of MCs and Degeneration of Intervertebral Disc on MRI
MRI evaluations were conducted using a 1.5 Tesla system (Signa Excite HD 1.5 T, GE Healthcare, Milwaukee, WI), with T2-weighted sagittal images (TR/TE: 5000/100 ms; slice thickness: 4 mm; field of view: 24 cm; matrix: 256 × 192) as previously described. 26
MCs and Degenerative changes from L1/2 to L5/S1 were assessed on MRI images. Endplate and bone marrow changes were classified into 4 categories based on established MRI criteria. These included normal endplates (no changes), Modic Type 1 (MC1) (decreased signal on T1-weighted images and increased signal on T2-weighted images), Modic Type 2 (MC2) (increased signal on T1-weighted images and isointense or slightly increased signal on T2-weighted images), and Modic Type 3 (MC3) (low signal intensity on both T1- and T2-weighted images).
Disc degeneration was evaluated by assessing decreased signal intensity (DSI) and disc space narrowing (DSN) on T2-weighted sagittal images29-31 (Supplemental Data 1). For statistical analysis, DSI grades were numerically quantified as follows: Grade 0 = 0, Grade 1a = 1, Grade 1b = 2, Grade 1c = 3, and Grade 2 = 4. DSN grades were scored as Grade 0 = 0, Grade 1 = 1, and Grade 2 = 2. Scores from all lumbar levels (L1/2 to L5/S1) were summed to calculate a total degeneration score for each patient.
Image interpretation was performed independently by 2 experienced spine surgeons who were blinded to clinical outcomes. Interobserver reliability was assessed using the weighted kappa statistic.
Radiographic Assessment
Preoperative standing lateral radiographs of the whole spine were used to evaluate sagittal alignment. The following spinopelvic parameters were measured: pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), PI-LL mismatch (PI minus LL), sagittal vertical axis (SVA), and the C7 plumb line (C7PL).
A slip percentage at the affected level was also measured to assess segmental instability. A slip of more than 10% was regarded as radiographic evidence of segmental instability at that level in this study.
Clinical Outcome Assessment
Clinical outcomes were evaluated preoperatively and at the 10-year follow-up using the Japanese Orthopaedic Association (JOA) scoring system (Supplemental data 2). The low back pain (LBP) category of the JOA score comprises 4 levels: no pain (3 points), occasional mild pain (2 points), frequent mild pain with occasional severe pain (1 point), and continuous severe pain (0 points). The JOA recovery rate (%) was calculated using the following formula:

This study focused on 2 primary evaluations: (1) changes in preoperatively recognized Modic changes over the 10-year follow-up period, and (2) the influence of preoperative MCs on clinical outcomes as assessed by the JOA score at 10 years postoperatively.
Statistical Analysis
Comparisons between patients with and without Modic changes were performed using either Fisher’s exact test or the Student’s t-test, as appropriate. A P-value of <0.05 was considered statistically significant. To evaluate differences in clinical outcomes at the 10-year follow-up, analysis of covariance (ANCOVA) was used to compare JOA total scores and recovery rates between the Modic-negative group and those with MC1 or MC2, while adjusting for age, sex, sagittal alignment parameters (SVA, PI-LL), and preoperative disc degeneration scores (DSI or DSN).
Interobserver reliability between the 2 neuroradiologists was assessed using the weighted kappa statistic on 20 randomly selected intervertebral discs. All statistical analyses were performed using STATA 16 (Stata Corporation, College Station, TX, USA).
Results
Prevalence and Progression of MCs
Distribution of Modic Changes Preoperatively and at 10-Year Postoperative Follow-Up
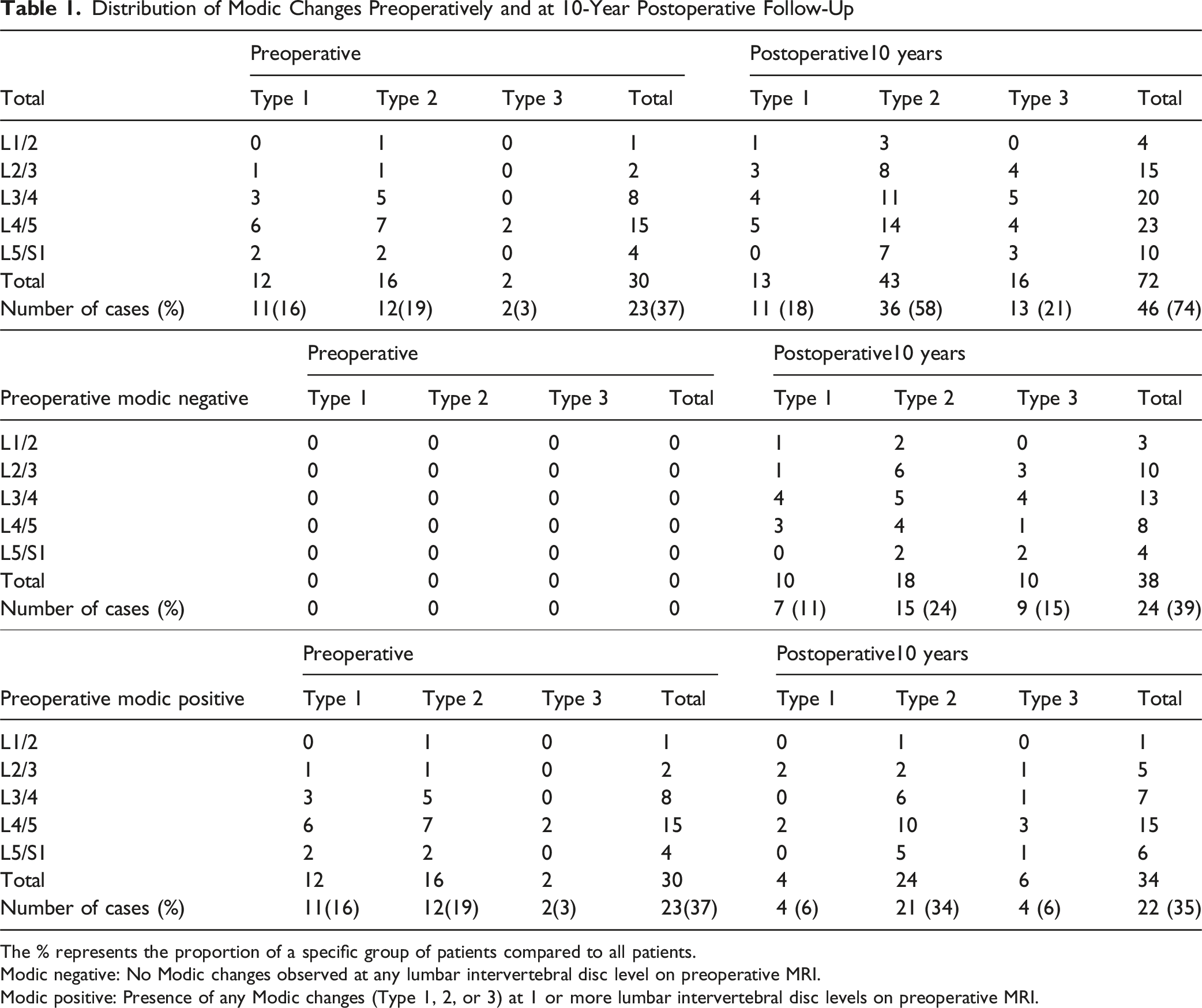
The % represents the proportion of a specific group of patients compared to all patients.
Modic negative: No Modic changes observed at any lumbar intervertebral disc level on preoperative MRI.
Modic positive: Presence of any Modic changes (Type 1, 2, or 3) at 1 or more lumbar intervertebral disc levels on preoperative MRI.
At the 10-year postoperative follow-up, the prevalence of MCs had increased to 46 patients (74.2%), involving 72 levels in total. During the 10-year interval, 38 new MCs developed in 24 patients (38.7%). Among the newly developed MCs, MC2 was the most frequent (18 levels), followed by MC3 (10 levels). The L3/4 and L2/3 levels were most frequently affected, with 13 and 10 levels, respectively.
Distribution and Progression of Preoperative Modic Type 1 Changes by Lumbar Level at 10-Year Follow-up
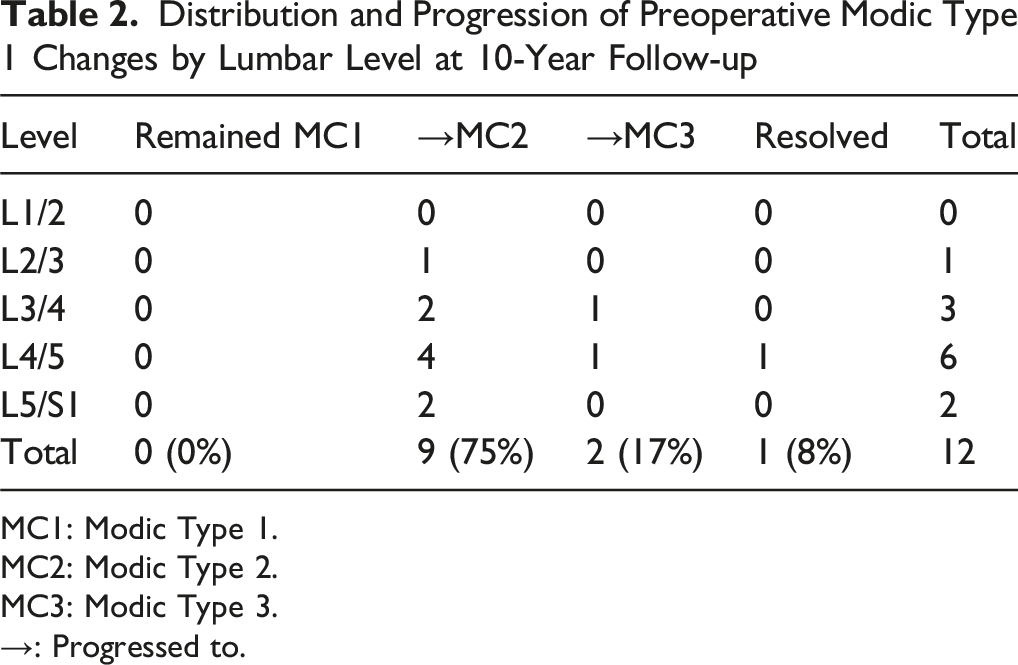
MC1: Modic Type 1.
MC2: Modic Type 2.
MC3: Modic Type 3.
→: Progressed to.
Distribution and Progression of Preoperative Modic Type 2 Changes by Lumbar Level at 10-Year Follow-up
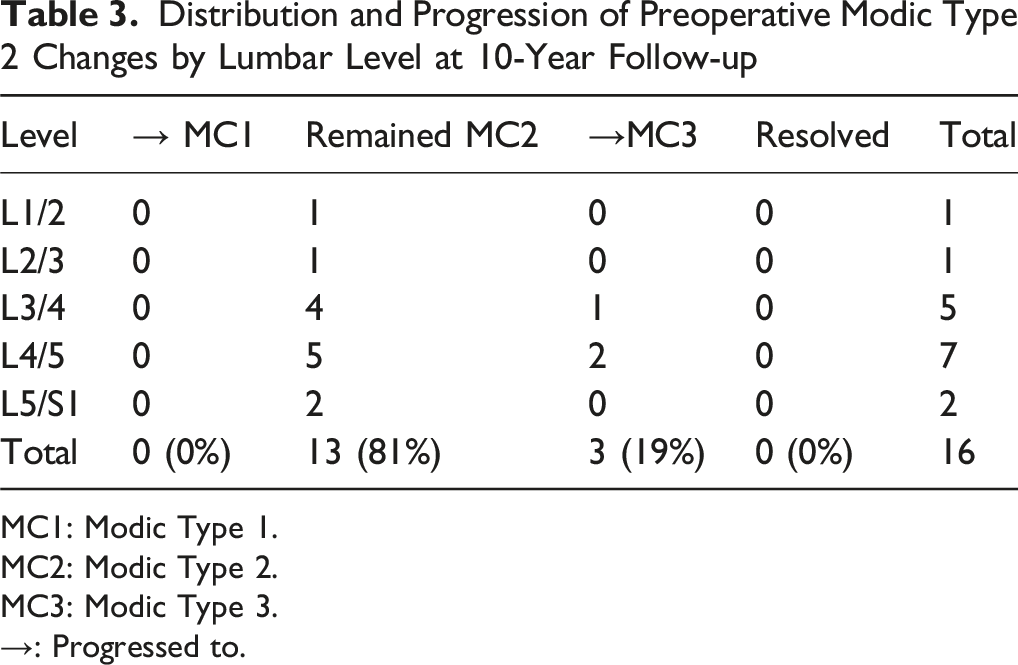
MC1: Modic Type 1.
MC2: Modic Type 2.
MC3: Modic Type 3.
→: Progressed to.
Among the 39 patients who were Modic-negative at baseline, we compared those who remained Modic-negative (n = 15) and those who developed new Modic changes at 10-year follow-up (n = 24) (Supplemental data 3). Most baseline characteristics, including age, BMI, number of decompressed levels, and preoperative disc degeneration (DSI, DSN), were comparable between groups. However, the postoperative Modic-positive group exhibited a significantly greater PI–LL mismatch (13.8 ± 10.8 vs 8.2 ± 10.9, P = 0.048). In addition, lumbar lordosis tended to be smaller (41.5 ± 10.4 vs 46.9 ± 10.2, P = 0.13), and SVA tended to be larger (46.7 ± 34.3 vs 33.9 ± 33.8, P = 0.44) in the Modic-positive group. Although not statistically significant, DSI and DSN were also slightly greater in the Modic-positive group, suggesting a trend toward more advanced disc degeneration.
Comparison Between Modic-Negative and Modic-Positive Groups
Demographic, Radiographic, and Surgical Characteristics of Patients Stratified by the Presence and Type of Modic Changes
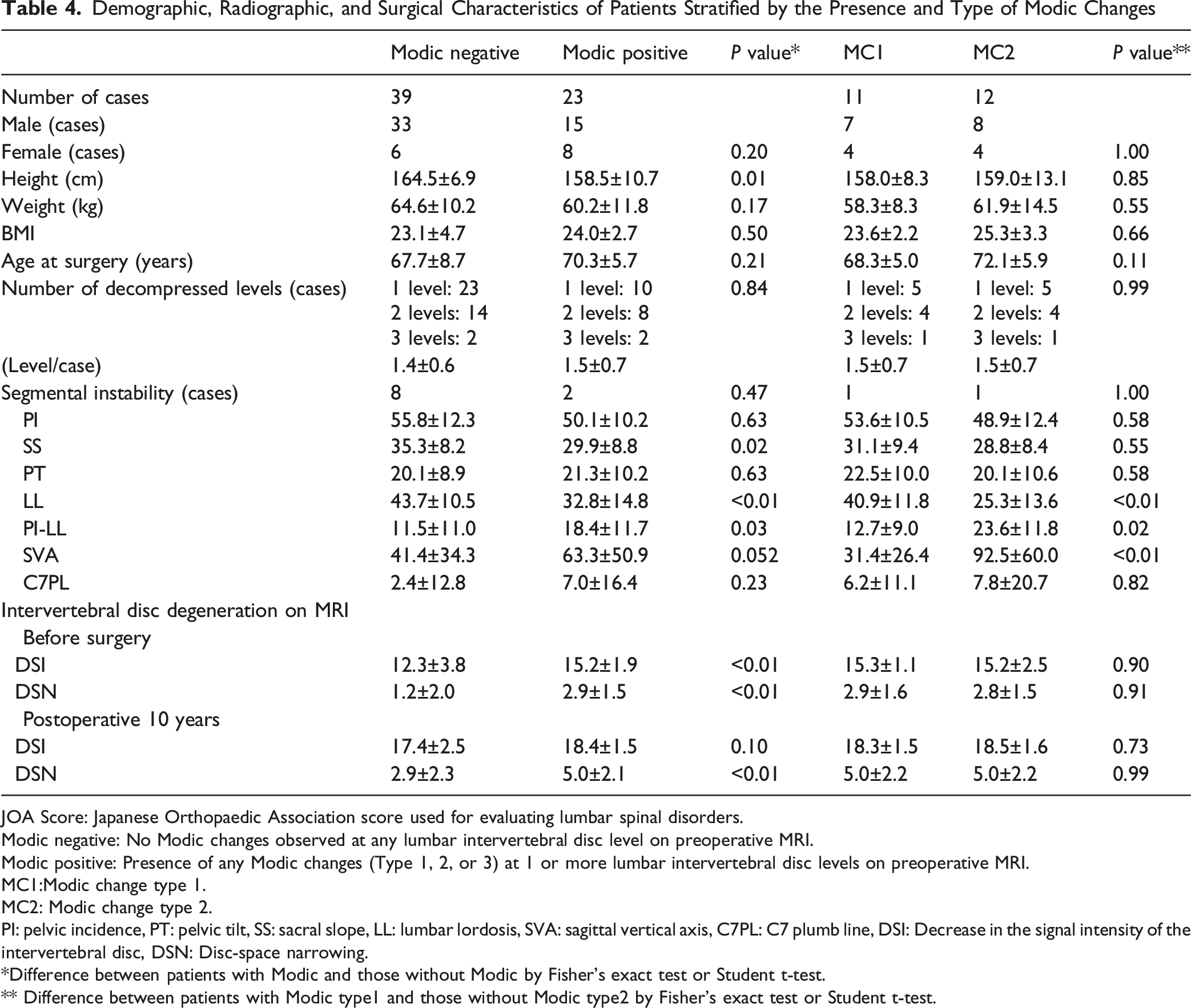
JOA Score: Japanese Orthopaedic Association score used for evaluating lumbar spinal disorders.
Modic negative: No Modic changes observed at any lumbar intervertebral disc level on preoperative MRI.
Modic positive: Presence of any Modic changes (Type 1, 2, or 3) at 1 or more lumbar intervertebral disc levels on preoperative MRI.
MC1:Modic change type 1.
MC2: Modic change type 2.
PI: pelvic incidence, PT: pelvic tilt, SS: sacral slope, LL: lumbar lordosis, SVA: sagittal vertical axis, C7PL: C7 plumb line, DSI: Decrease in the signal intensity of the intervertebral disc, DSN: Disc-space narrowing.
*Difference between patients with Modic and those without Modic by Fisher’s exact test or Student t-test.
** Difference between patients with Modic type1 and those without Modic type2 by Fisher’s exact test or Student t-test.
Among the 62 patients, 10 had mild segmental instability of more than 10% slip. Of these, 2 patients were in the M group and 8 in the MN group (Table 4). There was no statistically significant difference in the frequency of segmental instability between the 2 groups (P = 0.47).
In terms of sagittal alignment, the M group showed a significantly lower SS (29.9 ± 8.8 vs 35.3 ± 8.2, P = 0.02), smaller LL (32.8 ± 14.8 vs 43.7 ± 10.5, P < 0.01), and a greater PI–LL mismatch (18.4 ± 11.7 vs 11.5 ± 11.0, P = 0.03) (Table 4). The SVA also tended to be larger in the M group (63.3 ± 50.9 mm vs 41.4 ± 34.3 mm), although this did not reach statistical significance (P = 0.052).
MRI evaluation revealed more pronounced intervertebral degeneration in the M group (Table 4). The mean DSI score was significantly higher in the M group than in the MN group (15.2 ± 1.9 vs 12.3 ± 3.8, P < 0.01), and the mean DSN score was also significantly greater (2.9 ± 1.5 vs 1.2 ± 2.0, P < 0.01).
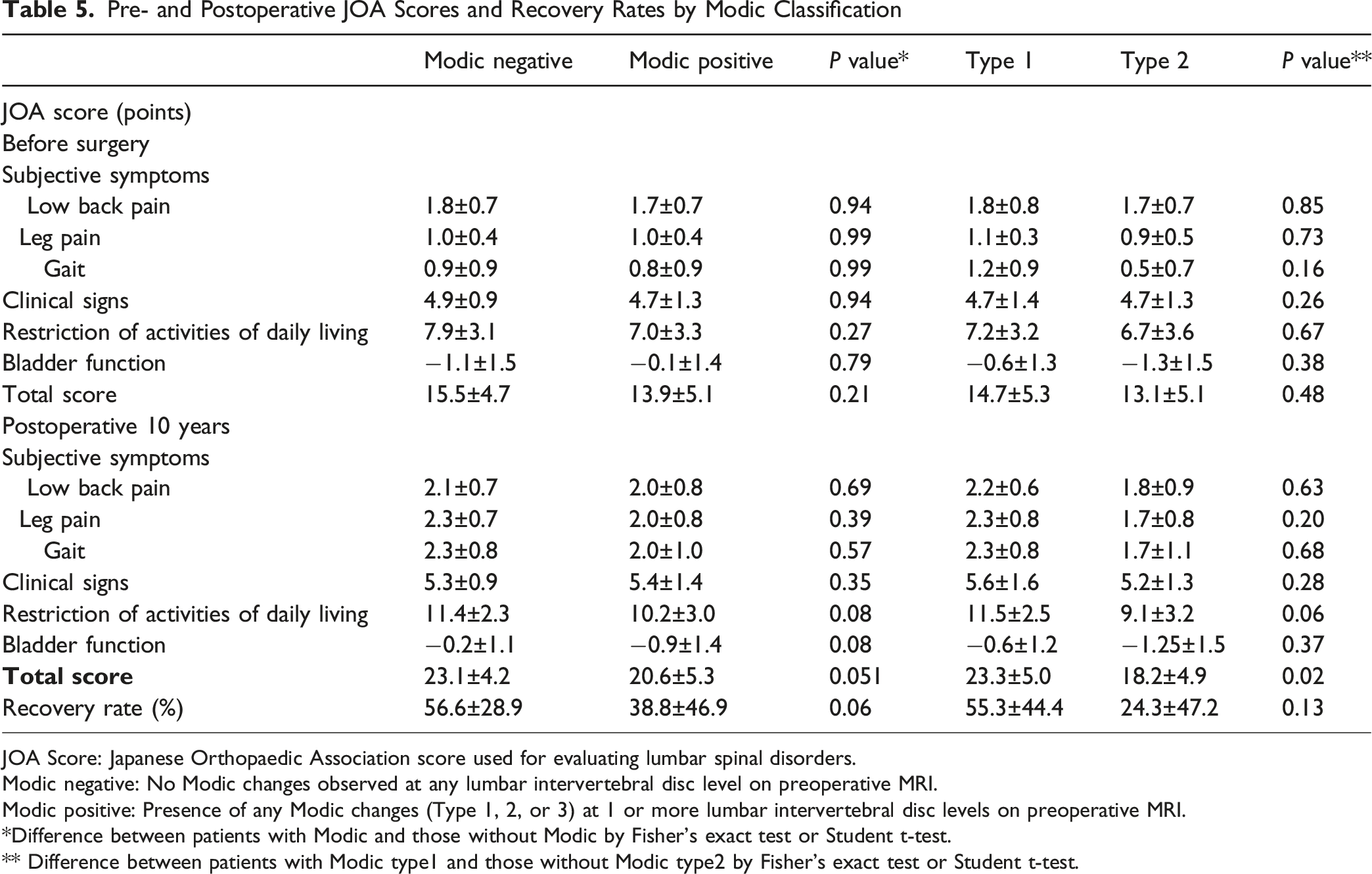
Pre- and Postoperative JOA Scores and Recovery Rates by Modic Classification
JOA Score: Japanese Orthopaedic Association score used for evaluating lumbar spinal disorders.
Modic negative: No Modic changes observed at any lumbar intervertebral disc level on preoperative MRI.
Modic positive: Presence of any Modic changes (Type 1, 2, or 3) at 1 or more lumbar intervertebral disc levels on preoperative MRI.
*Difference between patients with Modic and those without Modic by Fisher’s exact test or Student t-test.
** Difference between patients with Modic type1 and those without Modic type2 by Fisher’s exact test or Student t-test.
At the 10-year follow-up, the mean total JOA score remained lower in the M group compared to the MN group (20.6 ± 5.3 vs 23.1 ± 4.2, P = 0.051). Similarly, the recovery rate was reduced in the M group (38.8 ± 46.9%) compared to the MN group (56.6 ± 28.9%, P = 0.06). Although subscores, including the low back pain component, did not differ significantly between the 2 groups.
Comparison Between MC1, and MC2 Groups
The M group was further subdivided based on preoperative MC classification into 11 patients with MC1 (MC1 group) and 12 patients with MC2 (MC2 group). Baseline characteristics, including DSI and DSN scores, were similar between the 2 subgroups, with the exception of LL, PI-LL mismatch, and SVA (Table 4).
Preoperatively, the total JOA scores did not differ significantly between the 2 groups (14.7 ± 5.3 for MC1 vs 13.1 ± 5.1 for MC2, P = 0.48) (Table 5). Likewise, no significant differences were observed in subscores, including the low back pain category (1.8 ± 0.7 vs 1.7 ± 0.7, P = 0.85).
At the 10-year follow-up, the MC2 group had significantly lower total JOA scores compared to the MC1 group (18.2 ± 4.9 vs 23.1 ± 4.2, P = 0.02). Subscores across the domains were consistently lower in the MC2 group, indicating a generally poorer clinical outcome for patients with preoperative MC2 Modic changes. The mean recovery rate was also lower in the MC2 group (24.3 ± 47.2%) compared to the MC1 group (55.3 ± 4.4%), although this difference did not reach statistical significance (P = 0.13).
Comparison Between Modic Negative (MN) Group and MC1 or MC2 Groups
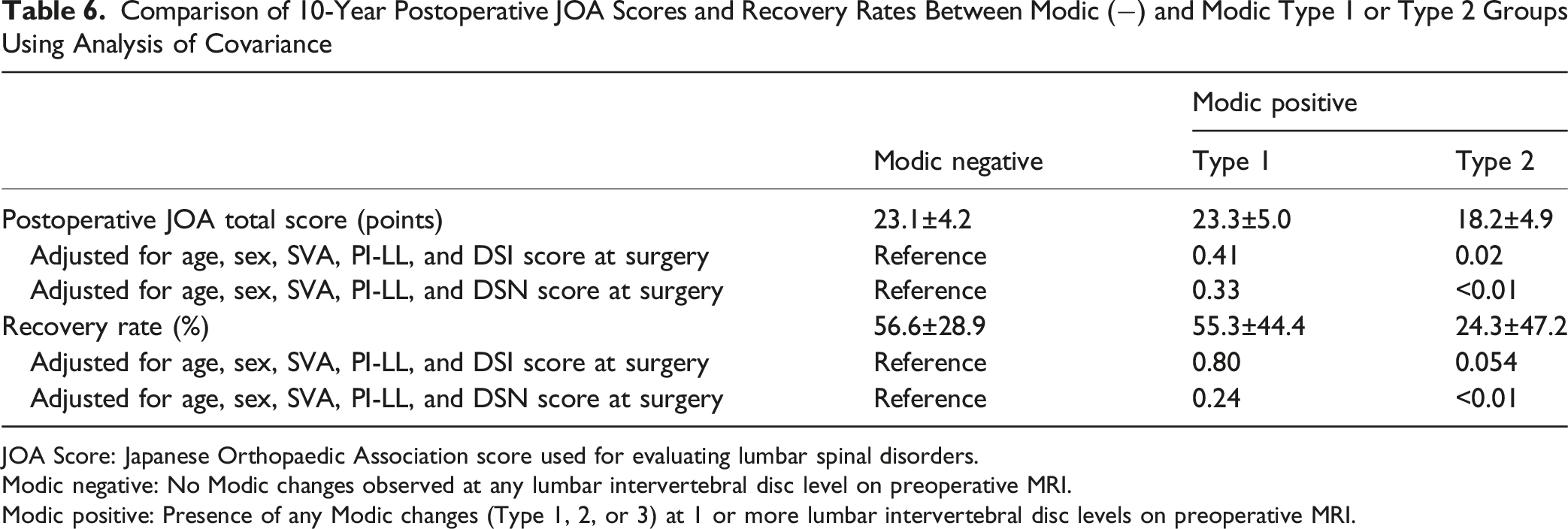
Comparison of 10-Year Postoperative JOA Scores and Recovery Rates Between Modic (−) and Modic Type 1 or Type 2 Groups Using Analysis of Covariance
JOA Score: Japanese Orthopaedic Association score used for evaluating lumbar spinal disorders.
Modic negative: No Modic changes observed at any lumbar intervertebral disc level on preoperative MRI.
Modic positive: Presence of any Modic changes (Type 1, 2, or 3) at 1 or more lumbar intervertebral disc levels on preoperative MRI.
After adjusting for these factors, postoperative JOA scores in the MC2 group remained significantly lower than those in the MN group (P = 0.02 after adjustment for DSI; P < 0.01 after adjustment for DSN). Similarly, the recovery rate was lower in the MC2 group compared to the MN group, with a trend toward significance (P = 0.054 after adjustment for DSI; P < 0.01 after adjustment for DSN). These findings suggest that the presence of Modic Type 2 changes is associated with inferior clinical outcomes, independent of age, sex, sagittal alignment, and disc degeneration severity.
Inter-rater Reliability
For intervertebral disc degeneration evaluations, the weighted kappa values were 0.94 for both DSI and DSN, indicating excellent agreement. For MC classification, the weighted kappa values were 0.80 for MC1, 0.90 for MC2, and 0.92 for MC3, also reflecting a high level of inter-rater reliability across all Modic subtypes.
Discussion
Prevalence of MCs
We observed a marked increase in the prevalence of MCs from 37% preoperatively to 74% at the 10-year follow-up. Jensen et al. previously reported that the overall prevalence of MCs ranges from 14% to 36%, with an estimated increase of 6% per decade. 7 MCs are most frequently observed in individuals aged 60-79, with prevalence exceeding 40%. The 37% preoperative prevalence in our cohort aligns with these findings. However, the doubling of prevalence to 74% over the follow-up period exceeds rates reported in general populations. This likely reflects the more advanced and progressive disc degeneration typical of patients with LSS, as opposed to healthy individuals. 26
Progression Patterns of Modic Changes
Our longitudinal analysis demonstrated that MCs are dynamic in nature and can progress over time. Among the 3 types, MC1 were the most unstable, with the majority progressing to MC2 and, less commonly, to MC3. Notably, 1 MC1 lesion completely resolved during the follow-up period, reinforcing the hypothesis that MC1 may reflect an active inflammatory phase with the potential for reversibility. In contrast, MC2 were more stable but occasionally progressed to MC3, supporting the view that MC2 reflects more chronic, structural alterations in the vertebral endplate and adjacent bone marrow.
These observations are consistent with previous imaging studies that suggest a pathophysiological continuum in the development of MCs.3,20,32-35 For example, Rahme et al. 20 reported that in patients with lumbar disc herniation treated with microdiscectomy, approximately 60% of MC1 had progressed to MC2 at a median follow-up of 41 months. Similarly, Ohtori 24 found that in patients with lumbar canal stenosis who underwent posterior lumbar fusion, MC1 changes frequently converted to MC2 over time. Importantly, MC2 rarely reverted to MC1, suggesting that MC2 represents a stabilized and potentially irreversible stage in the MC spectrum.
Clinical Significance of Modic Changes
Importantly, our study found that patients with preoperative MC2 experienced worse clinical outcomes, including significantly lower total scores, and lower postoperative JOA recovery rates, compared to those without MCs or with MC1.
The relationship between preoperative MCs and surgical outcomes in lumbar spine disorders remains controversial. In the setting of microdiscectomy for lumbar disc herniation, several studies have reported that the presence of MCs is associated with less favorable postoperative results.17-19,21 Conversely, other studies have found no significant impact of MCs on postoperative outcomes.15,16,20,22,23
Evidence specifically examining the impact of MCs in LSS patients treated surgically is limited.14,24,25 These prior studies consistently concluded that the presence of MCs did not significantly affect clinical outcomes, regardless of the surgical approach. In contrast, our study found that preoperative MC2 was associated with significantly worse clinical outcomes compared to both MC-negative and MC1 group. This discrepancy may be due to differences in outcome measures, follow-up duration, and surgical techniques used across studies. Ohtori 24 evaluated patients treated with posterolateral fusion, while Gautschi 25 included a mix of microdiscectomy, decompression, with or without fusion. Among the prior studies, Ulrich 14 conducted a study with a design similar to ours, directly comparing clinical outcomes between patients with and without Modic changes who underwent decompression surgery. However, their study used different outcome measures—the Spinal Stenosis Measure (SSM), Numeric Rating Scale (NRS), and EQ-5D-3L—and had a shorter follow-up period of 36 months. In comparison, our study employed the JOA score and assessed outcomes over a 10-year period, potentially capturing long-term effects that earlier studies may have missed.
A likely explanation for the poorer outcomes observed in the MC2 group lies in the underlying pathophysiological differences between Modic types. MC1 is thought to represent an active inflammatory phase, which may resolve spontaneously or respond favorably to decompression. In contrast, MC2 represents a more chronic, fibrofatty stage with irreversible endplate damage. Importantly, this distinction suggests that the worse outcomes seen in MC2 patients may not be due to a poor surgical response per se, but rather due to the more advanced and less reversible stage of degeneration that MC2 represents.
Decompression primarily targets neurogenic symptoms such as claudication and radiculopathy, but does not adequately address axial low back pain. In our study, many patients experienced frequent or activity-limiting low back pain preoperatively, as reflected by the JOA scores (1.8 ± 0.7 in the MN group and 1.7 ± 0.7 in the M group). Following decompression, the MN group improved to 2.1 ± 0.7 and the MC1 group to 2.2 ± 0.6, suggesting that decompression alone can relieve low back pain in many cases. In contrast, minimal improvement was observed in the MC2 group (from 1.7 ± 0.7 to 1.8 ± 0.9 ). Although the difference between groups was not statistically significant, this trend suggests that Modic Type 2 may be associated with persistent axial symptoms, likely reflecting irreversible degenerative changes.
Sagittal imbalance is a well-known contributor to postoperative low back pain. Our study found that patients with Modic Type 2 changes had greater PI–LL mismatch and SVA, indicating a tendency toward global malalignment. However, even after adjusting for these parameters, clinical outcomes remained significantly worse in the MC2 group. These results suggest that Modic Type 2 changes may serve as an independent marker of advanced segmental degeneration and poor surgical prognosis, regardless of global spinal alignment.
Although decompression remains the standard of care for LSS in the absence of apparent instability, our findings suggest that patients with MC2 located at the decompressed level—especially those presenting with axial low back pain or potential segmental instability—may be less responsive to decompression alone. In such cases, additional fusion procedures may be considered on a case-by-case basis. Thus, low back pain, especially in the context of Modic Type 2 changes, may serve as a clinically relevant prognostic factor in the evaluation of long-term surgical outcomes.
Study Limitations
This study has several limitations. First, the final sample size was relatively small, with only 62 patients completing the 10-year follow-up (24% follow-up rate), introducing the potential for selection bias. However, the ability to conduct both clinical and MRI assessments at a 10-year interval in these 62 patients remains a significant strength of this study and provides valuable long-term prognostic insight.
Another limitation is the lack of consistent data on the longitudinal trajectory of clinical outcomes. While interim clinical information was available for some cases, it was not uniformly collected across all patients and therefore was not included in this analysis. As a result, changes in clinical symptoms over time could not be fully assessed.
In addition, while Modic changes were analyzed only at the decompressed level for clinical correlation, signal changes were present throughout the lumbar spine. Some patients developed new Modic changes during the 10-year follow-up; however, these were not included in the outcome analysis to maintain focus on the impact of preoperative Modic changes. The influence of non-operative level and newly developed Modic changes, as well as global sagittal alignment, on postoperative outcomes warrants further investigation.
Conclusions
This 10-year longitudinal study demonstrates that MCs become increasingly prevalent following posterior decompression surgery for LSS. MC1s were dynamic, frequently progressing to more chronic forms such as Type 2 or 3 over time. Notably, patients with preoperative MC2s exhibited significantly worse long term clinical outcomes, including lower JOA scores and recovery rates. These findings suggest that Modic Type 2 may serve as a prognostic marker of advanced and less reversible degeneration, which may limit the potential for recovery following decompression surgery.
Supplemental Material
Supplemental Material - Ten-Year Clinical Outcomes After Decompression Surgery for Lumbar Spinal Stenosis: The Impact of Preoperative Modic Changes
Supplemental Material for Ten-Year Clinical Outcomes After Decompression Surgery for Lumbar Spinal Stenosis: The Impact of Preoperative Modic Changes by Kota Watanabe, Takeshi Fujii, Takehiro Michikawa, Takahito Iga, Toshiki Okubo, Kazuki Takeda, Satoshi Suzuki, Masahiro Ozaki, Osahiko Tsuji, Narihiro Nagoshi, Morio Matsumoto, and Masaya Nakamura in Global Spine Journal
Footnotes
Author Contributions
Kota Watanabe: Conceptualization, Writing – original draft, supervision, project administration. Takeshi Fujii: Study design, MRI evaluation, data collection, analysis, Writing – review & editing. Takehiro Michikawa: Statistical analysis, methodology consultation, data interpretation. Takahito Iga, Toshiki Okubo, Kazuki Takeda: MRI evaluation, data acquisition. Satoshi Suzuki, Masahiro Ozaki: Clinical data collection, patient recruitment, clinical outcome review. Osahiko Tsuji, Narihiro Nagoshi: Patient recruitment, clinical outcome review. Morio Matsumoto, Masaya Nakamura: Critical revision of the manuscript, supervision.
Ethical Approval
This study was conducted in accordance with institutional ethical standards and was approved by the appropriate ethics committee (IRB approval number 20110142).
Informed Consent
Written informed consent was obtained from all participants prior to enrollment.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request. Due to privacy or ethical restrictions, the data are not publicly available but may be shared for academic purposes.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.